- About
- Mission Statement
Education. Evidence. Regrowth.
- Education.
Prioritize knowledge. Make better choices.
- Evidence.
Sort good studies from the bad.
- Regrowth.
Get bigger hair gains.
Team MembersPhD's, resarchers, & consumer advocates.
- Rob English
Founder, researcher, & consumer advocate
- Research Team
Our team of PhD’s, researchers, & more
Editorial PolicyDiscover how we conduct our research.
ContactHave questions? Contact us.
Before-Afters- Transformation Photos
Our library of before-after photos.
- — Jenna, 31, U.S.A.
I have attached my before and afters of my progress since joining this group...
- — Tom, 30, U.K.
I’m convinced I’ve recovered to probably the hairline I had 3 years ago. Super stoked…
- — Rabih, 30’s, U.S.A.
My friends actually told me, “Your hairline improved. Your hair looks thicker...
- — RDB, 35, New York, U.S.A.
I also feel my hair has a different texture to it now…
- — Aayush, 20’s, Boston, MA
Firstly thank you for your work in this field. I am immensely grateful that...
- — Ben M., U.S.A
I just wanted to thank you for all your research, for introducing me to this method...
- — Raul, 50, Spain
To be honest I am having fun with all this and I still don’t know how much...
- — Lisa, 52, U.S.
I see a massive amount of regrowth that is all less than about 8 cm long...
Client Testimonials150+ member experiences.
 Scroll DownPopular Treatments
Scroll DownPopular Treatments- Treatments
Popular treatments. But do they work?
- Finasteride
- Oral
- Topical
- Dutasteride
- Oral
- Topical
- Mesotherapy
- Minoxidil
- Oral
- Topical
- Ketoconazole
- Shampoo
- Topical
- Low-Level Laser Therapy
- Therapy
- Microneedling
- Therapy
- Platelet-Rich Plasma Therapy (PRP)
- Therapy
- Scalp Massages
- Therapy
- More
IngredientsTop-selling ingredients, quantified.
- Saw Palmetto
- Redensyl
- Melatonin
- Caffeine
- Biotin
- Rosemary Oil
- Lilac Stem Cells
- Hydrolyzed Wheat Protein
- Sodium Lauryl Sulfate
- More
ProductsThe truth about hair loss "best sellers".
- Minoxidil Tablets
Xyon Health
- Finasteride
Strut Health
- Hair Growth Supplements
Happy Head
- REVITA Tablets for Hair Growth Support
DS Laboratories
- FoliGROWTH Ultimate Hair Neutraceutical
Advanced Trichology
- Enhance Hair Density Serum
Fully Vital
- Topical Finasteride and Minoxidil
Xyon Health
- HairOmega Foaming Hair Growth Serum
DrFormulas
- Bio-Cleansing Shampoo
Revivogen MD
- more
Key MetricsStandardized rubrics to evaluate all treatments.
- Evidence Quality
Is this treatment well studied?
- Regrowth Potential
How much regrowth can you expect?
- Long-Term Viability
Is this treatment safe & sustainable?
Free Research- Free Resources
Apps, tools, guides, freebies, & more.
- Free CalculatorTopical Finasteride Calculator
- Free Interactive GuideInteractive Guide: What Causes Hair Loss?
- Free ResourceFree Guide: Standardized Scalp Massages
- Free Course7-Day Hair Loss Email Course
- Free DatabaseIngredients Database
- Free Interactive GuideInteractive Guide: Hair Loss Disorders
- Free DatabaseTreatment Guides
- Free Lab TestsProduct Lab Tests: Purity & Potency
- Free Video & Write-upEvidence Quality Masterclass
- Free Interactive GuideDermatology Appointment Guide
- More
Articles100+ free articles.
-
Does Anavar Cause Hair Loss?
-
10 Best Shampoos for Hair Loss in 2026
-
XYON Review: Do Their Products Actually Regrow Hair?
-
Minoxidil Before and After Photos [2026] | Does It Work?
-
How to Get Finasteride: Is It Over the Counter?
-
Keeps Review: The Truth About Their Hair Loss Treatments?
-
7 Best Oils for Hair Growth
-
Hims Hair Growth Reviews: The Pros, Cons, and Real Results
PublicationsOur team’s peer-reviewed studies.
- Microneedling and Its Use in Hair Loss Disorders: A Systematic Review
- Use of Botulinum Toxin for Androgenic Alopecia: A Systematic Review
- Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia
- Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results
- A Hypothetical Pathogenesis Model For Androgenic Alopecia:Clarifying The Dihydrotestosterone Paradox And Rate-Limiting Recovery Factors
Menu- AboutAbout
- Mission Statement
Education. Evidence. Regrowth.
- Team Members
PhD's, resarchers, & consumer advocates.
- Editorial Policy
Discover how we conduct our research.
- Contact
Have questions? Contact us.
- Before-Afters
Before-Afters- Transformation Photos
Our library of before-after photos.
- Client Testimonials
Read the experiences of members
Before-Afters/ Client Testimonials- Popular Treatments
-
Articles
When it comes to microneedling vs. platelet-rich plasma, which is better? Dermatologists often recommend platelet-rich plasma therapy (PRP) as a treatment for hair loss. This autologous therapy evokes the body’s natural healing response, as does microneedling. We look at what the research studies say about the effectiveness of these two treatments. Time and cost factors are also important considerations for most people.
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.

What is Microneedling?
Microneedling, a minimally invasive cosmetic procedure, has emerged as a promising treatment for various forms of hair loss, including androgenic alopecia (AGA). This technique involves using specialized devices, like rollers of pens, equipped with fine needles to create controlled micro-injuries on the scalp.

A derma roller for at-home microneedling.
These micro-injuries stimulate the body’s natural wound-healing processes, enhancing blood flow and promoting the release of growth factors essential for hair regeneration. This method not only improves hair density and thickness but also increases the efficacy of topical hair growth products by facilitating deeper penetration into the scalp.[1]Dhurat, R., Sukesh, M.S., Avhad, G., Dandale, A., Pal, A., Pund, P. (2013). A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study. International … Continue reading,[2]English, R.S., Ruiz, S., DoAmaral, P. (2021). Microneedling and Its Use in Hair Loss Disorders: A Systematic Review. Dermatology and Therapy. 12. 41-60. Available at: … Continue reading
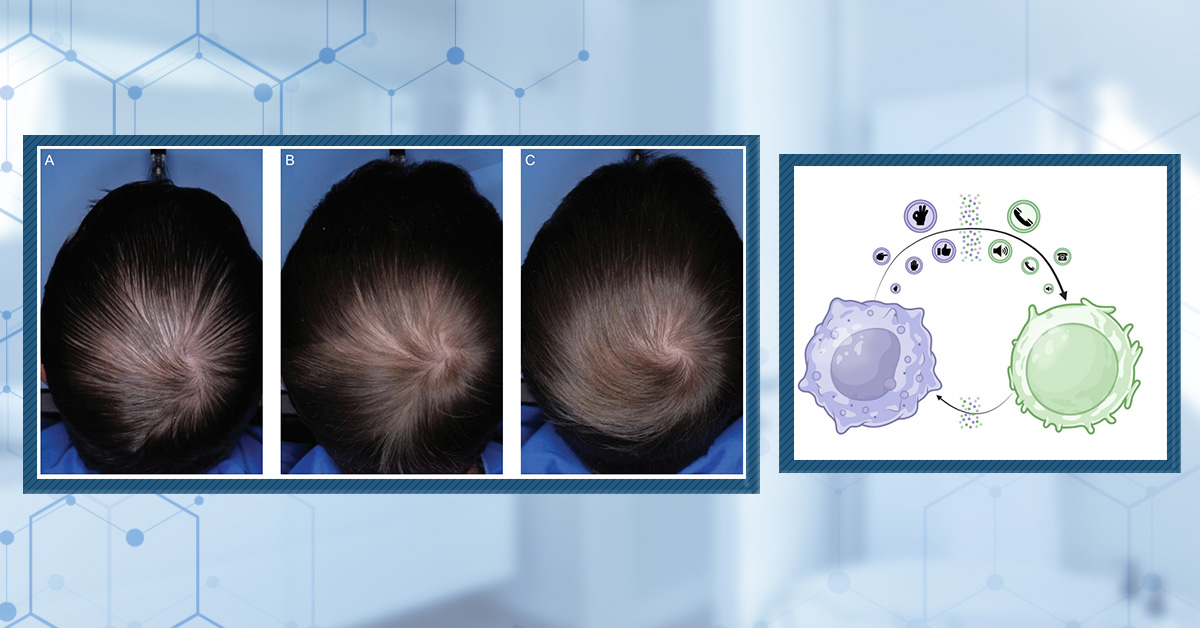
What is Platelet-Rich Plasma Therapy?
Platelet-rich plasma (PRP) therapy is increasingly recognized as an effective treatment for hair loss, particularly AGA. This procedure involves drawing a patient’s blood, processing it to concentrate platelets and growth factors, and injecting this enriched plasma into the scalp.
PRP therapy stimulates hair follicles, promotes new hair growth, and enhances hair density and thickness. The growth factors and proteins in PRP promote tissue repair and regeneration, making it a promising non-surgical option for hair loss. Clinical studies have also demonstrated the efficacy of PRP in improving hair count and thickness in individuals with hair loss.[3]Gentile, P., Garcovich, S., Bielli, A., Scioli, M.G., Orlandi, A., Cervelli, V. (2015). The Effect of Platelet-Rich Plasma in Hair Regrowth: A Randomized Placebo-Controlled Trial. Stem Cells … Continue reading,[4]Cervantes, J., Perper, M., Wong, L.L., Eber, A. E., Fricke, A.C.V., Wikramanayake, T.C., Jiminez, J.J. (2018). Effectiveness of Platelet-Rich Plasma for Androgenetic Alopecia: A Review of the … Continue reading
Microneedling vs. PRP: Which Is Better?
When hair loss patients visit dermatologists for advice, it’s not uncommon for those physicians to recommend autologous therapies. These hair loss therapies, such as platelet-rich plasma (PRP) therapy, PRP + Acell, adipose-derived stem cells, exosomes, and others, are derived from our tissues. These treatments must be conducted in a clinical setting and administered by a healthcare professional. While there is scientific evidence behind these therapies, it is also a significant cash cow for dermatologists, so it is no surprise that they recommend this treatment.
What these dermatologists won’t tell patients is that there is an alternative to PRP that:
- Can be administered at home
- Leverages the exact same mechanisms of action as PRP
- Costs just a fraction of the price (usually 0.1% of the cost of a single PRP session)
- Might be just as effective as PRP
That alternative is microneedling.
What Does the Clinical Evidence Say?
Two randomized, blinded, controlled clinical trials indicate that microneedling produces the same hair parameter improvements as PRP. Let’s take a closer look at these studies and determine if PRP has any benefits over microneedling.
Study 1 – Split Scalp Study Comparing Microneedling Alone to Microneedling with PRP
This one-year-long study included 30 male patients with varying degrees of androgenic alopecia. Each participant received treatments on different halves of their scalp – one half received microneedling only, and the other half of the scalp received microneedling and PRP together. The treatments were conducted over four months, with a follow-up evaluation three months after the final session. The effectiveness was measured using dermoscopic microphotographs and patient satisfaction scores.[5]Aggarwal K, Gupta S, Jangra RS, Mahendra A, Yadav A, Sharma A. Dermoscopic Assessment of Microneedling Alone versus Microneedling with Platelet-Rich Plasma in Cases of Male Pattern Alopecia: A … Continue reading
The Results
- Hair Thickness and Density: Both treatments significantly improved hair thickness and density. The microneedling-only group nearly doubled the increase in hair thickness compared to the microneedling and PRP groups, though the difference between the groups was not statistically significant (Figure 1).
- Patient Satisfaction: Most patients reported moderate satisfaction with the treatment outcomes, noting reduced hair loss but not necessarily new hair growth.
- Long-Term Effects: A follow-up revealed that some patients experienced a recurrence of hair loss, indicating the need for ongoing or maintenance treatments.

Figure 1: Average hair density before and after treatment for microneedling and microneedling + PRP treated groups. While there were significant improvements in both groups compared to before treatment, there was no significant difference between the two groups.[6]Aggarwal K, Gupta S, Jangra RS, Mahendra A, Yadav A, Sharma A. Dermoscopic Assessment of Microneedling Alone versus Microneedling with Platelet-Rich Plasma in Cases of Male Pattern Alopecia: A … Continue reading
The Conclusion
Both microneedling and PRP can effectively treat androgenic alopecia and improve hair parameters and patient satisfaction. However, adding PRP to microneedling did not show any significant additional benefits over microneedling alone.
Study 2 – PRP Compared to Saline Injection
Another study was conducted with 26 women with female pattern hair loss. The women were randomly assigned to receive either 10 mL of PRP or a normal saline placebo. The study’s primary endpoints were hair count and hair mass index (HMI), measured at baseline and after 26 weeks. Additionally, a patient survey was conducted to gauge personal perceptions of treatment effectiveness.[7]Puig CJ, Reese R, Peters M. Double-Blind, Placebo-Controlled Pilot Study on the Use of Platelet-Rich Plasma in Women With Female Androgenetic Alopecia. Dermatol Surg. 2016 Nov;42(11):1243-1247. Doi: … Continue reading
The Results
- Hair Count and Mass: There was no statistically significant difference between the PRP and placebo groups regarding hair count and HMI after 26 weeks. This suggests that the needle insertion and the subsequent acute inflammation may be the reason for the improvement in hair growth, rather than the injection and the PRP (spoiler alert, you can get the same effect from just microneedling).
- Patient Survey: A small percentage (13.3%) of the treatment group reported substantial improvement in aspects like hair loss rate, hair thickness, and ease of hair management compared to the placebo group. However, these subjective improvements did not align with the objective measurements of hair count and HMI.
The Conclusion
This study, despite being well-designed, did not demonstrate a significant advantage of PRP over placebo in treating female androgenetic alopecia. The findings suggest that further research is needed to fully understand the role of PRP in hair loss treatment, including the possible contribution of the injection process beyond the growth factors in PRP.
So, it’s not looking great for PRP compared to microneedling. But are there any other redeeming qualities?
What About the Cost?
We know that PRP can improve hair loss outcomes, but it does not appear to be any more effective than microneedling. So does the cost make it more appealing?
No.
PRP is several times more expensive than microneedling. Let’s break it down a bit.
Microneedling Cost-Benefit
Let’s start with the costs:
- Initial investment: A microneedling device (roller or pen) can range from $10 – $200 for at-home devices.
- Replacement costs: Needles or cartridges, if applicable.
- Maintenance: Limited to cleaning and sterilizing the device.
Now, let’s see the benefits:
- Effectiveness: Proven to improve hair thickness and density in several studies.
- Convenience: This can be done at home.
- One-time cost: Mostly just the initial investment; very low ongoing costs.
Platelet-Rich Plasma Cost-Benefit
Costs:
- Per Session Cost: Each PRP session can range from $400 – $1300, depending on material quality and where you go.
- Annual cost: $1500 – $10,000 (assuming 3-4 sessions)
- Frequency: Initially, multiple sessions are needed, often 3-4 per year
- Maintenance: Every 6 – 12 months after the initial treatment to maintain hair regrowth.
Benefits:
- Effectiveness: Clinical studies show that it can stimulate hair growth and increase hair density (though microneedling can produce the same results).
- Professional Supervision: Performed by medical professionals, offering expertise and safety.
Based on the above information, it’s safe to say that you get more for your money with microneedling, given its effectiveness and significantly lower costs.
What About the Convenience / Ease of Use?
Several key differences become apparent when comparing the convenience and ease of use between microneedling and PRP.
Microneedling
Microneedling is notably convenient, especially with at-home devices. It allows individuals to perform the treatment at their own pace and in the comfort of their own homes, eliminating the need for frequent clinic visits. Furthermore, these devices are relatively straightforward to use. After an initial learning curve, users can quickly integrate the treatment into their routine. These sessions can also be relatively quick, often taking less than 10 minutes, and can be easily scheduled around personal routines and commitments.
If you want to learn more about integrating microneedling into your routine, look at our Ultimate Guide here.
Platelet-Rich Plasma
PRP therapy, on the other hand, is less convenient compared to microneedling due to the necessity of visiting a clinic or a healthcare provider for each session. This requires scheduling appointments, possibly taking time off work, and traveling to the clinic.
It is also not a self-administered treatment. It requires a skilled medical professional to draw the blood, process it to concentrate the platelets and inject it into the scalp. The process is more complex and clinical compared to miconeedling. Moreover, each PRP session, including preparation and treatment, takes longer than a typical microneedling session (treatment alone can take ~1 hour!), and the need to schedule and attend clinic appointments adds to the time commitment.
Overview Comparing Microneedling and PRP Therapy
Take a look at this overview table that we’ve created to get a quick comparison between the two treatments.
Criteria Microneedling PRP Therapy Effectiveness Similar improvements in hair count and thickness in comparative studies. Cost per Session Relatively low; cost primarily involves the purchasing of a microneedling device. This can range from less than $10 for a derma roller to ~$80+ for a derma pen.
If you want an aesthetician to do it for you, it can cost $50 – $150 per session.Higher. It involves the cost of blood draws, processing, and injections per session. The cost of just one injection can range anywhere from $400 – $1300, depending on the materials’ quality and where you go for treatment. Total Cost for Treatment There is a one-time cost for the device, which can be reused multiple times. Treatments (3-4 rounds) could cost $1500 – $10,000. Session Frequency It can vary; typically, once a week to once every few weeks. Every 4-6 weeks for the first 3-4 months, then maintenance treatments every 6- 12 months. Ease-of-Use/Convenience You can perform it at home but must learn the proper technique. A healthcare professional must perform it in a clinical setting. Recovery Time/Side Effects Minimal; may include temporary redness or irritation. Minimal; may include scalp tenderness, swelling, or mild pain at the injection sites. Longevity of Results Long-term consistent use is required for sustained results – however, some benefits may be retained even after the stoppage of treatment. Periodic maintenance sessions are needed for sustained results. In addition to saving time and money (which can amount to tens of thousands of dollars), it’s important to be cautious when following a dermatologist’s recommendation for PRP or any other autologous hair growth therapy. Instead, when weighing the options between microneedling and PRP, it may be wise to consider the benefits of microneedling.
References[+]
References ↑1 Dhurat, R., Sukesh, M.S., Avhad, G., Dandale, A., Pal, A., Pund, P. (2013). A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study. International Journal of Trichology. 5(1). 6-11. Available at: https://doi.org/10.4103/0974-7753.114700 ↑2 English, R.S., Ruiz, S., DoAmaral, P. (2021). Microneedling and Its Use in Hair Loss Disorders: A Systematic Review. Dermatology and Therapy. 12. 41-60. Available at: https://doi.org/10.1007/s13555-021-00653-2 ↑3 Gentile, P., Garcovich, S., Bielli, A., Scioli, M.G., Orlandi, A., Cervelli, V. (2015). The Effect of Platelet-Rich Plasma in Hair Regrowth: A Randomized Placebo-Controlled Trial. Stem Cells Translational Medicine. 4(11). 131-1323. Available at: https://doi.org/10.5966/sctm.2015-0107 ↑4 Cervantes, J., Perper, M., Wong, L.L., Eber, A. E., Fricke, A.C.V., Wikramanayake, T.C., Jiminez, J.J. (2018). Effectiveness of Platelet-Rich Plasma for Androgenetic Alopecia: A Review of the Literature. Skin Appendage Disorders. 4. 1-11. Available at: https://doi.org/10.1159/000477671 ↑5, ↑6 Aggarwal K, Gupta S, Jangra RS, Mahendra A, Yadav A, Sharma A. Dermoscopic Assessment of Microneedling Alone versus Microneedling with Platelet-Rich Plasma in Cases of Male Pattern Alopecia: A Split-Head Comparative Study. Int J Trichology. 2020 Jul-Aug;12(4):156-163. doi: 10.4103/ijt.ijt_64_20. Epub 2020 Sep 19. PMID: 33376284; PMCID: PMC7759059. ↑7 Puig CJ, Reese R, Peters M. Double-Blind, Placebo-Controlled Pilot Study on the Use of Platelet-Rich Plasma in Women With Female Androgenetic Alopecia. Dermatol Surg. 2016 Nov;42(11):1243-1247. Doi: 10.1097/DSS.0000000000000883 Whether microneedling is done by a dermatologist or at home, how deep do the punctures need to be for the best results? Is bleeding when microneedling necessary, or is it a sign that it’s being done incorrectly? This guide explores how needle depth affects the efficacy of microneedling and whether bleeding needs to be involved in achieving the best results.
What is Microneedling?
Microneedling, a minimally invasive cosmetic procedure, has gained recognition for its potential to enhance outcomes in individuals with androgenic alopecia (AGA). This approach involves specialized devices equipped with fine, tiny needles that create controlled micro-injuries on the scalp’s surface. While intentionally inducing micro-injuries may seem counterintuitive, it triggers the body’s natural wound-healing response, fostering numerous processes that benefit individuals with AGA.
Microneedling can be conducted either in a clinical setting or at home. Various devices are available for this purpose, including needling stamps, manual rollers, and automated pens. Some of these devices may incorporate fractional radiofrequency technology. Regardless of the specific device used and the needling depth, microneedling has proven effective in clinical settings as both a primary treatment and a complementary therapy.
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What Evidence Supports the Use of Microneedling?
Clinical studies have demonstrated that microneedling can increase hair density, thickness, and count in individuals with AGA. A landmark study was conducted by Rachita Dhurat in 2013 on 100 subjects with AGA, using a 1.5 mm derma roller. The researchers found that over 12 weeks, once weekly microneedling combined with twice daily 5% minoxidil significantly increased hair counts compared to minoxidil treatment alone (Figure 1).[1]Dhurat, R., Sukesh, M.S., Avhad, G., Dandale, A., Pal, A., Pund, P. (2013). A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study. International … Continue reading

Figure 1: Microneedling plus 5% minoxidil for AGA: results over three months (weekly sessions).[2]Dhurat R., Sukesh, M.S., Avhad, G., Dandale, A., Pal, A., Pund, P. (2013). A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study. International … Continue reading
Further research has continued to investigate the mechanism of action of microneedling on hair growth, as well as its effects on hair regrowth.
We have covered many of these studies (and more) in our systematic review on the subject (which was published in Dermatology and Therapy in 2021).[3]English Jr, R.S., Ruiz, S., DoAmarel, P. (2022). Microneedling and its use in hair loss disorders: A systematic review. Dermatology and Therapy. 12. 41-60. Available at: … Continue reading
How Does Microneedling Improve Hair Growth?
Microneedling is not just a superficial treatment; it has the ability to enhance hair growth by stimulating biological responses within the skin’s layers. This process involves the stimulation of the scalp at different depths, which activates a cascade of healing and rejuvenating mechanisms that are crucial for promoting healthier and thicker hair. Microneedling may contribute to hair regrowth by enhancing the effectiveness of topical treatments and stimulating the body’s natural healing processes. Let’s explore in more detail how microneedling can help with hair regrowth.
Enhances Drug Penetration
At shorter needle lengths (0.25 mm to 5 mm), microneedling can enhance the absorption and penetration of topical hair growth products such as minoxidil. By creating microchannels in the scalp, microneedling facilitates the delivery of these products to hair follicles, potentially maximizing their effectiveness. However, these needle lengths likely won’t evoke the growth factors necessary to encourage hair follicle proliferation.
Induces Growth Factor and Protein Secretion
At longer needle depths (1.5 mm to 2.5 mm), microneedling punctures the vascular networks in the dermis, which induces the release of growth factors and proteins. The body perceives these micro-injuries as wounds and activates an acute inflammatory response. Inflammation is a natural defense mechanism that recruits various cells and molecules to the injured site.
As part of this inflammatory wound-healing process, platelets in the blood release growth factors such as platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), and fibroblast growth factor (FGF). These growth factors are crucial in signaling nearby cells, including fibroblasts and keratinocytes. They stimulate these cells to migrate to the wounded area and begin tissue repair.
Fibroblasts in the scalp’s dermal layer (more on this below) respond to these growth factors by producing collagen and other proteins. Collagen is essential for the structural support of tissues, and it contributes to the overall health and strength of hair follicles.
Stimulates Bulge Stem Cells
Another aspect of the wound healing response is the activation of bulge stem cells. The bulge is a region located in the outer root sheath of the hair follicle, just below the sebaceous gland (Figure 2). It’s recognized as a niche for adult stem cells, essential for the regeneration and growth of hair follicles. These bulge stem cells can give rise to the various cell types that form the hair shaft and its surrounding structures. Activation of these cells is important for hair cycle progression and repair after injury.

