- About
- Mission Statement
Education. Evidence. Regrowth.
- Education.
Prioritize knowledge. Make better choices.
- Evidence.
Sort good studies from the bad.
- Regrowth.
Get bigger hair gains.
Team MembersPhD's, resarchers, & consumer advocates.
- Rob English
Founder, researcher, & consumer advocate
- Research Team
Our team of PhD’s, researchers, & more
Editorial PolicyDiscover how we conduct our research.
ContactHave questions? Contact us.
Before-Afters- Transformation Photos
Our library of before-after photos.
- — Jenna, 31, U.S.A.
I have attached my before and afters of my progress since joining this group...
- — Tom, 30, U.K.
I’m convinced I’ve recovered to probably the hairline I had 3 years ago. Super stoked…
- — Rabih, 30’s, U.S.A.
My friends actually told me, “Your hairline improved. Your hair looks thicker...
- — RDB, 35, New York, U.S.A.
I also feel my hair has a different texture to it now…
- — Aayush, 20’s, Boston, MA
Firstly thank you for your work in this field. I am immensely grateful that...
- — Ben M., U.S.A
I just wanted to thank you for all your research, for introducing me to this method...
- — Raul, 50, Spain
To be honest I am having fun with all this and I still don’t know how much...
- — Lisa, 52, U.S.
I see a massive amount of regrowth that is all less than about 8 cm long...
Client Testimonials150+ member experiences.
 Scroll DownPopular Treatments
Scroll DownPopular Treatments- Treatments
Popular treatments. But do they work?
- Finasteride
- Oral
- Topical
- Dutasteride
- Oral
- Topical
- Mesotherapy
- Minoxidil
- Oral
- Topical
- Ketoconazole
- Shampoo
- Topical
- Low-Level Laser Therapy
- Therapy
- Microneedling
- Therapy
- Platelet-Rich Plasma Therapy (PRP)
- Therapy
- Scalp Massages
- Therapy
- More
IngredientsTop-selling ingredients, quantified.
- Saw Palmetto
- Redensyl
- Melatonin
- Caffeine
- Biotin
- Rosemary Oil
- Lilac Stem Cells
- Hydrolyzed Wheat Protein
- Sodium Lauryl Sulfate
- More
ProductsThe truth about hair loss "best sellers".
- Minoxidil Tablets
Xyon Health
- Finasteride
Strut Health
- Hair Growth Supplements
Happy Head
- REVITA Tablets for Hair Growth Support
DS Laboratories
- FoliGROWTH Ultimate Hair Neutraceutical
Advanced Trichology
- Enhance Hair Density Serum
Fully Vital
- Topical Finasteride and Minoxidil
Xyon Health
- HairOmega Foaming Hair Growth Serum
DrFormulas
- Bio-Cleansing Shampoo
Revivogen MD
- more
Key MetricsStandardized rubrics to evaluate all treatments.
- Evidence Quality
Is this treatment well studied?
- Regrowth Potential
How much regrowth can you expect?
- Long-Term Viability
Is this treatment safe & sustainable?
Free Research- Free Resources
Apps, tools, guides, freebies, & more.
- Free CalculatorTopical Finasteride Calculator
- Free Interactive GuideInteractive Guide: What Causes Hair Loss?
- Free ResourceFree Guide: Standardized Scalp Massages
- Free Course7-Day Hair Loss Email Course
- Free DatabaseIngredients Database
- Free Interactive GuideInteractive Guide: Hair Loss Disorders
- Free DatabaseTreatment Guides
- Free Lab TestsProduct Lab Tests: Purity & Potency
- Free Video & Write-upEvidence Quality Masterclass
- Free Interactive GuideDermatology Appointment Guide
- More
Articles100+ free articles.
-
Which Hormones Cause Hair Loss in Females?
-
Does Zepbound Cause Hair Loss?
-
Does Wegovy Cause Hair Loss?
-
Strut Health Review: 5 Things to Consider Before Purchasing
-
Does Tirzepatide Cause Hair Loss?
