- About
- Mission Statement
Education. Evidence. Regrowth.
- Education.
Prioritize knowledge. Make better choices.
- Evidence.
Sort good studies from the bad.
- Regrowth.
Get bigger hair gains.
Team MembersPhD's, resarchers, & consumer advocates.
- Rob English
Founder, researcher, & consumer advocate
- Research Team
Our team of PhD’s, researchers, & more
Editorial PolicyDiscover how we conduct our research.
ContactHave questions? Contact us.
Before-Afters- Transformation Photos
Our library of before-after photos.
- — Jenna, 31, U.S.A.
I have attached my before and afters of my progress since joining this group...
- — Tom, 30, U.K.
I’m convinced I’ve recovered to probably the hairline I had 3 years ago. Super stoked…
- — Rabih, 30’s, U.S.A.
My friends actually told me, “Your hairline improved. Your hair looks thicker...
- — RDB, 35, New York, U.S.A.
I also feel my hair has a different texture to it now…
- — Aayush, 20’s, Boston, MA
Firstly thank you for your work in this field. I am immensely grateful that...
- — Ben M., U.S.A
I just wanted to thank you for all your research, for introducing me to this method...
- — Raul, 50, Spain
To be honest I am having fun with all this and I still don’t know how much...
- — Lisa, 52, U.S.
I see a massive amount of regrowth that is all less than about 8 cm long...
Client Testimonials150+ member experiences.
 Scroll DownPopular Treatments
Scroll DownPopular Treatments- Treatments
Popular treatments. But do they work?
- Finasteride
- Oral
- Topical
- Dutasteride
- Oral
- Topical
- Mesotherapy
- Minoxidil
- Oral
- Topical
- Ketoconazole
- Shampoo
- Topical
- Low-Level Laser Therapy
- Therapy
- Microneedling
- Therapy
- Platelet-Rich Plasma Therapy (PRP)
- Therapy
- Scalp Massages
- Therapy
- More
IngredientsTop-selling ingredients, quantified.
- Saw Palmetto
- Redensyl
- Melatonin
- Caffeine
- Biotin
- Rosemary Oil
- Lilac Stem Cells
- Hydrolyzed Wheat Protein
- Sodium Lauryl Sulfate
- More
ProductsThe truth about hair loss "best sellers".
- Minoxidil Tablets
Xyon Health
- Finasteride
Strut Health
- Hair Growth Supplements
Happy Head
- REVITA Tablets for Hair Growth Support
DS Laboratories
- FoliGROWTH Ultimate Hair Neutraceutical
Advanced Trichology
- Enhance Hair Density Serum
Fully Vital
- Topical Finasteride and Minoxidil
Xyon Health
- HairOmega Foaming Hair Growth Serum
DrFormulas
- Bio-Cleansing Shampoo
Revivogen MD
- more
Key MetricsStandardized rubrics to evaluate all treatments.
- Evidence Quality
Is this treatment well studied?
- Regrowth Potential
How much regrowth can you expect?
- Long-Term Viability
Is this treatment safe & sustainable?
Free Research- Free Resources
Apps, tools, guides, freebies, & more.
- Free CalculatorTopical Finasteride Calculator
- Free Interactive GuideInteractive Guide: What Causes Hair Loss?
- Free ResourceFree Guide: Standardized Scalp Massages
- Free Course7-Day Hair Loss Email Course
- Free DatabaseIngredients Database
- Free Interactive GuideInteractive Guide: Hair Loss Disorders
- Free DatabaseTreatment Guides
- Free Lab TestsProduct Lab Tests: Purity & Potency
- Free Video & Write-upEvidence Quality Masterclass
- Free Interactive GuideDermatology Appointment Guide
- More
Articles100+ free articles.
-
Does Anavar Cause Hair Loss?
-
10 Best Shampoos for Hair Loss in 2026
-
XYON Review: Do Their Products Actually Regrow Hair?
-
Minoxidil Before and After Photos [2026] | Does It Work?
-
How to Get Finasteride: Is It Over the Counter?
-
Keeps Review: The Truth About Their Hair Loss Treatments?
-
7 Best Oils for Hair Growth
-
Hims Hair Growth Reviews: The Pros, Cons, and Real Results
PublicationsOur team’s peer-reviewed studies.
- Microneedling and Its Use in Hair Loss Disorders: A Systematic Review
- Use of Botulinum Toxin for Androgenic Alopecia: A Systematic Review
- Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia
- Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results
- A Hypothetical Pathogenesis Model For Androgenic Alopecia:Clarifying The Dihydrotestosterone Paradox And Rate-Limiting Recovery Factors
Menu- AboutAbout
- Mission Statement
Education. Evidence. Regrowth.
- Team Members
PhD's, resarchers, & consumer advocates.
- Editorial Policy
Discover how we conduct our research.
- Contact
Have questions? Contact us.
- Before-Afters
Before-Afters- Transformation Photos
Our library of before-after photos.
- Client Testimonials
Read the experiences of members
Before-Afters/ Client Testimonials- Popular Treatments
-
Articles
Methylene blue, a compound originally developed as a medical dye, has recently been stirring up attention due to its potential therapeutic applications beyond its initial purpose, particularly in the realm of age-related concerns such as cognitive and skin health. However, some are now exploring its potential use in hair regrowth.

Chemical structure of methylene blue.[1]PubChem. (no date). Methylene Blue. National Library of Medicine. Available at: https://pubchem.ncbi.nlm.nih.gov/compound/Methylene-Blue (Accessed: March 2025)
This research aligns with a broader trend in the pharmaceutical industry: repurposing old compounds for new indications. This offers several advantages, including reduced development time, lower costs, and decreased risk due to established safety trials. Approximately 30% of repurposed drugs typically gain approval compared to only 10% of new drug applications, making this strategy increasingly attractive for pharma companies.[2]Hernandez, J.J., Pryszlak, M., Smith, L., Yanchus, C., Kurji, N., Shahani, V.M., Molinski, S.V. (2017). Giving Drugs a Second Chance: Overcoming Regulatory and Financial Hurdles in Repurposing … Continue reading
In this article, we will examine the evidence surrounding methylene blue and whether it could translate to better hair growth outcomes.
Key Takeaways
- What Is It? Methylene blue is a medical dye with antioxidant, mitochondrial-supporting, and anti-inflammatory properties. It has been studied for neurodegenerative diseases, skin health, and aging, but its role in hair regrowth is unproven.
- Clinical Data. There are no human clinical trials testing methylene blue for hair regrowth. Most research comes from in vitro and animal studies. One study in hair transplants found no benefit over saline.
- Evidence Quality. Methylene blue scored 6/100 for evidence quality by our metrics.
- Safety. While generally safe at therapeutic doses, methylene blue can cause nausea, headaches, and urine discoloration. More serious risks include serotonin syndrome (when combined with SSRIs/SNRIs) and hemolytic anemia in G6PD-deficient individuals. The long-term effects of cosmetic use remain unknown.
- Best Practices. Given the lack of evidence and potential risks, methylene blue should not be considered a proven hair loss treatment. For those seeking regrowth solutions, clinically tested treatments remain the safest bet.
All-Natural Hair Supplement + Topical
The top natural ingredients for hair growth, all in one serum & supplement.
Take the next step in your hair growth journey with a world-class natural serum & supplement. Ingredients, doses, & concentrations built by science.

Let’s start off by exploring why people are so excited about methylene blue.
Methylene blue is purportedly a potent mitochondrial-targeting antioxidant that effectively scavenges reactive oxygen species (ROS).[3]Xue, H., Thaivalappil, A., Cao, K. (2021). The Potentials of Methylene Blue as an Anti-Aging Drug. Cells. 10(3379). 1-12. Available at: https://doi.org/10.3390/cells10123379 According to the free radical theory of aging, ROS are closely linked to cellular aging. ROS accumulation can cause a cellular state called oxidative stress, which damages DNA, protein, and lipids.[4]Labunskyy, V.M., Galdyshev, N.M. (2013). Role of Reactive Oxygen Species-Mediated Signaling in Aging. Antioxidants & Redox Signaling. 19(12). 1362-1372. Available at: … Continue reading
What Beneficial Properties Might Methylene Blue Have?
Methylene blue has shown promise for improving several aging pathways. Let’s take a look at the pre-clinical evidence and see how it might translate into improvements in hair regrowth.
Anti-Aging
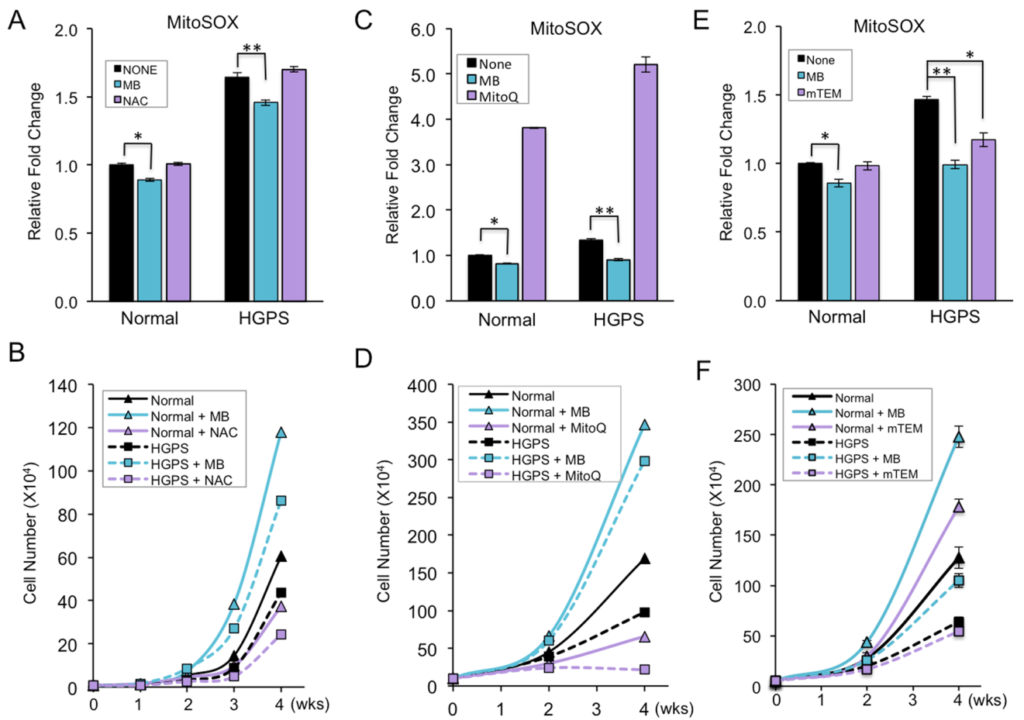
In cultured human skin, fibroblasts derived from healthy donors and patients with progeria (a genetic disorder leading to rapid aging in children) were used to evaluate the antioxidant activity of methylene blue.[5]Xiong, Z-M., O’Donovan, M., Sun, L., Choi, J.Y., Ren, M., Cao, K. (2017). Anti-aging potentials of methylene blue for human skin longevity. Scientific Reports. 7(2475). 1-12. Available at: … Continue reading Compared to other widely used mitochondrial-targeting antioxidants, the researchers found that methylene blue reduced levels of ROS (MitoSOX) and improved skin fibroblast proliferation more effectively (Figure 1).