Figure 2: Hair follicle structure and location of the bulge.[4]Pantaleyev, A.A., Jahoda, C.A.B., Christiano, A.M. (2001). Hair follicle predetermination. Journal of Cell Science. 114. 3419-3431. Available at: https://doi.org/10.1242/jcs.114.19.3419
(May) Promote Angiogenesis
Another suspected mechanism of microneedling is tissue remodeling, particularly in the form of angiogenesis: the formation of new blood vessel networks. The micro-injuries sustained during microneedling might stimulate increased blood circulation to the treated area, along with growth factors which, over a number of repeated sessions, might help grow new blood vessels in the microvascular networks supporting thinning hair follicles.. This increase in blood flow might deliver more essential nutrients and oxygen to hair follicles, which might improve their growth.
Note: microneedling-induced angiogenesis has been demonstrated in mouse models. However, it has not (yet) been demonstrated in human scalps – because the studies haven’t yet been conducted.[5]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5064188/ It’s suspected that repeated microneedling would also promote angiogenesis in human scalps. However, confirming this would require invasive and repeated biopsies from humans pre- and post-microneedling, which acts as a deterrent for human study. As more research is published, we’ll update this article.
(May) Reduce Scalp Fibrosis
Another suspected effect from microneedling is the potential reduction of scalp fibrosis or scarring, a common feature in individuals with AGA. Scalp fibrosis can hinder hair follicle function and might even drive aspects of hair follicle miniaturization. Microneedling has shown promise in breaking down scar tissue (for example, in acne patients). It’s not unreasonable to assume a similar histological effect might also occur in the scalp, and potentially promote a healthier scalp environment for hair growth. As is the case with angiogenesis, as research develops, we’ll update this article.
How is Microneedling Applied?
Microneedling is generally done with hundreds of tiny, medical-grade needles ranging from 0.1mm to 5.0mm, determining how far into the skin the needles penetrate.
A derma roller for at-home microneedling.
The skin comprises three main layers: the epidermis, dermis, and hypodermis (Figure 3).

Figure 3: The layers of the skin.[6]Yousef, H., Alhajj, M., Sharma, S. (2022). Anatomy, Skin (Integument), Epidermis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Available from: … Continue reading
Epidermis
The epidermis is the outermost layer of skin, and its thickness can vary from 0.04-0.4 mm in different body areas to serve various functions.[7]Skandalakis, L.J. (2009). Skin, Scalp, and Nail. In: Surgical Anatomy and Technique. Springer, New York, NY. Available at: https://doi.org/10.1007/978-0-387-09515-8_1 On the scalp, the epidermis plays a role in protecting the underlying tissues and structures, including the hair follicles; however, it is usually avascular (meaning that it doesn’t have any blood vessels running through it). The epidermis gets its nutrients and disposes of waste products via diffusion from/to the underlying dermis.[8]Kim, J.Y., Dao, H. (2023). Physiology, Integument. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Available at: https://www.ncbi.nlm.nih.gov/books/NBK554386/ (Accessed: 6 … Continue reading
Dermis
The dermis is the layer of skin located just beneath the epidermis on the scalp. It plays a crucial role in supporting hair growth and overall scalp health.
The primary functions of the scalp dermis include:
- housing hair follicles
- providing nourishment to the hair bulb through blood vessels
- anchoring hair follicles to the underlying structures
The scalp dermis is also responsible for regulating temperature and protecting the hair follicles. In terms of thickness, the dermis is the thickest and can range from 1.5 – 4 mm deep.[9]National Cancer Institute (no date). Layers of the Skin. National Cancer Institute. Available at: https://training.seer.cancer.gov/melanoma/anatomy/layers.html (Accessed: 6 November 2023)
Hypodermis
The scalp hypodermis, or subcutaneous layer, is the deepest layer of the scalp skin. Its role is primarily related to insulation, energy storage, and providing cushioning and protection for the underlying structures, such as the skull and blood vessels. The hypodermis is rich in fat cells, blood vessels, and connective tissue. This layer helps regulate temperature, acts as an insulator, and stores fat as an energy reserve. The thickness of the scalp hypodermis can vary from person to person, but it’s typically a few millimeters deep. Maintaining a healthy scalp hypodermis is crucial for overall scalp function and protection.
Do I Need to Bleed for Microneedling To Work?
The short answer is no; bleeding is not a requirement for effective microneedling. However, pinpoint bleeding from microneedling is not necessarily detrimental, and it can just be wiped away.
Excessive bleeding, however, can be an indication that the needles are penetrating too deeply, which may increase the risk of side effects and is not necessary for the therapeutic benefits of the procedure. Emissary veins are vessels that connect the hypodermis of the scalp to the brain through the skull, functioning in both directions.[10]Klein, B.M., Bordoni, B. (2023). Anatomy, Head and Neck, Emissary Veins. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Available at: … Continue reading Infections in the brain stemming from scalp injuries often result from these veins being compromised, allowing bacteria from the skin to enter the brain, potentially leading to severe consequences or even death.
These veins are not uniformly distributed across the scalp and are typically found deeper than 5 mm, near the lower regions of the hypodermis. There’s no need to risk damaging these veins with microneedling since activating the hair follicle’s stem cell bulge is possible at shallower depths, specifically between 1.5 mm and 2.5 mm.
The existing research on microneedling for hair loss does not involve needles longer than 2.5 mm, so it is advisable to stick within these clinically supported depths and avoid going deeper.
Microneedling: What Depth Of Punctures Will Cause Bleeding?
As mentioned above, our skin is segmented by three primary layers: the epidermis, dermis, and hypodermis. The epidermis is the outermost layer of skin and is relatively avascular (without microcapillary networks). The epidermis of scalp skin is estimated to be 0.4mm deep. So, most wounds at this depth and shallower do not bleed. However, you may not get the full beneficial effect from microneedling at this depth. It is only after this depth that punctures from microneedling might evoke erythema, swelling, or pinpoint bleeding.
What’s the Best Needle Depth?
While penetrating the epidermis may be beneficial for increasing drug penetration, it is avascular. Therefore, to produce an appreciable inflammatory response in scalp skin, penetration past the epidermis is necessary. But how far should we go? Well, not much further, according to one study.
Which Needle Length Is Better: 0.6 mm or 1.2 mm?
One study compared two depths of microneedling, 0.6 mm and 1.2 mm, in 60 participants aged 18-45 with mild-to-moderate alopecia. The participants were divided into three groups. One group was treated with only 5% minoxidil lotion, the second group (group A) received minoxidil plus biweekly microneedling at a depth of 1.2 mm and the third group (group B) received minoxidil plus biweekly microneedling at a depth of 0.6 mm over 12 weeks.[11]Faghihi, G., Nabavinejad, S., Mokhtari, F., Naeini, F.F., Iraji, F. (2020). Microneedling in androgenetic alopecia; comparing two different depths of microneedles. Journal of Cosmetic Dermatology. … Continue reading
Results
Both hair count and thickness significantly increased in all groups compared to the baseline, with group B showing a substantially more significant increase in hair count and thickness than the control group (Figure 4). Additionally, hair regrowth evaluated by investigators was significantly higher in both microneedling groups compared to the minoxidil group, with group B (0.6 mm depth) tending to show more benefit than group A (1.2 mm depth). This improvement was not statistically significant, however, and the 1.2 needle improved hair counts by about 15%, and the 0.6 mm needle improved hair counts by about 19%.

Figure 4: The effect of needle depth on mean hair count (white bar) and thickness (black bar).[12]Faghihi, G., Nabavinejad, S., Mokhtari, F., Naeini, F.F., Iraji, F. (2020). Microneedling in androgenetic alopecia; comparing two different depths of microneedles. Journal of Cosmetic Dermatology. … Continue reading
So, we can see that the 0.6 mm needle length was superior at improving hair counts and thickness, but what other benefits might we see from using the shorter needle length?
Other Benefits
Reduced Pain: According to the study, participants in group A (1.2 mm depth) reported more severe pain than the other groups. Therefore, using a shorter needle may reduce the pain associated with microneedling.
Less Trauma to Hair Follicles: It was speculated in the study that the deeper penetration of needles from group A might have caused some trauma to the hair bulge, thus decreasing its efficacy, indicating that shorter needle length may be more beneficial for overall hair follicle health.
Faster Wound Healing: Because the 0.6 mm needle depth does not penetrate as far, it is likely that wound healing will be faster (although this wasn’t examined in this study).
Other Studies
Interestingly, other studies have suggested that using a derma roller with 1.5 mm-sized needles also might improve hair growth for those with androgenic alopecia.[13]Jha, A.K., Udayan, U.K., Roy, P.K., Amar, A.K.J., Chaudhary, R.K.P. (2018). Original article: Platelet-rich plasma with microneedling in androgenetic alopecia along with dermoscopic pre-and … Continue reading,[14]Dhurat, R., Sukesh, M.S., Avhad, G., Dandale, A., Pal, A., Pund, P. (2013). A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study. International … Continue reading
Furthermore, needle penetration studies show that with microneedling automated pens, needling depths matched penetration depths up to 1.5 mm (meaning that the needle will penetrate to the exact depth).[15]Sasaki GH. (2017). Micro-needling depth penetration, presence of pigment particles, and fluorescein stained platelets: clinical usage for aesthetic concerns. Aesthetic Surgery Journal. 37(1):71–83. … Continue reading
However, when it comes to manual rollers, it’s estimated that due to pressure variability and angle of needle entry, microneedling rollers may only penetrate to skin depths of 50-70% of its needle length.[16]de Andrade Lima, E.V., de Andrade Lima, M. (2013). Microneedling experimental study and classification of the resulting injury. Surgical and Cosmetic Dermatology. 5(2). 110-114.
Therefore, to achieve an optimal depth of around 0.6 – 0.8 mm (based on the available clinical data), an automated pen set to 0.6 -0.8 mm or a manual roller set to 1.00 – 1.5 mm (to account for the loss of penetration) may be the most beneficial.[17]English Jr, R.S., Ruiz, S., DoAmarel, P. (2022). Microneedling and its use in hair loss disorders: A systematic review. Dermatology and Therapy. 12. 41-60. Available at: … Continue reading
Does Bleeding From Microneedling Improve Hair Growth Outcomes?
When looking at the methodologies across microneedling studies, we can see that investigation groups used various methods to denote the endpoint of any microneedling session.[18]English Jr, R.S., Ruiz, S., DoAmarel, P. (2022). Microneedling and its use in hair loss disorders: A systematic review. Dermatology and Therapy. 12. 41-60. Available at: … Continue reading Aside from using different microneedling devices and needle lengths, research groups also tended to vary their session endpoints based on:
- A set number of roller passes in any given area.
- Any number of passes horizontally, vertically, and diagonally until mild erythema (pink skin) occurred
- A set time limit (from just a few minutes to 45 minutes)
- The arrival of pinpoint bleeding
Despite the various methodologies across studies, microneedling led to similar ballpark hair parameter improvements. For these reasons, it’s unclear if pushing harder when microneedling or generating more acute inflammation via pinpoint bleeding induces better outcomes.
Based on the data available, there is nothing to suggest that bleeding when microneedling is necessary and worth the additional pain.
What If I’m Combining Microneedling With Topicals?
Microneedling’s mechanisms of action may change depending on the needle penetration depth.
- At shallower depths (0.5mm and lower), microneedling punctures the scalp’s epidermis. This can significantly enhance the efficacy of minoxidil by increasing both (1) dermal absorption of the drug and (2) sulfotransferase activity. Sulfotransferase is the enzyme required to activate minoxidil.
- At deeper depths (0.5mm-2.0mm), microneedling punctures into the dermis and evokes a stronger acute inflammatory reaction. This can induce growth factors, signaling proteins, and hormones linked to the anagen (growth) stage of the hair cycle.
If using microneedling alongside minoxidil, it’s possible to still benefit from microneedling with shorter needle lengths. Shorter needle lengths still produce the benefits of microneedling via enhancement of topical absorption and activation. Shallow microneedling will also minimize the pain associated with a microneedling session and help avoid bleeding.
So, no, it is not a requirement to bleed when microneedling to get the best results. But if bleeding occurs? Just wipe the blood away with an alcohol swab.
References[+]
References ↑1, ↑14 Dhurat, R., Sukesh, M.S., Avhad, G., Dandale, A., Pal, A., Pund, P. (2013). A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study. International Journal of Trichology. (5)1. 6-11. Available at: https://doi.org/10.4103/0974-7753.114700 ↑2 Dhurat R., Sukesh, M.S., Avhad, G., Dandale, A., Pal, A., Pund, P. (2013). A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study. International Journal of Trichology. 5(1). 6-11. Available at: https://10.4103/0974-7753.114700 ↑3, ↑17, ↑18 English Jr, R.S., Ruiz, S., DoAmarel, P. (2022). Microneedling and its use in hair loss disorders: A systematic review. Dermatology and Therapy. 12. 41-60. Available at: https://doi.org/10.1007/s13555-021-00653-2 ↑4 Pantaleyev, A.A., Jahoda, C.A.B., Christiano, A.M. (2001). Hair follicle predetermination. Journal of Cell Science. 114. 3419-3431. Available at: https://doi.org/10.1242/jcs.114.19.3419 ↑5 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5064188/ ↑6 Yousef, H., Alhajj, M., Sharma, S. (2022). Anatomy, Skin (Integument), Epidermis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Available from: https://www.ncbi.nlm.nih.gov/books/NBK470464/ (Accessed: 7 November 2023) ↑7 Skandalakis, L.J. (2009). Skin, Scalp, and Nail. In: Surgical Anatomy and Technique. Springer, New York, NY. Available at: https://doi.org/10.1007/978-0-387-09515-8_1 ↑8 Kim, J.Y., Dao, H. (2023). Physiology, Integument. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Available at: https://www.ncbi.nlm.nih.gov/books/NBK554386/ (Accessed: 6 November 2023) ↑9 National Cancer Institute (no date). Layers of the Skin. National Cancer Institute. Available at: https://training.seer.cancer.gov/melanoma/anatomy/layers.html (Accessed: 6 November 2023) ↑10 Klein, B.M., Bordoni, B. (2023). Anatomy, Head and Neck, Emissary Veins. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Available at: https://www.ncbi.nlm.nih.gov/books/NBK563196/ (Accessed: 7 November 2023) ↑11, ↑12 Faghihi, G., Nabavinejad, S., Mokhtari, F., Naeini, F.F., Iraji, F. (2020). Microneedling in androgenetic alopecia; comparing two different depths of microneedles. Journal of Cosmetic Dermatology. 20. 1241-1247. Available at: https://doi.org/10.1111/jocd.13714 ↑13 Jha, A.K., Udayan, U.K., Roy, P.K., Amar, A.K.J., Chaudhary, R.K.P. (2018). Original article: Platelet-rich plasma with microneedling in androgenetic alopecia along with dermoscopic pre-and post-treatment evaluation. Journal of Cosmetic Dermatology. 17(3). 313-318. Available at: https://doi.org/10.1111/jocd.12394. ↑15 Sasaki GH. (2017). Micro-needling depth penetration, presence of pigment particles, and fluorescein stained platelets: clinical usage for aesthetic concerns. Aesthetic Surgery Journal. 37(1):71–83. Available at: https://doi.org/10.1093/asj/sjw120 ↑16 de Andrade Lima, E.V., de Andrade Lima, M. (2013). Microneedling experimental study and classification of the resulting injury. Surgical and Cosmetic Dermatology. 5(2). 110-114. CB-03-01, also known as Breezula™ or clascoterone, is a topical medication generating interest as a potential therapy for androgenetic alopecia (AGA). It was developed by Cassiopea (now owned by Cosmo Pharmaceuticals) and is a synthetic androgen receptor antagonist. While it is primarily recognized for its potential in combating hair loss, particularly AGA, CB-03-01 has also exhibited efficacy in treating conditions like acne, hirsutism, polycystic ovary syndrome (PCOS), and seborrheic dermatitis. In this overview, we look at whether CB-03-01 can impact hair follicles and its potential in treating hair loss, and we will also look at CB-03-01’s safety profile and mechanism of action, drawing from clinical trials and research findings.
Key Takeaways
- Drug. CB-03-01, also known as Breezula™ or clascoterone, is a topical synthetic androgen receptor antagonist developed by Cassiopea (now owned by Cosmo Pharmaceuticals). It competes with natural androgens like dihydrotestosterone (DHT) for binding to androgen receptors, making it a promising treatment for hair loss that may be caused by androgen signaling, particularly androgenetic alopecia.
- Clinical Data. Three Phase II trials for CB-03-01 have been conducted – two for male and one for female AGA – the results of one of these trials were not published. The published studies are summarized below:
- Study 1: A study involving 293 women aged 18-55 with AGA. Of various treatments used, a 5% formulation of CB-03-01 was the only treatment that significantly improved, and only in women under 30.[1]Cassiopea Spa, (2021). Cassiopea SpA Announces Topline Results of Phase II Proof of Concept Trial of Clascoterone Solution for the Treatment of Androgenetic Alopecia in Females. Bloomberg. Available … Continue reading
- Study 2: A study involving 400 men aged 18-55 with mild to moderate AGA. A 7.5% concentration of CB-03-01 led to statistically significant improvements in hair length and width in the treated area. All treatment groups showed relative improvement compared to the control.[2]Cassiopea Spa, (2021). Cassiopea Announces Very Positive Phase II Twelve Months Results for Breezula® (Clascoterone) in Treating Androgenetic Alopecia Bloomberg. Available at: … Continue reading
- Phase III trials of CB-03-01 are expected to be completed in January 2025.
- Safety. CB-03-01 has reportedly demonstrated minimal side effects, with common issues being mild skin reactions such as scaling, redness, and itching. However, there is too little published data to make a definitive statement regarding the safety of CB-03-01.
- Evidence Quality. CB-03-01 scored 36/100 for evidence quality by our metrics.
- Best Practices. This product is not currently available at a 5% concentration for treatment of AGA. However, when available, this may be most effective when used twice daily by women with AGA under 30, based on the available data.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is CB-03-01?
CB-03-01, known by its brand name Breezula™ or clascoterone, is a topical synthetic androgen receptor antagonist owned by Cosmo Pharmaceuticals.[3]Cosmo, (no date). Breezula. Cosmo Pharmaceuticals Available at: https://www.cosmopharma.com/pipeline/breezula (Accessed: 17 October 2023) An androgen receptor antagonist is a substance that can interfere with or block androgen hormones from working as they normally would.[4]Kokal, M., Mirzakhani, K., Pungsrinont, T., Baniahmad, A. (2020). Mechanisms of Androgen Receptor Agonist- and Antagonist-Mediated Cellular Senescence in Prostate Cancer. Cancers (Basel). 12(7). … Continue reading CB-03-01 is a competitive antagonist, meaning it competes with natural androgen hormones in our bodies, such as dihydrotestosterone (DHT), for binding to the androgen receptor. CB-03-01 is primarily recognized for its potential in treating hair loss, particularly androgenetic alopecia. However, it has also been used to treat acne (under the brand name Winlevi), hirsutism (excess/unwanted facial hair in women), polycystic ovary syndrome (PCOS), and seborrheic dermatitis (Figure 1).

Figure 1: Chemical structure of CB-03-01.[5]Drugbank Online (no date), Clascoterone. Drugbank Online. Available at: https://go.drugbank.com/drugs/DB12499 (Accessed: 16 October 2023)
How Does CB-03-01 Work?
The mechanism of action of CB-03-01 (clascoterone) involves its interaction with androgen receptors in the skin, particularly in hair follicles and sebaceous glands. This compound is a selective androgen receptor antagonist with a specific affinity for androgen receptors.[6]Cosmo, (no date). Breezula. Cosmo Pharmaceuticals Available at: https://www.cosmopharma.com/pipeline/breezula (Accessed: 17 October 2023) Androgens are a group of hormones that include testosterone and dihydrotestosterone (DHT), which play a role in the development and growth of hair, but which can also contribute to conditions like androgenetic alopecia (AGA, also known as male pattern hair loss) and acne when androgen hormone activity becomes abnormal or excessive.[7]Handelsman, D.J. (2020). Androgen Physiology, Pharmacology, Use and Misuse. Endotext [Internet]. South Dartmouth (MA). Available at: https://www.ncbi.nlm.nih.gov/books/NBK279000/ (Accessed: 17 … Continue reading
Androgens like DHT normally activate androgen receptors to mediate their biological effects. CB-03-01 interferes with the ability of androgens to activate these receptors. In the context of hair loss, reducing androgen signaling can help slow down the miniaturization of hair follicles associated with androgenetic alopecia. By reducing the impact of androgens on hair follicles, CB-03-01 may help prevent hair follicle miniaturization and hair loss.
What is the Impact of CB-03-01 on Hair Follicle Biology?
There is one in vitro (or ‘test tube’) study that we could find that looks at how CB-03-01 could affect hair follicle biology. The study looked at dermal papilla cells (DPCs), which can be thought of as the hair follicle’s signaling center and which are negatively affected by testosterone in patients with AGA. DPCs from balding scalps grow slower than those of healthy scalps. They undergo a process called premature senescence, in which cells lose their ability to divide and grow.[8]Bahta, A.W., Farjo, N., Farjo, B., Philpott, M. Premature senescence of balding dermal papilla cells in vitro is associated with p16(INK4a) expression. Journal of Investigative Dermatology. 218(5). … Continue reading
Firstly, the researchers wanted to show that CB-03-01 could, in principle, interfere with androgen receptor signaling. They used an experimental tool called androgen receptor reporter cells, which are commonly used to study the activity of androgen receptors. These cells were treated with 0.4 nM testosterone in the presence or absence of CB-03-01 or finasteride. The IC50 value – the drug concentration required to give half the maximal response – was then calculated. CB-03-01 (called clascoterone here) had an IC50 of 1.55×10-6M, compared to 2.89×10-6 M for finasteride. As a lower IC50 value indicates that a drug is more effective, the results show that clascoterone is at least as potent as finasteride in inhibiting testosterone-induced androgen receptor activity; their IC50 values are in the same order of magnitude (Figure 2).[9]Rosetter, C., Rosette, N., Mazzetti, A., Moro, L., Gerloni, M. Cortexolone 17ɑ-Proprionate (Clascoterone) is an Androgen Receptor Antagonist in Dermal Papilla Cells in Vitro. Journal of Drugs in … Continue reading

Figure 2: CB-03-01 (clascoterone) and finasteride have similar potency as inhibitors of testosterone-induced androgen receptor activity.[10]Rosetter, C., Rosette, N., Mazzetti, A., Moro, L., Gerloni, M. Cortexolone 17ɑ-Proprionate (Clascoterone) is an Androgen Receptor Antagonist in Dermal Papilla Cells in Vitro. Journal of Drugs in … Continue reading
The researchers then treated reporter cells with 200 μM DHT with or without finasteride or CB-03-01 under three conditions (Figure 3).- Treated with DHT plus androgen receptor inhibitor (finasteride of CB-03-01) for 24 hours (to mimic once-daily application)
- Treated with DHT plus androgen receptor inhibitor for 12 hours, then washed off and treated with DHT alone for a further 12 hours (to mimic once daily application and examine the metabolism of the drug)
- Treated with DHT plus androgen receptor inhibitor for 12 hours, then washed off and treated with DHT plus androgen receptor inhibitor for a further 12 hours (to mimic twice-daily application)
In conditions 1 and 3, where CB-03-01 was continuously present, AR activity was significantly inhibited. This suggests that continuous exposure to the inhibitor effectively blocks androgen receptor activity. In condition 2, where CB-03-01 was removed after 12 hours, and the cells were exposed to DHT alone, the inhibitor’s effectiveness significantly decreased. The drug’s IC50 was much higher in this case. This indicates a need for a continuous presence of the inhibitor for sustained antagonism of DHT-induced AR activity. The study also found finasteride was more effective when present for 24 hours than 12 hours (Figure 3), and CB-03-01 seemed to be as effective as finasteride at a similar concentration.