-
Musely Reviews for Hair Loss: Are They Trustworthy?
-
Best Minoxidil for Women: Top 6 Brands of 2026
-
Best Topical Finasteride: 5 Top Products of 2026
PublicationsOur team’s peer-reviewed studies.
- Microneedling and Its Use in Hair Loss Disorders: A Systematic Review
- Use of Botulinum Toxin for Androgenic Alopecia: A Systematic Review
- Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia
- Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results
- A Hypothetical Pathogenesis Model For Androgenic Alopecia:Clarifying The Dihydrotestosterone Paradox And Rate-Limiting Recovery Factors
Menu- AboutAbout
- Mission Statement
Education. Evidence. Regrowth.
- Team Members
PhD's, resarchers, & consumer advocates.
- Editorial Policy
Discover how we conduct our research.
- Contact
Have questions? Contact us.
- Before-Afters
Before-Afters- Transformation Photos
Our library of before-after photos.
- Client Testimonials
Read the experiences of members
Before-Afters/ Client Testimonials- Popular Treatments
-
ArticlesThe Leading Alternative Theories Of Pattern Hair Loss
First Published Nov 1 2016Last Updated Sep 19 2025Miscellaneous Researched & Written By:Perfect Hair Health Team
Researched & Written By:Perfect Hair Health Team Reviewed By:Rob English, Medical Editor
Reviewed By:Rob English, Medical Editor
Want help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Learn MoreArticle Summary
Why do men and women lose their hair? Uncover the science and shortcomings of popular pattern hair loss theories – from genetics to gravity to scalp tension. Discover what the DHT hair loss theory fails to answer, and find out what all theories have yet to address.
Full Article
Do Any Hair Loss Theories Hold Water?
When it comes to explaining why men and women lose their hair, no theory has all the answers.
Some researchers say that DHT causes pattern hair loss. That’s true. But unfortunately, even the DHT theory cannot fully explain:
- …why men start thinning at the hairline and vertex
- …why women start thinning evenly across the scalp
- …why men usually don’t lose hair at the scalp sides
- …why women thin all over, even at the scalp sides
- …why DHT encourages body hair growth, but scalp hair loss (the DHT paradox)
And while alternative hair loss theories attempt to get us closer to answers, they still have holes.
This article uncovers the leading (alternative) hypotheses to pattern hair loss. For each theory, we’ll cover:
- The Science
- The Shortcomings
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.

Theory #1: DHT Theory Of Baldness
This is the theory of all hair loss theories. It’s touted by most doctors, surgeons, and researchers trying to quickly summarize why someone’s balding.
The Science
Dihydrotestosterone, or DHT, is a hormone that comes from testosterone.
DHT is higher in thinning regions of men’s scalps. As a result, many researchers say that DHT causes hair loss.
I first heard about DHT when I was diagnosed with pattern hair loss in 2007. Here’s how my doctor described the process:
For reasons not fully understood, hair loss begins when DHT starts accumulating in our scalps. Our hair follicles become sensitive to DHT, then begin shrinking. Over a series of hair cycles, DHT makes our hair thinner and wispier, until our hair becomes so thin that it disappears. The end result: pattern baldness.

Beyond my doctor’s summary, there are three findings which form the DHT-hair loss argument:
- DHT is higher in the scalps of men with thinning hair.
- If a man is castrated, his testosterone and DHT levels plummet forever. Men castrated before puberty (ie: before their DHT levels spike) never go bald later in life.
- Some men have a rare genetic condition where they the lack an enzyme which converts testosterone into DHT in the scalp. Men who have this condition never lose their hair.
- Finasteride –a DHT-reducing drug – improves pattern hair loss in 80-90% of men and increases hair counts by 10% over two years.
That’s a very compelling case… Just look at the extremes. If we never make any DHT, we never go bald. And if DHT is too high in our scalps, we lose our hair. And if we reduce DHT, our hair starts to come back.
So what’s wrong with this theory? Mainly, it’s not the causal relationship. It’s the questions still left unanswered.