Figure 1: Effect of 100 nM methylene blue (MB) compared to 100 µMm N-acetyl-cysteine (NAC) (A,B), 100 nM MitoQ (C,D), and 100 nM mTEM (E,F) on mitochondrial-specific superoxide (MitoSOX) levels and cell growth after four weeks of treatment. (*p < 0.05, **p < 0.01).[6]Xiong, Z-M., O’Donovan, M., Sun, L., Choi, J.Y., Ren, M., Cao, K. (2017). Anti-aging potentials of methylene blue for human skin longevity. Scientific Reports. 7(2475). 1-12. Available at: … Continue reading
The researchers also found that methylene blue could reduce signs of aging in old skin cells. Before treatment, the old fibroblasts (harvested from two subjects over 80 years old) showed signs of cellular senescence, including increased ꞵ-galactosidase (a marker of senescence) and higher levels of mitochondrial ROS than younger cells (harvested from two subjects below 30 years old). Both the old and young cells were grown in a medium supplemented with methylene blue for four weeks. Compared to a control, methylene blue significantly reduced levels of mitochondrial ROS, reduced ꞵ-galactosidase marker signal and decreased the gene expression of senescence marker p16 in the old cells. It also improved cell growth in both old and young cells (Figure 2).

Figure 2: Effect of methylene blue on molecular signs of cell aging in young (1-YM, 2-YF) and old (3-OM, 4-OF) fibroblasts. A = ꞵ-galactosidase (blue) staining reduced in cells treated with methylene blue, B = p16 gene expression (a gene that is upregulated in senescence) is significantly reduced in both young and old fibroblasts, C = MitoSOX levels in cells treated with methylene blue were significantly decreased in the two older fibroblasts, D = both young and old fibroblast cells grew better in medium supplemented with methylene blue than without.[7]Xiong, Z-M., O’Donovan, M., Sun, L., Choi, J.Y., Ren, M., Cao, K. (2017). Anti-aging potentials of methylene blue for human skin longevity. Scientific Reports. 7(2475). 1-12. Available at: … Continue reading
In addition to this, the researchers analyzed the effect of methylene blue on the expression of key antioxidant response genes. Methylene blue was found to upregulate the expression of Nrf2, which is an important transcription factor involved in the antioxidant response. In 3D reconstructed human skin, it was also found to promote wound healing, increase tissue viability, skin thickness and hydration, and upregulate elastin and collagen 2A1, which are important for maintaining skin elasticity and thickness.
UV Protection
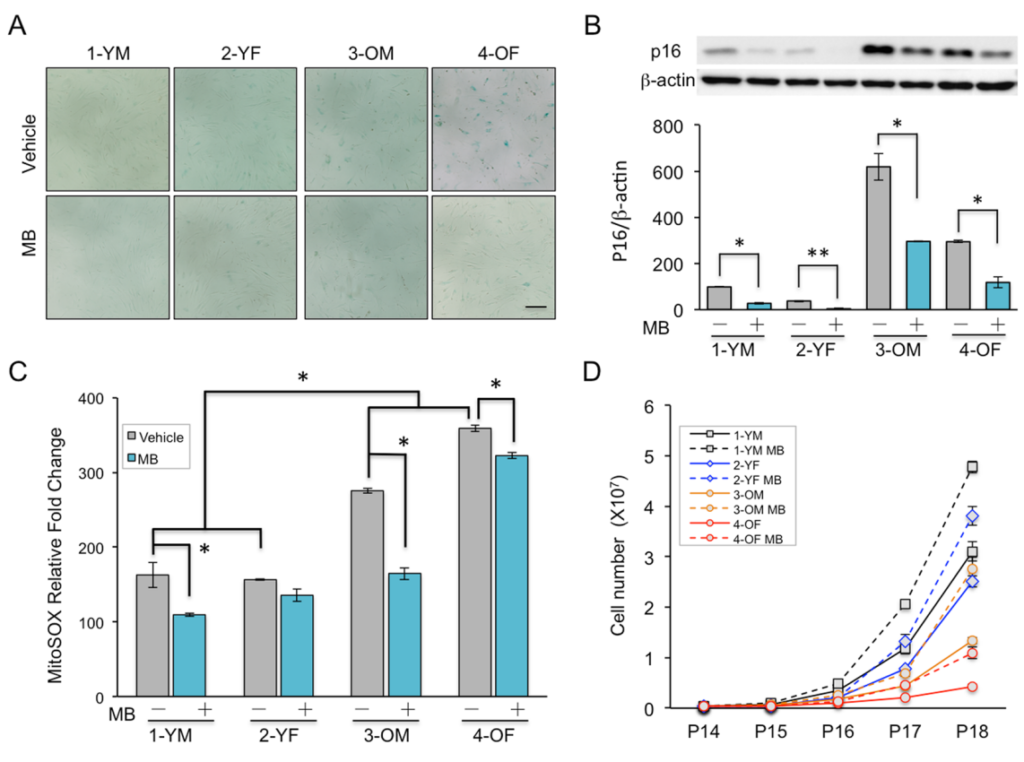
Another in vitro (in cells) study was conducted in which primary human keratinocytes were irradiated with UV rays and treated with methylene blue to test if it had any protective effects against UV-induced DNA damage and cell death.[8]Xiong, Z-M., Mao, X., Trappio, M., Arya, C., el Kordi, J., Cao, K. (2021). Ultraviolet radiation protection potentials of methylene blue for human skin and coral reef health. Scientific Reports. … Continue reading
The cells were treated with 100 nM of methylene blue for two weeks and then exposed to 0, 5, 10, and 20 seconds of UVB rays at 1 W/cm2 (Watt per cm2). A common marker for DNA damage, ℽH2AX, was measured, with methylene blue treated cells showing significantly reduced expression at each dosage compared to the control (PBS) (Figure 3).

Figure 3: Methylene blue reduces DNA damage induced by UVB irradiation in human keratinocytes. A = The experimental timeline starting from pre-incubation with methylene blue or PBS for 2 weeks, then exposure to UVB light and collection at specific time points, B = Western blot images showing the protein expression of DNA damage markers H2AX and ℽH2AX, C = graph representation of the western blot results, showing that methylene blue reduces DNA damage after UVB irradiation.[9]Xiong, Z-M., Mao, X., Trappio, M., Arya, C., el Kordi, J., Cao, K. (2021). Ultraviolet radiation protection potentials of methylene blue for human skin and coral reef health. Scientific Reports. … Continue reading
The researchers also found that it prevented human keratinocytes from undergoing UVB irradiation-induced cell death and that it was more effective at blocking high-energy UVB/C rays than a common UV blocker used in most sunscreens, oxybenzone.
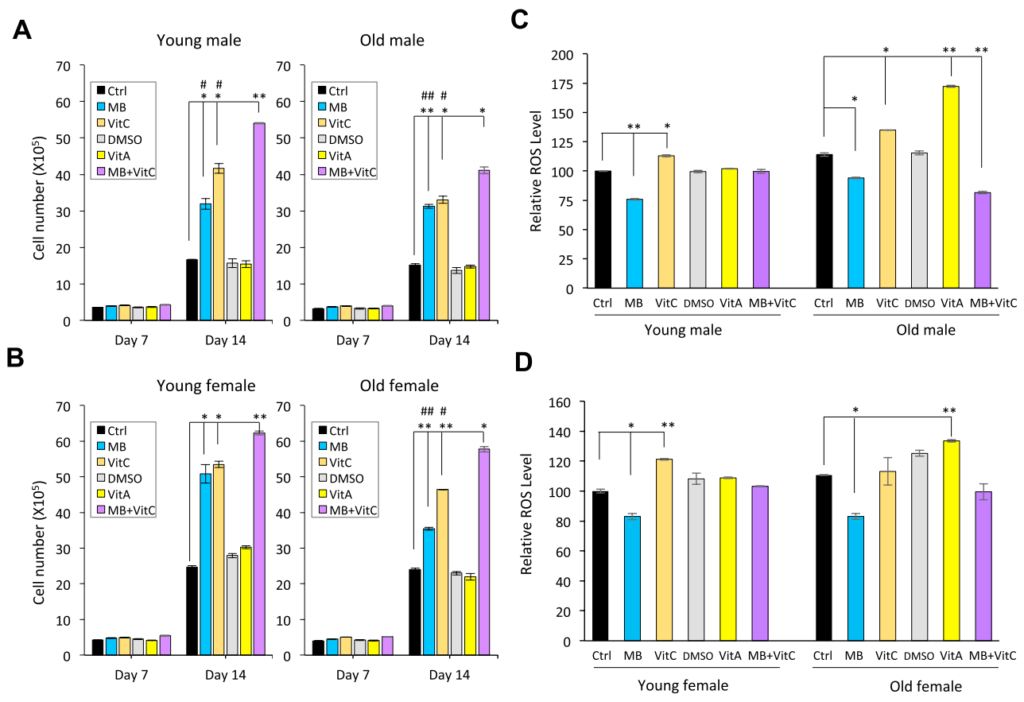
They also found that methylene blue was a more robust scavenger of ROS (meaning that it can effectively neutralize and remove ROS) than oxybenzone, Vitamin A, and Vitamin C in keratinocytes. A separate experiment was also conducted on young and old fibroblasts derived from males and females treated with either PBS, DMSO (controls), methylene blue, Vitamin A, Vitamin C, or a combination of Vitamin C and methylene blue. The combination treatment showed increased cell growth in both young and old cells (male and female) compared to all other treatments. When it came to ROS levels, the methylene blue alone treatment and the combination treatment both showed the most effective reductions in ROS levels (Figure 4).