Figure 3: Continuous presence of CB-03-01 (clascoterone) is required for sustained androgen receptor antagonism.[11]Rosetter, C., Rosette, N., Mazzetti, A., Moro, L., Gerloni, M. Cortexolone 17ɑ-Proprionate (Clascoterone) is an Androgen Receptor Antagonist in Dermal Papilla Cells in Vitro. Journal of Drugs in … Continue reading
DPCs were treated with 200 μM DHT or vehicle control (0.1% DMSO) for 24 hours. The researchers found that exposure to high levels of DHT increased the expression of the androgen receptor in healthy dermal papilla cells. This mimicked the conditions found in the balding scalp, where DHT sensitivity contributes to hair loss. Additionally, the experiment revealed that exposure to high levels of DHT significantly increased the secretion of two cytokines: Interleukin-6 (IL-6) and basic fibroblast growth factor (bFGF) by DPCs (Figure 4A & B).
The researchers then investigated whether clascoterone (CB-03-01) could antagonize the synthesis and secretion of these cytokines. They used enzalutamide as a positive control because it also acts as an androgen receptor antagonist, competing with DHT for binding to the androgen receptor. However, it would have been more useful to compare to finasteride, which is commonly used to treat AGA.
Clascoterone was found to be more effective at reducing the secretion of IL-6 compared to enzalutamide. The IC50 (the concentration at which it inhibits 50% of IL-6 secretion) for clascoterone was much lower than that of enzalutamide, indicating that clascoterone more effectively reduced the secretion of this inflammatory cytokine (Figure 4B). However, neither of the drugs had any effect on bFGF (Figure 4C).
The researchers finally performed cell viability assays to ensure the results were not due to cell death – this is important because cell viability changes could affect cytokine secretion. These assays showed that neither clascoterone nor enzalutamide significantly affected cell viability, indicating that the results were not an artifact caused by variations in cell death (Figure 4D).

Figure 4: A: DHT-treated DPCs increased secretion of both IL-6 and bFGF; B, C: CB-03-01 (clascoterone) was effective at reducing IL-6 secretion; however, neither drug was able to inhibit bFGF secretion; D: Cell viability assays showed that the responses were not due to cell death.[12]Rosetter, C., Rosette, N., Mazzetti, A., Moro, L., Gerloni, M. Cortexolone 17ɑ-Proprionate (Clascoterone) is an Androgen Receptor Antagonist in Dermal Papilla Cells in Vitro. Journal of Drugs in … Continue reading
So, we know that CB-03-01 can effectively compete with DHT for the androgen receptor, reducing the harmful effects of the hormone. However, these experiments were conducted in cells in a dish. Let’s move on to studies conducted on human patients.
Is CB-03-01 Clinically Effective at Treating Hair Loss?
CB-03-01 has undergone three Phase II trials, which have informed the dosage for an upcoming Phase III trial that is expected to be completed in 2025. The first Phase II trial was a proof-of-concept study conducted in 2014 with 95 males with androgenetic alopecia. However, the Phase II trial results for male AGA were not publicly disclosed or published.[13]Clinical Trials, (2017). A Phase 2 Study to Evaluate the Safety and Efficacy of CB-03-01 Solution, a Comparator Solution and Vehicle Solution in Males with Androgenetic Alopecia. Clinical Trials. … Continue reading
The second Phase II study was another proof-of-concept study for the use of CB-03-01 in the treatment of female pattern baldness. Once again, there have yet to be fully published results. However, Bloomberg did publish a press release summarizing the main findings.[14]Cassiopea Spa, (2021). Cassiopea SpA Announces Topline Results of Phase II Proof of Concept Trial of Clascoterone Solution for the Treatment of Androgenetic Alopecia in Females. Bloomberg. Available … Continue reading. The trial enrolled 293 women aged 18 to 55, all experiencing androgenetic alopecia (AGA). The participants were divided into groups, with each group containing 70 individuals. The trial’s main objective was to evaluate the effects of different treatments over six months, comparing them to a control group that received a placebo (vehicle) and another group that used a 2% minoxidil solution.
All participants applied their assigned treatment twice daily. The treatment groups included two concentrations of CB-03-01, specifically 5% and 7.5%. The primary outcome measurements were changes in hair count and assessing hair growth over the six months of treatment.
Interestingly, only a subgroup of women under 30 using the 5% CB-03-01 solution showed statistically significant improvements in hair count, which was unexpected. Cassiopea mentioned that they were encouraged by the data and would further analyze it to identify further subgroups. However, since female-pattern hair loss typically occurs later in life for women (in their 50s or 60s), this treatment may not be appropriate for most patients. Therefore, further research is needed to determine its broader applicability.[15]Fabbrocini, G., Cantelli, M., Masara, A., Annunziata, M.C., Marasca, C., Cacciapuoti, S. (2018). Female pattern hair loss: A clinical, pathophysiologic, and therapeutic review. International Journal … Continue reading
Furthermore, although the press release mentioned that some participants were treated with 2% minoxidil, there was no information on how CB-03-01 performed compared to this. This highlights the issue of using press releases instead of peer-reviewed journal articles, as important data can be omitted.
The third phase II study recruited more than 400 male participants in Germany, aged 18-55, with mild to moderate AGA. All participants applied CB-03-01 at concentrations of 2.5%, 5%, 7.5% twice daily, or 7.5% once daily. The control group applied a vehicle solution (once- or twice daily).[16]Cassiopea Spa, (2021). Cassiopea Announces Very Positive Phase II Twelve Months Results for Breezula® (Clascoterone) in Treating Androgenetic Alopecia Bloomberg. Available at: … Continue reading Once again, the results were only available via a press release, so while some data was present we do not know if any has been omitted. It is reported that the results showed statistically significant improvements in target area hair counts and hair growth assessment scores across all active groups compared to the vehicle control. Notably, the highest change occurred in the 7.5% twice-daily group. This group also showed the highest statistically significant improvements in hair width in the treated area.
Two Phase III studies are awaiting recruitment, with expected completion dates in January 2025.[17]Clinical Trials, (no date). CB-03-01. NIH. Available at: https://clinicaltrials.gov/search?cond=Hair%20Loss%2FBaldness&term=CB-03-01 (Accessed: 17 October 2023)
Is CB-03-01 Safe?
According to the Bloomberg press release, treatment-emergent adverse events (TEAEs) were mostly minimal, mild, or trace and unrelated to the study drug. However, very little detail is given. The most frequently observed local skin reactions across all treatment groups were minimal to mild scaling, redness, or minimal itching.[18]Cassiopea Spa, (2021). Cassiopea SpA Announces Topline Results of Phase II Proof of Concept Trial of Clascoterone Solution for the Treatment of Androgenetic Alopecia in Females. Bloomberg. Available … Continue reading
In a Phase III trial of CB-03-01 for patients with facial acne, TEAEs were also generally mild in severity and similar to the control. The most common were pain, dryness, hypersensitivity at the site of application, redness, contact dermatitis, and headache.[19]Hebert, A., Thiboutot, D., Gold, L.S., Cartwright, M., Gerlonim M., Fragasso, E., Mazzetti, A. (2020). Efficacy and Safety of Topical Clascoterone Cream, 1% for Treatment in Patients with Facial … Continue reading
CB-03-01 has yet to receive FDA approval for hair loss treatment, and certainly, more information on its safety and efficacy is required. The results from the upcoming Phase III studies should provide more information.
Can I Make CB-03-01 at Home?
We want to make it clear here – we do not endorse the use of homemade CB-03-01 (or any other treatment) as there may be issues with the purity of CB-03-01 and may lead to other unintended side effects. However, some people are buying powdered CB-03-01 and making a topical solution at home. CB-03-01 powder is widely available online for research and is easy to buy. As for a vehicle, some are using ethanol, propylene glycol (PG), and diethylene glycol monoethyl ether (DEGEE) at a 1:1:1 ratio, whereas others are using ethanol and PG alone.[20]Reddit, (2020). Anyone know how to make your own CB0301 vehicle? Reddit. Available at: https://www.reddit.com/r/tressless/comments/l5y0di/anyone_know_how_to_make_your_own_cb0301_vehicle/ (Accessed: … Continue reading According to Selleckchem, it is soluble in both dimethylsulfoxide (DMSO) and ethanol.[21]Selleckchem, (no date). Clascoterone. Selleckchem. Available at: https://www.selleckchem.com/datasheet/clascoterone-S689601-DataSheet.html (Accessed 17 October 2023)
Is CB-03-01 for Me?
While CB-03-01 is available under the brand name Winlevi for acne at a 1% concentration, it will not be available at the 5% dosage (which seemed effective in Phase II studies) until Phase III studies have been completed and FDA approval application has begun.
However, when it is available, you may want to try this treatment if:
- You are male or female
- You are female and 30 or under
- You have AGA (this treatment targets androgen receptors, so it will not be beneficial for those with other types of hair loss)
References[+]
References ↑1, ↑14, ↑18 Cassiopea Spa, (2021). Cassiopea SpA Announces Topline Results of Phase II Proof of Concept Trial of Clascoterone Solution for the Treatment of Androgenetic Alopecia in Females. Bloomberg. Available at: https://www.bloomberg.com/press-releases/2021-09-10/eqs-adhoc-cassiopea-spa-announces-topline-results-of-phase-ii-proof-of-concept-trial-of-clascoterone-solution-for-the-treatment (Accessed: 17 October 2023) ↑2, ↑16 Cassiopea Spa, (2021). Cassiopea Announces Very Positive Phase II Twelve Months Results for Breezula® (Clascoterone) in Treating Androgenetic Alopecia Bloomberg. Available at: https://www.bloomberg.com/press-releases/2019-04-16/cassiopea-announces-very-positive-phase-ii-twelve-months-results-for-breezula-clascoterone-in-treating-androgenetic (Accessed: 17 October 2023) ↑3, ↑6 Cosmo, (no date). Breezula. Cosmo Pharmaceuticals Available at: https://www.cosmopharma.com/pipeline/breezula (Accessed: 17 October 2023) ↑4 Kokal, M., Mirzakhani, K., Pungsrinont, T., Baniahmad, A. (2020). Mechanisms of Androgen Receptor Agonist- and Antagonist-Mediated Cellular Senescence in Prostate Cancer. Cancers (Basel). 12(7). Available at: https://doi.org/10.3390/cancers12071833 ↑5 Drugbank Online (no date), Clascoterone. Drugbank Online. Available at: https://go.drugbank.com/drugs/DB12499 (Accessed: 16 October 2023) ↑7 Handelsman, D.J. (2020). Androgen Physiology, Pharmacology, Use and Misuse. Endotext [Internet]. South Dartmouth (MA). Available at: https://www.ncbi.nlm.nih.gov/books/NBK279000/ (Accessed: 17 October 2023) ↑8 Bahta, A.W., Farjo, N., Farjo, B., Philpott, M. Premature senescence of balding dermal papilla cells in vitro is associated with p16(INK4a) expression. Journal of Investigative Dermatology. 218(5). 1088-1094. Available at: https://doi.org/10.1038/sj.jid.5701147 ↑9 Rosetter, C., Rosette, N., Mazzetti, A., Moro, L., Gerloni, M. Cortexolone 17ɑ-Proprionate (Clascoterone) is an Androgen Receptor Antagonist in Dermal Papilla Cells in Vitro. Journal of Drugs in Dermatology. 18(2). 197-201 Available at: https://jddonline.com/articles/cortexolone-17a-propionate-clascoterone-is-a-novel-androgen-receptor-antagonist-that-inhibits-produc-S1545961619P0412X/ (Accessed 17 October 2023) ↑10, ↑11, ↑12 Rosetter, C., Rosette, N., Mazzetti, A., Moro, L., Gerloni, M. Cortexolone 17ɑ-Proprionate (Clascoterone) is an Androgen Receptor Antagonist in Dermal Papilla Cells in Vitro. Journal of Drugs in Dermatology. 18(2). 197-201 Available at: https://jddonline.com/articles/cortexolone-17a-propionate-clascoterone-is-a-novel-androgen-receptor-antagonist-that-inhibits-produc-S1545961619P0412X/ (Accessed 17 October 2023) ↑13 Clinical Trials, (2017). A Phase 2 Study to Evaluate the Safety and Efficacy of CB-03-01 Solution, a Comparator Solution and Vehicle Solution in Males with Androgenetic Alopecia. Clinical Trials. Available at: https://clinicaltrials.gov/study/NCT02279823 (Accessed: 17 October 2023) ↑15 Fabbrocini, G., Cantelli, M., Masara, A., Annunziata, M.C., Marasca, C., Cacciapuoti, S. (2018). Female pattern hair loss: A clinical, pathophysiologic, and therapeutic review. International Journal of Womens Dermatology. 4(4). 203-211. Available at: https://doi.org/10.1016/j_ijwd.2018.05.001 ↑17 Clinical Trials, (no date). CB-03-01. NIH. Available at: https://clinicaltrials.gov/search?cond=Hair%20Loss%2FBaldness&term=CB-03-01 (Accessed: 17 October 2023) ↑19 Hebert, A., Thiboutot, D., Gold, L.S., Cartwright, M., Gerlonim M., Fragasso, E., Mazzetti, A. (2020). Efficacy and Safety of Topical Clascoterone Cream, 1% for Treatment in Patients with Facial Acne. Two Phase 3 Randomized Clinical Trials. JAMA Dermatol. 156(6). 1-10. Available at: https://doi.org/10.1001/jamadermatol.2020.0465 ↑20 Reddit, (2020). Anyone know how to make your own CB0301 vehicle? Reddit. Available at: https://www.reddit.com/r/tressless/comments/l5y0di/anyone_know_how_to_make_your_own_cb0301_vehicle/ (Accessed: 17 October 2023) ↑21 Selleckchem, (no date). Clascoterone. Selleckchem. Available at: https://www.selleckchem.com/datasheet/clascoterone-S689601-DataSheet.html (Accessed 17 October 2023) Corticosteroids are a class of steroid hormones that have emerged as a treatment against, in particular, alopecia areata and scarring alopecia. These compounds, synthesized to mimic the activity of cortisol, a hormone produced by the adrenal glands, exhibit potent anti-inflammatory and immunosuppressive properties. This makes them effective in treating hair loss conditions where inflammation or an autoimmune response plays a critical role.
However, long-term corticosteroid use is not without potential drawbacks. When overused (or used for too long), topical corticosteroids are causally linked to hormonal changes, alterations to skin pigmentation, the creation of spider veins, and even skin thinning. Some adverse effects can be permanent – with the risk of irreversibility increasing alongside the dose and duration of use. Without usage breaks and/or careful dosing guidelines, long-term users of topical corticosteroids can inadvertently disfigure their skin.
In the last two years, we’ve observed a concerning trend in the hair loss industry: big-brand telehealth companies now add low-dose corticosteroids – i.e., 1% hydrocortisone and 0.01% fluocinolone – to their prescription hair growth topicals. They’re also recommending patients apply corticosteroids to their scalps up to twice daily, forever.
These corticosteroids undoubtedly help lower scalp inflammation and may offset skin irritation from ingredients like tretinoin (retinoic acid) – which is often paired with hair growth drugs, such as minoxidil, to enhance drug activation and penetration.But is there any evidence that twice-daily use of topical corticosteroids – applied daily, forever, and with no pulse dosing or dosing breaks – is safe? Or are these telehealth companies exposing their patients to unknown risks, gambling with their health, and selling them into short-term hair gains without considering the long-term consequences?
This article will delve into the efficacy and long-term safety of corticosteroids – particularly as a therapy for hair loss disorders. We’ll explore corticosteroids and their therapeutic role in treating hair loss. We’ll also explore considerations for dosing and duration. This is particularly important for people who might be currently using topical corticosteroids on their scalps and who don’t understand the risks they might be exposing themselves to 5-10 years into the future.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What Role Do Corticosteroids Play in Treating Alopecia?
In the context of alopecia, corticosteroids reduce inflammation and suppress the immune system’s activity around hair follicles. This action can halt the progression of hair loss and, in many cases, stimulate hair regrowth. The application of corticosteroids in hair loss treatment can vary; they can be administered topically, injected directly into the scalp, or taken orally.
Within the class of corticosteroids are:
Glucocorticoids: such as cortisol and cortisone, influence carbohydrate, fat, and protein metabolism.[1]Macfarlane, D.P., Forbes, S., Walker, B.R. (2008). Glucocorticoids and fatty acid metabolism in humans: fuelling fat redistribution in the metabolic syndrome. Journal of Endocrinology. 197(2), … Continue reading They are anti-inflammatory, immunosuppressive, and vasoconstrictive (narrow blood vessels). Their anti-inflammatory effects occur through inhibiting inflammatory mediators and stimulating anti-inflammatory mediators. Their immunosuppressive effects occur through direct action on immune cells.[2]Coutinho, A.E., Chapman, K.E. (2011). The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments, and mechanistic insights. Molecular and Cellular Endocrinology. … Continue reading
Mineralocorticoids: such as aldosterone, regulate electrolyte and water balance. They modulate ion transport in the renal tubules of the kidneys.[3]Yang, J., Young, M.J. (2009). The mineralocorticoid receptor and its coregulators. Journal of Molecular Endocrinology. 43(2), 53-64. Available at: https://doi.org/10.1677/JME-09-0031
How is the Potency of a Corticosteroid Decided?
There are seven potency classifications for corticosteroids, which range from Class I – super potent corticosteroids to Class VII – least potent corticosteroids.[4]Gabros, S., Nessel, T.A., Zito, P.M. (2023) Topical Corticosteroids. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Available from: … Continue reading This is based on several factors, including its chemical structure, formulation, and the ability of the drug to cause vasoconstriction in the skin, which is often assessed through vasoconstrictor assays.[5]Stoughton, R.B. (1992). The vasoconstrictor assay in bioequivalence testing: practical concerns and recent developments. International Journal of Dermatology. Available at: … Continue reading These assays measure the degree of skin blanching (induction of longer-than-normal skin paleness) induced by the corticosteroid.
What are the Benefits of Corticosteroids in Treating Alopecia?
Corticosteroids are particularly beneficial in treating alopecia areata and scarring alopecias because they modulate inflammatory and immune response pathways. High potency, medium potency, and low potency have all shown some efficacy in treating alopecia, with the highest efficacy observed with high-potency corticosteroids under occlusion.[6]Alsantali, A. (2011). Alopecia areata: a new treatment plan. Clinical Cosmetic and Investigational Dermatology. 4, 107-115. Available at: https://doi.org/10.2147/CCID.S22767
However, it should be noted that their maximum usage durations depend on the potency of the corticosteroid. Super potent corticosteroids have a maximum duration of 3 weeks, high and medium potency have a maximum duration of 12 weeks, and low potency have no specified limit.[7]Stacey, S.K., Mceleney, M. (2021). Topical Corticosteroids: Choice and Application. American Family Physician. 103(6). 337-343. Available at: … Continue reading Continuing to use corticosteroids after these time points may increase the risk of experiencing adverse effects.
What Risks Are Associated with Corticosteroid Use?
Topical corticosteroids can lead to both skin-related (cutaneous) and whole-body (systemic) side effects, with risk increasing with a larger area of application and higher potency of the drug.[8]Stacey, S.K., Mceleney, M. (2021). Topical Corticosteroids: Choice and Application. American Family Physician. 103(6). 337-343. Available at: … Continue reading
Some common skin-related effects can include:
- Skin thinning
- Stretch marks
- Spider veins
- Easy bruising and purpura
- Delayed wound healing
- Hyper or hypopigmentation
- Acne and rosacea like eruptions
- Hypertrichosis (increased hair growth)
- Infections or aggravation of existing infections
Long-term use may lead to whole-body (systemic) effects. These can include:
- Hypothalamus-pituitary-adrenal activity suppression (characterized by weakened immunity, anxiety, midday fatigue, difficulty sleeping, depression, and aching joints, amongst others)
- Cushingoid appearance (moon face, acne, and thin, easily bruised skin, amongst others)
- Unwanted facial skin hair in women (hirsutism)
- Impotence
- Menstrual irregularities
- Peptic ulcer disease
- Cataracts
- Increased intraocular pressure/glaucoma
- Myopathy
- Osteoporosis
- Vertebral compression fractures
Some patients may also experience a rebound phenomenon – although this is rare in low-potency corticosteroids.
One case study shows a patient who experienced worsening rebound after being treated with first 0.5%, then 1% of hydrocortisone, and again after a 5-day course of clobetasol butyrate and then hydrocortisone.[9]MEDSAFE, (2013). Steroid Rebound – A Topical Issue. MEDSAFE. Available at: https://www.medsafe.govt.nz/profs/PUArticles/June2013Steroid.htm (Accessed: 12 January 2023) It only resolved 3.5 months after stopping all steroid treatments.
However, a retrospective study of 300 patients found that patients who had received hydrocortisone 0.75% and precipitated sulfur 0.5% lotion for up to 15 years for common dermatological conditions of the face showed no evidence of rebound phenomenon, steroid acne, and perioral dermatitis.[10]Harlan, S.L. (2008). Steroid acne and rebound phenomenon. Journal of Drugs in Dermatology. 7(6). 547-550. Available at: PMID:18561585
What are the Long-Term Effects and Safety Profiles of Low Potency Corticosteroids?
There is no specified limit on the duration of use of low-potency corticosteroids. But how safe are they really? Are there any long-term studies showing that these steroids are safe to use long-term?
We’ve collated the longest studies available for several low-potency corticosteroids to help us determine this.
Corticosteroid Study: alopecia Study: other indication Safety profile (adverse effects?) References Alclometasone dipropionate 0.05% N/A Applied twice daily for 21 days in 31 patients with psoriasis. A comparative study with clobetasone butyrate cream 0.5%. No reported adverse events. [11]Aggerwal, A., Maddin, S. (1982). Alclometasone Dipropionate in Psoriasis: A Clinical Study. Journal of International Medical Research. 10, 414-418. Available at: … Continue reading Desonide 0.05% N/A Twice daily application of either desonide 0.05% hydrogel or desonide 0.05% ointment in 46 patients with mild to moderate atopic dermatitis. The study length was 4 weeks. No reported adverse events. [12]Trookman, N.S., Rizer, R.L. (2011). Randomized Controlled Trial of Desonide Hydrogel 0.05% versus Desonide Ointment 0.05% in the Treatment of Mild-to-moderate Atopic Dermatitis. The Journal of … Continue reading Fluocinolone acetonide 0.01% N/A Once daily application for 12 months alongside hydroquinone 4% and tretinoin 0.05% in 228 patients for treating facial melasma. Six cases of telangiectasia (spider veins), 5 mild and 1 moderate. [13]Torok, H.M., Jones, T., Rich, P., Smith, S., Tschen, E. (2005). Hydroquinone 4%, tretinoin 0.05%, fluocinolone acetonide 0.01%: a safe and efficacious 12-month treatment for melasma. Cutis. 75(1), … Continue reading Hydrocortisone 1% Applied twice daily to areas of hair loss for 2 cycles of 6 weeks on and 6 weeks off for a total of 24 weeks. 42 children with alopecia areata. Hydrocortisone 1% compared to clobetasol propionate 0.05%. Twice daily application of either hydrocortisone 1% or desonide 0.05% for 5 weeks in 113 children with mild-to-moderate atopic dermatitis. 36 children continued the study through to 6 months. Alopecia study: 2 patients in the hydrocortisone group experienced abnormal cortisol levels, which were resolved by the end of the study. One patient showed skin atrophy, which resolved by week 6. [14]Lenane, P., Macarthur, C., Parkin, C.P., Krafchik, B., DeGroot, J., Khambalia, A., Pope, E. (2014). Clobetasol Propionate, 0.05%, vs. Hydrocortisone, 1% for Alopecia Areata in Children. A Randomized … Continue reading,[15]Jorizzo, J., Levy, M., Lucky, A., Shavin, J., Goldberg, G., Dunlap, F., Hinds, A., Strelka, L., Baker, M., Tuley, M., Czernielewski, J.M. (1995). Multicenter trial for long-term safety and efficacy … Continue reading,[16]Salava, A., Perala, M., Pelkonen, A.S., Remitz, A., Makela. (2022). Safety of tacrolimus 0.03% and 0.1% ointments in young children with atopic dermatitis: a 36-month follow-up study. Clinical and … Continue reading,[17]Sigurgeirsson, B., Boznanski, A., Todd, G., Vertruyen, A., Schuttelaar, M.L.A., Zhu, X., Schauer, U., Qaqundah, P., Poulin, Y., Kristjansson, S., von Berg, A., Nieto, A., Boguniewicz, M., Paller, … Continue reading Twice daily application of 1. Hydrocortisone 1% or, if needed, hydrocortisone-17-butyrate or 2. 0.03% tacrolimus ointment for a 3-7 day course until clearance was achieved in 152 young children (aged 1-3) with eczema. 3 year follow-up. No side effects were observed for the hydrocortisone group. Application (not mentioned how often) of either pimecrolimus or 1% hydrocortisone in 2418 infants with atopic dermatitis. The treatment was used at the first signs/symptoms until clearance and initiated at the first signs/symptoms of atopic dermatitis. 5-year follow-up. 1% hydrocortisone was associated with an increased incidence of fever, cough, pharyngitis, viral rash, and lower respiratory tract infection. A number of the corticosteroids did not have any studies conducted for alopecia areata. Furthermore, several studies did not report any side effects; however, the corticosteroids were only used for 21 – 28 days in these cases. The study using fluocinolone 0.01% was the longest and was used daily for one year, with few side effects, which is promising.[18]Torok, H.M., Jones, T., Rich, P., Smith, S., Tschen, E. (2005). Hydroquinone 4%, tretinoin 0.05%, fluocinolone acetonide 0.01%: a safe and efficacious 12-month treatment for melasma. Cutis. 75(1), … Continue reading However, the researchers claimed that there were no signs of skin atrophy or thinning, but 6 patients did experience telangiectasia (otherwise known as spider veins) – which incidentally is a sign of skin thinning.[19]Mount Sinai, (no date), Telangiectasia. Mount Sinai. Available at: … Continue reading
The only study that used a low-potency corticosteroid to treat alopecia areata was hydrocortisone 1%. In this study, participants applied hydrocortisone 1% or clobetasol propionate 0.05% twice daily to areas of hair loss for 2 cycles of 6 weeks on and 6 weeks off for 24 weeks. During this time, there were few adverse events reported. These were abnormal cortisol levels, which were resolved before the end of the study. Furthermore, one patient who had extensive alopecia areata showed skin atrophy, which resolved by itself in 6 weeks.[20]Lenane, P., Macarthur, C., Parkin, C.P., Krafchik, B., DeGroot, J., Khambalia, A., Pope, E. (2014). Clobetasol Propionate, 0.05%, vs. Hydrocortisone, 1% for Alopecia Areata in Children. A Randomized … Continue reading
Furthermore, the only two studies that did include long-term follow-up either used very short pulses of the topical corticosteroid treatment or didn’t mention how often it was used at all.
It is clear from the above table that there is a distinct lack of long-term safety data for the use of corticosteroids in dermatological conditions and hair loss conditions. However, short-term or pulsed use (in the case of hydrocortisone) showed very few, if any, adverse effects.
What Role Do Telehealth Companies Play in The Sale and Use of Corticosteroid Treatments?
Telehealth companies provide a convenient alternative to accessing personalized medication and specialized knowledge that may not be readily available in general practice. Furthermore, you can do this from home, eliminating the need for travel and spending time in waiting rooms. You can buy compounded medications from these companies, including mixtures of finasteride, minoxidil, retinoids, and corticosteroids, amongst other treatments.
However, it appears that some telehealth companies may not be providing enough information for the typical buyer to determine how often they should be using their products that contain corticosteroids.
Some of these companies are also burying the known safety concerns of low-potency corticosteroids deep within their website navigations, while also not clearly stating these concerns upfront to prospective consumers. This strategy might help to mitigate these companies from legal actions related to non-disclosures, while at the same time, not truly informing their customers of the very real (and uncertain) risks they may face 2, 3, or 5 years into the future while using their products.
Conclusion
Short-term or pulsed use of low-potency corticosteroids might be safe and effective for hair loss conditions such as alopecia areata. However, the long-term safety of these treatments is less clear, with a distinct lack of extensive, long-term studies. The risks of long-term corticosteroid use are well-documented, which underscores the importance of careful monitoring and following medical guidance when using these treatments. While telehealth companies offer convenience and access to a range of hair loss treatments, including those containing corticosteroids, there is a gap in providing comprehensive safety information and use guidelines that align with the currently available data. This lack of information raises concerns about the potential for overuse or misuse of these products.
References[+]
References ↑1 Macfarlane, D.P., Forbes, S., Walker, B.R. (2008). Glucocorticoids and fatty acid metabolism in humans: fuelling fat redistribution in the metabolic syndrome. Journal of Endocrinology. 197(2), 189-204. Available at: https://doi.org/10.1677/JOE-08-0054 ↑2 Coutinho, A.E., Chapman, K.E. (2011). The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments, and mechanistic insights. Molecular and Cellular Endocrinology. 335(1), 2-13. Available at: https://doi.org/10.1016/j.mce.2010.04.005 ↑3 Yang, J., Young, M.J. (2009). The mineralocorticoid receptor and its coregulators. Journal of Molecular Endocrinology. 43(2), 53-64. Available at: https://doi.org/10.1677/JME-09-0031 ↑4 Gabros, S., Nessel, T.A., Zito, P.M. (2023) Topical Corticosteroids. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532940 ↑5 Stoughton, R.B. (1992). The vasoconstrictor assay in bioequivalence testing: practical concerns and recent developments. International Journal of Dermatology. Available at: https://doi.org/10.1111/j.1365-4362.1992.tb04009.x ↑6 Alsantali, A. (2011). Alopecia areata: a new treatment plan. Clinical Cosmetic and Investigational Dermatology. 4, 107-115. Available at: https://doi.org/10.2147/CCID.S22767 ↑7, ↑8 Stacey, S.K., Mceleney, M. (2021). Topical Corticosteroids: Choice and Application. American Family Physician. 103(6). 337-343. Available at: https://www.aafp.org/pubs/afp/issues/2021/0315/p337.html#:~:text=Triamcinolone%20acetonide%200,Ointment%2C%20cream%2C%20lotion%2C%20gel%2C%20foam (Accessed: 12 January 2024) ↑9 MEDSAFE, (2013). Steroid Rebound – A Topical Issue. MEDSAFE. Available at: https://www.medsafe.govt.nz/profs/PUArticles/June2013Steroid.htm (Accessed: 12 January 2023) ↑10 Harlan, S.L. (2008). Steroid acne and rebound phenomenon. Journal of Drugs in Dermatology. 7(6). 547-550. Available at: PMID:18561585 ↑11 Aggerwal, A., Maddin, S. (1982). Alclometasone Dipropionate in Psoriasis: A Clinical Study. Journal of International Medical Research. 10, 414-418. Available at: https://doi.org/10.1177/030006058201000605 ↑12 Trookman, N.S., Rizer, R.L. (2011). Randomized Controlled Trial of Desonide Hydrogel 0.05% versus Desonide Ointment 0.05% in the Treatment of Mild-to-moderate Atopic Dermatitis. The Journal of Clinical and Aesthetic Dermatology. 4(11), 34-38. Available at: PMID:22125657 ↑13 Torok, H.M., Jones, T., Rich, P., Smith, S., Tschen, E. (2005). Hydroquinone 4%, tretinoin 0.05%, fluocinolone acetonide 0.01%: a safe and efficacious 12-month treatment for melasma. Cutis. 75(1), 57-62. Available at: PMID:15732437 ↑14, ↑20 Lenane, P., Macarthur, C., Parkin, C.P., Krafchik, B., DeGroot, J., Khambalia, A., Pope, E. (2014). Clobetasol Propionate, 0.05%, vs. Hydrocortisone, 1% for Alopecia Areata in Children. A Randomized Clinical Trial. JAMA Dermatology. 150(1). 47-50. Available at: https://doi.org/10.1001/jamadermatol.2013.5764 ↑15 Jorizzo, J., Levy, M., Lucky, A., Shavin, J., Goldberg, G., Dunlap, F., Hinds, A., Strelka, L., Baker, M., Tuley, M., Czernielewski, J.M. (1995). Multicenter trial for long-term safety and efficacy comparison of 0.05% desonide and 1% hydrocortisone ointments in the treatment of atopic dermatitis in pediatric patients. American Academy of Dermatology. 33(1). 0-77. Available at: https://doi.org/10.1016/0190-9622(95)90014-4 ↑16 Salava, A., Perala, M., Pelkonen, A.S., Remitz, A., Makela. (2022). Safety of tacrolimus 0.03% and 0.1% ointments in young children with atopic dermatitis: a 36-month follow-up study. Clinical and Experimental Dermatology. 47(5). 889-902. Available at: https://doi.org/10.1111/ced. ↑17 Sigurgeirsson, B., Boznanski, A., Todd, G., Vertruyen, A., Schuttelaar, M.L.A., Zhu, X., Schauer, U., Qaqundah, P., Poulin, Y., Kristjansson, S., von Berg, A., Nieto, A., Boguniewicz, M., Paller, A.S., Dakovic, R., Ring, J., Luger, T. (2015). Safety and Efficacy of Pimecrolimus in Atopic Dermatitis: A 5-year Randomized Trial. Pediatrics. 135(4). 597-607. Available at: https://doi.org/10.1542/peds.2014-1990 ↑18 Torok, H.M., Jones, T., Rich, P., Smith, S., Tschen, E. (2005). Hydroquinone 4%, tretinoin 0.05%, fluocinolone acetonide 0.01%: a safe and efficacious 12-month treatment for melasma. Cutis. 75(1), 57-62. Available at: PMID:15732437 ↑19 Mount Sinai, (no date), Telangiectasia. Mount Sinai. Available at: https://www.mountsinai.org/health-library/symptoms/telangiectasia#:~:text=Telangiectasias%20of%20the%20skin%20occur,in%20the%20formation%20of%20telangiectasias. (Accessed: 12 January 2024) Finasteride is an FDA-approved medication for androgenic hair loss in men. Clinical studies suggest that 1 mg daily of finasteride can improve hair loss in 80-90% of men with androgenic alopecia (AGA) – with 5- and 10-year studies demonstrating hair maintenance in a large portion of users who continue treatment.
As such, many consider finasteride to be the gold-standard medical therapy for AGA.
But what happens when someone stops using finasteride? How long are hair gains preserved? When does hair loss resume? And can someone quit finasteride, but keep their hair gains by replacing finasteride with other treatments and/or therapies?
This article explores some of the studies attempting to answer these questions.[1]https://pubmed.ncbi.nlm.nih.gov/9777765/[2]https://pubmed.ncbi.nlm.nih.gov/11809594/[3]https://www.oatext.com/Long-term-(10-year)-efficacy-of-finasteride-in-523-Japanese-men-with-androgenetic-alopecia.php
Interested in Oral Finasteride?
Oral finasteride & minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.