The DHT-Hair Loss Theory’s Shortcomings
The DHT-hair loss theory leaves at least four questions unanswered:
- If DHT is the problem, then what causes DHT levels to rise in the first place?
- Why do our follicles become “sensitive” to DHT?
- How does DHT actually shrink our follicles?
- Why do men lose their hair in a horseshoe pattern, while women thin all over?
Researchers are still working to answers these questions. For example: some suggest that DHT increases because of enhanced androgen receptor activation in balding scalps – partly a result of the overexpression of the Hic5-ARA55 androgen receptor coactivator in balding tissues. So, why do these androgen receptor coactivators increase? We don’t yet know. And, whenever we hit a, “We don’t know”, the answer often defaults to “genetics”.
Unfortunately, “genetics” has sort of become a cop-out to any phenomenon we cannot fully explain with the current state of science. And perhaps most interestingly, the DHT-hair loss theory has not been able to effectively address DHT’s biggest paradox:
DHT in body and facial tissue encourages hair growth. DHT in scalp tissue discourages hair growth. Why?
Another alternative theory takes a stab at answering this.
Theory #2: Gravity Theory Of Baldness
Another theory is the Gravity Theory Of Baldness, which came about in an effort to answer the paradox of DHT:
Why does tissue DHT encourage body hair growth and simultaneously discourage scalp hair growth?
The theory’s answer is quite simple: gravity.
Gravity Theory: The Science
One symptom of a balding scalp is an eroded subcutaneous fat layer.
Subcutaneous fat is an insulating layer of fat. It’s found all over the body – including our scalps (on the sides, back, and top). At the tops of our scalps, the subcutaneous fat rests between the scalp skin and the galea (more on that later):

(source)
When we’re younger, our scalp’s subcutaneous fat is relatively equal on the sides and top of our scalp. But during pattern hair loss, the subcutaneous fat at the top of the scalp starts getting thinner and more eroded.
According to the theory, here’s why:
Our heads are upright for most of the day, creating chronic pressure against the hair follicles and our scalp’s subcutaneous fat layer.
At the start of puberty, men’s androgen levels surge (we get more testosterone and DHT).
The Gravity Theory Of Baldness states that downward force + high androgens kickstart the erosion of subcutaneous fat in the scalp.
For women, the theory states that high estrogen levels preserve the scalp’s subcutaneous fat layer – at least until menopause when estrogen levels plummet.
According to the theory, this is why men start balding into early adulthood, and why women typically don’t lose their hair until later in life.
How Does This Explain The DHT-Paradox?
Well, DHT encourages body hair growth while also encouraging scalp hair loss.
According to the Gravity Theory Of Baldness, DHT will only encourage hair loss if there is constant downward force at that skin site (aka: gravity).
So, the top of men’s heads is under constant gravitational force. But their beards and body hair aren’t under the same force, because they’re angled differently.
And that’s why men don’t go bald at the sides of the scalp or on their bodies or faces. Gravity’s force isn’t directly downward there, so the subcutaneous fat layer doesn’t erode in the presence of androgens like it does at the top of the scalp.
Summarizing The Theory Step-By-Step
Men’s scalps are protected against the downward forces of gravity until puberty, at which point testosterone levels increase and begin to erode the scalp’s subcutaneous fat layer. When this happens, our hair follicle’s subcutaneous “cushion” starts disappearing. The hair has to work harder to continue growing and survive.
Since androgens encourage hair growth in other parts of the body, our body responds to the decrease in the scalp’s subcutaneous fat by sending more androgens there – in the form of DHT.
DHT is supposed to encourage hair growth! But in an effort to encourage hair growth, DHT – a testosterone derivative – also erodes more of the scalp’s subcutaneous fat layer. The process continues until the subcutaneous fat layer nearly entirely dissipates, miniaturizing the hair follicle until it eventually turns dormant.
Gravity, according to the author, explains why men only bald at the top of the scalp, and why DHT encourages body hair growth and scalp hair loss simultaneously.
The Gravity-Androgen-Hair Loss Theory Shortcomings:
If this theory feels incomplete, it’s because it is.