Figure 4: Methylene Blue is a more effective ROS scavenger than Vitamin A and Vitamin C in human skin fibroblasts. A and B = young and old fibroblast cell growth during fourteen-day treatment with PBS, DMSO, 100 nM methylene blue, 100 nM Vitamin A, 100 µM Vitamin C, and 100 nM methylene blue + 100 µM Vitamin C. C and D = Comparison of MitoSOX levels in young and old male fibroblasts after treatment with PBS, DMSO, 100 nM methylene blue, 100 nM Vitamin A, 100 µM Vitamin C, and 100 nM methylene blue + 100 µM Vitamin C for four weeks.[10]Xiong, Z-M., Mao, X., Trappio, M., Arya, C., el Kordi, J., Cao, K. (2021). Ultraviolet radiation protection potentials of methylene blue for human skin and coral reef health. Scientific Reports. … Continue reading
Anti-Inflammatory
One study has shown that methylene blue decreases inflammation by reducing serum levels of interleukin-6 (a pro-inflammatory cytokine that plays a significant role in both acute and chronic inflammatory responses) and inhibiting the activation of STAT3 in the skin.[11]Li, Y., Ying, W. (2023). Methylene blue reduces the serum levels of interleukin-6 and inhibits STAT3 activation in the brain and the skin of lipopolysaccharide-administered mice. Frontiers in … Continue reading STAT3 is implicated in the pathogenesis of alopecia areata.[12]Roche, F.C., Hedberg, M.L. Fischer, A.S., Ray, A., Dentchev, T., Rice, X., Taylor, S.C., Seykora, J.T. (2023). Activation of STAT3 in lymphocytes associated with central centrifugal cicatricial … Continue reading
Mice were split into four groups: control (PBS injected intraperitoneally every day for 3 days), and 5 mg/kg, 10 mg/kg, and 20 mg/kg methylene blue groups (injected intraperitoneally every day for 3 days). Another three groups of mice were treated with lipopolysaccharide (1 mg/kg) to induce inflammation, with two groups also being treated with 10 mg/kg of methylene blue and 20 mg/kg of methylene blue.
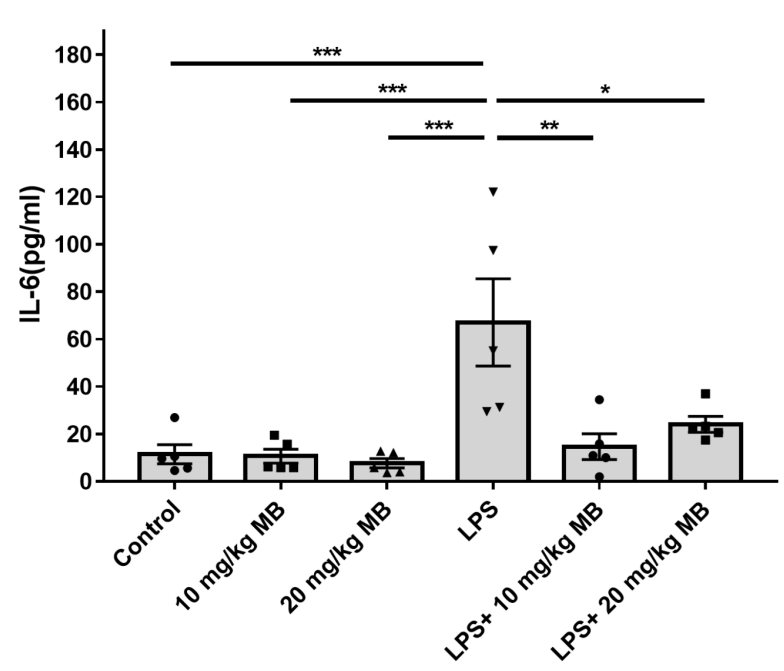
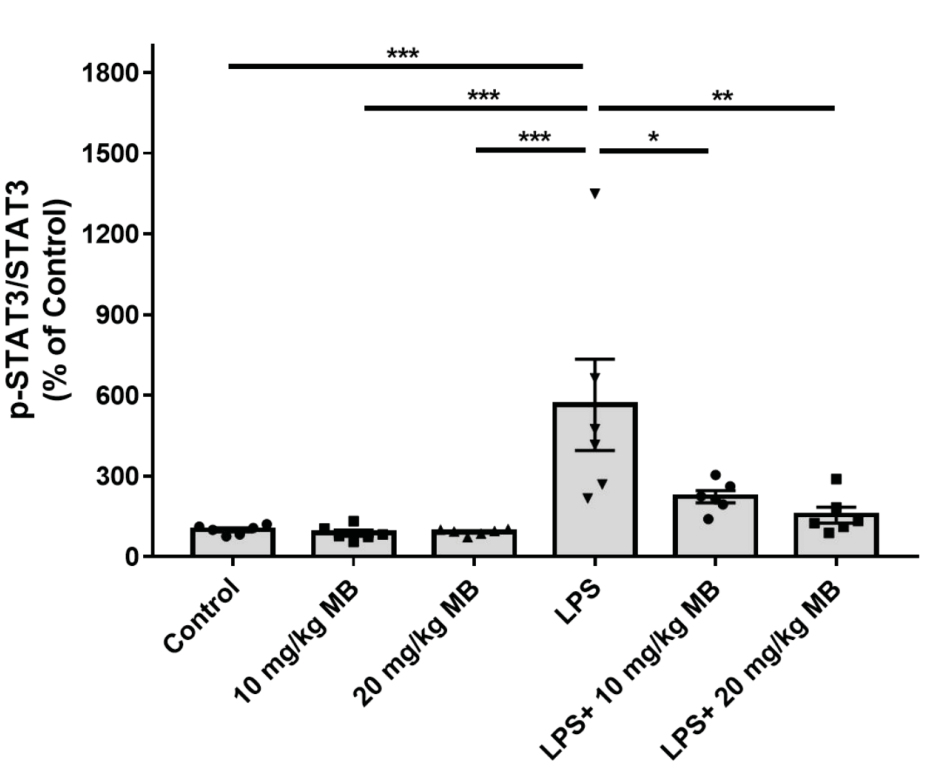
Mice treated with both 10 and 20 mg/kg methylene blue alongside LPS showed a significant reduction in serum levels of LPS-induced IL-6 (Figure 5) and STAT3 (Figure 6). Other markers of inflammation that were reduced after methylene blue treatment were iNOS (inducible nitric oxide synthase, which can induce or enhance the inflammatory response) and COX2 (an enzyme implicated in inflammation by producing prostaglandins).

Figure 5: Effect of methylene blue on serum levels of LPS-induced IL-6 levels on mice treated with methylene blue alone or combined with LPS. The mice treated with LPS and both 10 and 20 mg/kg showed significant reductions in serum IL-6 compared to LPS alone.[13]Li, Y., Ying, W. (2023). Methylene blue reduces the serum levels of interleukin-6 and inhibits STAT3 activation in the brain and the skin of lipopolysaccharide-administered mice. Frontiers in … Continue reading}