What Happens If I Stop Using Finasteride?
Package inserts for the drug Propecia® (brandname finasteride) suggest that within 3-12 months of quitting finasteride, hair loss resumes and hair counts return to where they were prior to starting the drug.
But what’s the basis for this statement? In other words, where’s the scientific support?
The evidence actually comes from the original Phase II and Phase III clinical trials that granted finasteride FDA-approval for the treatment of androgenic alopecia.[4]https://pubmed.ncbi.nlm.nih.gov/9777765/
In a subset of finasteride users, participants were given the drug for a full year, then unknowingly switched into the placebo (i.e., sugar pill) group for the second year (i.e., months 12-24).
The investigators then charted these participants’ hair count changes from months 0-24, and compared those changes to those who continued using finasteride and those who were always receiving the placebo pill.
The results: unknowingly quitting finasteride led to a return to month 0 hair counts (actually, slightly below baseline) after 12 months of discontinuance. Just see the following chart. The group labeled Fin→Pbo is the group who took finasteride for year one, and a placebo pill for year two.

Kaufman KD, Olsen EA, Whiting D, Savin R, DeVillez R, Bergfeld W, Price VH, Van Neste D, Roberts JL, Hordinsky M, Shapiro J, Binkowitz B, Gormley GJ. Finasteride in the treatment of men with androgenetic alopecia. Finasteride Male Pattern Hair Loss Study Group. J Am Acad Dermatol. 1998 Oct;39(4 Pt 1):578-89. doi: 10.1016/s0190-9622(98)70007-6. PMID: 9777765.
This chart provides the scientific backing for the claims made within the Propecia® package insert. It’s also the reason why manufacturers of finasteride state that the drug must be used for a lifetime in order to maintain any of the hair gained and/or preserved by the drug.
What If I Stop Taking Finasteride Temporarily?
Under some circumstances, it is possible to stop taking finasteride temporarily, and without losing much (or any) hair. This is because there is a delay between the time at which finasteride is discontinued and when hair loss resumes.
The reason for this delay is because of the way finasteride behaves in the body – i.e., the drug’s pharmacokinetics. More specifically, finasteride’s metabolism and timing of effects on the body depend on factors such as its:
- Terminal half-life
- Biological half-life
- Tissue dissociation timings
For a deep-dive into these topics, see these articles.
- Finasteride: How Long Does It Stay In The Bloodstream?
- Finasteride: How Long Does It Stay Active In Scalp Tissue?
Otherwise, here are the key takeaways:
1. Finasteride’s biological effects can last up to 30 days after quitting
Due to finasteride’s terminal half-life of 5-7 hours and tissue dissociation timing of 4-5 days, the drug can actually exert biological effects on hormone profiles even up to ~30 days after quitting.
That means that finasteride can continue to therapeutically lower scalp levels of dihydrotestosterone (DHT), even for weeks after quitting the medication.
Just see this chart, which shows that even after men quit using finasteride, it still took several weeks before their serum DHT levels returned to baseline.[5]https://academic.oup.com/jcem/article/89/5/2179/2844345

Richard V. Clark, David J. Hermann, Glenn R. Cunningham, Timothy H. Wilson, Betsy B. Morrill, Stuart Hobbs, Marked Suppression of Dihydrotestosterone in Men with Benign Prostatic Hyperplasia by Dutasteride, a Dual 5α-Reductase Inhibitor, The Journal of Clinical Endocrinology & Metabolism, Volume 89, Issue 5, 1 May 2004, Pages 2179–2184
(Note: these relationships assume that finasteride reachced full tissue distribution and a steady-state plasma level commensurate with 1-5 mg of daily use over a number of weeks. For those who only took finasteride a handful of times, the drug’s effects may only take a matter of days to reverse).
2. Users can take advantage of the pharmacokinetics of finasteride to reduce drug exposure and still preserve their hair gains
Finasteride is FDA-approved for androgenic alopecia at 1 mg daily doses. However, given the pharmacokinetics of the drug, some researchers have wondered if daily dosing is necessary.
One investigation group decided to explore this by putting a group of men on 1 mg of finasteride daily for a year. But for year two, they randomized the men into two groups: one group who would continue taking finasteride every day, and the other group who would start a 30 days-on, 30 days-off dosing approach.
The researchers found that both groups achieved comparable hair parameter improvements in year two – even despite the second group only technically using finasteride for half the time (i.e., a total of 6 months versus 12 months).[6]https://jaad.org/retrieve/pii/S0190962220319289
The hypothesis: that finasteride’s pharmacokinetics allow for dosing schedules that alternate month-to-month. For those wanting to lower their drug exposure or simply “take breaks” from the medication – for any reason – this type of dosing might allow for this to happen without sacrificing much (or any) hair gains.
What If I Stop Finasteride For Longer Than One Month?
Say you’re troubleshooting side effects, or trying to conceive, and you decide to pause your use of finasteride for longer than one month.
Under these circumstances, there is a higher likelihood of hair loss resuming versus the 30-day withdrawal window. We see this reflected clinically in the withdrawal studies on finasteride, as well as anecdotally amongst members of our membership community.
This is because after 30 days of withdrawal, the effects of finasteride on scalp DHT levels have mostly worn off. This means that scalp DHT levels return to baseline, and under these circumstances, hair loss will eventually resume.
However, for many people, the resumption of hair loss doesn’t happen immediately. While there aren’t any studies of which we’re aware that track finasteride withdrawal versus hair count changes on a month-by-month basis, we have communicated with many finasteride users who’ve consistently reported, after quitting, that hair shedding and hair loss didn’t seem to pick back up again until months 2, 3, and beyond.
Even still, if you’re considering pausing finasteride use for any reason, try to keep the window of time beyond 30 days to a minimum. In doing so, you’ll put yourself in the best possible position for drug-related hair maintenance.
What If I Quit Finasteride And Replace It With Other Treatments?
We get this question all the time, and unfortunately, there’s no good clinical data to answer this question.
Scientifically speaking, finasteride’s mechanism of action is that it suppresses scalp DHT levels low enough to allow for hair cycle normalization and the partial reversal of hair follicle miniaturization. This typically occurs only at therapeutic levels of DHT reduction, which according to clinical studies for hair regrowth, seem to require lowering scalp DHT by 60-70%.
If someone quits finasteride and replaces the drug with other treatments, the preservation of any hair gains from finasteride will, for the most part, directly depend on the ability for those “replacement treatments” to suppress DHT levels to the same degree of finasteride.
For better or for worse, finasteride is one of the best tools we have to therapeutically and safely suppress scalp DHT levels enough to generate long-lasting hair growth – even despite its risk of side effects, which seem to affect 5-15% of users trying the drug.
Therefore, for anyone considering quitting finasteride, the most important question is to understand why. Then, we can create a roadmap or action plan based on that answer. For example:
- If quitting finasteride (as a male) to start to conceive: this can be done temporarily, and without a high risk of hair loss provided that you can conceive after month one of quitting but before month three of discontinuance.
- If quitting finasteride due to side effects: there’s a good chance that those side effects can be managed or eliminated with dose titration strategies, and/or the use of topical finasteride.
- If quitting finasteride because you want to try a natural approach to treating hair loss: we recommend first adding in a natural approach alongside finasteride use, rather than quitting finasteride abruptly.
- If quitting finasteride because you no longer want to use drugs to treat hair loss: we recommend watching this video to ensure your decision isn’t rooted in cognitive dissonance or misinformation.
If quitting finasteride for any other reason, please note that there are no studies exploring outcomes for men or women who withdraw from finasteride and replace the drug with other treatments.
Having said that, the totality of evidence strongly suggests that this is not necessarily a good gamble to make – as finasteride tends to suppress DHT levels in the scalp by a far larger margin (and for a far longer time period) than natural extracts such as saw palmetto. So, your expectation should be that hair loss, in all likelihood, will slowly resume.
Even still, we have seen success stories of people transitioning off finasteride and maintaining their hair gains. While this isn’t an approach we recommend unless absolutely necessary, here are the commonalities amongst people who’ve reported success with this:
- They multi-target their hair loss. In other words, they replace finasteride use with an array of supplements, topicals, and stimulation-based interventions that target their hair loss from multiple angles: DHT reduction, growth stimulation, angiogenesis, and more.
- They don’t immediately withdraw from finasteride. Instead, they add in all replacement interventions alongside finasteride use – and for at least 9-12 months. This allows for any potential synergies to occur between finasteride use and other therapies. Then, after achieving a new level of hair regrowth, they slowly wean away from finasteride via strategies such as topical finasteride and every-other-month oral dosing followed by titration – until after 3-5 months, they’re no longer using finasteride at all. Under the circumstances where users start noticing more hair fall, they hop back on finasteride until things stabilize. Under the circumstances whereby hair gains are maintained, they continue their drug withdrawal.
To reiterate, this is not something we actively recommend. But for those considering doing this, we recommend the above two strategies to minimize your downside risks.
Want Help With Your Hair Loss?
We offer one-on-one support to hair loss sufferers inside our membership community. This is where you can interact directly with hair loss researchers, access our library of product reviews, use our automated tools to build yourself a personalized regrowth plan, and protect yourself from the overwhelming negativity of most online hair loss forums.
If you’re interested in learning more, you can access our membership community right here.
Otherwise, we hope this article helps you make more informed decisions about your treatment choices.
References[+]
References ↑1, ↑4 https://pubmed.ncbi.nlm.nih.gov/9777765/ ↑2 https://pubmed.ncbi.nlm.nih.gov/11809594/ ↑3 https://www.oatext.com/Long-term-(10-year)-efficacy-of-finasteride-in-523-Japanese-men-with-androgenetic-alopecia.php ↑5 https://academic.oup.com/jcem/article/89/5/2179/2844345 ↑6 https://jaad.org/retrieve/pii/S0190962220319289 In this article, we’ll explore the science behind topical finasteride, if incidental exposure to the drug comes with a risk of harming pregnant women and/or children, and strategies you can employ starting today to minimize inadvertently exposing your household to secondary finasteride exposure – all while still preserving your hair gains from the drug.
Topical Finasteride: Benefits & Drawbacks
Finasteride is the world’s most effective FDA-approved treatment for androgenic alopecia in men. Having said that, the drug is not safe for use in children or in pregnant woman – mainly because it inhibits an enzyme that is critical for proper fetal and adolescent development.
Oral formulations of finasteride are ingested by the user, and thereby eliminate almost all possibilities of incidental drug exposure to partners or other household members of the drug user. The only exception to this is a small amount of detectable finasteride in semen, which can be absorbed by a partner during periods of unprotected intercourse – and in amounts that are considered far below danger levels (even while pregnant).[1]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2018472/pdf/11785276.pdf
In recent years, interest has exploded in an alternative delivery vehicle for finasteride: topical finasteride. This is because preliminary studies suggest topical finasteride can confer similar hair improvements versus the oral formulations, but also better localize the effects of the drug mainly to the scalp – thus lowering the risk of finasteride’s side effects.
Having said that, the switch to topical formulations comes alongside new risks: incidental drug exposure to partners and other members of the household. But are these risks quantifiable, and if so, how can we reduce them?
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
How Might Incidental Exposure To Finasteride Occur?
After applying topical finasteride, there is often a period of time – up to 30 minutes – whereby that finasteride solution has yet to fully dry onto the scalp. During this period, it’s much easier for topical finasteride to find its way onto other household surfaces or people – particularly if contact is made with the scalp.
During this window of time (when topical finasteride isn’t yet fully dried), here a few ways inadvertent exposure to topical finasteride can occur:
- Putting your head down on a pillowcase, thereby rubbing residual finasteride onto sheets that might be shared with your partner and/or children
- Resting your head on couch pillows and/or furniture surfaces
- Letting your partner and/or children play with your hair
In all of these scenarios, the amount of exposure to a partner or child will be relatively small. However, with repeated daily exposure throughout critical periods of development – such as a partner’s pregnancy or a child’s adolescence – each repeated contact comes alongside a cumulative increased risk of adverse events.
While the long-term effects of repeated, residual contact by spouses and/or children from topical finasteride have not been thoroughly investigated – and likely never will be (due to the difficulties of conducting such a study) – it goes without saying that it’s within our best interests not to expose our loved ones to unnecessary risks, particularly those that come with the potential for long-long adverse effects.
Topical Finasteride: How To Minimize Incidental Exposure To Loved Ones
Fortunately, when it comes to topical finasteride, there are great science-based management strategies that should allow you to keep using the medication while also minimizing – or even eliminating – your loved ones’ risks of incidental exposure. Here are a few that might take most of the risk off the table.
1. After applying topical finasteride, avoid physical contact for ~30 minutes
Depending on the carrier agents used for topical finasteride (alcohol, propylene glycol, etc.), most topicals should fully dry within a 30-minute window after application. At this point, most of the topical finasteride will remain trapped within the dried portion of the topical.
Once this window is reached, it’s far less likely that scalp contact with pillow cases, furniture, or even a partner’s hands will lead to appreciable leeching off the scalp. So, by making this very simple change, men and women can perhaps take most of the risk away regarding incidental finasteride exposure.
2. Wash pillow cases regularly, and try to dedicate a pillowcase just for the user of finasteride
Even after letting the topical dry, some topical finasteride (albeit significantly less) will leech onto the pillowcase or wherever else you might rest your head. While the amount will be substantially smaller than if you were to rest your hand on that pillowcase before the 30-minute time window for drying is completed, there’s still some topical finasteride that will end up in those sheets.
Under these circumstances, weekly washing of pillowcases is warranted. If that’s not of interest to you or your partner, you can instead dedicate one pillowcase to the person using topical finasteride that the other partner will not use.
If that’s not enough to create peace-of-mind, you can also consider wearing a loosely-fitting shower cap to bed. Some members of our membership community do this – particularly fathers with young boys who don’t want to leave any incidental exposure risks to chance.
3. Time your application windows for when you are out-of-the-house and/or unlikely to have skin contact with household members
Topical finasteride users can dramatically reduce the cumulative exposure risk to loved ones by timing their topical applications to periods where they are (mostly) outside of the home and/or unlikely to come into skin-to-skin contact with other household members. This can be done by either:
- Applying topical finasteride at least 30 minutes before bed, then washing it out each morning
- Applying topical finasteride prior to leaving for work, then washing it out after arriving home
If opting for either strategy, it’s critical to let topical finasteride site in the scalp skin for at least 6-12 hours. Otherwise, the diminishment in the drug’s contact time in the scalp may begin to hinder its efficacy. Here’s why.
How Long Should Topical Finasteride Stay on the Scalp Before Washing It Out?
When topicals are applied to the skin, there are multiple stages of absorption.
- Stage #1: the drug sits on the epidermis (the outermost layer of skin). Over several hours, some of the drug will absorb into the dermis, and some will evaporate.
- Stage #2: the drug absorbs percutaneously. This is when some of the drug moves from the epidermis into the dermis, where it can begin to affect hair follicles.
- Stage #3: the drug absorbs systemically. This is when some of the drug moves from the dermis into the bloodstream, where it can have systemic effects.
So, what’s the minimum amount of time topical finasteride must be left on the scalp to have an effect? First, one needs to know how much of the drug absorbs into the dermis over time.
To answer this, there is an in vitro study measuring percutaneous absorption of topical finasteride across various formulations: ethosomes, ethanol, liposomes, and aqueous (water). [2]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2977015/
Here’s a chart showing the percent of topical finasteride that percutaneously absorbs (enters the dermis) over a 24-hour period:

Penetration profiles of finasteride permeating through human skin from different preparations (mean ± SD, n = 4)
According to these study results, if applying hydroethanolic finasteride to the scalp, then at the 10-hour mark, ~5 ug/cm2 will have been absorbed percutaneously. By hours 22-24, that absorption rises to ~8 ug/cm2. That means leaving the drug on the scalp for an additional 12-14 hours before washing it off only offers an additional 3 ug/cm2 of percutaneous absorption.
So, say that to minimize a partner’s exposure to finasteride means only keeping it on the scalp for 10 hours before washing it off. This begs the question: is the 5 ug/cm2 of absorbed finasteride enough to therapeutically lower scalp levels of dihydrotestosterone (DHT) and regrow hair?
Topical Finasteride: How Long Does It Need To Stay In The Scalp To Be Effective?
There aren’t any clinical studies attempting to answer this question. However, a look at surrogate data can help ballpark an answer.
First, a percentage of topical finasteride will absorb into the dermis, and a smaller percentage of topical finasteride absorbed into the dermis will later absorb into the bloodstream. This means after applying topical finasteride; people can use time-dependent DHT reductions in the bloodstream to “ballpark” how much DHT is likely also getting reduced in the scalp. This is, again, because there is more topical finasteride that percutaneously absorbs than systemically absorbs.
So, for lower dosages, the effects we see in the system can be used as signals for what’s happening, at a minimum, in the scalp skin.
In that regard, see this figure from a 2014 study measuring the effects of one versus two applications of 1 mL of 0.25% topical finasteride on serum DHT levels. [3]https://pubmed.ncbi.nlm.nih.gov/25074865

Caserini, M., Radicioni, M., Leuratti, C., Annoni, O., & Palmieri, R. (2014). A novel finasteride 0.25% topical solution for androgenetic alopecia: pharmacokinetics and effects on plasma androgen levels in healthy male volunteers. International journal of clinical pharmacology and therapeutics, 52(10), 842–849.
Six hours after applying 1 mL or 2 mL applications of 0.25% topical finasteride (2.275-4.550 mg of finasteride), serum DHT reductions flatline. This means that for the 2 mL application group (the black circle with a dotted line), there was enough systemic absorption by the 6-hour mark to effectively lower serum DHT levels as much as they would normally lower with 1 mg of oral finasteride.
Keep in mind that finasteride has an upper limit for its effects on serum DHT reduction. After hitting ~70% reduction in serum DHT, more finasteride doesn’t reduce serum DHT. The same is true with scalp DHT reductions.
So, the above study shows that with topical finasteride applications of 2.275 mg or higher in a hydroxypropyl chitosan delivery vehicle, systemic reductions in DHT equal that of 1 mg of oral finasteride. And with topical finasteride, since serum DHT reductions are sort of like “canaries in the coal mine” for scalp DHT reduction, we can take an educated guess that 6-12 hours after applying topical finasteride. There’s likely enough percutaneous absorption to therapeutically lower scalp DHT levels for hair regrowth.
This is corroborated by a 1997 study suggesting that 2 mL daily of 0.005% topical finasteride (0.0912 mg of finasteride exposure) improved hair parameters for men with AGA and without affecting serum DHT levels – even after 16 months of treatment. [4]https://www.tandfonline.com/doi/abs/10.3109/09546639709160517
Taken together, all of the above evidence signals that, depending on the exposure level, 6-12 hours of exposure to topical finasteride should be enough to have a therapeutic effect on scalp DHT reductions (and hair growth).
Do these time windows apply to all topical finasteride formulations?
No. Obviously, the contact time required for topical finasteride to be effective depends on a number of factors:
- The finasteride dilution (i.e., 0.01% vs. 0.1% topical finasteride)
- The volume of topical applied (i.e., 1 mL vs. 2 mL)
- The topical’s carrier ingredients (i.e., hydroxypropyl chitosan vs. ethanol vs. propylene glycol vs. liposomes)
- The frequency of application (i.e., once-daily, twice-daily, every-other-day, etc.)
Nonetheless, a 6-12 hour contact window should allow for therapeutic efficacy of many big-brand topical finasteride formulations available to consumers currently. However, if you’d like to get specific about adjustments on an individual basis, we offer that level of support inside our membership community.
Final Thoughts
For the most part, occasional incidental exposure to topical finasteride should not cause problems for household members. With that said, there are certain groups at an elevated risk – particularly pregnant women and children – and in these groups, cumulative risk over a lifetime of incidental topical finasteride exposure has yet to be studied.
If this is a concern for you, men and women can minimize the risk of incidental drug exposure from topical finasteride by doing any (or all) of the following:
- Avoiding all physical contact with the scalp for at least 30 minutes after topical finasteride application (so that it fully dries)
- Dedicating a pillowcase to the topical finasteride user, and washing that pillowcase weekly
- Wearing a loosely-fitting shower cap to bed
- Timing topical finasteride applications to 6-12 hour windows where the user is out-of-the-house and/or unlikely to come into contact with household members
Using the evidence and strategies above, our hope is that topical finasteride users can minimize or even eliminate the risk of incidental exposure, all while preserving their hair gains.
References[+]
Fluridil: Scientific Deep-Dive
Fluridil, otherwise known as topilutamide (or by the brand name Eucapil) is a topical medication that has been tested as a treatment for both androgenetic hair loss and hirsutism (excess facial hair growth in women). In 2021, the patent for fluridil expired, however, there have been no generic fluridil treatments that have come to the market. Fluridil has been approved for cosmetic use in Europe but does not have FDA or EMA approval as a treatment for androgenetic alopecia. You can however buy this product on shopping websites, such as Amazon, for around $83 (at the time of writing). But is fluridil worth your money?
In this article, we will look at how Fluridil works, what the clinical evidence for it is, and whether it is safe to use.
Key Takeaways
-
- Drug. Fluridil is an anti-androgenic drug that is currently on the market for the treatment of androgenetic alopecia and hirsutism. It is known to reduce the gene expression of androgens. Due to its similar structure to other anti-androgens, it’s thought to also exert its effect by binding to androgen receptors. As it readily breaks down in aqueous solutions, some researchers believe that it is safer to use than other anti-androgens, and can be applied locally without the risk of side effects on the rest of the body.
- Clinical Data. There are only two studies that have been completed for fluridil: one on men and one on women.
- The first study was 9 months long and completed on 43 men with diagnosed androgenetic alopecia (AGA) aged between 20-56, in which 2mls of 2% fluridil was topically applied once nightly. Researchers found that in the first 3 months, there was a significant increase in the number of growing hairs, and a significant decrease in the number of non-growing hair, with no effects on testosterone levels or perceived sexual libido and function. Furthermore, fluridil, or its by-products, was not found to be present in the serum. Researchers also found, however, that the positive effects on the number of growing hairs/non-growing hairs did not last past the 3-month mark, and were instead maintained. A small safety study completed alongside this determined that either 2% or 4% fluridil was ok to use without adverse effects.
- The second study was 9 months long and only completed on 11 women, 2 of which had to drop out of the study due to adverse effects from the isopropanol that the fluridil was diluted in. The participants applied 2mls of 2% fluridil, once nightly. The researchers did not find any significant change in growing or non-growing hairs, however, they did measure an increase in hair thickness. Due to the small sample size, the lack of a placebo, and the fact that every participant had taken another anti-androgenic medication within 3 months of the beginning of the study, it’s not possible to conclude whether fluridil has any effect or not for women with AGA.
- Safety. Unlike oral anti-androgenic drugs, fluridil should only work at the point of application as it should break down once it comes into contact with the blood. Additionally, across the limited parameters of both the studies mentioned above, no serious adverse effects were reported, however as both of the studies were 9 months long, with small sample sizes, we have no real information about what the long-term effects of fluridil usage may be.
- Best Practices. Based on the limited clinical data, if you decide to use fluridil, you could apply 2ml of a 2% fluridil solution in isopropanol once, at night before bed on a dry scalp (it will degrade if your hair or scalp is wet). You might be a candidate for fluridil if you are male with AGA (as the data isn’t sufficient for females with AGA), are comfortable with using a product that has very limited efficacy or safety data, have potentially seen results using other anti-androgens (such as finasteride), and don’t mind limiting hair washing to once or twice a week. If you’re interested in trying fluridil, although it’s not approved by the FDA, you can buy it on shopping sites like Amazon, and it’s possible that you may see limited results, at least over the first 3 months of usage.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is Fluridil?
As mentioned above, fluridil is a topical treatment that has been used in studies to determine its efficacy and safety in hair loss and excessive hair growth in women (hirsutism).
Fluridil was synthesized alongside four other compounds in a study designed to discover a novel, topical anti-androgenic compound. [1]Seligson, A.L., Campion, B.K., Brown, J.W., Terry, R.C., Kucerova, R., Bienova, M., Hajduch, M., Sovak, M. (2003). Development of Fluridil, a Topical Suppressor of the Androgen Receptor in … Continue reading Androgens are linked to certain types of hair loss such as androgenetic alopecia.
The researchers were also searching for a compound that rapidly degraded (broken down) into non-harmful by-products in the blood so that it does not have effects at the systemic (whole-body) level (but rather limits its activity locally to the area of application). Out of the five total compounds synthesized, the researchers determined that fluridil best fit their criteria, which are described below:
1. Down-regulation of androgen receptors
The growth of prostate cancer is often androgen receptor-dependent.[2]Fujita, K., Nonomura, N. (2019). Role of Androgen Receptor in Prostate Cancer: A Review. The World Journal of Men’s Health. 37(3), 288-295. Available at: https://doi.org/10.5534/wjmh.180040Therefore treating prostate cancer cells in a dish can be a useful way of seeing whether drugs have any anti-androgen receptor activity. In the human prostate cancer cell line LNCaP, fluridil reduced protein expression of androgen receptors by 40% at a concentration of 3μM, and by up to 95% at a 10μM concentration (Figure 1). Whilst this was not the most effective result, (BP-521 further reduced expression), it was the combination of this and results shown further down (Figure 2) that led the researchers to choose fluridil. Additionally, these compounds were compared to two other anti-androgen drugs (bicalutamide and hydroxyflutamide) and found that they did not decrease the expression of androgen receptors, indicating an additional mechanism of action of fluridil that other anti-androgen drugs may not have.

Figure 1: Reduction of protein expression of androgen receptors after 48 hours of drug incubation. BP-766 = fluridil. Adapted from: [3]Seligson, A.L., Campion, B.K., Brown, J.W., Terry, R.C., Kucerova, R., Bienova, M., Hajduch, M., Sovak, M. (2003). Development of Fluridil, a Topical Suppressor of the Androgen Receptor in … Continue reading
2. Degradation of the compound after incubation in human serum at 38°C
Fluridil was found to be the only compound that fully degraded in human serum by 48h of incubation (Figure 2). By contrast, BP-521, the compound that showed better down-regulation of androgen receptors barely showed any degradation, so did not match the criteria set by the researchers.
Fluridil degrades into BP-34 which – as the researchers show in Figure 1 – doesn’t have a large effect on the expression of androgen receptors. It also degrades into a perfluorocarboxylic acid (PFCA) called trifluoroacetic acid (TFA) which mammals are thought to be insensitive to. [4]Solomon, K., Velders, G., Wilson, S., MAdronich, S., Longstreth, J., Aucamp, P., Bornman, J. (2016). Sources, Fates, Toxicity and Risks of Trifluoroacetic Acid and its Salts: Relevance to Substances … Continue reading
The researchers state that the by-products are non-toxic and that they should be processed rapidly by the kidneys because they are ionic. Ionic substances are attracted to water molecules and undergo dissociation, where they disperse throughout the water, and can therefore be excreted in the urine.[5]Urine pH. (no date). University of Nottingham. Available at: https://www.nottingham.ac.uk/nmp/sonet/rlos/bioproc/kidneydrug/page_six.html (Accessed: 22 January 2022)

Figure 2: Percentage of compound remaining in human serum after incubation at 38°C. BP-766=fluridil. Adapted from:[6]Seligson, A.L., Campion, B.K., Brown, J.W., Terry, R.C., Kucerova, R., Bienova, M., Hajduch, M., Sovak, M. (2003). Development of Fluridil, a Topical Suppressor of the Androgen Receptor in … Continue reading
The researchers determined that based on their criteria, fluridil was the most promising in terms of its capacity to reduce androgen expression and due to its short half-life in aqueous solutions. This study however did not look at the efficacy of fluridil in the context of hair loss, and also did not provide data that established its safety in humans.
How does Fluridil work?
Androgenetic alopecia (AGA) is a form of hair loss with causes not yet fully understood, however, it is thought to be related to either excess androgens present, or an exaggerated response to androgens such as dihydrotestosterone (DHT). It affects both men and women and is characterized by progressive loss of hair over time in a particular pattern.[7]Ho, C.H., Sood, T., Zito, PM. (2022). Androgenetic Alopecia. StatPearls [Internet]. Treasure Island (FL). Available at: https://www.ncbi.nlm.nih.gov/books/NBK430924/. (Accessed: 22 January 2023)
Fluridil belongs to a class of drugs known as non-steroidal anti-androgens (NSAAs). NSAAs are chemicals that stop androgens (like testosterone and DHT) from binding to their receptors. This means that androgens then can’t exert their effects, as they need to bind to these receptors to initiate the signaling events that can lead to hair follicle miniaturization, amongst other things. NSAAs may also be called androgen receptor antagonists, or androgen receptor blockers. [8]Iverson, P., Melezinek, I., Schmidt, A. (2002). Nonsteroidal antiandrogens: a therapeutic option for patients with advanced prostate cancer who wish to retain sexual interest and function. BJUI … Continue reading [9]Ustuner, E.T. (2013). Cause of Androgenic Alopecia: Crux of the Matter. Plastic and Reconstructive Surgery. Global Open. 1(7), e64. Available at: https://doi.org/10.1097/GOX.0000000000000005
Receptors are specialized proteins in cells that allow specific chemicals to bind to them. In response to the correct chemical binding to the receptor, the receptor can exert downstream effects that have an impact on biology (a process known as signal transduction).[10]Miller, E.J., Lappin, S.L. (2022). Physiology, Cellular Receptor. StatPearls [Internet]. Treasure Island (FL). Available at: https://www.ncbi.nlm.nih.gov/books/NBK554403/#_NBK554403_pubdet_ … Continue reading Other NSAAs include flutamide and bicalutamide.
It’s important to note that there have been no studies to determine if this is really how fluridil works. Researchers have stated that this is because of fluridil’s instability in aqueous environments (meaning it is difficult to store, handle, and therefore study). Researchers hypothesize that because its structure is similar to other NSAAs, it has a similar mechanism of action, in addition to its ability to reduce the expression of androgen receptors. [11]Seligson, A.L., Campion, B.K., Brown, J.W., Terry, R.C., Kucerova, R., Bienova, M., Hajduch, M., Sovak, M. (2003). Development of Fluridil, a Topical Suppressor of the Androgen Receptor in … Continue reading
So, how fluridil actually works has not been fully determined, but is there any information on if and how fluridil affects hair follicles?
How can Fluridil have an impact on hair follicles?
Other than what has been hypothesized above (fluridil may be an androgen receptor inhibitor), it is not possible to know for sure exactly how fluridil might work on the hair follicle. As mentioned, there have been no studies in cells or isolated hair follicles in a dish (which may be due to fluridil being unstable in aqueous environments). Cells and isolated hair follicles require physiological media solutions that contain all the nutrients needed to survive and grow, creating a barrier in experimentation with this drug/to experiment with this drug.
Furthermore, the only work completed on animals was in the initial paper in which the researchers completed skin irritant tests and absorption tests, where they found that fluridil was non-irritant at a concentration of 2% (the concentration at which they sell the product, although they don’t mention whether it’s weight/volume or volume/volume) and that there was no fluridil (or its by-products) detected in rabbit serum after a 1% solution was applied twice daily for 10 days. Samples were collected at 2, 5, 21, and 48 hours after treatment and then once every other day for the next 3 days. [12]Seligson, A.L., Campion, B.K., Brown, J.W., Terry, R.C., Kucerova, R., Bienova, M., Hajduch, M., Sovak, M. (2003). Development of Fluridil, a Topical Suppressor of the Androgen Receptor in … Continue reading
The most important thing however is whether, in humans, fluridil actually works and is safe to use. There have been two studies using fluridil in humans diagnosed with androgenetic alopecia. So let’s see if, regardless of knowing exactly how fluridil works, it is effective at treating hair loss.
Is Fluridil effective at treating hair loss?
There are currently only two studies that look at the efficacy and safety of fluridil in humans.
Study 1
The first study was a randomized, double-blind study to determine the efficacy and safety of a topical 2% fluridil solution on 43 men between 20-56 years of age with diagnosed AGA. [13]Sovak, M., Seligson, A.L., Kucerova, R., Bienova, M., Hajduch, M., Bucek, M. (2002).Fluridil, a Rationally Designed Topical Agent for Androgenetic Alopecia: First Clinical Experience. American … Continue reading Fluridil was dissolved in isopropanol to make the solution, because of its instability in water-based liquids. The participants were randomly assigned into two groups, 23 receiving the fluridil, and 20 receiving a placebo of just isopropanol. Participants were required to apply the fluridil or the placebo solution once nightly before bed, to avoid direct sun exposure and to only wash hair a maximum of twice a week using warm water.
After 3 months, the study then became open-label (all participants knew what they were receiving) and all participants began receiving the 2% fluridil solution with a further follow-up 6 months later (so the study was a total of 9 months long).
Data was collected through:
- Phototrichogram – an area of the hair is shaved (1.1cm2) and then photographed using a digital camera. Individual hairs/follicles are counted at baseline and at specific time points throughout.
- Calculating the ratio of growing (anagen) to non-growing (telogen) hairs.
- Global scalp imaging – photographs are taken of the entire scalp for subjective comparison.
- Blood collection – for measuring serum testosterone, measuring for the presence of serum fluridil and its by-products, and determining other relevant blood chemistry values.
- Self-perception questionnaire – for sexual function and libido
Results at 3 months
After 3 months, the number of growing to non-growing hairs was compared between the placebo and fluridil groups (Figure 3). The researchers found that the percentage of anagen hairs significantly increased from the baseline in the fluridil-treated group (75.68% at 0 months – 85.09% at 3 months) and the percentage of telogen hairs significantly decreased (25.41% at 0 months -14.61% at 3 months). The placebo group, however, also showed a significant decrease in the percentage of telogen hairs, however (29.51% at 0 months – 21.87 at 3 months) as well.
When comparing the fluridil-treated group to the placebo group after 3 months of treatment, the percentage of anagen hairs was higher in the fluridil (85.09% and 77.25% respectively). Furthermore, there were fewer telogen hairs in the fluridil-treated group than in the placebo group (14.61% and 21.87% respectively).

Figure 3: Effect of fluridil and placebo on the percentage of growing/non-growing hairs after 3 months. (a) Comparing baseline to 3 months of treatment, (b) Comparing fluridil treated to placebo after 3 months. Adapted from:[14]Sovak, M., Seligson, A.L., Kucerova, R., Bienova, M., Hajduch, M., Bucek, M. (2002).Fluridil, a Rationally Designed Topical Agent for Androgenetic Alopecia: First Clinical Experience. American … Continue reading
At this point, the researchers decided that the effects of fluridil on hair growth were significant enough to change all participants to the treated group. It would however have been useful for the researchers to have stated what percentage of participants did see a positive effect.
Results at 9 months
To keep us all on track, by the end of the 9 months, the fluridil-treated group will have been using fluridil for 9 months, and the placebo group will have used the placebo for 3 months and then fluridil for 6 months. We’ll call the placebo group the ‘former placebo’ group now.
After counting growing and non-growing hairs, the researchers found that all groups now experienced significant increases in anagen hairs, and significant reductions in telogen hairs (Figure 4).

Figure 4: Effect of fluridil on the percentage of growing/non-growing hairs after 9 months. Comparing measurements taken at 3 months and 9 months for the former placebo group. Comparing measurements at baseline and 9 months for the fluridil-treated group. Adapted from:[15]Sovak, M., Seligson, A.L., Kucerova, R., Bienova, M., Hajduch, M., Bucek, M. (2002).Fluridil, a Rationally Designed Topical Agent for Androgenetic Alopecia: First Clinical Experience. American … Continue reading
The researchers then compared the changes in growing and non-growing hairs after 3 months and 9 months for the fluridil-treated group and found that there were no significant differences, which indicates that there may be a limit to the effect that fluridil can have on hair growth, and that this limit might be achieved only within the first 3 months. Fluridil however did appear to maintain the number of growing/non-growing hairs after that.

Figure 5: Comparing growing/non-growing hair counts at 3 months and 9 months of treatment for the fluridil group. Comparing growing/non-growing hair counts at 9 months of treatment for the fluridil and former placebo groups. Adapted from: [16]Sovak, M., Seligson, A.L., Kucerova, R., Bienova, M., Hajduch, M., Bucek, M. (2002).Fluridil, a Rationally Designed Topical Agent for Androgenetic Alopecia: First Clinical Experience. American … Continue reading
Let’s have a look at before-and-after images to see if this improvement shown in the data actually correlates to a visual improvement. Unfortunately, there is only one image shown (Figure 6), and we are left to wonder if this was the best case and if the reason that the others weren’t shown was that it was more difficult to see the improvements. Furthermore, there are no photos shown of anyone from the placebo group, so we cannot compare between groups.

Figure 6: Before-and afters (A-B) of a participant from the fluridil-treated group at A. Day 0 and B. 6-month time-points. Adapted from: [17]Sovak, M., Seligson, A.L., Kucerova, R., Bienova, M., Hajduch, M., Bucek, M. (2002).Fluridil, a Rationally Designed Topical Agent for Androgenetic Alopecia: First Clinical Experience. American … Continue reading
Other than measuring the number of growing/non-growing hairs, serum testosterone levels were also measured. Whilst variation between participants was observed, testosterone levels remained between the physiological range of 8-35 nm/L (Figure 7). Questionnaires also determined that participants did not experience any changes to libido or sexual performance either, however, it is not stated at what time points this data was collected. This is an indication that fluridil can only affect the hair follicle without leading to the systemic side effects that other anti-androgen drugs can cause. Additionally, the researchers did not detect fluridil or its by-product BP-34 in the serum of participants, further lending credence to this hypothesis.