Problem #1: the theory doesn’t actually explain the “pattern” of male pattern hair loss.
While the author explains why men lose hair at the top of the scalp, he doesn’t necessarily explain why the loss occurs in a pattern – or why men generally start thinning at the temples and vertex, then progresses from there.
Problem #2: the Gravity Theory doesn’t explain why men bald differently than women.
Males typically recede at the hairline and thin at the crown, but most women thin all over.
How does the Gravity Theory explain women’s even thinning at the top and sides of the scalp? Technically, any thinning on the scalp sides refute this theory, or at least give evidence of another mechanism.
Problem #3: like women, men can also lose hair at the sides of the scalp, not just at the top.
Men in advanced stages of hair loss typically lose hair on the sides and even parts of their sideburns.
According to the Gravity Theory, the subcutaneous tissue shouldn’t erode here because it’s not under the same chronic gravitational force. But in advanced stages, men and women definitely experience hair loss in these places.
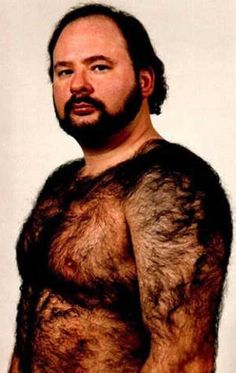
Problem #4: If this theory were 100% true, we’d also expect DHT to exert the same hair loss effect on other parts of our body that stay upright as long and as often as our heads.
For example, our shoulders. By the logic of the gravity theory, men should never get hairy shoulders. Why? The shoulders are on the same horizontal plane as the tops of our scalps. Our shoulders stay upright just about as long as the tops of our scalps, which means they’re under about the same gravitational pressure.
And at puberty, we’d expect a surge in androgens and the degradation of subcutaneous fat tissue in our shoulders, which means we’d be hard pressed to find any guy who’s balding with hairy shoulders.
Except here is a balding guy with hairy shoulders:

And another:

Hairy shoulders are so common I could start naming friends of mine with them.
As such, the Gravity Theory offers an incomplete explanation as to why DHT encourages hair growth and hair loss depending on the tissue. It doesn’t explain female pattern hair loss. And while the Gravity Theory might explain the relationship between a scalp’s decreased subcutaneous fat, increased DHT, and hair loss, it doesn’t come close to explaining the actual “pattern” of male pattern hair loss – or why recession and thinning starts at the temples and vertex.
The next theory does.
Theory #3: The Skull Expansion Theory
The third theory that offers an alternative explanation to the “pattern” of male pattern hair loss is The Skull Expansion Theory.
The theory is as follows: we know that the bones of the human skull continue growing throughout adulthood. We also know – based on observations – that balding men typically have a different head shape than non-balding men. Their forehead has a bulge at the midline, and some would even say their entire heads are larger than the heads of those unaffected by hair loss.
It turns out that DHT –which is elevated in balding scalp tissues – is also a hormone used by the body for bone remodeling.
The Skull Expansion Theory argues, like the Gravity Theory, that the presence of DHT should encourage hair growth, not hair loss. But because DHT also encourages bone growth, then elevated DHT in the scalp also increases skull bone growth. This bone growth expands the size of the skull, and in doing so, moves the follicles further away from the capillary networks that supports them. The resulting reduction of blood flow leads to follicle miniaturization, and subsequently, hair loss.
This theory is versatile in that it explains all the different patterns of hair loss for men. Skull bone growth at the front of the scalp leads to thinning at the temples. Skull bone growth at the back of the scalp leads to thinning at the vertex. If you take a walk around town, you can see for yourself the evidence of the skull expansion theory. Men who are receding at the temples typically have a bulge at the front of their scalp. If you’re suffering from pattern hair loss and you have older photos of yourself, you might even notice the development of this bulge as you began to thin over the years.