Figure 6: Effect of methylene blue on LPS-induced p-STAT3/STAT3 ratios in the skin tissue of mice treated with methylene blue alone or combined with LPS. Methylene blue significantly reduced LPS-induced increases in pSTAT3/STAT3 ratio.[14]Li, Y., Ying, W. (2023). Methylene blue reduces the serum levels of interleukin-6 and inhibits STAT3 activation in the brain and the skin of lipopolysaccharide-administered mice. Frontiers in … Continue reading
Based on the positive effects seen in these studies, methylene blue could assist in hair growth through several mechanisms:
- Reduction of Oxidative Stress (ROS Regulation)
Hair follicle stem cells and dermal papilla cells are highly susceptible to oxidative stress, which can impair hair follicle cycling and contribute to hair loss. Methylene blue has demonstrated the ability to effectively scavenge reactive oxygen species (ROS), reducing oxidative damage and potentially improving hair follicle resilience and function.
- Enhancement of Mitochondrial Function and ATP Production
Hair follicles require significant energy (ATP) for active growth during the anagen phase. Methylene blue has been shown to enhance mitochondrial function, increase ATP production, and improve cellular energy metabolism, which may support hair follicle growth and maintenance.
- Stimulation of Fibroblast Proliferation and Extracellular Matrix Support
Dermal fibroblasts and dermal papilla cells play crucial roles in hair follicle anchoring and signaling. Methylene blue can enhance fibroblast proliferation and extracellular matrix production, which could promote a supportive environment for robust hair follicle development.
- Anti-Senescence Effects
Cellular senescence in hair follicle stem cells is linked to age-related hair thinning and loss. Methylene blue has been found to reduce markers of cellular senescence, such as p16 and β-galactosidase expression, which may help maintain hair follicle stem cell viability and prolong the anagen phase in aging individuals.
- Upregulation of Antioxidant Response (Nrf2 Activation)
Methylene blue activates Nrf2, a transcription factor involved in cellular defense against oxidative stress. Since Nrf2 is associated with protection against chemotherapy-induced alopecia and inflammatory hair loss conditions (e.g., lichen planopilaris), its activation by methylene blue could offer therapeutic benefits for hair regrowth.
- Improvement in Wound Healing and Scalp Thickness
A healthy scalp environment is critical for hair follicle regeneration. Methylene blue has been shown to promote wound healing, increase skin thickness, and enhance tissue hydration, which may contribute to a more favorable microenvironment for hair growth.
- Reduction of Inflammatory Markers
Chronic inflammation, mediated by IL-6 and STAT3 activation, is implicated in autoimmune and scarring alopecia (e.g., alopecia areata, central centrifugal cicatricial alopecia (CCCA)). Methylene blue can significantly reduce inflammatory markers such as IL-6 and STAT3, potentially mitigating inflammatory hair loss conditions.
What Clinical Evidence Shows Methylene Blue’s Positive Effects?
The only evidence that we could find in humans showing positive effects from methylene blue are those surrounding neurodegenerative diseases and cognitive enhancement.
Neurodegenerative diseases
A double-blind, dose-finding Phase II clinical trial involving 321 patients with mild-to-moderate Alzheimer’s disease tested three doses of methylene blue.[15]Wischik, C.M., Staf, R.T., Wischik, D.J., Bentham, P., Murray, A.D., Storey, J., Kook, K.A., Harrington, C.R. (2015). Tau Aggregation Inhibitor Therapy: An Exploratory Phase 2 Study in Mild or … Continue reading
The study met its predefined primary efficacy endpoint at 24 weeks of reduction in cognitive decline at the 138 mg/day dose. The beneficial effect was sustained for 50 weeks in both mild and moderate subjects at this dose, with a 90% reduction in the rate of cognitive decline overall.
Cognitive enhancement
In a randomized controlled trial involving 26 healthy subjects aged 22-62, low-dose methylene blue (280 mg) improved memory performance and increased brain activity in regions associated with attention and short-term memory.[16]Rodriguez, P., Zhou, W., Barrett, D.W., Altmeyer, W., Gutierrez, J.E., Li, J., Lancaster, J., Gonzalez-Lima, F., Duong, Q.T. (2016). Multimodal Randomized Functional MR Imaging of the Effects of … Continue reading
Do These Results Show That Methylene Blue Can Regrow Hair?
While methylene blue has shown potential in preclinical studies for various therapeutic applications, its efficacy in promoting hair regrowth remains unproven. The enthusiasm surrounding the potential benefits of methylene blue is primarily based on in vitro and animal studies, which often do not translate directly to human outcomes.
As you can see above, preclinical studies have demonstrated that methylene blue possesses antioxidant properties, improves mitochondrial function, and exhibits anti-inflammatory effects. However, we could not find any preclinical or clinical studies looking at its potential effects on hair regrowth, so we can’t say for sure whether it will work or not.
In fact, the only study we could find that included methylene blue and hair follicles is a pilot study testing methylene blue as a storage solution during hair transplants. In this study, normal saline solution outperformed methylene blue in graft survival rates at 8, 12, and 18 months post-surgery.[17]Tangjaturonrusamee, C., Thientaworn P., Arunrattanapong, N., Castillejos, D.K.O., Patjomvanich, D. (2016). Methylene blue: Its Efficacy and Safety as a Storage Solution in Hair Transplantation. … Continue reading
Potential Safety Risks
While methylene blue is considered to be safe at therapeutic doses, it can cause some side effects:[18]Michael. (2025). Is Methylene Blue Safe for Long-Term Use? Covenant Health Products. Available at: https://covenanthealthproducts.com/our-blog/is-methylene-blue-good-for-you (Accessed: March 2025),[19]Drugs.com. (2024). Methylene Blue Side Effects. Drugs.com. Available at: https://www.drugs.com/sfx/methylene-blue-side-effects.html (Accessed: March 2025)
- Common: Skin/urine discoloration, nausea, dizziness, and headaches.
- Severe: Serotonin syndrome (when combined with SSRIs/SNRIs), hemolytic anemia in G6PD-deficient individuals, and rate causes of organ toxicity.
There is also some evidence that prolonged use may strain liver and kidney function due to metabolism demands. Furthermore, there have been no rigorous studies confirming the safety of chronic, low-dose methylene blue use for cosmetic purposes.
Risk vs. Reward: Is It Worth It?
Considering the potential side effects, drug interactions and lack of evidence, we would say that it is currently not worth trying methylene blue to counteract your hair loss. Long-term safety data for methylene blue has not been collected at this point, so it is worth waiting until new research has been conducted.
Final Thoughts
While methylene blue shows promise in anti-aging and cellular health, there’s no clinical evidence supporting its use for hair regrowth. Most findings come from in vitro and animal studies, which don’t always translate to real-world results.
Beyond the lack of evidence, potential risks—including drug interactions and unknown long-term effects—make it a high-risk, low-reward option for hair loss. Until human trials confirm its efficacy and safety, methylene blue remains speculative. For now, clinically tested treatments are the safer bet.
References[+]
References ↑1 PubChem. (no date). Methylene Blue. National Library of Medicine. Available at: https://pubchem.ncbi.nlm.nih.gov/compound/Methylene-Blue (Accessed: March 2025) ↑2 Hernandez, J.J., Pryszlak, M., Smith, L., Yanchus, C., Kurji, N., Shahani, V.M., Molinski, S.V. (2017). Giving Drugs a Second Chance: Overcoming Regulatory and Financial Hurdles in Repurposing Approved Drugs as Cancer Therapeutics. Frontiers in Oncology. 7(273). Available at: https://doi.org/10.3389/fonc.2017.00273 ↑3 Xue, H., Thaivalappil, A., Cao, K. (2021). The Potentials of Methylene Blue as an Anti-Aging Drug. Cells. 10(3379). 1-12. Available at: https://doi.org/10.3390/cells10123379 ↑4 Labunskyy, V.M., Galdyshev, N.M. (2013). Role of Reactive Oxygen Species-Mediated Signaling in Aging. Antioxidants & Redox Signaling. 19(12). 1362-1372. Available at: https://doi.org/10.1089/ars.2012.4891 ↑5 Xiong, Z-M., O’Donovan, M., Sun, L., Choi, J.Y., Ren, M., Cao, K. (2017). Anti-aging potentials of methylene blue for human skin longevity. Scientific Reports. 7(2475). 1-12. Available at: https://doi.org/10.1038/s41598-017-02419-3 ↑6, ↑7 Xiong, Z-M., O’Donovan, M., Sun, L., Choi, J.Y., Ren, M., Cao, K. (2017). Anti-aging potentials of methylene blue for human skin longevity. Scientific Reports. 7(2475). 1-12. Available at: https://doi.org/10.1038/s41598-017-02419-3 Figure used in line with the Creative Commons License: https://creativecommons.org/licenses/by/4.0/ ↑8 Xiong, Z-M., Mao, X., Trappio, M., Arya, C., el Kordi, J., Cao, K. (2021). Ultraviolet radiation protection potentials of methylene blue for human skin and coral reef health. Scientific Reports. 11(10871). 1-9. Available at: https://doi.org/10.1038/s41598-021-89970-2 ↑9, ↑10 Xiong, Z-M., Mao, X., Trappio, M., Arya, C., el Kordi, J., Cao, K. (2021). Ultraviolet radiation protection potentials of methylene blue for human skin and coral reef health. Scientific Reports. 11(10871). 1-9. Available at: https://doi.org/10.1038/s41598-021-89970-2 Figure used in line with the Creative Commons License: https://creativecommons.org/licenses/by/4.0/ ↑11 Li, Y., Ying, W. (2023). Methylene blue reduces the serum levels of interleukin-6 and inhibits STAT3 activation in the brain and the skin of lipopolysaccharide-administered mice. Frontiers in Immunology. 14(1181932). Available at: https://doi.org/10.3389/fimmu.2023.1181932 ↑12 Roche, F.C., Hedberg, M.L. Fischer, A.S., Ray, A., Dentchev, T., Rice, X., Taylor, S.C., Seykora, J.T. (2023). Activation of STAT3 in lymphocytes associated with central centrifugal cicatricial alopecia. 89(6). 1245-1246. Available at: https://doi.org/10.1016/j.jaad.2023.01.045 ↑13, ↑14 Li, Y., Ying, W. (2023). Methylene blue reduces the serum levels of interleukin-6 and inhibits STAT3 activation in the brain and the skin of lipopolysaccharide-administered mice. Frontiers in Immunology. 14(1181932). Available at: https://doi.org/10.3389/fimmu.2023.1181932 Figure used in line with the Creative Commons License: https://creativecommons.org/licenses/by/4.0/ ↑15 Wischik, C.M., Staf, R.T., Wischik, D.J., Bentham, P., Murray, A.D., Storey, J., Kook, K.A., Harrington, C.R. (2015). Tau Aggregation Inhibitor Therapy: An Exploratory Phase 2 Study in Mild or Moderate Alzheimer’s Disease. 44(2). 705-720. Available at: https://doi.org/10.3233/JAD-142874 ↑16 Rodriguez, P., Zhou, W., Barrett, D.W., Altmeyer, W., Gutierrez, J.E., Li, J., Lancaster, J., Gonzalez-Lima, F., Duong, Q.T. (2016). Multimodal Randomized Functional MR Imaging of the Effects of Methylene Blue in the Human Brain. Radiology. 281(2). 516-526. Available at: https://doi.org/10.1148/radiol.2016152893 ↑17 Tangjaturonrusamee, C., Thientaworn P., Arunrattanapong, N., Castillejos, D.K.O., Patjomvanich, D. (2016). Methylene blue: Its Efficacy and Safety as a Storage Solution in Hair Transplantation. International Society of Hair Restoration Surgery. 26(5). 194-196. Available at: https://doi.org/10.33589/26.5.0194 ↑18 Michael. (2025). Is Methylene Blue Safe for Long-Term Use? Covenant Health Products. Available at: https://covenanthealthproducts.com/our-blog/is-methylene-blue-good-for-you (Accessed: March 2025) ↑19 Drugs.com. (2024). Methylene Blue Side Effects. Drugs.com. Available at: https://www.drugs.com/sfx/methylene-blue-side-effects.html (Accessed: March 2025) Seborrheic dermatitis is a common, chronic inflammatory skin condition that primarily affects areas with a high concentration of sebaceous (oil-producing) glands, such as the scalp, face, upper back, and chest. It is characterized by red, itchy patches of skin covered with greasy, yellowish scales or flakes.
In the scalp, seborrheic dermatitis is also called dandruff. It can vary widely in symptoms and severity, and a number of treatment options are marketed to treat and prevent dandruff. But what is actually happening to your scalp and hair follicles when seborrheic dermatitis hits, and what are the best treatment combinations? Let’s find out below.
Key Takeaways
- What is it? Seborrheic dermatitis is a chronic inflammatory skin condition that affects areas rich in oil glands, like the scalp, causing red, itchy patches with greasy, yellowish flakes.
- What are the symptoms? Symptoms include visible flakes (dandruff), itchiness, redness, and, in severe cases, crusting and hair shafts around hair follicles.
- What Is The Prevalence of Seborrheic Dermatitis in Patients with AGA? One study found that out of 250 patients with AGA, 56.9% also had seborrheic dermatitis.
- What are the most common treatments? Antifungal topicals are most often used (e.g., ketoconazole and selenium sulfide), topical corticosteroids, and newer options like roflumilast foam to reduce inflammation and yeast overgrowth.
- How else can I improve it? Lifestyle changes, like reducing stress, eating a balanced diet, and avoiding known triggers like harsh hair products or cold weather, can help manage symptoms.
- Final thoughts. Managing seborrheic dermatitis often involves trial and error with different therapies, but with the right combination, most people can achieve long-term symptom control.
What Are the General Features of Seborrheic Dermatitis?
- Appearance: The condition manifests as oily patches with yellow or white scales, which may appear darker or lighter in people of color and redder in those with white skin.
- Common locations: Scalp, face, sides of the nose, eyebrows, ears, eyelids, chest, armpits, and groin area.
- Symptoms: Itching, flaking skin, and sometimes a ring-shaped (annular) rash called petaloid seborrheic dermatitis.
Why Does Seborrheic Dermatitis of the Scalp Happen?
Seborrheic dermatitis of the scalp (also called dandruff) occurs due to a combination of factors, one of which is sebum production. The condition primarily affects areas with a high concentration of sebaceous glands, including the scalp.[1]Ro, B.I., Dawson, T.L. (2005). The role of sebaceous gland activity and scalp microfloral metabolism in the etiology of seborrheic dermatitis and dandruff. The Journal of Investigative Dermatology. … Continue reading Excess sebum creates a favorable environment for the growth of Malassezia yeasts, which are naturally present on the skin.
Another factor is the overgrowth of Malassezia yeasts. Malassezia species, particularly M.globosa and M.restricta, are commonly found on the scalps of individuals with seborrheic dermatitis. These yeasts are normally harmless but can trigger an inflammatory response when they overgrow.[2]Wikramanayake, T.C., Borda, L.J., Miteva, M., Paus, R. (2019). Seborrheic dermatitis-looking beyond Malassezia. Experimental Dermatology. 28(9). 991-1001. Available at: … Continue reading
Malessezia lipase breaks down human sebum, releasing free fatty acids (FFAs) and other metabolites. These FFAs can penetrate the stratum corneum (the outer layer of the skin), altering skin barrier permeability and leading to inflammation and abnormal keratinization, which are key features of seborrheic dermatitis.[3]Dawson Jr. (2007). Malassezia globosa and restricta: breakthrough understanding of the etiology and treatment of dandruff and seborrheic dermatitis through whole-genome analysis. Journal of … Continue reading
Genetic predisposition is also a contributing factor in the pathogenesis of seborrheic dermatitis.[4]Karakadze, M.A., Hirt, P.A., Wikramanayake, T.C. (2018). The genetic basis of seborrheic dermatitis: a review. Journal of the European Academy of Dermatology and Venereology. 32(4). 529-536. … Continue reading Several gene mutations and protein deficiencies have been associated with the condition or similar phenotypes. The affected genes are involved in the immune response (e.g., ACT1, C5, IKBG/NEMO) and epidermal maturation (differentiation) (e.g., ZNF750, MPZL3).
Other genetic mutations that can affect the complement system, which is part of the immune response, have been associated with an increased risk of seborrheic dermatitis. This dysfunction can lead to an inability to effectively restrict the growth of Malassezia.[5]Adalsteinsson, J.A., Kaushik, S., Muzumdar, S., Guttman-Yassky, E., Ungar, J. (2020). An update on the microbiology, immunology, and genetics of seborrheic dermatitis. Experimental Dermatology. … Continue reading
In addition to these, a number of other elements can influence the development of seborrheic dermatitis and its exacerbation. These include immune system abnormalities, such as reduced numbers of helper T cells.[6]Bergbrant, I.M., Johansson, S., Robbins, D., Scheynius, A., Faergemann, J., Soderstrom, T. (1991). An immunological study in patients with seborrheic dermatitis. Clinical and Experimental … Continue reading Hormonal changes can also aggravate the condition.[7]Kashiri, A., Maghsoudloo, N. (2024). Exploring the Impact of Vitamin D and Zinc Deficiencies on Sebhorreic Dermatitis: A Comparative Study. Health Science Reports. 7(12). E70283. Available at: … Continue reading Furthermore, cold weather can worsen symptoms, and stress can trigger or exacerbate flare-ups.
What Are the Symptoms of Seborrheic Dermatitis in the Scalp?
We can split the symptoms of seborrheic dermatitis into three levels: cosmetic, symptom, and microscopic levels.
Cosmetic Level
At the cosmetic level, the most noticeable sign of seborrheic dermatitis on the scalp is the presence of visible flakes on the scalp, which may fall onto clothing. These flakes can range from mild dandruff to more severe scaling.[8]Schwartz, R.A., Janusz, C.A., Janniger, C.K. (2006). Seborrheic dermatitis: an overview. American Family Physician. 74(1). 125-130. Available at: PMID:16848386 The scales often appear greasy and may have a yellow-brown color. In more pronounced cases, you might see white or yellowish scales covering patches of skin on the scalp. These scales can sometimes form crusts, especially in areas where the scalp meets the hairline or behind the ears. The flakiness can be accompanied by noticeable redness (erythema) and bumps or pustules.[9]Saunte, D.M., Gaitanis, G., Hay, R.J. (2020). Malassezia-Associated Skin Diseases, the Use of Diagnostics and Treatment. Frontiers in Cellular and Infection Microbiology. 10. 112. Available at: … Continue reading