Figure 7: Testosterone levels after treatment with fluridil (comparing baseline to the 90-day mark/comparing 90 days of fluridil to 90 days of the placebo group). Adapted from: [18]Sovak, M., Seligson, A.L., Kucerova, R., Bienova, M., Hajduch, M., Bucek, M. (2002).Fluridil, a Rationally Designed Topical Agent for Androgenetic Alopecia: First Clinical Experience. American … Continue reading
A separate study within the same paper was completed with 20 male participants between the ages of 18-60. Patches containing 2,4, or 6% fluridil in either isopropanol or Vaseline Intensive Care Lotion were applied once a day for 21 days (excluding weekends) to determine if fluridil caused any irritancy to the skin. Isopropanol was also given alone as a control. 2% and 4% fluridil were found to be non-irritant and non-sensitizing. 6% fluridil however caused a slight degree of macular erythema (a rash with flat discolored areas of skin and small raised bumps).
So, to summarize, the data indicates that fluridil treatment leads to more growing hairs and fewer non-growing hairs. This effect however plateaus after 3 months, with no improvement or deterioration occurring after. Fluridil doesn’t appear to affect testosterone levels (which other anti-androgen medications can), and, holding up to the claim of hydrolyzation neither fluridil nor its by-product BP-34 were found to be present in the serum of participants throughout the study. There is only one comparison photo however, and while it does look like there is an improvement, it’s not possible to know if this was just the very best case or whether other participants also experienced a similar level of improvement. Of course, the long-term effects of fluridil (beyond 9-months) are unknown.
Study 2
The second study completed by the same research group was an open study. An open study is a study in which both participants and researchers are aware of what they are using. It sought to determine the efficacy and safety of a 2% fluridil solution in isopropanol on 11 female participants, aged 22-45, with diagnosed AGA. [19]Kucerova, R., Bienova, M., Novotny, R., Fiuraskova, M., Hajduch, M., Sovak, M. (2006). Current Therapies of Female Androgenetic Alopecia and Use of Fluridil, a Novel Topical Antiandrogen, Scripta … Continue reading
Participants were required to massage 2 ml of the fluridil solution into their scalps once a day, in the evening. 2 women discontinued the study due to itching and reddening that developed at the site after treatment. It was determined with an allergy study that this was due to the isopropanol causing irritation, rather than a reaction to the fluridil itself.
Participants were advised to only apply the solution to a dry scalp and to limit hair washes to a maximum of 2 times a week.
In this study, all 11 participants were treated with fluridil, so there was no placebo or a no-treatment group. A placebo group is useful in clinical trials as it provides a group to compare throughout the study. The participants are also aware that they are receiving the actual treatment without a placebo, which may influence the participant’s perception of the effect of the treatment.
Several types of data were collected, including the following methods:
- Phototrichogram
- Global scalp imaging
- Hair Diameter measurement – an area of hair shaved and 3 weeks later ~50 new hairs collected and measured using a microscope.
- Changes in hair surface – five hairs from each patient were collected and prepared for scanning electron microscopy (SEM*).
- Evaluation by a physician (using a scoring system)
- Self-evaluation by participants (using a scoring system) to determine self-perception of hair growth and quality as well as effects on libido and sexual function.
- Blood tests – to measure serum testosterone, sex hormone binding globulin, other relevant blood chemistry, and serum fluridil or its by-products.
*(SEM is a special type of microscope that produces images of a sample by scanning the surface with electrons. These interact with the atoms that make up the sample, creating a much higher resolution image than might be obtained from a light-based camera). [20]Scanning Electron Microscopy. (no date). Nanoscience Instruments. Available at: https://www.nanoscience.com/techniques/scanning-electron-microscopy/ (Accessed: 22 January 2023)
Results
The authors of this study stated that they only included statistically significant data and what they considered to be “otherwise remarkable observations” in their results section.
The researchers found that fluridil treatment did not significantly increase the number of growing hairs or decrease the number of non-growing hairs over the whole study period (9 months), however, there was a significant improvement in hair diameter when it was measured at the 6 months and 9-month marks compared to the baseline. Whilst there are no images included in this paper, it is mentioned that the SEM images showed no changes in the overall morphology of the hair and that after evaluating global scalp images (photos taken from the top of the head) hair appeared to be thicker.

Figure 8: Hair diameter measurements and baseline, 6 months, and 9 months. Adapted from: [21]Kucerova, R., Bienova, M., Novotny, R., Fiuraskova, M., Hajduch, M., Sovak, M. (2006). Current Therapies of Female Androgenetic Alopecia and Use of Fluridil, a Novel Topical Antiandrogen, Scripta … Continue reading
5 out of 11 participants reported that they perceived themselves to have reduced hair loss after 6 months of treatment. 1 out of 11 participants reported that they perceived their hair to have improved quality after 6 months, with another one reporting the same after 9 months. One person observed thickening of the hair (after 9 months), one reported new undergrowth (after 6 months) and one person reported accelerated hair growth (after 3 months). Undergrowth is the growth of short, fine hairs underneath longer hair.
So, not very convincing. We have measurements of hair diameter thickening but no data showing any increase in growing hairs or reduction in non-growing hairs. Moreover, the reported ‘positive’ data is almost entirely based on subjective patient self-reporting.
The safety data however does generally follow the same results as with the previous study on men, with no patients reporting adverse side effects.
The blood chemistry data was within normal parameters throughout the study (measured at 3, 6, and 9 months) and there was no presence of fluridil or its by-products in the serum of any of the participants.
With regards to testosterone levels and sexual hormone binding globulin (SHBG), the researchers found no statistically significant differences between measurements taken at baseline and 9 months of treatment. There were however patients with higher than the physiological range of SHBG, which has been attributed to the fact that 8 out of 9 of the final patients were taking the combined oral contraceptive pill, which is known to increase SHBG. [22]Amiri, M., Tehrani, F.R., Nahidi, F., Kabir, A., Azizi, F. (2018). Comparing the Effects of Combined Oral Contraceptives Containing Progestins with Low Androgenic and Antiandrogenic Activities on the … Continue reading

Figure 9: SHBG and Testosterone levels at baseline and 9 months. Adapted from: [23]Kucerova, R., Bienova, M., Novotny, R., Fiuraskova, M., Hajduch, M., Sovak, M. (2006). Current Therapies of Female Androgenetic Alopecia and Use of Fluridil, a Novel Topical Antiandrogen, Scripta … Continue reading
So, why didn’t fluridil work in the same way for women as it did for men? Well, the researchers attribute this to the fact that the participants were taking cyproterone acetate (aka Diane 35) another anti-androgen, and (in some cases) contraceptive at least 3 months previous to the study. They determined that because they were taking Diane 35, it can be assumed that there was a sufficient anti-androgenic effect being exerted and so fluridil could not provide a further effect.
But this is just one of several other problems with this study, such as:
- Small participant number
- No placebo
- Participants had been taking medication that may interfere with the efficacy of fluridil
Overall, we cannot conclude that fluridil has any real beneficial effect for women with AGA.
Is Fluridil safe?
Within the limited parameters of the published studies, fluridil doesn’t appear to have any treatment-related side effects. Furthermore, unlike taking oral anti-androgenic medications, fluridil should work only at the point of application and not have effects anywhere else in the body, due to its ability to degrade when it comes into contact with water.
However, fluridil has not been approved by the FDA or the European Medicines Agency as an anti-androgenic medication and is only approved for use in Europe as a cosmetic. The long-term effects of using fluridil are completely unknown.
Is Fluridil for me?
You may want to try fluridil if you:
- Are male with AGA.
- Want to either maintain the current status of hair loss or see short-term improvement and then a plateau.
- Are comfortable with using a product that has no FDA or EMA approval.
- Have no issues using a product that has very little recent (or otherwise) efficacy or safety data.
- Are ok with reducing hair washing to around once or twice a week.
- Have perhaps seen positive results with other anti-androgens (such as finasteride)
Whilst the previously mentioned points (easily degradable and topical application) may prove appealing, we cannot currently recommend using fluridil until more data becomes available. If you want to take the risk, however, it is possible that you may see some limited benefits.
References[+]
References ↑1 Seligson, A.L., Campion, B.K., Brown, J.W., Terry, R.C., Kucerova, R., Bienova, M., Hajduch, M., Sovak, M. (2003). Development of Fluridil, a Topical Suppressor of the Androgen Receptor in Androgenetic Alopecia. Drug Development Research. 59, 292-306. Available at: https://doi.org.10.1002/ddr.10166 ↑2 Fujita, K., Nonomura, N. (2019). Role of Androgen Receptor in Prostate Cancer: A Review. The World Journal of Men’s Health. 37(3), 288-295. Available at: https://doi.org/10.5534/wjmh.180040 ↑3, ↑6, ↑11, ↑12 Seligson, A.L., Campion, B.K., Brown, J.W., Terry, R.C., Kucerova, R., Bienova, M., Hajduch, M., Sovak, M. (2003). Development of Fluridil, a Topical Suppressor of the Androgen Receptor in Androgenetic Alopecia. Drug Development Research. 59, 292-306. Available at: https://doi.org.10.1002/ddr.10166 ↑4 Solomon, K., Velders, G., Wilson, S., MAdronich, S., Longstreth, J., Aucamp, P., Bornman, J. (2016). Sources, Fates, Toxicity and Risks of Trifluoroacetic Acid and its Salts: Relevance to Substances Regulated Under the Montreal and Kyoto Protocols. Journal of Toxicology and Environmental Health. 43(15-16), 597-603. Available at: https://doi.org/10.1080/10937404.2016.1175981 ↑5 Urine pH. (no date). University of Nottingham. Available at: https://www.nottingham.ac.uk/nmp/sonet/rlos/bioproc/kidneydrug/page_six.html (Accessed: 22 January 2022) ↑7 Ho, C.H., Sood, T., Zito, PM. (2022). Androgenetic Alopecia. StatPearls [Internet]. Treasure Island (FL). Available at: https://www.ncbi.nlm.nih.gov/books/NBK430924/. (Accessed: 22 January 2023) ↑8 Iverson, P., Melezinek, I., Schmidt, A. (2002). Nonsteroidal antiandrogens: a therapeutic option for patients with advanced prostate cancer who wish to retain sexual interest and function. BJUI International. 87(1), 47-56. Available at: https://doi.org/10.1046/j.1464-410x.2001.00988.x ↑9 Ustuner, E.T. (2013). Cause of Androgenic Alopecia: Crux of the Matter. Plastic and Reconstructive Surgery. Global Open. 1(7), e64. Available at: https://doi.org/10.1097/GOX.0000000000000005 ↑10 Miller, E.J., Lappin, S.L. (2022). Physiology, Cellular Receptor. StatPearls [Internet]. Treasure Island (FL). Available at: https://www.ncbi.nlm.nih.gov/books/NBK554403/#_NBK554403_pubdet_ (Accessed: 22 January 2023) ↑13, ↑14, ↑15, ↑16, ↑17, ↑18 Sovak, M., Seligson, A.L., Kucerova, R., Bienova, M., Hajduch, M., Bucek, M. (2002).Fluridil, a Rationally Designed Topical Agent for Androgenetic Alopecia: First Clinical Experience. American Society for Dermatologic Surgery. 28, 678-685. https://doi.org/10.1046/j.1524-4725.2002.02017.x ↑19 Kucerova, R., Bienova, M., Novotny, R., Fiuraskova, M., Hajduch, M., Sovak, M. (2006). Current Therapies of Female Androgenetic Alopecia and Use of Fluridil, a Novel Topical Antiandrogen, Scripta Medica (Brno). 79(1), 35-48 ↑20 Scanning Electron Microscopy. (no date). Nanoscience Instruments. Available at: https://www.nanoscience.com/techniques/scanning-electron-microscopy/ (Accessed: 22 January 2023) ↑21, ↑23 Kucerova, R., Bienova, M., Novotny, R., Fiuraskova, M., Hajduch, M., Sovak, M. (2006). Current Therapies of Female Androgenetic Alopecia and Use of Fluridil, a Novel Topical Antiandrogen, Scripta Medica (Brno). 79(1), 35-48 ↑22 Amiri, M., Tehrani, F.R., Nahidi, F., Kabir, A., Azizi, F. (2018). Comparing the Effects of Combined Oral Contraceptives Containing Progestins with Low Androgenic and Antiandrogenic Activities on the Hypothalamic-Pituitary-Gonadal Axis in Patients with Polycystic Ovary Syndrome: Systematic Review and Meta-Analysis. JMIR Research Protocols, 7(4), e113. https://doi.org/10.2196/resprot.9024 Topical minoxidil is an FDA-approved treatment for male and female pattern hair loss, also known as androgenic alopecia (AGA).
Despite its popularity, not very many people continue using topical minoxidil for the long-run. In fact, one clinical study found that by the one-year mark, 95% of topical minoxidil users voluntarily quit applying the drug – with more than 2/3rds of them citing “low effect” as their rationale.[1]https://pubmed.ncbi.nlm.nih.gov/17917938/
So, what sort of hair regrowth can we expect from minoxidil? Why do so many people quit using the topical? And what can we do to maximize minoxidil’s hair growth-promoting effects, and in doing so, set ourselves up for sustainable hair regrowth years into the future?
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What Is Minoxidil?
Topical minoxidil is the only medication approved by the FDA for the treatment of androgenic alopecia (AGA) in both males and females. Since its use as an anti-hypertensive drug in 1979, researchers have long-noted a nearly universal “adverse event” in oral minoxidil users: unexpected new hair growth along the limbs, chest, face, and scalp.[2]https://pubmed.ncbi.nlm.nih.gov/7030707/
This led to to the reformulation of minoxidil as a topical, and subsequent clinical trials to test its efficacy on treating AGA. In 1988 and 1992, 5% and 2% minoxidil became commercial available as an over-the-counter hair growth treatment for men and women, respectively.
How Does Minoxidil Work?
Researchers aren’t totally sure how minoxidil regrows hair.
Having said that, they suspect that minoxidil may work through at least one (or all) of the following mechanisms:
- Opening potassium ion channels – which increases blood, oxygen, and nutrient transport to balding regions (i.e., increased microcirculation)
- Modulation of prostaglandin analogues (i.e., decreased inflammation)
- Anti-androgenic activity in hair follicle sites (i.e., decreased dihydrotestosterone (DHT) – the hormone causally linked to baldness).
How Much Regrowth Should We Expect From Minoxidil?
Technically speaking, “hair regrowth” isn’t a term specific enough to be meaningful. Are we talking about changes to total hair counts? Changes to hair thicknesses? Increases to terminal hairs? Vellus hairs? Hair density changes? Over what time period: 1 month, 3 months, 5 years? What about the percentage of people who notice increased hair growth versus those who don’t?
Depending on how we define “hair regrowth”, our answers will vary wildly.
For these reasons, our team prefers to use more specific language surrounding hair regrowth. Here are the two metrics we tend to consider most important when evaluating the efficacy of a hair loss treatment option:
- Response Rate. This term can be defined through a question: “Of the people who try this intervention, what percent will see a slowing, stopping, or partial reversal of their hair growth versus a placebo group – and over a reasonable time period?”
- Regrowth Rate. This term’s definition varies depending on the quality of data on an intervention. But in general, it’s the change in an objective hair growth endpoint that closely mirrors the perception of “visual improvements” to hair. For instance, this might be the change in terminal hair counts, hair density (i.e., the ∆ in hair counts x the ∆ in hair thickness), or hair weight (i.e., the difference in the weight of hair shaved off before/after a study was conducted, controlling for hair growth timing).
What Is Minoxidil’s Response Rate?
Despite being an FDA-approved hair growth drug, topical minoxidil’s response rate is as low as 40-60%.[3]https://pubmed.ncbi.nlm.nih.gov/25112173/
This is because topical minoxidil is applied to the scalp as a pro-drug – meaning that it’s inactive. It needs to come into contact with a skin enzyme called sulfotransferase – which is produced by the SULT1A1 gene – in order to active in the skin, and then attach to hair follicles where it can elicit its hair growth-promoting effects.
Unfortunately, upwards of 60% of men and women do not have high enough levels of sulfotransferase in their skin to elicit a response to topical minoxidil.[4]https://pubmed.ncbi.nlm.nih.gov/24283387/
This means that for (potentially) a majority of people who try topical minoxidil, it won’t lead to any hair growth, because not enough of it will activate within the scalp to create an effect on hair growth.
Fortunately, there are ways to enhance minoxidil’s efficacy – and the activity levels of sulfotransferase in the scalp skin. We’ll get into these later in the article.
What Is Minoxidil’s Regrowth Rate?
This depends on a number of factors, including someone’s:
- Gender
- Severity of hair loss
- Genetic variance in the SULT1A1 gene
- The delivery method of minoxidil (oral vs. topical)
- The dosing amount and schedule
- If minoxidil is combined with interventions that might enhance its hair growth-promoting effects (more on this later).
Having said that, if we narrow our definition of Regrowth Rate to changes to “hair weight” occurring over a 1+ year usage period, and we narrow our patient population to healthy men and women who are facing androgenic alopecia, we can use clinical data to set ballpark expectations.
A well-designed study by Price et al. (1999) sought to determine the effect of 2% and 5% topical minoxidil on cumulative hair weight changes throughout 96 weeks of treatment. Compared to the placebo and untreated groups, hair weight changes from 2% and 5% topical minoxidil were 20% and 30% higher for 2% and 5% topical minoxidil users at the 52-week mark, respectively.[5]https://pubmed.ncbi.nlm.nih.gov/10534633/
Here’s a chart summarizing the details (Note: participants withdrew from treatment at the vertical line denoted at week 96):

Price VH, Menefee E, Strauss PC. Changes in hair weight and hair count in men with androgenetic alopecia, after application of 5% and 2% topical minoxidil, placebo, or no treatment. J Am Acad Dermatol. 1999 Nov;41(5 Pt 1):717-21. doi: 10.1016/s0190-9622(99)70006-x. PMID: 10534633.
So, despite that 40-60% of topical minoxidil users don’t respond to treatment, after averaging out all participants’ hair growth results, most studies on topical minoxidil show that overall hair growth results are statistically improved.
This is the big problem with topical minoxidil: its hair growth outcomes are bifurcated.
On the one hand, we have 40-60% of users seeing zero effect from the drug. On the other hand, we have 40-60% of users seeing big amounts of hair growth. These bifurcated results can average a 20-30% cumulative hair weight change at the one-year mark.
Key Takeaway: despite ~50% of people not responding to 2% or 5% topical minoxidil, most studies show statistically significant improvements to hair counts. This is because a subset of participants are often hyper-responders to minoxidil, which bring up the average hair counts for everyone.
Do Minoxidil’s Results Last Long-Term?
Unfortunately, hair regrowth from topical minoxidil is not necessarily as long-lasting as most would hope.
This is because clinical studies also show that, over time, the efficacy of topical minoxidil wanes – meaning that its hair growth-promoting effects diminish over a number of years, even despite keeping users above the placebo group. [6]https://pubmed.ncbi.nlm.nih.gov/12196747/[7]https://pubmed.ncbi.nlm.nih.gov/2180995/
This was already evident in the above study, which showed a trend downward for cumulative changes to hair weights from weeks 52 to 96. And these results are consistent across other studies. Just see the diminishing regrowth results from this 48-week study on 2% and 5% topical minoxidil versus placebo:[8]https://pubmed.ncbi.nlm.nih.gov/12196747/

Olsen, E. A., Dunlap, F. E., Funicella, T., Koperski, J. A., Swinehart, J. M., Tschen, E. H., & Trancik, R. J. (2002). A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men. Journal of the American Academy of Dermatology, 47(3), 377–385.
Moreover, here’s a five-year study tracking topical minoxidil’s efficacy, which seems to wane after year one:[9]https://pubmed.ncbi.nlm.nih.gov/2180995/

Olsen, E. A., Weiner, M. S., Amara, I. A., & DeLong, E. R. (1990). Five-year follow-up of men with androgenetic alopecia treated with topical minoxidil. Journal of the American Academy of Dermatology, 22(4), 643–646.
For more information on these topics, see this article: Minoxidil: How Long Do Results Last (Even After Quitting)?
Factors Affecting Topical Minoxidil’s Ability To Grow Hair
To summarize from the above, topical minoxidil has a response rate of just 40-60%. This is because a large number of users lack enough skin activity of an enzyme known as sulfotransferase – which is used to turn minoxidil into minoxidil sulfate, where the drug can then become active, attach to hair follicle sites, and have a positive impact on hair parameters.
But even with these poor response rates, 2% to 5% topical minoxidil still can improve hair weights by 20-30% over a 52-week period – and lead to modest hair count improvements – a portion of which will lead to cosmetically significant improvements to hair.
This is because the 40-60% of people who do respond to topical minoxidil tend to respond relatively robustly.
Factors affecting minoxidil’s response rates and regrowth rates are person-specific, and depend on (at least) the following:
- The person. Age, gender, hair loss severity, and genetic variations in the SULT1A1 gene
- The drug. Delivery methods (i.e., topical versus oral), along with dosing amounts and schedules (i.e., 5% twice-daily)
- Minoxidil enhancers. Whether minoxidil is used alongside therapies that enhance skin penetration and/or sulfotransferase activity (i.e., retinoic acid and/or microneedling)
This begs the question: if we’re worried we may not respond to minoxidil, how can we enhance the drug’s efficacy?
Fortunately, there are a number of ways to take someone from a non-responder to a great responder.
How Can Minoxidil Results Be Improved?
There are a handful of strategies to improve the effectiveness of minoxidil. If you’re looking for a deep-dive into the science, this article is a great resource.
Otherwise, here are the highlights:
- Increase the dilution of topical minoxidil to 15%. Clinical studies show that suspected non-responders to 2% and 5% minoxidil tend to see robust hair regrowth at higher dilutions ranging from 10% to 15% minoxidil.
- Add in minoxidil enhancers. Retinoic acid (i.e., tretinoin) and microneedling both help increase dermal penetration of minoxidil and active more sulfotransferase.
- Switch to oral minoxidil. Unlike topical minoxidil – which gets sulfated in the skin – oral minoxidil goes through processing in the liver whereby most people have an abundance of sulfotransferase to activate the drug. This leads to dramatically higher response rates – with daily doses of 2.5 mg and higher sometimes promoting 90% response rates in clinical trials.
Many people inside our membership community have used these strategies above to move from minoxidil non-responders to minoxidil hyper-responders. We hope they help you, too.
We hope these recommendations help take your hair growth results to a new level.
References[+]
References ↑1 https://pubmed.ncbi.nlm.nih.gov/17917938/ ↑2 https://pubmed.ncbi.nlm.nih.gov/7030707/ ↑3 https://pubmed.ncbi.nlm.nih.gov/25112173/ ↑4 https://pubmed.ncbi.nlm.nih.gov/24283387/ ↑5 https://pubmed.ncbi.nlm.nih.gov/10534633/ ↑6, ↑8 https://pubmed.ncbi.nlm.nih.gov/12196747/ ↑7, ↑9 https://pubmed.ncbi.nlm.nih.gov/2180995/ How Often Does Topical Finasteride Need To Be Applied?
Most clinicians recommend using topical finasteride at least once daily. However, its minimum viable frequency of application depends on factors such as daily drug exposure and contact time with the scalp.
For those who can keep topical finasteride on their scalps for 10-12 hours (or longer), once-daily applications of low-dose topical finasteride might suffice. For those who can only keep topical finasteride on their scalps for 4-6 hour periods, twice-daily applications may be more helpful – or higher-dose topical finasteride.
After maximum drug saturation has occurred in the scalp (typically after ~30 days of daily applications), it is possible to reduce the frequency of use from once daily to five times weekly – and perhaps even lower – while still seeing hair parameter improvements. However, doing so with low-dose finasteride may come with a reduction in efficacy.
More explanations can be found below.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
Finasteride: How Much Is Enough To Regrow Hair?
Clinical studies have demonstrated a steep, dose-dependent, logarithmic response curve for finasteride’s effects on DHT levels. In other words, a little finasteride reduces almost as much DHT as a lot of finasteride. See this chart:

Clinical studies also show that topical formulations of topical finasteride as low as 0.005% x 1 mL, applied twice daily, can improve hair parameters over 16-month periods.[1]https://www.tandfonline.com/doi/abs/10.3109/09546639709160517
That’s a total daily exposure volume of just 0.1mg daily – or one-tenth that of what is prescribed orally on a daily basis to treat androgenic alopecia (AGA). Needless to say, people with localized hair loss (i.e., just at temples and/or crown) may be able to switch to topical finasteride, reduce their drug exposure, and still see impressive hair growth-promoting effects.
Can Topical Finasteride Be Used Every Other Day?
While usage frequencies lower than once daily haven’t been clinically studied, it’s likely that topical finasteride would still be effective with less frequent dosing schedules.
Why? Because finasteride has a tissue dissociation timing of 4-5 days. In other words, it takes multiple days (and sometimes weeks) for finasteride bound to skin tissue to finally leave that skin tissue and enter the bloodstream, where it is later metabolized and excreted.
Moreover, clinical studies on 1 mg daily of oral finasteride suggest that after one year of use, switching to a 30-days-on, 30-days-off dosing schedule is just as effective as continuing with a once-daily dosing schedule – despite not using the drug for a total of 6 months throughout the same year.[2]https://jaad.org/retrieve/pii/S0190962220319289
For these reasons, finasteride can still have a therapeutic effect on DHT reduction in the scalp skin, even up to ~30 days after quitting the drug.
This is even reflected in withdrawal studies of oral finasteride, which show that blood levels of DHT can still take multiple weeks to rebound to baseline levels prior to starting the drug.[3]https://academic.oup.com/jcem/article/89/5/2179/2844345