The Skull Expansion Theory Shortcomings
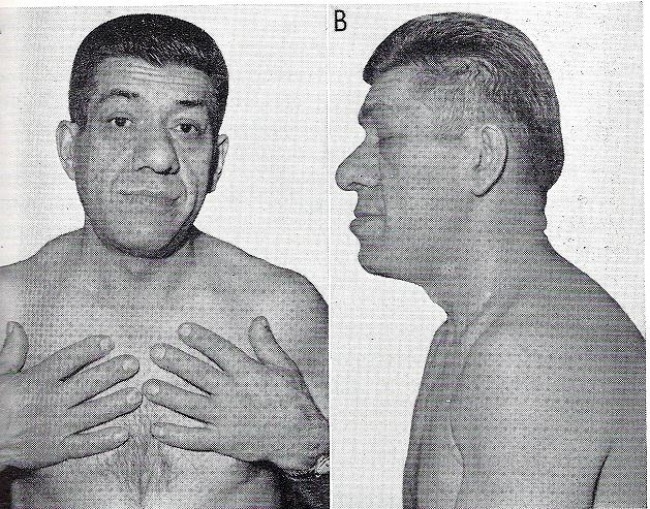
The first problem with the Skull Expansion Theory is that there are some men who clearly have experienced skull expansion, but also minimal or no hair loss. This is evident when we look specific cases of frontal bossing — or when the brow line begins to protrude far beyond the forehead.

Not all people with frontal bossing or forehead protrusion experience hair loss.
Moreover, frontal bossing and severe forms of skull expansion are often the result of excessive growth hormone release – sometimes due to a tumor in the pituitary gland. In some cases, the release can be so excessive and so chronic that a person’s hands, feet, face, head, and body continue to grow throughout adulthood.
This is called Acromegaly. Andre The Giant had the condition, but despite his bone growth, he also had pretty good hair.

So did this guy:

There are also cases of men whose skulls haven’t expanded much but have still gone bald.
Take Kelly Slater at 19-years old and then in his forties.
His scalp is very well rounded – there’s no frontal bossing, and minimal (if any) expansion on the sides of his scalp. It looks as if he just shaved his head. He did. But during that period, he also lost a lot of hair.
The second problem is that the Skull Expansion Theory, like the Gravity Theory, doesn’t fully explain the difference in male versus female pattern hair loss, or why women typically thin evenly everywhere while men thin at the temples and vertex first.
With that said, I believe in the association between a bigger head and a balding scalp. Skull expansion is definitely a factor in many pattern hair loss cases. The theory deserves more attention and more research, and its author, Paul Taylor, deserves significant recognition for putting out an idea with more merit than, in my opinion, nearly every other theory. But as far as the skull expansion causing hair loss — I think this has still yet to be proven.
Which brings us to the last and most specific theory of all.
Theory #4: Muscular Tension / Tight Galea Theory
There are a few iterations of the tight galea and muscular tension theories of pattern hair loss. I believe these theories – while still incomplete – take us closer to answers than others (though still have plenty of problems).
Here are the basic principles behind the theories. If you’re interested in learning more for yourself, I encourage you to read our peer-reviewed study on the scalp tension hypothesis.
(In fact, that data are why I recommend spending so much time massaging the sides, nape, and sutures of your scalp – and not just your thinning areas.)
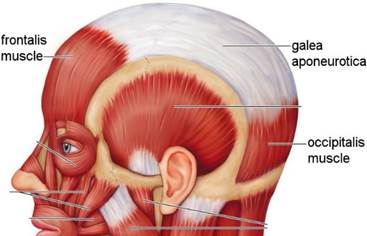
The theory is as follows: the parts of the scalp predominantly affected by male pattern baldness are all above the galea. The galea is a fibrous tissue that rests over the entire top of the scalp. It’s a connective tissue that links the muscles above your eyebrow (frontalis) and the muscles behind your ears (occipitalis). There are no muscles on the top of your scalp – just the tendon-like fibrous tissue known as the galea.

(source)
For men, the areas of the galea aren’t really affected by hair loss. It’s just the hair residing over the galea that tends to disappear. So the question is, why?