Figure 1: Scalp seborrheic dermatitis can present as scaling and redness.[10]DermNet. (no date). Seborrheic Dermatitis. Available at: https://dermnetnz.org/imagedetail/2050-seborrhoeic-dermatitis (Accessed: February 2025)
Symptom Level
On a symptom level, itchiness (pruritis) is often the most bothersome aspect of seborrheic dermatitis.[11]Zhang, F., Li, Y., Ren, W., Li, S. (2023). Establishment of clinical evaluation criteria for scalp seborrheic dermatitis. Journal of Cosmetic Dermatology. 22(11). 3042-3046. Available at: … Continue reading The itching can range from mild to intense and may lead to scratching, which can further irritate the scalp and, in some cases, cause hair loss.[12]National Eczema Associations. (no date). Seborrheic Dermatitis. Available at: https://nationaleczema.org/eczema/types-of-eczema/seborrheic-dermatitis/ (Accessed: February 2025) Some people may experience soreness or tenderness in the affected areas, especially if the condition is severe and there has been excessive scratching. In the most severe cases, the rash may weep or ooze, leading to the formation of crusts.
Microscopic Level
At the microscopic level, several distinctive factors characterize seborrheic dermatitis. One of the most notable is the presence of dandruff casts, which are accumulations of dead skin cells and sebum around hair shafts.[13]Franca, K., Villa, R.T., Silva, I.R., de Carvalho, C.A., Bedin, V. (2011). Hair Casts or Pseudonits. International Journal of Trichology. 3(2). 121-122. Available at: … Continue reading These casts are typically white, firm, and tubular in shape and can range from 2 to 7 mm in length.

Figure 2: Presence of hair casts in a 12-year-old girl with seborrheic dermatitis.[14]Kaliyadan, F., Ashique, K.T. (2019). Hair Casts and Nits – Differentiating Using Dermoscopy. Images in Clinical Practice. 85(4). 434-435. Available at: https://doi.org/10.4103/ijdvl.IJDVL_815_17
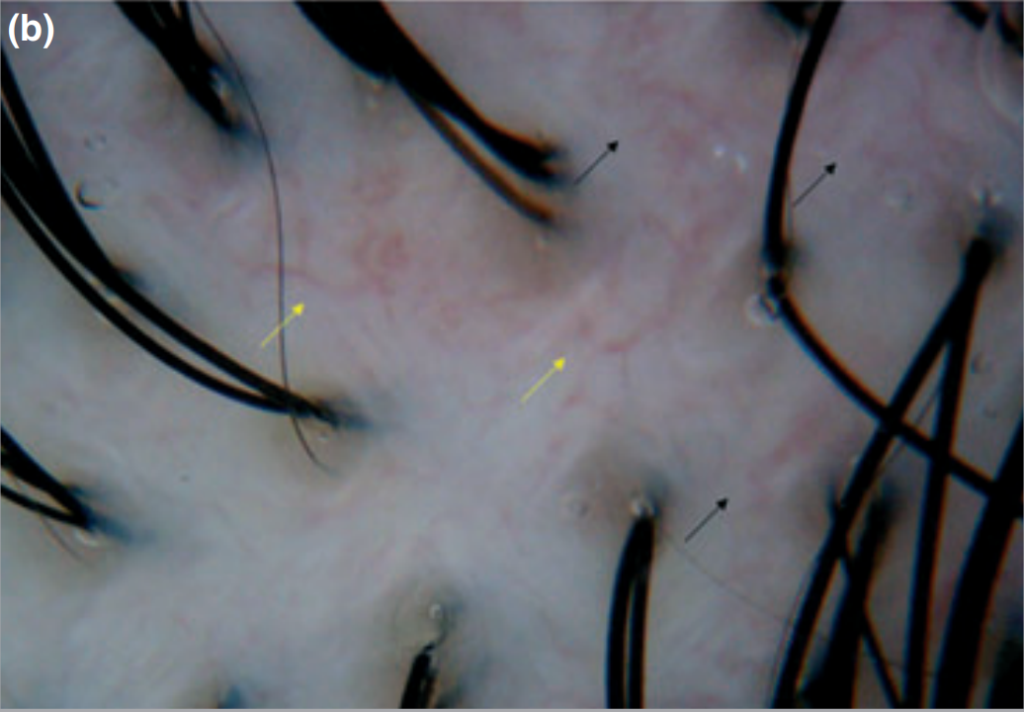
Several characteristic vascular patterns can be observed in seborrheic dermatitis under dermoscopy, a noninvasive imaging tool.[15]Kim, G.W., Jung, H.J., Ko, H-C., Kim, M.B., Lee, W-J., Lee, S-J., Kim, D-W., Kim, B-S. (2011). Dermoscopy can be useful in differentiating scalp psoriasis from seborrheic dermatitis. British Journal … Continue reading These include arborizing red lines (ARL), which appear as branching blood vessels, and twisted red loops (TRL), which are coiled blood vessels specific to seborrheic dermatitis. Comma vessels (CV) and short-curved blood vessels are also indicative of this condition. These vascular patterns help differentiate seborrheic dermatitis from other skin conditions.

Figure 3: Aborizing vessels (indicated by yellow arrows) and atypical red vessels (indicated by black arrows) in seborrheic dermatitis.[16]Kim, G.W., Jung, H.J., Ko, H-C., Kim, M.B., Lee, W-J., Lee, S-J., Kim, D-W., Kim, B-S. (2011). Dermoscopy can be useful in differentiating scalp psoriasis from seborrheic dermatitis. British Journal … Continue reading
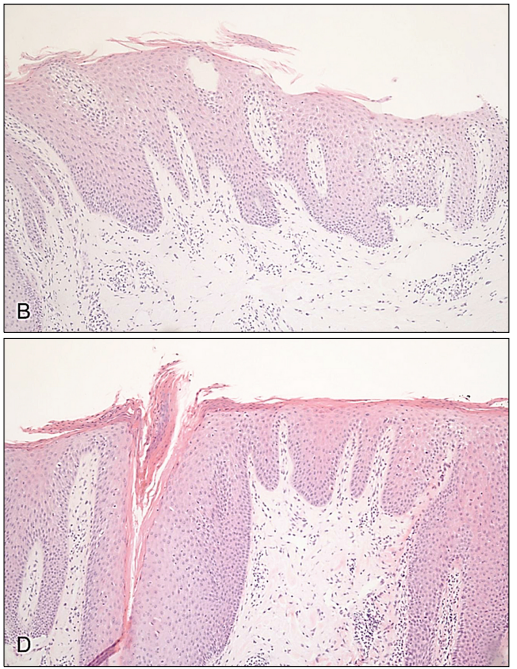
In addition to these, other microscopic characteristics include spongiosis (buildup of fluid between skin cells in the epidermis) in acute seborrheic dermatitis lesions, psoriasiform hyperplasia (thickening of the epidermis), swelling, and infiltration of antibodies.[17]Park, J-H., Park, Y.J., Kim, S.K., Kwon, J.E., Kang, Y.H., Lee, E-S., Choi, J.H., Kim, Y.C. (2016). Histopathological Differential Diagnosis of Psoriasis and Seborrheic Dermatitis of the Scalp. … Continue reading In some cases, the opening of a hair follicle can become blocked with excess skin cells (follicular plugging), and maturation (differentiation) of keratinocytes can become impaired, leading to cells in the stratum corneum retaining nuclei (shoulder parakeratosis). This contributes to the scaling characteristic of seborrheic dermatitis.
As epidermal cells differentiate through the skin layers, they usually lose their nuclei and become filled with keratin. By the time they reach the stratum corneum, they are typically flat, dead cells without nuclei, forming a protective barrier.[18]Alberts, B., Johnson, A., Lewis J. Molecular Biology of the Cell. 4th edition. New York: Garland Science; 2002. Epidermis and Its Renewal by Stem Cells. Available from: … Continue reading

Figure 4: Seborrheic dermatitis can cause (B) shoulder parakeratosis (where an abnormally large number of keratinocytes retain their nuclei in the stratum corneum) and (D) follicular plugging (where the opening of the hair follicle becomes blocked with excess epidermal cells).[19]Park, J-H., Park, Y.J., Kim, S.K., Kwon, J.E., Kang, Y.H., Lee, E-S., Choi, J.H., Kim, Y.C. (2016). Histopathological Differential Diagnosis of Psoriasis and Seborrheic Dermatitis of the Scalp. … Continue reading
How Common is Seborrheic Dermatitis?
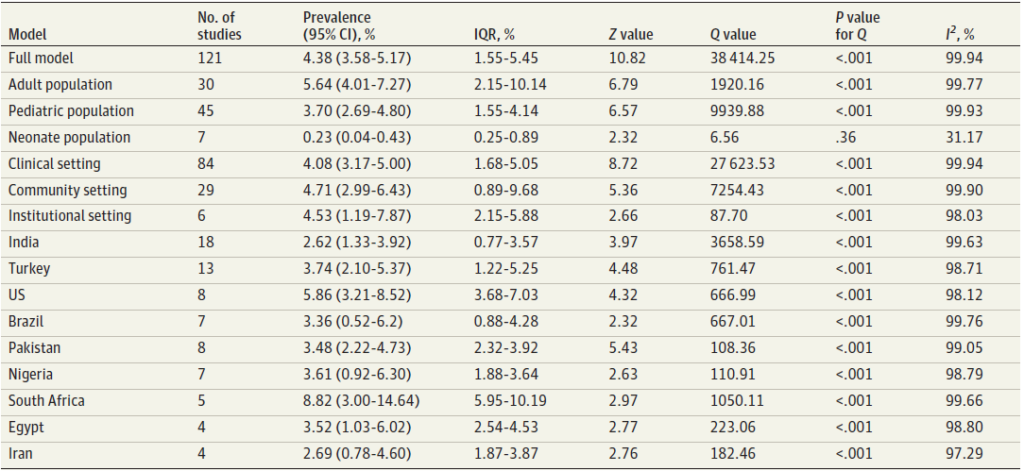
A comprehensive meta-analysis published in JAMA Dermatology in 2024 found that the global pooled prevalence (meaning all body locations, including the scalp) of seborrheic dermatitis is 4.38%, which is higher than previous large-scale global estimates.[20]Polaskey, M.T., Chang, C.H., Daftary, K., Fakhraie, S., Miller, C.H., Chovatiya, R. (2024). The Global Prevalence of Seborrheic Dermatitis: A Systematic Review and Meta-Analysis. JAMA Dermatology. … Continue reading In the US, the prevalence is 5.86%, which appears to be middle-of-the-road compared to places like South Africa, which has a prevalence of 8.82%, and India, with a prevalence of 2.62%.