Richard V. Clark, David J. Hermann, Glenn R. Cunningham, Timothy H. Wilson, Betsy B. Morrill, Stuart Hobbs, Marked Suppression of Dihydrotestosterone in Men with Benign Prostatic Hyperplasia by Dutasteride, a Dual 5α-Reductase Inhibitor, The Journal of Clinical Endocrinology & Metabolism, Volume 89, Issue 5, 1 May 2004, Pages 2179–2184
The same pharmacokinetic relationships also apply to topical finasteride – provided that enough finasteride has saturated the scalp skin to match the levels of exposure in these oral finasteride withdrawal studies.
For a deeper dive into the pharmacokinetics supporting alternate doses and dosing schedules for finasteride, see these articles:
- How Often Should I Take Oral Finasteride?
- How Long Does Finasteride Stay In The Bloodstream?
- How Long Does Finasteride Remain In Scalp Tissues?
What About Scalp Contact Time?
In most cases, the longer a topical sits on the scalp skin, the better chance it has of absorbing into the skin, where it can positively impact hair follicles.
When it comes to topical finasteride, in vitro studies have measured skin absorption rates of the drug over a 24-hour period, and versus different topical formulations – such as finasteride paired with carrier ingredients such as ethosomes, alcohol, liposomes, or water.
The relationships change depending on the finasteride formulation. Just see this chart from the following study:[4]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2977015/

Penetration profiles of finasteride permeating through human skin from different preparations (mean ± SD, n = 4)
This chart suggests that absorption of topical finasteride is linear across time. In other words, the longer you leave in topical finasteride, the more of it will absorb into your scalp skin – with no diminishing returns over a 24-hour period.
Moreover, these results reveal that across the same time period, those using liposomal finasteride will absorb up to 30% less finasteride into the skin versus those using alcohol-based finasteride – and across the same time period.
This might explain why there are anecdotal reports of fewer side effects while on liposomal finasteride: less of it is getting into the scalp skin, and thereby less of it is leaching into the bloodstream and causing systemic effects. It causes fewer side effects, because it is perhaps less effective.
Additionally, liposomal finasteride users may need to let their topical sit for twice as long on the scalp to reach the same level of absorption as those using alcohol-based finasteride.
To illustrate this, look at the level of absorption for liposomal finasteride at 22 hours. It’s nearly the same as the level of absorption for hydroethanolic finasteride at 10 hours.
Finally, we also have (at least) three other variables at play that will affect finasteride absorption rates, and thereby the frequency at which we should apply topical finasteride on a daily or weekly basis:
- The total dilution of finasteride (i.e., 0.005%, 0.025%, 0.1%, etc.)
- The mL per application (i.e., 1 mL for those with localized hair loss, or 2 mL for those with diffuse hair loss)
- The application frequency (i.e., twice-daily, once-daily, once every-other-day, etc.)
For an example of how important these factors are, just see the results of this 2014 study exploring the effects of once- versus twice-daily dosing of topical finasteride on serum DHT levels:[5]https://pubmed.ncbi.nlm.nih.gov/25074865
Caserini, M., Radicioni, M., Leuratti, C., Annoni, O., & Palmieri, R. (2014). A novel finasteride 0.25% topical solution for androgenetic alopecia: pharmacokinetics and effects on plasma androgen levels in healthy male volunteers. International journal of clinical pharmacology and therapeutics, 52(10), 842–849.
As we can see from the following chart, a doubling of the daily dose had a dramatic effect on serum DHT reductions.
Which Factors Influence How Often We Can Use Topical Finasteride?
If it isn’t already obvious, it’s impossible to answer the question, “Can I use topical finasteride less than once-daily?” without more context.
Each of the variables we’ve mentioned is critically important, because minor differences in any variable can dramatically change your total weekly finasteride exposure, and thereby the actual effectiveness of the drug.
This is particularly important for those who are trying to build a topical finasteride application schedule that prevents inadvertent exposure to family members, or for those who are opting for topical finasteride to lower their risk of side effects.
So, here’s a recap of the five critical factors influencing how much topical finasteride will actually penetrate into the scalp skin:
- Topical Dilution (i.e., % finasteride). The higher the dilution, the less frequently you need to apply topical finasteride.
- Carrier Vehicles (i.e., liposomes, alcohol, etc.). Liposomal vehicles are significantly less effective versus alcohol.
- Application Dose (i.e., how many mL you apply each time). The higher the mL applied, the more drug exposure.
- Application Frequency (i.e., how often you apply). The more frequent the application, the more drug exposure.
- Scalp Contact Time (i.e., how many hours before washing out?). This is influenced by your % dilution and carrier vehicles.
Moreover, there’s a sixth factor that hasn’t yet gotten discussed: adjuvant treatments alongside topical finasteride.
If you’re combining topical finasteride with other ingredients or therapies that augment skin penetrability – i.e., retinoic acid, topical corticosteroids, or even microneedling – then you can expect more of the drug to penetrate the skin over the same time period.
That’s because these therapies wear down the stratum corneum (i.e. the outermost layer of skin), decrease the side of the epidermis, or create channels into the dermis for better drug penetration – all of which influence topical drug absorption.
What’s The Minimum Days Per Week I Can Apply Topical Finasteride?
To reiterate: the answer depends entirely on your topical dilution, carrier vehicles, application dose, how long you leave in that topical before washing it out, and your use of adjuvant therapies alongside topical finasteride.
Moreover, if someone isn’t experiencing side effects from finasteride, or if someone isn’t trying to limit other household members’ inadvertent exposure to the drug, then it doesn’t make much sense to adopt an alternate dosing schedule. It just introduces a level of complexity to your life that is, largely, unnecessary.
Nonetheless, if you are troubleshooting side effects, trying to limit a loved one’s inadvertent exposure to the drug, or simply traveling and wondering how long you can stop using topical finasteride before your hair starts falling out, you can lower your dosing frequency without necessarily hurting your hair gains.
The exact strategy will depend on why you’re doing this. For instance:
- If you’re troubleshooting side effects, you’ll likely want to lower your total weekly drug exposure. This is because total finasteride exposure is tied to side effect risks.
- If you don’t have any side effects, but you’re just trying to limit the amount of time you’re wearing topical finasteride around a partner, pregnant person, or family member – you may not want to lower your total weekly drug exposure. Instead, you may want to increase the dilution of your finasteride by a factor of 2x or more, but decrease the amount of time you wear in-the-house by washing it out more frequently, or only applying it on certain days of the week.
- If you don’t want to take topical finasteride with you on a vacation, chances are you can stop using it for 1-2 weeks (or more) without seeing much of a negative effect. After all, oral dosing studies showed that every-other-month daily doses were just as effective as every-month daily doses in the second year of use. Just make sure you reach scalp skin saturation points for finasteride before opting for this strategy – which you can likely achieve after ~30 days worth of applications.
How Much Topical Finasteride to Apply Daily
If you are opting for daily use of topical finasteride, regardless of the delivery vehicles, here are a few rules-of-thumb to consider:
- Leave for as long as possible on the scalp (If exposure is ≤ 0.1 mg daily and/or if applying less frequently than once daily). This includes a minimum of 10-12 hours, and preferably longer, before washing finasteride out of the scalp skin.
- Stick with 6-12 hour contact windows (if using twice daily)
We hope this article helps! If you’d like personal advice troubleshooting topical finasteride formulations, our research team is happy to support you inside our membership community.
References[+]
In this article, we’ll explore the history of minoxidil, how it became a hair loss drug, and the debate over its mechanisms of action for hair growth.
Despite decades of study, researchers still do not know how minoxidil promotes hair growth. But they do have some ideas, and these ideas have remained the subject of significant debate – even 70 years after the discovery of the drug.
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What Is Minoxidil?
Minoxidil is a drug that was originally developed in the 1950’s by Upjohn Company, which later became a part of Pfizer. In early experiments, minoxidil consistently improved vasodilation in animals, which led to human trials as a potential treatment for hypertension (i.e., high blood pressure).
In 1979, the FDA approved the use of oral minoxidil as a treatment for hypertension. But during its clinical trials and post-marketing studies, “nearly all” oral minoxidil users reported excessive hair growth as a side effect – and even the development of new hair along the face, chest, back, and scalp.[1]https://pubmed.ncbi.nlm.nih.gov/7030707/
This led to the reformulation of minoxidil as a topical, followed by clinical studies to evaluate topical minoxidil’s effectiveness in men and women facing androgenic alopecia (AGA) – one of the world’s most common hair loss disorders.
Throughout the 1980’s, a series of clinical studies consistently demonstrated that topical minoxidil was able to improve hair counts, increase hair thickness, and reduce hair shedding in male and female hair loss sufferers. And in 1988 and 1992, topical minoxidil at 5% and 2% formulations were approved by the FDA for male and female pattern hair loss, respectively.[2]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6691938/
How Does Minoxidil Work?
Despite decades of study, it’s still unclear exactly how minoxidil improves hair growth.
In animal studies, topical minoxidil has been shown to shorten the telogen (rest) phase of the hair cycle and stimulate the initiation of the anagen (active) stage of the hair cycle.[3]https://pubmed.ncbi.nlm.nih.gov/14996087/ These effects also consistently translate to humans using minoxidil (oral and topical) to treat AGA. But despite knowing what minoxidil does to most hair follicles, researchers still aren’t exactly sure of the mechanisms governing the hair growth improvements.
With that said, investigation groups do have some ideas what might be going on. In particular, there are (at least) three suspected ways minoxidil might regrow hair: its activity as a vasodilator, as well as its anti-inflammatory and anti-androgenic effects.
We’ll explore arguments for and against each hypothesis – all to elucidate why there’s still debate.
Hypothesis #1: Vasodilation (i.e, Increased Blood Flow)
The hypothesis: minoxidil improves blood, oxygen, and nutrient transport to balding hair follicles – which stimulates more robust hair growth.
Argument For
Minoxidil opens potassium ion channels, which improves circulation in microvascular networks. These potassium channels are located in a variety of places – including the muscles of peripheral arteries and within and nearby the hair follicles themselves.[4]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6691938/[5]https://faseb.onlinelibrary.wiley.com/doi/epdf/10.1096/fj.07-099424
The human scalp has a broad network of blood vessels, and is considered one of the most densely vascularized regions of the body. However, as AGA progresses, balding scalp regions undergo a loss of blood supply. For instance, clinical studies have shown 40% declines in transcutaneous oxygen levels in frontal balding regions versus non-balding controls.[6]https://pubmed.ncbi.nlm.nih.gov/8628793/ Similarly, another study found that subcutaneous blood flow is 2.6x lower in balding versus non-balding scalps.[7]https://www.jidonline.org/article/0022-202X(89)90189-9/pdf
Whether reduced blood supply is a cause or effect of the balding process is still debated – with research groups arguing both sides. However, current consensus is that if blood flow is causally linked to pattern hair loss, it is probably a secondary contributor to the balding process – rather than its root cause.
So, if minoxidil increases blood vessel diameters by opening potassium ion channels, more blood, oxygen, and nutrients might reach hair follicles and thereby lead to more robust hair growth.[8]https://pubmed.ncbi.nlm.nih.gov/22409453/
Studies using Doppler devices (a measurement tool for blood flow) showed that minoxidil appears to do this. Specifically, minoxidil improve microvascular vasodilation in skin tissues supporting hair follicles, and that these improvements coincide with hair growth.[9]https://pubmed.ncbi.nlm.nih.gov/10233226/
Other studies have found that minoxidil application grows new blood vessel openings surrounding the hair follicles themselves – a term known as fenestration.[10]https://pubmed.ncbi.nlm.nih.gov/10233226/ Fenestration is a process supporting angiogenesis, or the growth and formation of new blood vessel networks.
Therefore, mechanistic, animal, and clinical data all suggest that minoxidil might work by improving blood flow to balding regions – and that this might be the main mechanism by which minoxidil regrows hair.
Argument Against
There are three main counterarguments to the idea that minoxidil might regrow hair by improving blood flow to balding regions:
1. Reduced blood flow is likely a consequence of androgenic alopecia, rather than a cause.
While minoxidil might increase blood flow, reductions to blood flow are not considered to be the fundamental driver of AGA. Instead, the evidence most strongly supports that the overwhelming majority of reductions to blood flow that occurs during the progression of AGA is a consequence of hair cycle-mediated hair follicle miniaturization, rather than a cause of hair loss.Because of the conflation of cause-and-effect, improving circulation to thinning regions cannot be the main way in which minoxidil regrows hair – much like an increase in ice cream sales is not the cause of more shark attacks, despite both being correlated. Instead, there must be some other unidentified variable at play (in the case of ice cream sales and shark attacks, it’s “nice weather”).Therefore, minoxidil must be working to regrow hair through some other mechanism outside of increased blood flow.
2. If minoxidil works primarily by increasing blood supply, why don’t other vasodilating medications also regrow hair?
If increasing blood circulation were truly a plausible treatment target for androgenic alopecia, why don’t other antihypertensive medications regrow hair? Why is it only minoxidil?This is further evidence that minoxidil probably doesn’t work primarily through increasing blood supply to miniaturized hairs. There must be some other mechanism at play.
3. Minoxidil has other suspected mechanisms beyond circulation enhancements.
These mechanisms include, but are not limited to, prostaglandin modulation and anti-androgenic effects – the latter of which is far closer to the suspected root cause of androgenic alopecia: dihydrotestosterone (DHT), a hormone that is causally associated with the balding process.
Altogether, these three arguments form the basis by which some people reject the idea that minoxidil works primarily through increasing blood supply. But – as is the case with many topics in hair loss research – the science isn’t completely settled, because there also counterpoints to each of the above counterarguments.
Rebuttals
While the case against minoxidil working through vasodilation might appear strong, there are also compelling rebuttals to each of the counterpoints raised.
1. “Reduced blood flow is likely a consequence of androgenic alopecia, rather than a cause.”
This can be true, and simultaneously, it can also be true that targeting secondary contributors to AGA – like reductions to blood supply – can still promote hair growth.This has even been demonstrated in the context of human hair loss, whereby targeting to reduce factors such as inflammation in the infundibulum (which is believed to be partly caused by microorganisms) and/or inflammation near the dermal papillae (which is believed to be driven by the hormone DHT) in AGA patients can still improve hair growth outcomes – even without necessarily resolving the root cause(s) of that inflammation.Moreover, despite minoxidil being an FDA-approved to treat AGA, its effects on hair growth are relatively mild – particularly in the long-run – whereby hair density improvements from minoxidil start trending downward after the first year of use. The steepness of minoxidil’s downward slope is not matched by other treatments like finasteride, which directly lower scalp DHT levels and, in doing so, lead to longer-term hair gains – probably because of the drug’s ability to address factors closer to the “root cause” of AGA.
Therefore, minoxidil’s mild and long-run diminishing effects on hair growth actually support the idea that the drug targets an accelerator or secondary contributor to the balding process – rather than something closer to its root cause. There is enough alignment in mechanistic, animal, and clinical data on minoxidil to suggest that this might be increased blood supply via fenestration of vascular networks nearby hair follicles.
2. “If minoxidil works primarily by increasing blood supply, why don’t other vasodilating medications also regrow hair?”
Other anti-hypertensive medications do improve hair growth in humans. So at the outset, this counterargument makes no sense.Studies have shown that medications like diazoxide and pinacidil also increase blood flow by opening the same potassium ion channels as minoxidil, and also promote hair growth in humans.[11]https://faseb.onlinelibrary.wiley.com/doi/epdf/10.1096/fj.07-099424[12]https://www.karger.com/Article/Pdf/248368[13]https://journals.lww.com/cardiovascularpharm/abstract/1988/12002/clinical_pharmacology_of_pinacidil,_a_prototype.8.aspx[14]https://www.sciencedirect.com/science/article/pii/S0022202X9290089M
This is important, because it suggests that the mechanism of vasodilation – i.e., opening potassium ion channels – likely matters for hair growth. Because in mechanistic and animal studies, vasodilation stimulated by opening potassium ion channels seems to also enhance the vasculature surrounding the hair follicles and the fenestration of microvascular networks, whereas other vasodilating medications working through other mechanisms might not achieve the same effect.
This is because other anti-hypertensive medications do not all target potassium ion channels. Therefore, other anti-hypertensive medications will not always have the same magnitude of effect on vasodilation as minoxidil, nor will they always influence vasodilation in areas relevant to hair growth – like the microvascular regions of the scalp skin.
For an example, just see our article on peppermint oil for hair growth – in which we reviewed research showing that menthol (which is widely labeled as a “vasodilator”) happens to cause vasodilation in the vascular endothelium but vasoconstriction in vascular smooth muscle tissues.
This degree of specificity matters, but the nuance tends to get left behind by people blindly assuming that all vasodilation medications must improve hair growth in order for vasodilation to be a worthy mechanism of action by which minoxidil might work.
That’s not a reasonable assumption. Depending on the medication, dosing schedule, delivery method, and regions of application – anti-hypertensive compounds can have a range of blood flow-related effects across organ sites, arteries, veins, and microvascular networks – some of which are paradoxical.
3. “Minoxidil has other suspected mechanisms beyond circulation enhancements.”
This is true. It is also true that these mechanisms might also contribute to minoxidil’s hair growth-promoting effects. However, these mechanisms of action remain speculative, and they are supported by low-quality studies (and conflicting research) regarding their plausibility.Therefore, the existence of this speculation does not disprove the possibility that minoxidil might still work through vascular fenestration of AGA-affected hair follicles. All mechanisms can simultaneously contribute to hair growth; there need not be a “one versus the other” mentality.
Hypothesis #2: Prostaglandin Modulation
The hypothesis: minoxidil modifies prostaglandin activity, and in doing so, reduces inflammation in balding regions.
Argument For
Prostaglandins are fatty acid derivatives that come from our ingestion of omega 6 fatty acids. These lipid derivatives can have hormone-like effects on the body, and are often involved in inflammatory processes. Specifically, prostaglandins tend to increase in response to tissue damage or infection – with different prostaglandins playing roles in both inflammation generation and inflammation resolution.
In 2012, a renowned research team from the University of Pennsylvania demonstrated that prostaglandin D2 (PGD2) and prostaglandin J2 (PGJ2) were elevated in balding regions, and that in mouse models, prostaglandin D2 inhibited hair lengthening.[15]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3319975/[16]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3982925/
Moreover, research from more than a decade prior had demonstrated that minoxidil appears to enhance the activity of prostaglandins associated with the growth phase of the hair cycle, and perhaps dampen prostaglandins associated with hair loss.[17]https://pubmed.ncbi.nlm.nih.gov/9008235/
For these reasons, some researchers now believe that prostaglandin modifications are perhaps one of the ways in which minoxidil might regrow hair. In modifying prostaglandin activity, minoxidil might lower inflammation within certain hair follicle sites and, in doing so, improve hair growth outcomes.
Argument Against
When Garza et al.’s 2012 study on prostaglandin D2 was published, hair loss forums were enthralled with the possibility of developing and/or repurposing a new class of treatments for AGA: prostaglandin analogues. Excitingly, a drug developed to inhibit prostaglandin D2-mediated inflammation – setipiprant – was already undergoing clinical trials to treat asthma. As such, the drug developers repurposed the drug and began a clinical trial to see if it would also help fighting hair loss from AGA.
In 2021, the clinical trial evaluating setipiprant as a hair loss treatment was quietly published, and without a major press release. The results: the drug was well tolerated, but it did not work. Specifically, it produced no statistically significant effects on hair parameters versus the placebo group, whereas the study’s positive treatment-control group (who were taking oral finasteride) saw improvements to hair counts throughout the duration of the study.[18]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8526366/
Over the last two decades, other drugs with prostaglandin-modulating activities have also been tested to treat AGA – such as latanoprost and bimatoprost. While some clinical studies show a mild effect, these studies are poorly designed: they tend to have small sample sizes and poor methods (or no methods) of randomization for participants; they tend to include participants with other hair loss disorders in addition to AGA; and they tend to show relatively low response rates across participants, despite some endpoints achieving statistical significance.[19]https://my.perfecthairhealth.com/courses/latanoprost/ This makes it difficult to ascertain any true effects on prostaglandin modulation for AGA – if any.
Finally, follow-up studies conducted by Garza et al. (and other research groups) have actually found conflicting results regarding the presence of prostaglandins throughout the progression of AGA – with some studies showing elevated pro-inflammatory and anti-inflammatory prostaglandin levels only during specific stages of the hair cycle or specific stages of AGA’s progression.[20]https://pubmed.ncbi.nlm.nih.gov/33854354/
Altogether, these findings have significantly dampened excitement surrounding prostaglandin activity as an effective treatment target for AGA.
Rebuttals
Much like it is irresponsible to group together all anti-hypertensive medications as having the same effects on hair growth, we must also not make the same mistake by lumping together all prostaglandin analogues – setipiprant, latanoprost, bimatoprost, minoxidil, and more.
In other words, just because setipiprant failed its phase II clinical trials on AGA, and just because latanoprost appears to be inferior to minoxidil in terms of hair growth, this does not automatically mean that we can dismiss the possibility of prostaglandin modification as a potential treatment target for AGA, nor can we fully dismiss the idea that minoxidil does not work through prostaglandin modification.
Hypothesis #3: Androgen Receptor Antagonization
The hypothesis: minoxidil may reduce androgen activity in the scalp skin, and in doing so, regrow hair.
Argument For
An in vitro study published in 2014 suggested that minoxidil might make androgen receptor pathways less stable – thereby acting as a mild androgen receptor antagonist and/or anti-androgen (at least in cell culture studies).[21]https://pubmed.ncbi.nlm.nih.gov/24742982/
Overwhelming evidence implicates the hormone DHT as causally associated with the balding process. Drugs like finasteride lower DHT levels in the scalp, and in doing so, consistently improve AGA outcomes across dozens of studies spanning tens of thousands of participants.
If the results of this in vitro study hold true in vivo, this would suggest that minoxidil might help lower hormones in the scalp that are causally associated with the balding process. In doing so, minoxidil might actually target hormonal causes of hair loss – even though the drug isn’t believed to change hormonal profiles in the (serum) blood or elicit significant anti-androgenic effects elsewhere throughout the body.[22]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6691938/
Argument Against
This 2014 in vitro study conflicts with other studies exploring whether minoxidil has anti-androgenic effects.
For instance, a 1987 study and a 2017 study both found that minoxidil doesn’t appear to affect androgens – with the latter study suggesting that minoxidil may even enhance androgenic activity in the scalp.[23]https://pubmed.ncbi.nlm.nih.gov/3800423/[24]https://pubmed.ncbi.nlm.nih.gov/30064598/
Therefore, it can just as easily be argued that minoxidil enhances androgenic activity in the scalp skin, rather than inhibits it.
Rebuttals
To our knowledge, there aren’t any strong rebuttals to these counterpoints. With such little evidence existing on this subject – and with the existing studies finding conflicting results – the jury is still out on whether minoxidil has any anti-androgenic effects at all.
Final Thoughts
The way in which minoxidil grows hair is still up for debate.
To date, there are (at least) three leading hypotheses, all of which have their problems:
- Increased microcirculation to balding regions through vascular fenestration
- Prostaglandin modulation – specifically related to PGE2
- Anti-androgenic activity
What’s important to note is that there is not enough evidence to dismiss any of these suspected mechanisms. As such, all of them are still in the running, and all of them might contribute toward minoxidil hair growth-promoting effects.
With more research, we’ll hopefully have a final answer. And if we ever do, we’ll update this article with more information.
References[+]
References ↑1 https://pubmed.ncbi.nlm.nih.gov/7030707/ ↑2, ↑4, ↑22 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6691938/ ↑3 https://pubmed.ncbi.nlm.nih.gov/14996087/ ↑5, ↑11 https://faseb.onlinelibrary.wiley.com/doi/epdf/10.1096/fj.07-099424 ↑6 https://pubmed.ncbi.nlm.nih.gov/8628793/ ↑7 https://www.jidonline.org/article/0022-202X(89)90189-9/pdf ↑8 https://pubmed.ncbi.nlm.nih.gov/22409453/ ↑9, ↑10 https://pubmed.ncbi.nlm.nih.gov/10233226/ ↑12 https://www.karger.com/Article/Pdf/248368 ↑13 https://journals.lww.com/cardiovascularpharm/abstract/1988/12002/clinical_pharmacology_of_pinacidil,_a_prototype.8.aspx ↑14 https://www.sciencedirect.com/science/article/pii/S0022202X9290089M ↑15 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3319975/ ↑16 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3982925/ ↑17 https://pubmed.ncbi.nlm.nih.gov/9008235/ ↑18 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8526366/ ↑19 https://my.perfecthairhealth.com/courses/latanoprost/ ↑20 https://pubmed.ncbi.nlm.nih.gov/33854354/ ↑21 https://pubmed.ncbi.nlm.nih.gov/24742982/ ↑23 https://pubmed.ncbi.nlm.nih.gov/3800423/ ↑24 https://pubmed.ncbi.nlm.nih.gov/30064598/ Oral finasteride is a drug that helps lower levels of dihydrotestosterone (DHT) – the hormone causally associated with androgenic alopecia (AGA). Since 1997, the FDA has approved oral finasteride at 1 mg daily doses to treat AGA.[1]https://www.ncbi.nlm.nih.gov/books/NBK513329/
Having said that, clinical studies also suggest that daily doses of finasteride as low as 0.2 mg can reduce nearly as much DHT as 1.0 mg daily, and lead to similar hair count improvements.[2]europepmc.org/article/med/15319158
For these reasons, many finasteride users have wondered why physicians routinely prescribe 1 mg pills when they can potentially reap the same hair gains with 0.2 mg, or 1/5th the total drug exposure.
In this article, we’ll explore the science behind finasteride’s dosing, and if alternate dosing schedules make sense.
Interested in Oral Finasteride?
Oral finasteride & minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What’s the Ideal Oral Finasteride Dosage For Hair Growth?
In pharmaceutical settings, ideal doses are determined based on the perfect intersection whereby a drug maximizes benefit while minimizing side effects. For finasteride, that would be the dose that maximizes DHT reduction (and thereby hair regrowth) while minimizing the risk of adverse events.
To determine what this dose is, investigators must conduct a range of dosing studies on finasteride for the treatment of AGA – and then measure hair parameter outcomes against any perceived side effects.
Luckily for us, these studies have already been conducted.
Finasteride’s dose-dependent effects on serum DHT
Finasteride is a drug that lowers levels of the hormone DHT – which is causally linked to the balding process in men and women with androgenic alopecia.
A 1999 study sought to determine the effects of finasteride on DHT levels in the blood and scalp, depending on the dose someone took: 0.01 mg, 0.2 mg, 0.05 mg, 1.0 mg, or 5.0 mg.[3]https://pubmed.ncbi.nlm.nih.gov/10495374/
The investigators found that finasteride had what’s known as a logarithmic, dose-dependent effect on DHT reduction. That’s just a fancy way of saying that a little finasteride had nearly the same effect on DHT as a lot of finasteride – and that with higher doses, the marginal reduction of DHT got smaller and smaller.