Well, it turns out that in balding men, the muscles surrounding the galea are chronically involuntarily contracted.
This causes two problems, both of which might accelerate pattern hair loss.
#1. Chronically Contracted Muscles Pinch Arterial Branches
The carotid artery is the main source of bloody supply pumping up through the neck to the top of the scalp. Essentially, it’s the “big branch” that supplies nearly all of the blood (and thereby oxygen and nutrients) that reaches the top part of our scalps.
Some carotid arterial branches run between the muscles that surround our galeas. For instance, the subraorbital and subratrochlear branches run under the frontalis muscles and then pierce through those muscles to supply our temple regions with blood flow. Branches of the auricularis muscles run between the muscles. The deep supertemporal arterial branches run between the muscle and pericranium. All of these arteries are likely impacted by muscular contraction. Specifically, when these muscles end up chronically contracted, they may pinch the carotid artery – thereby drastically reducing the blood supply that can reach the top of the scalp.
When blood supply is reduced, so is oxygen (since blood carries oxygen). And fascinatingly, in areas of “low oxygen” – also known as hypoxia – there is a hypothesis that our bodies begin to favor the conversion of testosterone into DHT, because this conversion is not oxygen-dependent.
This might increase levels of DHT in the scalp, thereby explaining why balding scalps see not only increased DHT, but also decreased blood and oxygen supply.
Chronic muscular contractions surrounding the galea >> carotid artery gets pinched >> blood flow to the top of the scalp gets reduced >> “hypoxic” (i.e., low oxygen) environment >> increased DHT
This is interesting and all, and it might help explain why DHT increases in balding regions. But it still doesn’t explain why DHT behaves differently in the scalp versus the body (in other words, why DHT is linked to scalp hair loss and body hair growth).
Fortunately, the next component of this theory may answer that!
#1. Chronically Contracted Muscles Create Chronic Tension In The Galea
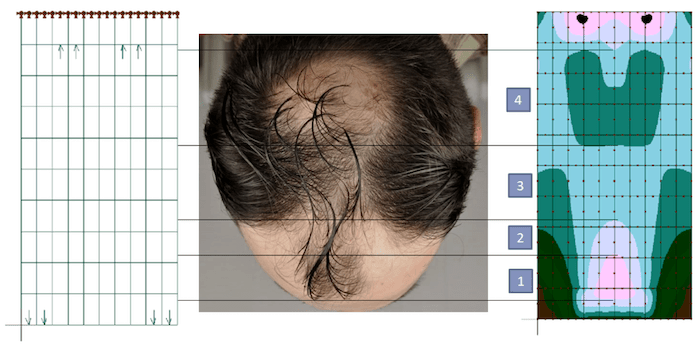
To reiterate, these scalp perimeter muscles are attached to the galea. And when these muscles become chronically contracted, this chronic contraction “pulls” the galea tight – like the skin of a drum.
Interestingly, if we model out what this tension pattern looks like across the top part of the scalp, it nearly perfectly aligns with the patterning and progression of male and female pattern hair loss.

Why is this important? Well, in other tissues of the body, if any area remains “tensed” for too long, the body begins to read that tension as inflammation… and it starts sending signaling proteins and hormones to that region in an attempt to resolve that inflammation.
We’ve seen this exact relationship in chronically tensed periodontal tissues, finger ligaments, prostate tissues, and in the eyelids of Grave’s disease patients. And one of the hormones sent to these sites of chronic inflammation? DHT.
Chronic muscular contractions surrounding the galea >> galea is pulled chronically tight >> body reads this chronic tension as chronic inflammation >> sends DHT to the top of the scalp
Fascinatingly, since we generally cannot resolve chronic tension with an inflammatory response, our bodies will instead lay down scar tissue as a means to stop what it thinks is a chronic inflammatory cascade. And where there’s scar tissue, hair cannot grow.
This theory, then, might explain not only why DHT arrives to balding areas, but also why DHT seems to behave differently at the top of the scalp versus everywhere else in the body.