Figure 5: The prevalence of seborrheic dermatitis (%) split by age, community, or country.[21]Polaskey, M.T., Chang, C.H., Daftary, K., Fakhraie, S., Miller, C.H., Chovatiya, R. (2024). The Global Prevalence of Seborrheic Dermatitis: A Systematic Review and Meta-Analysis. JAMA Dermatology. … Continue reading
Is Seborrheic Dermatitis More Common in People with Pattern Hair Loss?
Recent studies have shown a significant association between seborrheic dermatitis and androgenic alopecia (AGA).
- One five-year study from 2006 to 2010 found that seborrheic dermatitis was the most commonly associated disease in both men and women with AGA.[22]Jang, W.S., Son, I.P., Yeo, K.I., Park, K.Y., Li, K., Kim, B.J., Seo, S.J., Kim, M.N., Hong, C.K. (2013). The Annual Changes of Clinical Manifestation of Androgenetic Alopecia Clinic in Korean Males … Continue reading
- A retrospective study published in 2024 found that out of 250 patients with AGA, 56.9% also had seborrheic dermatitis.[23]Faghihkhorasani, A., Sadeghzadeh, A., Goodarzi, A., Rohaninasab, M. (2024). The Relationship between Seborrheic Dermatitis and Androgenetic Alopecia in Patients Referred to a Skin Clinic in Tehran, … Continue reading
- A significant correlation was found between the pattern of AGA in men and the severity of seborrheic dermatitis.
- A significant relationship was also observed between dandruff symptoms and AGA patterns.
- In men, the highest severity of seborrheic dermatitis (grade 3) was related to the Hamilton Norwood type 2 pattern of hair loss (triangular hair loss on both sides of the frontoparietal line).
- In women, the highest severity of seborrheic dermatitis (grade 2) was observed in the Ludwig type 2 hair loss pattern (thinning of hair about 1-3 cm behind the hairline).
What Is the Biology Behind This Correlation?
Although there is no established explanation, there are several factors that could explain the correlation between seborrheic dermatitis and AGA.
- Androgen sensitivity: Both conditions are influenced by androgens, particularly dihydrotestosterone (DHT). The enzyme 5-alpha reductase (5-AR) converts testosterone to DHT, which affects both sebum production and hair follicle miniaturization.[24]Kim, B.J., Kim, J.Y., Eun, H.C., Kwon, O.S., Kim, M.N. (2006). Androgenetic alopecia in adolescents: A report of 43 cases. The Journal of Dermatology. 33(10). 696-699. Available at: … Continue reading
- Sebum production: Increased sebum production is characteristic of both conditions. In AGA, there are increased levels of 5-AR in the follicles of the temporal, frontal, and crown regions.[25]Kure, K., Isago, T., Hirayama, T. (2015). Changes in the sebaceous gland in patients with male pattern hair loss (androgenic alopecia). Journal of Cosmetic Dermatology. 14(3). 178-184. Available at: … Continue reading This excess sebum creates an environment conducive to the overgrowth of Malassezia yeast.
- Microbiome imbalance (dysbiosis): Patients with AGA exhibit scalp dysbiosis, with an increased abundance of Cutibacterium and a decreased abundance of Corynebacterium.[26]Suzuki, K., Inoue, M., Cho, O., Mizutani, R., Shimizu, Y., Nagahama, T., Sugita, T. (2021). Scalp microbiome and sebum composition in Japanese male individuals with and without androgenetic alopecia. … Continue reading This altered microbiome may contribute to inflammation and exacerbate both conditions.
- Malassezia yeast: Malassezia restricta is more abundant on the scalps of patients with AGA and is also implicated in seborrheic dermatitis, which may exacerbate the condition.
While there is no established causality for AGA and seborrheic dermatitis, these underlying factors mean that seborrheic dermatitis and AGA can exacerbate one another.
So, what can you do to treat seborrheic dermatitis on the scalp?
What Are the Typical Treatments for Seborrheic Dermatitis on the Scalp?
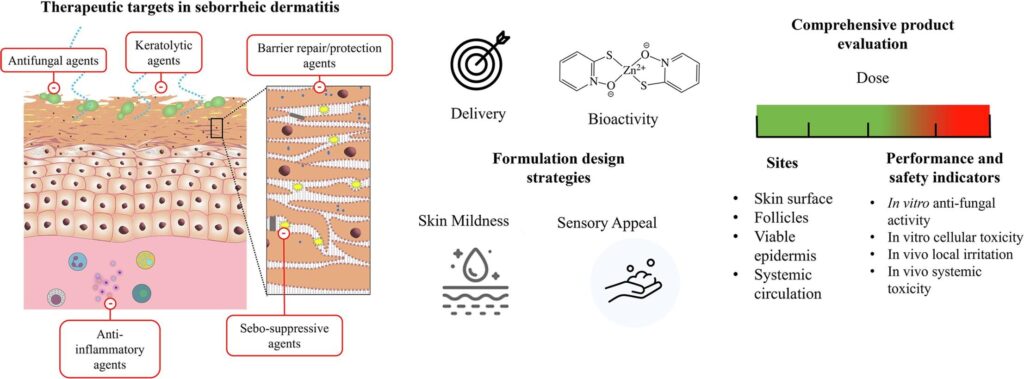
Seborrheic dermatitis of the scalp can be managed through various treatment options. It can be attacked in multiple ways, such as through the use of antifungals, anti-inflammatories, treatments that suppress sebum, corticosteroids, and topical keratolytic agents.

Figure 6: Therapeutic Targets in Seborrheic Dermatitis.[27]Mangion, S.E., Mackenzie, L., Roberts, M.S., Holmes, A.M. (2023). Seborrheic dermatitis: topical therapeutics and formulation design. European Journal of Pharmaceutics and Biopharmaceutics. 185. … Continue reading
FDA-Approved Options
Among the FDA-approved treatments, Roflumilast foam 0.3% (Zoryve) is a recent addition, approved on December 2023, for treating seborrheic dermatitis in individuals aged 9 and older.[28]Arcutis Biotherapeutics. (no date). FDA Approves Arcutis’ ZORYVE (roflumilast) Topical Foam, 0.3% for the Treatment of Seborrheic Dermatitis in Individuals Aged 9 Years and Older. Available at: … Continue reading This treatment is a topical non-steroidal phosphodiesterase 4 (PDE4) inhibitor. PDE4 plays a key role in the inflammatory response, so by inhibiting this, it reduces inflammation and associated symptoms like redness, scaling, and itching.[29]Zirwas, M.J., Draelos, Z.D., DuBois, J., Kircik, L.H., Moore, A.Y., Gold, L.S., Alonso-Llamazares, J., Bukhalo, M., Bruce, S., Eads, K., Green, L.J., Guenthner, S., Ferris, L.K., Forman, S.B., … Continue reading
Ketoconazole is FDA-approved for patients 12 years of age and older with healthy immune systems. It acts through multiple mechanisms to treat seborrheic dermatitis in the scalp. It inhibits the production of lanosterol, a precursor for ergosterol biosynthesis, which is essential for fungal membrane integrity.[30]Tynes, B.E., Johnson, C.D., Vaish, M.H., Abbott, B., Vucenovic, J., Varrassi, G., Potharaju, P., Torres, Y.L., Lee, Z., Ahmadzadeh, S., Shekoohi, S., Kaye, A.D. (2024). Ketoconazole Shampoo for … Continue reading
This halts the growth of Malassezia yeasts associated with seborrheic dermatitis. It also strongly binds to the cytochrome p450 mono-oxygenase complex, hindering the fungal biosynthesis of triglycerides and phospholipids and shifting sebum secretion in the stratum corneum, addressing the hypersecretion of sebum characteristic of the condition.[31]Borgers, M., Degreed, H. (2007). The Role of Ketoconazole in Seborrheic Dermatitis. Therapeutics for the Clinician. 80. 359-363. Available at: … Continue reading
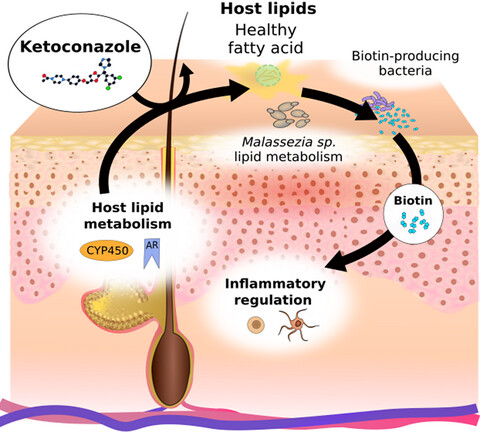
Ketoconazole also exhibits anti-inflammatory properties and antiproliferative effects and may favor biotin-producing bacteria, which could improve the skin microbiome.[32]Goularte-Silva, V., Paulino, C.L. (2021). Ketoconazole beyond antifungal activity: Bioinformatics-based hypothesis on lipid metabolism in dandruff and seborrheic dermatitis. Experimental Dermatology. … Continue reading