Serum DHT Reductions vs. Finasteride Dosages
For instance, the above chart shows that while 0.01 mg daily of finasteride barely reduces any DHT, 0.2 mg daily reduces almost as much as DHT as 5 mg daily – even though 5 mg of finasteride 25x higher than the 0.2 mg dose.
Thus, the investigators concluded:
“In this study, doses of finasteride as low as 0.2 mg per day maximally decreased both scalp skin and serum DHT levels. These data support the rationale used to conduct clinical trials in men with male pattern hair loss at doses of finasteride between 0.2 and 5 mg.”
Interestingly, finasteride’s phase III clinical trials (which granted the drug FDA approval) tested a dose of 1 mg daily – and with impressive results on hair count parameters and a relatively low rate of reported side effects versus placebo.[4]https://pubmed.ncbi.nlm.nih.gov/9777765/
But what about lower daily doses of finasteride? Might those also work to regrow hair – all while reducing drug exposure and perhaps side effects?
According to small clinical studies, yes – albeit with caveats.
Finasteride: dose-dependent effects on hair counts & side events
While the evidence is limited, there have been a handful of small clinical trials comparing different daily doses of finasteride on hair counts (and side effects) in men with androgenic alopecia.
One study tested daily doses of finasteride at 0.01 mg, 0.2 mg, 1.0 mg, and 5.0 mg versus placebo for 1-2 years. The researchers found that doses at or above 0.2 mg daily were effective at regrowing hair versus placebo, but that doses of 1.0 mg to 5.0 mg were directionally superior versus 0.2 mg doses.[5]https://pubmed.ncbi.nlm.nih.gov/10495375/
Just see this chart for a breakdown of the numbers:

Roberts JL, Fiedler V, Imperato-McGinley J, Whiting D, Olsen E, Shupack J, Stough D, DeVillez R, Rietschel R, Savin R, Bergfeld W, Swinehart J, Funicella T, Hordinsky M, Lowe N, Katz I, Lucky A, Drake L, Price VH, Weiss D, Whitmore E, Millikan L, Muller S, Gencheff C, et al. Clinical dose ranging studies with finasteride, a type 2 5alpha-reductase inhibitor, in men with male pattern hair loss. J Am Acad Dermatol. 1999 Oct;41(4):555-63. PMID: 10495375.
Moreover, here’s a chart visualizing the differences in hair counts across the full two years:

Roberts JL, Fiedler V, Imperato-McGinley J, Whiting D, Olsen E, Shupack J, Stough D, DeVillez R, Rietschel R, Savin R, Bergfeld W, Swinehart J, Funicella T, Hordinsky M, Lowe N, Katz I, Lucky A, Drake L, Price VH, Weiss D, Whitmore E, Millikan L, Muller S, Gencheff C, et al. Clinical dose ranging studies with finasteride, a type 2 5alpha-reductase inhibitor, in men with male pattern hair loss. J Am Acad Dermatol. 1999 Oct;41(4):555-63. PMID: 10495375.
So, what about adverse events? That same study concluded:
“The incidence of these side effects with finasteride therapy was generally comparable to that observed with treatment with placebo, and there was no evidence of dose dependency or increased incidence with longer therapy out to 12 months. In addition, these side effects ceased in some patients while they continued to receive finasteride.”
In other words, the authors of the study found that while 1mg daily doses of finasteride produced directionally better – but not statistically significantly better – hair count improvements, these improvements did not come at the expense of a higher rate of side effects.
Thus, the investigators concluded that 1mg daily of finasteride was probably the best dose for treating androgenic alopecia.
Having said that, other studies haven’t shared the exact same conclusions.
For instance, a 2004 study on 414 Japanese men found that 1.0 mg daily doses of finasteride produced “numerically superior” results versus 0.2 mg daily, but that 1.0 mg daily doses also came with a numerically superior risk of side effects.[6]https://www.researchgate.net/publication/8392775_Finasteride_in_the_treatment_of_Japanese_men_with_male_pattern_hair_loss
Similar to the other finasteride dosing study, none of the differences in hair count changes or side effect incidences were statistically significant. Nonetheless, the investigators felt the differences in results were still strong enough to note in the conclusions of their study.
Summary (so far)
Based on the totality of data currently available, this leads us to believe the following:
- DHT reduction. Finasteride daily doses of 0.2 mg, 1.0 mg, and 5.0 mg all reduce nearly the same amount of DHT in the body.
- Hair counts. Compared to 0.2 mg doses, 1.0 mg and 5.0 mg doses of finasteride result in directionally better hair counts over 1-2 years.
- Side effects. Compared to 0.2 mg doses, 1.0 mg and 5.0 mg may also come with a directionally higher risk (or magnitude) of side effects.
So, if we choose to lean into these directional (but not statistically significant) results and believe that lower doses of finasteride come with a lower risk of side effects, the next question becomes: “How infrequently can I use finasteride and still see hair gains?”
Can I Use Finasteride Less Than Once Daily?
The answer depends on a number of factors, including finasteride’s:
- Terminal half-life (i.e., how long it takes for 50% of the drug to become inactivated)
- Tissue dissociation timing (i.e., how long it takes for finasteride to leave skin tissues)
- Biological half-life (i.e., how long it takes for finasteride’s effect on DHT to get cut in half)
We’ve covered these topics in great detail inside the following articles. For more information, please read:
For now, here are the key takeaways from the literature:
- Finasteride has a terminal half-life of 5-7 hours.
- After multiple daily doses, finasteride reaches a tissue dissociation timing of 4-5 days.
- Due to both of the above, finasteride’s effects on DHT suppression can remain for up to 14-30 days after quitting the drug.
On that note, one dosing study on finasteride found that after a year of daily use, every-other-month dosing of 1 mg daily of finasteride was just as effect as once-daily dosing – despite users in the first group using the drug for a total of 6 versus 12 months throughout the same year.[7]https://jaad.org/retrieve/pii/S0190962220319289
Again, this is because finasteride’s effects don’t immediately dissipate upon cessation of the drug. They can last up to 14-30 days from the last dose – at least after reaching a certain saturation point in the body (which often requires a handful of days of use at 1 mg daily).
With all of this in mind, finasteride users who are interested in (1) achieving some hair gains, and (2) minimizing their drug exposure – all in hopes of lowering their risk of side effects – may be able to achieve this by reducing their dosing schedule of finasteride.
Alternate Dosing Schedules For Finasteride
To best conceptualize this, it’s easier to think of finasteride dosing in terms of weekly exposure levels, rather than daily. This is because finasteride’s effects on DHT can accumulate across doses, and because lower doses tend to have a similar impact on DHT as higher doses (up to a point).
For instance, those studies showing statistically equivalent efficacy of 0.2 mg versus 1.0 mg daily of finasteride represented dosing difference of 1.4 mg versus 7.0 mg weekly of finasteride.
So, how can we take into account finasteride’s biological half-life to build an alternate dosing schedule that might help support hair growth, albeit with a lower overall drug exposure?
We can likely do so by trying a finasteride dosing schedule of 0.5 mg, 3x weekly.
For most people, that would involve taking 0.5 mg of finasteride every Monday, Wednesday, and Friday. That’s ~1.5 mg weekly of exposure, which is roughly the same as 0.2 mg daily (or 1.4 mg weekly).
In that regard, you can achieve this by simply getting a standard prescription of finasteride for 1.0 mg daily. Companies like Hims, Keeps, and Roman (no affiliation!) often offer these bundled in 90-day supply.
Then, you can cancel that subscription product, buy a pill cutter, and just cut the pills in half.
You can take one-half pill every Monday, Wednesday, and Friday – which equates to 1.5 pills weekly.
If you received a 90-day supply of 1.0 mg daily of finasteride from any of these companies, this alternate dosing schedule should last you a total of 60 weeks – which is more than a year.
With this alternate dosing schedule, you also reduce your total costs of finasteride treatment to just a few dollars per month. So for those who are financially constrained, it’s potentially a wonderful option.
Whether or not these lower doses actually worsen hair count outcomes or lower side effect risks is still up for debate. Nonetheless, this reduced dosing schedule should – at a minimum – lower your overall drug exposure. For this reason, this alternate dosing schedule is also included as part of our guide on troubleshooting finasteride-related side effects.
We hope this article helps. If you’re looking for personal support on hair growth journey, you can receive personalized support and work with our team of researchers directly inside our membership community.
References[+]
References ↑1 https://www.ncbi.nlm.nih.gov/books/NBK513329/ ↑2 europepmc.org/article/med/15319158 ↑3 https://pubmed.ncbi.nlm.nih.gov/10495374/ ↑4 https://pubmed.ncbi.nlm.nih.gov/9777765/ ↑5 https://pubmed.ncbi.nlm.nih.gov/10495375/ ↑6 https://www.researchgate.net/publication/8392775_Finasteride_in_the_treatment_of_Japanese_men_with_male_pattern_hair_loss ↑7 https://jaad.org/retrieve/pii/S0190962220319289 After quitting finasteride, many users wonder how long they have until:
- The drug leaves the bloodstream
- Hormone levels to return to baseline
- When hair loss will resume
The answers vary slightly from person-to-person, but all relate to how finasteride behaves in the body: its distribution, saturation, tissue binding capacity, metabolism, and excretion. These terms are all related to the pharmacokinetics.
In this article, we’ll dive into the pharmacokinetics of finasteride to answer how long finasteride stays active in the scalp skin. In doing so, we’ll also reveal an alternate dosing strategy that some finasteride users employ to maintain hair gains, but potentially lower their risk or magnitude of side effects.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What Is Finasteride?
Finasteride is an FDA-approved drug for androgenic alopecia (AGA) – one of the world’s most common hair loss disorders in adults.
Finasteride works by blocking the formation of an enzyme called 5α-reductase, which transforms free testosterone into dihydrotestosterone (DHT). An abundance of evidence shows that DHT is causally associated with hair growth cycle disruptions, hair thinning, and hair loss from AGA. Clinical studies also show that finasteride can therapeutically lower DHT and, in doing so, improve AGA outcomes in 80-90% of the men who use it.[1]https://pubmed.ncbi.nlm.nih.gov/9777765/
For these reasons, many consider finasteride to be the gold-standard treatment for AGA.
Unfortunately, as with all drugs, finasteride is also causally linked to side effects in a portion of men and women trying the drug. It’s also contraindicated in women who are planning to become pregnant, already pregnant, and/or breastfeeding – with debate over whether men should stop finasteride prior to conceiving.
For these reasons, some finasteride users choose to stop using the drug for a variety of reasons: (1) troubleshoot side effects, (2) conceive without finasteride detectable in the semen, or (3) just take a break due to travel.
What Happens When Someone Quits Finasteride?
Clinical studies on finasteride also show that once the drug is paused, hair loss eventually presumes and converges back to where a user would’ve been had they never started the drug in the first place.
Just see this chart from a two-year clinical study on men using 1 mg daily of finasteride.[2]https://pubmed.ncbi.nlm.nih.gov/9777765/ In the group labeled Fin → Pbo, users were given finasteride for the first year, and then unknowingly switched into the placebo group from year one to year two. As we can see, hair counts improve up until year one, then decline below baseline by the end of year two:

Kaufman KD, Olsen EA, Whiting D, Savin R, DeVillez R, Bergfeld W, Price VH, Van Neste D, Roberts JL, Hordinsky M, Shapiro J, Binkowitz B, Gormley GJ. Finasteride in the treatment of men with androgenetic alopecia. Finasteride Male Pattern Hair Loss Study Group. J Am Acad Dermatol. 1998 Oct;39(4 Pt 1):578-89. doi: 10.1016/s0190-9622(98)70007-6. PMID: 9777765.
For these reasons, the manufacturers of finasteride often warn users that after quitting the drug, hair loss will resume, and within 3-12 months, any hair gains maintained by the drug will be lost.
But just how long after quitting finasteride will it take for hair loss to resume? The question depends entirely on finasteride’s biological half-life in scalp skin tissues. More specifically, it depends on how long finasteride can continue suppressing DHT levels in the scalp, even after a user has stopped taking it.
Finasteride: Effects On Scalp DHT
To reiterate, DHT is the hormone causally linked to hair loss from AGA. Finasteride can therapeutically lower DHT levels by ~70% throughout the body. At this level of suppression, AGA often stabilizes and some hair regrowth can be achieved.[3]https://pubmed.ncbi.nlm.nih.gov/10495374/
However, when it comes to scalp hair regrowth, DHT reduction is not as important throughout the body as it is in the scalp.
After all, several studies from the 1980’s and 1990’s suggest that up to 80% of the DHT found in balding scalps is manufactured at the site of the hair follicle – more specifically, the outer root sheath, dermal papillae cell cluster, and even the mesodermal sheath.[4]https://www.ncbi.nlm.nih.gov/books/NBK557634/[5]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6459338/[6]https://dm5migu4zj3pb.cloudfront.net/manuscripts/113000/113003/JCI87113003.pdf
Therefore, when many people ask, “How long does finasteride stay in the bloodstream?”, they’re mostly asking the wrong question. Instead, they should be asking, “How long does finasteride continue to impact scalp DHT levels – even after quitting the drug?”
The answer to that question depends on finasteride’s:
- Terminal half-life. In other words, how long will it take for 50% of the finasteride ingested to get metabolized and sent to the digestive tract for excretion?
- Tissue dissociation. In other words, how long does it take for active finasteride to “unbind” to those tissues and re-enter circulation and/or get sent to the digestive tract for excretion?
- Biological half-life. In other words, given finasteride’s terminal half-life and tissue dissociation timing, how long will it take for 50% of the drug to stop having its biological impact (i.e., lowering DHT levels)?
The answers will help provide a more nuanced perspective on just how long finasteride stays active in the scalp, and how long someone has before hair loss might presume.
Finasteride Pharmacokinetics
According to pharmacokinetic studies, here’s some key information about finasteride:[7]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3481923/
- Terminal half-life: 5-7 hours, with slightly longer half-lives in older populations
- Tissue dissociation: 4-5 days, meaning that finasteride can remain attached and/or bound to organs for longer than its half-life – which potentiates the drug having a longer-lasting effect than its terminal half-life might suggest
- Biological half-life: 14-30 days, mainly due to its tissue dissociation timings after reaching peak drug distribution and saturation throughout the body (which can happen after only a handful of 1 mg daily ingestions of the drug)
How Long Does Finasteride Impact Scalp DHT Levels?
For most people, finasteride appears to still appreciably lower scalp DHT levels for up to 30 days after quitting the medication.
This was best illustrated in a clinical study measuring blood DHT levels before, during, and after use of finasteride and dutasteride versus a placebo group.[8]https://academic.oup.com/jcem/article/89/5/2179/2844345

Richard V. Clark, David J. Hermann, Glenn R. Cunningham, Timothy H. Wilson, Betsy B. Morrill, Stuart Hobbs, Marked Suppression of Dihydrotestosterone in Men with Benign Prostatic Hyperplasia by Dutasteride, a Dual 5α-Reductase Inhibitor, The Journal of Clinical Endocrinology & Metabolism, Volume 89, Issue 5, 1 May 2004, Pages 2179–2184
Again, the answer is due to how finasteride is stored in organs like the skin. Studies suggest that once finasteride binds to cells within the skin, it has a tissue dissociation timing of 4-5 days.[9]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3481923/
In other words, it can take 4-5 days before the finasteride that has bound to skin cells dissociates from those tissues and reenters the bloodstream for metabolism and excretion.
Interestingly, once finasteride users understand these pharmacokinetics, they can actually use them to their advantage in order to (1) temporarily quit finasteride (if needed), while also (2) preserving hair gains from the drug.
Taking Advantage Of Finasteride’s Tissue Dissociation Timings
Given the relatively long biological half-life of finasteride, many users have wondered, “Can I temporarily quit the drug for any reason, and without sacrificing any of my hair gains?”
So far, clinical studies seem to suggest it’s possible – at least within short-enough cessation periods.
One clinical study on men showed that after one year of taking finasteride, men who switched to a 30-day on, 30-day off dosing schedule for year two achieved comparable hair regrowth to those who continued taking finasteride daily.[10]https://jaad.org/retrieve/pii/S0190962220319289
In other words, these men were able to cut their drug exposure by 50% throughout year two – and take a total of 6 months off the drug – without sacrificing any hair gains versus those taking the drug daily throughout that same year.
This is, again, due to finasteride’s biological half-life – which relates to its terminal half-life and tissue dissociation timings.
Anecdotally, many members of our community have found that taking a 2- to 3-week break from finasteride to troubleshoot side effects, or to fully disconnect during family vacations, does not seem to adversely impact their hair gains. So, at least within our community, we have a number of people to corroborate this clinical evidence with real-world experience.
Beyond a full month of quitting, it’s very likely that scalp levels of DHT fully return to baseline and that hair loss resumes. So, keep this in mind before deciding to experiment with different finasteride dosing schedules.
References[+]
References ↑1, ↑2 https://pubmed.ncbi.nlm.nih.gov/9777765/ ↑3 https://pubmed.ncbi.nlm.nih.gov/10495374/ ↑4 https://www.ncbi.nlm.nih.gov/books/NBK557634/ ↑5 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6459338/ ↑6 https://dm5migu4zj3pb.cloudfront.net/manuscripts/113000/113003/JCI87113003.pdf ↑7, ↑9 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3481923/ ↑8 https://academic.oup.com/jcem/article/89/5/2179/2844345 ↑10 https://jaad.org/retrieve/pii/S0190962220319289 IngredientsPharmaceuticalsNatural RemediesCompany Reviews
By Ben Fletcher, PhDApr 29, 2025Topical Cetirizine: An Anti-Histamine That Regrows Hair? (New Evidence)
Curious if an allergy medication could help with hair loss? Cetirizine, a second-generation antihistamine, is best known for treating allergies, but emerging research suggests it might also promote hair growth when applied topically. From reducing inflammation and mast cell activity to lowering leve...
By Sarah King, PhDMar 25, 2025Scalp Psoriasis: Symptoms, Causes, and Effects on Hair Loss
Scalp psoriasis goes beyond surface-level flaking; it’s a chronic autoimmune condition driven by genetic and immune system factors. From thick plaques and itching to potential hair loss, it can seriously impact daily life. Curious about what causes it, how to tell it apart from similar conditions, a...
By Sarah King, PhDMar 11, 2025Can Methylene Blue Regrow Your Hair? A Look At The Science.
Methylene blue, a well-known compound with antioxidant and anti-aging properties, has recently gained attention as a potential hair loss treatment. But does the science support the hype? In this article, we examine preclinical research on methylene blue, its mechanisms related to hair health, and wh...
By Sarah King, PhDMar 4, 2025Hair Loss Breakthroughs or Media Hype? Stem Cell Secretome Treatments
Stem cell secretome treatments are making headlines as the next big breakthrough in hair regrowth—but do they really work? While the science behind exosomes and growth factors sounds promising, media hype often overshadows the need for rigorous clinical trials. Curious about the real evidence behind...
By Sarah King, PhDFeb 25, 2025Seborrheic Dermatitis: Symptoms, Treatments, & Its Impact On Hair Loss
Seborrheic dermatitis is a common cause of dandruff, but what’s really happening to your scalp when it flares up? From excess sebum and yeast overgrowth to genetic factors, this condition has multiple triggers. Wondering what treatments work best and how to manage symptoms long-term? Check out our i...
By Sarah King, PhDJan 17, 2025New Study: Does Finasteride Cause Birth Defects?
A recent study has raised concerns about paternal finasteride use and cryptorchidism (undescended testicles) in offspring, but does the data actually support a causal link? The study, based on FAERS reports, shows a statistical association—but not proof of risk. Issues like reporting bias, lack of a...
By Sarah King, PhDJan 14, 2025Can Intermittent Fasting Cause Hair Loss? A Look Into A New Study
Intermittent fasting has gained popularity for its potential health benefits, but recent research highlights its possible impact on hair health. Studies on mice and humans suggest that fasting-induced metabolic shifts can slow hair growth and weaken hair shafts by depleting activated hair follicle s...
By Ben Fletcher, PhDJan 13, 2025Burdock Root For Hair Loss? A Look Into The Evidence
Burdock root, derived from the plant Arctium lappa, has long been used in traditional medicine for its purported anti-inflammatory, antimicrobial, and antioxidant properties. In recent years, it has been included in natural hair loss treatments, with claims that it promotes hair growth. Some studies...
By Sarah King, PhDDec 11, 2024Which Vitamin Deficiences Can Cause Hair Loss?
Hair loss is a complex issue influenced by various factors, including vitamin deficiencies. We explored the impact (or lack thereof) of deficiencies in five vitamins – Vitamin D, Biotin, Vitamin B12, Vitamin E, and Vitamin A – on hair health and whether supplementation can aid hair regrowth. While d...
By Perfect Hair Health TeamNov 21, 2024Genetic Tests: A Breakthrough for Personalized Hair Loss Treatments?
Genetic testing is trending in the hair loss industry. The premise? Our genes hold the secrets to better hair growth, and genetic tests can help hair loss sufferers unlock new levels of hair gains with customized treatments. It’s an enticing proposition, albeit one that holds little-to-no scie... - Mission Statement
 Scroll Down
Scroll Down More
More More
More