A Deeper Dive: More Science Behind The Scalp Tension / Tight Galea Theory
We know that androgens, like DHT, play a role in pattern hair loss because men who are castrated before puberty have very low levels of DHT and don’t go bald later in life. We also know that tissue DHT levels are higher in balding versus non-balding parts of the scalp. This is why people associate DHT with hair loss. There’s definitely a relationship, but whether DHT is the cause of hair loss is still debated (as evidenced above). In any case, this phenomenon begs the question: why do tissue DHT levels increase only in balding areas, and not everywhere in the scalp?
Some researchers believe DHT levels are higher in balding regions because of an idea known as “enhanced androgen sensitivity.” But in order for DHT to accumulate in the scalp, DHT needs to attach itself to a receptor site. These receptor sites are known as androgen receptors.
Androgen receptors are located inside our cells. When DHT attaches to a cell’s androgen receptor, that DHT molecule will influence that cell’s functionality. For example, in certain facial and body tissue cells, DHT appears to influence cell function by encouraging hair growth. But for cells surrounding the hair above the galea, DHT appears to encourage hair loss.
How can that be? How can the same hormone encourage both hair growth and hair loss, with the only difference being body location?
It turns out that DHT molecules aren’t the only thing that influences a cell’s function. Certain proteins can also change cell behavior. These proteins are called androgen receptor “coactivators.” These coactivators interact with androgen receptors – the place where DHT binds – and “enhance” the androgen receptor’s function. In other words, these protein “coactivators” increase a cell’s sensitivity to androgens.
One of these coactivators is called Hic-5 / ARA55. This coactivator is highly active in beard tissues and in balding tissues of the scalp, but not so active in non-balding parts of the scalp like the back of the head.
This is important. In tissues with elevated DHT (the tissues that grow facial hair and the tissues in bald parts of the scalp), this protein coactivator is also higher. Some research suggests that this very coactivator regulates androgen sensitivity in human hair follicles. To put it bluntly, if a cell expresses the Hic-5 / ARA55 coactivator, you can bet that DHT will bind to it.
According to the theory, this is why some tissues accumulate DHT and others don’t. At puberty, the Hic-5 / ARA55 coactivator increases in facial, body, and scalp tissues above the galea. As a result, more DHT binds to those cells’ androgen receptors. Paradoxically, in the scalp, more DHT leads to hair loss. In the face and body, more DHT leads to hair growth.
But why? If an increase in Hic-5 / ARA55 explains why certain tissues start accumulating more DHT, then why does an increase in DHT cause hair loss at the scalp but hair growth in the body?
This is where the mechanical force element comes into play (i.e., chronic tension).
The Hic-5 / ARA55 coactivator is activated by both androgens and mechanical force – specifically, stretching tension, the kind of tension occurring naturally in the galea.
It also turns out that increased DHT in the scalp also stimulates something called transforming growth factor beta 1 (TFG-β1). TFG-β1 is a signaling protein, and when it’s overexpressed, it leads to perifollicular fibrosis – or scarring surrounding the hair shaft that miniaturizes the hair and leads to hair loss. Chronically elevated levels of TFG-β1 are suspected to cause the fibrotic fusing we observe in the top three layers of balding scalps.
This creates the “perfect storm” hair loss cycle. It goes something like this:
- At puberty, an increase in androgens stimulates the expression of Hic-5 / ARA55 coactivators in body, facial, and certain scalp sites. This coactivator makes a cell’s androgen receptor more “sensitive” to DHT – and thereby more likely for DHT to bind to it.
- More DHT binds to androgen receptors in body, facial, and scalp tissues… But in the scalp tissues, more DHT also leads to an overexpression of TFG-β1.
- Above the galea, the overexpression of TFG-β1 results in perifollicular fibrosis. The hair follicles begin to miniaturize, and over time, fibrosis begins to set in, creating a rate-limiting recovery factor (again, where there is scar tissue, hair cannot grow).
- This “fusion” may create more mechanical tension, especially at the the vertex and temples, which may encourage an even higher expression of the Hic-5 / ARA55 coactivator.