Figure 7: Effect of Ketoconazole on Malassezia lipid metabolism and biotin-producing bacteria.[33]Goularte-Silva, V., Paulino, C.L. (2021). Ketoconazole beyond antifungal activity: Bioinformatics-based hypothesis on lipid metabolism in dandruff and seborrheic dermatitis. Experimental Dermatology. … Continue reading
Ciclopirox shampoo is approved for people 16 years of age and older with seborrheic dermatitis on the scalp. It works differently from other common antifungals. It acts like a magnet for certain metals, especially iron and aluminum, which are important for fungal survival.[34]LOPROX® (cicloporox) Shampoo 1%. (2006). MEDICIS Pharmaceutical Corp. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2006/021159s009lbl.pdf (Accessed: February 2025) By grabbing these metals, ciclopirox prevents important fungal enzymes from working properly, leading to peroxide build-up and cellular damage.
Other Treatments
Some over-the-counter treatments are used to treat seborrheic dermatitis. These are often antifungal shampoos containing ingredients such as:
- Selenium sulfide: A treatment with antifungal, cytostatic, keratolytic, anti-inflammatory, and sebum regulatory properties. In clinical studies, 2.5% selenium sulfide shampoo improved dandruff scores by 78.3% after 4 weeks.[35]Godse, G., Godse, K. (2024). Safety, Efficacy and Attributes of 2.5% Selenium Sulfide Shampoo in the Treatment of Dandruff: A Single-Center Study. Cureus. 16(3). E57148. Available at: … Continue reading
- Coal tar: This helps to reduce inflammation and redness associated with seborrheic dermatitis and has antifungal and keratolytic properties. It also slows the rate of skin cell production, helping to minimize the buildup of scales and dry patches. However, it has been found to be less effective than ciclopirox and ketoconazole.[36]Davies, D.B., Boorman, G.C., Shuttleworth, D. (1999). Comparative efficacy of shampoos containing coal tar (4.0% w/w; Tarmed), coal tar (4.0% w/w) plus ciclopirox olamine (1.0% w/w Tarmed AF), and … Continue reading
- Salicylic acid: Salicylic acid helps to slough off dead skin cells and remove flakes from the scalp, which can be beneficial for those with seborrheic dermatitis. It also has keratolytic, oil-controlling, anti-inflammatory, and anti-fungal effects.[37]Ge, L., Liu, Z., Xu, S., Li, C., Jin, M., Luo, Y., Kong, Y., Meng, J., Zheng, G., Gao, J., Wang, P., Bai, W., Na, H., Zhou, X., Jin, Z., Pi, L. (2025). A Cohort Clinical Study on the Efficacy of … Continue reading
- Zinc pyrithione: Zinc pyrithione increases cellular copper levels, which damages iron-sulfur clusters of proteins essential for fungal metabolism. This, alongside its antifungal, antibacterial, anti-inflammatory, and sebum-regulatory properties, contributes to its effectiveness in treating seborrheic dermatitis. One study found that a shampoo containing 1% zinc pyrithione was effective in controlling dandruff when used on half of the scalp.[38]Marks, R., Pearse, A.D., Walker, A.P. (1985). The effects of a shampoo containing zinc pyrithione on the control of dandruff. British Journal of Dermatology. 112(4). 415-422. Available at: … Continue reading
- Piroctone olamine: A number of clinical studies have used piroctone olamine alongside other treatments to improve seborrheic dermatitis, with one study showing a clinical improvement of 80%.[39]Ge, L., Liu, Z., Xu, S., Li, C., Jin, M., Luo, Y., Kong, Y., Meng, J., Zheng, G., Gao, J., Wang, P., Bai, W., Na, H., Zhou, X., Jin, Z., Pi, L. (2025). A Cohort Clinical Study on the Efficacy of … Continue reading
Prescription medications such as topical corticosteroids and calcineurin inhibitors may also be used off-label.[40]Paula Ludmann. (2024). Seborrheic Dermatitis: Diagnosis and Treatment. American Academy of Dermatology Association. Available at: … Continue reading UVB light therapy can be used for widespread rash and scales. Other treatments include fluconazole 2%, naftifine hydrochloride 1% gel, and climbazole.[41]Dall’Oglio, F., Nasca, M.R., Gerbino, C., Micali, G. (2022). An Overview of the Diagnosis and Management of Seborrheic Dermatitis. Clinical, Cosmetic and Investigational Dermatology. 6(15). … Continue reading
Lifestyle and Dietary Modifications
In addition to these medical treatments, dietary and lifestyle changes can help manage seborrheic dermatitis.
One case-control study involving 257 participants found associations between white bread, carbonated drinks, and daily fast food, with a higher percentage of seborrheic dermatitis compared to those without the condition.[42]Alshaebi, M., Zahed, L., Osalyan, M., Sulaimani, S., Albahlool, A., Abduljabbar, M.H., Hariri, J. (2023). Association Between Diet and Seborrheic Dermatitis: A Case-Control Study. Cureus. 15(11). … Continue reading The same study reported that increased fruit consumption was associated with a lower risk of seborrheic dermatitis. Furthermore, adherence to a Western diet has been associated with a higher risk of seborrheic dermatitis in female patients.[43]Woolhiser, E., Keime, N., Patel, A., Weber, I., Adelman, M., Dellavalle, R.P. (2024). Nutrition, Obesity, and Seborrheic Dermatitis: Systematic Review. JMIR Dermatology. E50143. Available at: … Continue reading
It is recommended to increase the intake of high-fiber carbohydrates and lean protein foods, as well as foods rich in monounsaturated and omega-3 fatty acids.
Should You Avoid Certain Hair Loss Treatments if You Have Seborrheic Dermatitis?
In our experience, those with seborrheic dermatitis may have problems if they use:
- Topicals containing retinoic acid
- Microneedling
- Scalp massaging
- PRP
- Mesotherapy
These may actually lead to more inflammation, so we would recommend avoiding these until you get your seborrheic dermatitis under control.
Which Treatments Are Best Used for Which Disease Severity?
Management of seborrheic dermatitis of the scalp often involves rotating or combining a number of therapies to target multiple aspects of the disease.
Mild to Moderate Severity
For patients with mild to moderate seborrheic dermatitis, first-line treatments typically include over-the-counter antifungals combined with topical anti-inflammatory agents.
This can include:
- Anti-dandruff shampoos containing 2.5% selenium sulfide or 1-2% zinc pyrithione, used daily or every other day.[44]Paula Ludmann. (2024). Seborrheic Dermatitis: Diagnosis and Treatment. American Academy of Dermatology Association. Available at: … Continue reading
- Ketoconazole shampoo (1-2%) applied for 5-10 minutes before rinsing, used daily initially, then twice weekly for maintenance.
- Topical corticosteroids, like hydrocortisone 1% cream, applied once or twice daily until inflammation clears, then as needed.
- One clinical trial found that the usage of traditional Chinese medicine can also show significant efficacy in treating mild to moderate seborrheic dermatitis without relapse, especially for those with moderate severity.[45]Zhang, F., Li, Y-H., Ren, W., Li, S-R., Chen, Y-C. (2023). Clinical efficacy of a combination treatment of traditional Chinese medicine for scalp seborrheic dermatitis. Journal of Cosmetic … Continue reading
Moderate to Severe
For more severe or persistent cases, treatment may include:
- Oral antifungal medications like itraconazole (200 mg/day for one week, followed by a maintenance dose).[46]Goldenberg, G. (2013). Optimizing Treatment Approaches in Seborrheic Dermatitis. Journal of Clinical and Aesthetic Dermatology. 6(2). 44-49. Available at: PMID: 23441240
- UVB light therapy, with 3 treatment sessions per week for up to 8 weeks. However, some studies have shown relapse within 1 month.[47]Jaalouk, D., Pulumati, A., Algarin, Y.A., Kircik, L., Issa, N.T. (2024). Dermatologic Procedures for the Treatment of Seborrheic Dermatitis. Journal of Drugs in Dermatology. 23(10). 819-824. … Continue reading
- Combination therapy of clobetasol propionate shampoo (0.05%) and ketoconazole (2%) twice weekly has been shown to provide greater efficacy than ketoconazole alone, with a more sustained effect in the treatment of moderate to severe seborrheic dermatitis.[48]Ortonne, J-P., Nikkels, A.F., Reich, K., Oliver, R.M.P., Lee., J.H., Kerrouche, N., Sidou, F., Faergemann, J. (2011). Efficacious and safe management of moderate to severe scalp seborrheic dermatitis … Continue reading
- A recent study conducted on 20 patients with moderate to severe seborrheic dermatitis combined salicylic acid, piroctone olamine, zinc PCA gel, and a cleansing lotion, finding that the combination significantly reduced dandruff, itchiness, redness, and greasiness scores over 4 weeks. Patients with moderate and those with severe seborrheic dermatitis improved to mild with an overall clinical improvement of 80%.[49]Ge, L., Liu, Z., Xu, S., Li, C., Jin, M., Luo, Y., Kong, Y., Meng, J., Zheng, G., Gao, J., Wang, P., Bai, W., Na, H., Zhou, X., Jin, Z., Pi, L. (2025). A Cohort Clinical Study on the Efficacy of … Continue reading
Shampoo Rotations
For people dealing with treatment-resistant seborrheic dermatitis, rotating shampoos may be beneficial. Some of our members have consulted with Dr. Donovan, a leading hair specialist and have experienced success with his approach.
The key to this method is using different active ingredients rather than specific brands. If certain additives in a product don’t suit you, you can opt for alternative with the same active ingredients and concentrations.
- 2% Ketoconazole
- Selenium sulfide
- Coal tar
- Zinc pyrithione
Finding the most effective treatment often requires a trial-and-error approach.[50]University of Utah Health. (no date). Seborrheic Dermatitis. Available at: https://healthcare.utah.edu/dermatology/conditions/seborrheic-dermatitis (Accessed: February 2025) You might be advised by your doctor to start with a basic regimen and assess response after 2-4 weeks. If no improvement has been observed, then your doctor might increase the strength, change the treatment, or add complementary therapies. Once control has been achieved, you can gradually reduce treatment frequency to find the minimal effective maintenance regimen.
When Should You See a Healthcare Professional?
While mild seborrheic dermatitis can be effectively treated with over-the-counter or off-the-shelf treatments, you should see a healthcare professional if any of the following occur:
- Symptoms persist or worsen: If your symptoms don’t improve after using over-the-counter dandruff shampoos for at least two weeks or if they suddenly get worse.[51]Cleveland Clinic. (2020). Seborrheic Dermatitis. Cleveland Clinic. Available at: https://my.clevelandclinic.org/health/diseases/14403-seborrheic-dermatitis (Accessed: February 2025)