- The Hic-5 / ARA55 coactivator encourages more DHT to the scalp tissue (increased androgen sensitivity), which increases TFG-β1, which increases perifollicular fibrosis, and then more tension, which then activates more Hic-5 / ARA55…
- …and the cycle repeats.
The more Hic-5 / ARA55, the more DHT, the more TFG-β1, the more perifollicular fibrosis, and the more hair we lose…
Or so the theory goes.
Shortcomings
This theory is the most complicated, and thereby lends itself to serious nitpicking. I won’t get into all of the issues, but these three shortcomings alone warrant more research:
- The theory’s argument that TFG-β1 increases more in the scalp than other body sites is unfounded. TFG-β1 is a signaling protein. It’s used in tissues all over the body for processes ranging from inflammatory responses to cell proliferation. While there’s evidence to suggest TFG-β1 inhibits hair growth, I’ve never seen anything that says TFG-β1 is higher in balding scalps than body or facial tissues that bear hair. That needs to be true for the theory to hold. But for now, this statement is just conjecture.
- The theory doesn’t explain why, at puberty, androgens stimulate the expression of Hic-5 / ARA55 in soon-to-be hair bearing body and facial tissues, on scalp tissue above the galea where hair is already present, but not on hair-bearing sites on the sides of the scalp. The theory says this coactivator over-expresses above the galea because of the mechanical tension already naturally occurring in the galea… But if this is the reason why the coactivator expresses itself above the galea but not on the sides of the head, then is there also similar tension at every other hair site on the body and face? Here we have a chicken-and-egg problem. Which came first: the tension or the Hic-5 / ARA55 coactivator? And even ignoring this, the theory still doesn’t explain the mechanism behind which androgens activate the Hic-5 / ARA55 coactivator. Basically, the theory consists of a lot of unproven assumptions.
- Hair follicle miniaturization (the defining characteristic of AGA) can still happen in regions outside of the galea aponeurotica (like the sides of the scalp). So, if scalp tension is involved in AGA, it’s likely an accelerator of the condition rather than a root cause.
But to be clear: the absence of evidence is not evidence against something. And beyond these criticisms, I tend to find that this theory gets us somewhat close to explaining the patterning and progression of pattern hair loss… and in answering all of those questions that the DHT-genetics pattern hair loss argument cannot answer.
What About Hair Transplants?
A lot of people argue that hair transplants refute the scalp tension hypothesis.
At face-value, this may seem true, but it’s not. We’ve written an article exploring this topic in better detail (see the last link).
Which Hair Loss Theory Do I Believe?
I don’t adhere to any specific theory.
I think the Gravity Theory, Skull Expansion Theory, and Muscular Tension / Tight Galea Theory all have their flaws and merits. Each theory is capable of explaining some, but not all, of the pieces to the puzzle of male and female pattern hair loss.
With that said, here’s what all these theories miss:
- None do a perfect job at explaining why women bald in a different pattern than men.
- None of these theories adequately address the DHT paradox – why DHT encourages body and facial hair growth but discourages scalp hair growth. (At the same time, this may just be due to an absence of evidence from lacking studies.)
What can we glean from all of this?
We need to do more research.
If hair loss research orient their studies to answer…
- Why men bald differently than women
- Why DHT encourages body hair growth, and scalp hair loss
- Why, in advanced stages of androgenic alopecia, men lose hair at the sides and napes of the neck
…then I think those answers will take us closer to a universal cure.
Want help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Learn More
Perfect Hair Health Team
"... Can’t thank @Rob (PHH) and @sanderson17 enough for allowing me to understand a bit what was going on with me and why all these [things were] happening ... "
— RDB, 35, New York, U.S.A."... There is a lot improvement that I am seeing and my scalp feel alive nowadays... Thanks everyone. "
— Aayush, 20’s, Boston, MA"... I can say that my hair volume/thickness is about 30% more than it was when I first started."
— Douglas, 50’s, Montréal, CanadaWant help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Join Now - Mission Statement
 Scroll Down
Scroll Down More
More More
More