- Severity interferes with daily life: When the condition causes anxiety, embarrassment, or disrupts your daily routine.
- Signs of severe disease appear: If you develop yellow-red scaling papules along the hairline, behind the ears, on the eyebrows, or in the others of the face and body.[52]National Eczema Association. (2025). Seborrheic Dermatitis. National Eczema Association. Available at: … Continue reading
- Suspected complications: If you notice signs of skin infection.
- Difficulty in diagnosis: If you are unsure if it is seborrheic dermatitis or another skin condition.
- Presence of other skin conditions: If you suspect you might have seborrheic dermatitis along with other skin conditions, this can complicate diagnosis and treatment.
Final Thoughts
Seborrheic dermatitis of the scalp is a complex condition influenced by factors such as sebum production, Malassezia overgrowth, genetics, and immune responses. While a range of treatments, from over-the-counter antifungal shampoos to prescription medications like roflumilast and ketoconazole, are available, their effectiveness varies depending on the individual and the severity of the condition. Finding the right approach often involves trial and error, with combination therapies frequently offering the best results. Ultimately, consistent management, lifestyle adjustments, and working closely with healthcare providers are key to keeping symptoms under control. If one treatment isn’t working, don’t get discouraged; there are plenty of options to explore.
References[+]
References ↑1 Ro, B.I., Dawson, T.L. (2005). The role of sebaceous gland activity and scalp microfloral metabolism in the etiology of seborrheic dermatitis and dandruff. The Journal of Investigative Dermatology. Symposium Proceedings. 10(3). 194-197. Available at: https://doi.org/10.1111/j.1087-0024.2005.10104.x. ↑2 Wikramanayake, T.C., Borda, L.J., Miteva, M., Paus, R. (2019). Seborrheic dermatitis-looking beyond Malassezia. Experimental Dermatology. 28(9). 991-1001. Available at: https://doi.org/10.1111/exd.14006 ↑3 Dawson Jr. (2007). Malassezia globosa and restricta: breakthrough understanding of the etiology and treatment of dandruff and seborrheic dermatitis through whole-genome analysis. Journal of Investigative Dermatology. Symposium Proceedings. 12(2). 15-19. Available at: https://doi.org/10.1038/sj.idsymp.5650049. ↑4 Karakadze, M.A., Hirt, P.A., Wikramanayake, T.C. (2018). The genetic basis of seborrheic dermatitis: a review. Journal of the European Academy of Dermatology and Venereology. 32(4). 529-536. Available at: https://doi.org/10.1111/jdv.14704 ↑5 Adalsteinsson, J.A., Kaushik, S., Muzumdar, S., Guttman-Yassky, E., Ungar, J. (2020). An update on the microbiology, immunology, and genetics of seborrheic dermatitis. Experimental Dermatology. 29(5). 481-489. Available at: https://doi.org/10.1111/exd.14091 ↑6 Bergbrant, I.M., Johansson, S., Robbins, D., Scheynius, A., Faergemann, J., Soderstrom, T. (1991). An immunological study in patients with seborrheic dermatitis. Clinical and Experimental Dermatology. 16(5). 331-338. Available at: https://doi.org/10.1111/j.1365-2230.1991.tb00395.x. ↑7 Kashiri, A., Maghsoudloo, N. (2024). Exploring the Impact of Vitamin D and Zinc Deficiencies on Sebhorreic Dermatitis: A Comparative Study. Health Science Reports. 7(12). E70283. Available at: https://doi.org/10.1002/hsr2.70283 ↑8 Schwartz, R.A., Janusz, C.A., Janniger, C.K. (2006). Seborrheic dermatitis: an overview. American Family Physician. 74(1). 125-130. Available at: PMID:16848386 ↑9 Saunte, D.M., Gaitanis, G., Hay, R.J. (2020). Malassezia-Associated Skin Diseases, the Use of Diagnostics and Treatment. Frontiers in Cellular and Infection Microbiology. 10. 112. Available at: https://doi.org/10.3389/fcimb.2020.00112 ↑10 DermNet. (no date). Seborrheic Dermatitis. Available at: https://dermnetnz.org/imagedetail/2050-seborrhoeic-dermatitis (Accessed: February 2025) ↑11 Zhang, F., Li, Y., Ren, W., Li, S. (2023). Establishment of clinical evaluation criteria for scalp seborrheic dermatitis. Journal of Cosmetic Dermatology. 22(11). 3042-3046. Available at: https://doi.org/10.1111/jocd.15804 ↑12 National Eczema Associations. (no date). Seborrheic Dermatitis. Available at: https://nationaleczema.org/eczema/types-of-eczema/seborrheic-dermatitis/ (Accessed: February 2025) ↑13 Franca, K., Villa, R.T., Silva, I.R., de Carvalho, C.A., Bedin, V. (2011). Hair Casts or Pseudonits. International Journal of Trichology. 3(2). 121-122. Available at: https://doi.org/10.4103/0974-7753.90834 ↑14 Kaliyadan, F., Ashique, K.T. (2019). Hair Casts and Nits – Differentiating Using Dermoscopy. Images in Clinical Practice. 85(4). 434-435. Available at: https://doi.org/10.4103/ijdvl.IJDVL_815_17 ↑15 Kim, G.W., Jung, H.J., Ko, H-C., Kim, M.B., Lee, W-J., Lee, S-J., Kim, D-W., Kim, B-S. (2011). Dermoscopy can be useful in differentiating scalp psoriasis from seborrheic dermatitis. British Journal of Dermatology. 164(3). 652-656. Available at: https://doi.org/10.1111/j.1365-2133.2010.10180.x ↑16 Kim, G.W., Jung, H.J., Ko, H-C., Kim, M.B., Lee, W-J., Lee, S-J., Kim, D-W., Kim, B-S. (2011). Dermoscopy can be useful in differentiating scalp psoriasis from seborrheic dermatitis. British Journal of Dermatology. 164(3). 652-656. Available at: https://doi.org/10.1111/j.1365-2133.2010.10180.x ↑17 Park, J-H., Park, Y.J., Kim, S.K., Kwon, J.E., Kang, Y.H., Lee, E-S., Choi, J.H., Kim, Y.C. (2016). Histopathological Differential Diagnosis of Psoriasis and Seborrheic Dermatitis of the Scalp. Annals of Dermatology. 28(4). 427-432. Available at: https://dx.doi.org/10.5021/ad.2016.28.4.427 ↑18 Alberts, B., Johnson, A., Lewis J. Molecular Biology of the Cell. 4th edition. New York: Garland Science; 2002. Epidermis and Its Renewal by Stem Cells. Available from: https://www.ncbi.nlm.nih.gov/books/NBK26865/ (Accessed: February 2025) ↑19 Park, J-H., Park, Y.J., Kim, S.K., Kwon, J.E., Kang, Y.H., Lee, E-S., Choi, J.H., Kim, Y.C. (2016). Histopathological Differential Diagnosis of Psoriasis and Seborrheic Dermatitis of the Scalp. Annals of Dermatology. 28(4). 427-432. Available at: https://dx.doi.org/10.5021/ad.2016.28.4.427 ↑20 Polaskey, M.T., Chang, C.H., Daftary, K., Fakhraie, S., Miller, C.H., Chovatiya, R. (2024). The Global Prevalence of Seborrheic Dermatitis: A Systematic Review and Meta-Analysis. JAMA Dermatology. 160(8). 846-855. Available at: https://doi.org/10.1001/jamadermatol.2024.1987 ↑21 Polaskey, M.T., Chang, C.H., Daftary, K., Fakhraie, S., Miller, C.H., Chovatiya, R. (2024). The Global Prevalence of Seborrheic Dermatitis: A Systematic Review and Meta-Analysis. JAMA Dermatology. 160(8). 846-855. Available at: https://doi.org/10.1001/jamadermatol.2024.1987 ↑22 Jang, W.S., Son, I.P., Yeo, K.I., Park, K.Y., Li, K., Kim, B.J., Seo, S.J., Kim, M.N., Hong, C.K. (2013). The Annual Changes of Clinical Manifestation of Androgenetic Alopecia Clinic in Korean Males and Females: A Outpatient-Based Study. Annals of Dermatology. 25(2). 181-188. Available at: https://doi.org/10.5021/ad.2013.25.2.181 ↑23 Faghihkhorasani, A., Sadeghzadeh, A., Goodarzi, A., Rohaninasab, M. (2024). The Relationship between Seborrheic Dermatitis and Androgenetic Alopecia in Patients Referred to a Skin Clinic in Tehran, Iran: A Retrospective Study. Journal of Health Reports and Technology. 10(1). E144076. Available at: https://doi.org/10.5812/jhrt-144076 ↑24 Kim, B.J., Kim, J.Y., Eun, H.C., Kwon, O.S., Kim, M.N. (2006). Androgenetic alopecia in adolescents: A report of 43 cases. The Journal of Dermatology. 33(10). 696-699. Available at: https://doi.org/10.1111/j.1346-8138.20106.00161.x ↑25 Kure, K., Isago, T., Hirayama, T. (2015). Changes in the sebaceous gland in patients with male pattern hair loss (androgenic alopecia). Journal of Cosmetic Dermatology. 14(3). 178-184. Available at: https://doi.org/10.1111/jocd.12153. ↑26 Suzuki, K., Inoue, M., Cho, O., Mizutani, R., Shimizu, Y., Nagahama, T., Sugita, T. (2021). Scalp microbiome and sebum composition in Japanese male individuals with and without androgenetic alopecia. Microorganisms. 9(10). 2132. Available at: https://doi.org/10.3390/microorganisms9102132 ↑27 Mangion, S.E., Mackenzie, L., Roberts, M.S., Holmes, A.M. (2023). Seborrheic dermatitis: topical therapeutics and formulation design. European Journal of Pharmaceutics and Biopharmaceutics. 185. 148-164. Available at: https://doi.org/10.1016/j.ejpb.2023.01.023 ↑28 Arcutis Biotherapeutics. (no date). FDA Approves Arcutis’ ZORYVE (roflumilast) Topical Foam, 0.3% for the Treatment of Seborrheic Dermatitis in Individuals Aged 9 Years and Older. Available at: https://www.arcutis.com/fda-approves-arcutis-zoryve-roflumilast-topical-foam-0-3-for-the-treatment-of-seborrheic-dermatitis-in-individuals-aged-9-years-and-older/ (Accessed: February 2025) ↑29 Zirwas, M.J., Draelos, Z.D., DuBois, J., Kircik, L.H., Moore, A.Y., Gold, L.S., Alonso-Llamazares, J., Bukhalo, M., Bruce, S., Eads, K., Green, L.J., Guenthner, S., Ferris, L.K., Forman, S.B., Kempers, S.E., Lain, E., Lynde, C.W., Pariser, D.M., Toth, D.P., Yamauchi, P.S., Higham, R.C., Krupa, D., Burnett, P., Berk, D.R. (2023). Efficacy of Roflumilast Foam, 0.3%, in Patients with Seborrheic Dermatitis. JAMA Dermatology. 159(6). 613-620. Available at: https://doi.org/10.1001/jamadermatol.2023.0846 ↑30 Tynes, B.E., Johnson, C.D., Vaish, M.H., Abbott, B., Vucenovic, J., Varrassi, G., Potharaju, P., Torres, Y.L., Lee, Z., Ahmadzadeh, S., Shekoohi, S., Kaye, A.D. (2024). Ketoconazole Shampoo for Seborrheic Dermatitis of the Scalpe: A Narrative Review. Cureus. 16(8). E67532. Available at: https://doi.org/10.7759/cureus.67532 ↑31 Borgers, M., Degreed, H. (2007). The Role of Ketoconazole in Seborrheic Dermatitis. Therapeutics for the Clinician. 80. 359-363. Available at: https://cdn.mdedge.com/files/s3fs-public/Document/September-2017/080040359.pdf (Accessed: February 2025) ↑32 Goularte-Silva, V., Paulino, C.L. (2021). Ketoconazole beyond antifungal activity: Bioinformatics-based hypothesis on lipid metabolism in dandruff and seborrheic dermatitis. Experimental Dermatology. 31(5). 821-822. Available at: https://doi.org/10.1111/exd.14505 ↑33 Goularte-Silva, V., Paulino, C.L. (2021). Ketoconazole beyond antifungal activity: Bioinformatics-based hypothesis on lipid metabolism in dandruff and seborrheic dermatitis. Experimental Dermatology. 31(5). 821-822. Available at: https://doi.org/10.1111/exd.14505 ↑34 LOPROX® (cicloporox) Shampoo 1%. (2006). MEDICIS Pharmaceutical Corp. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2006/021159s009lbl.pdf (Accessed: February 2025) ↑35 Godse, G., Godse, K. (2024). Safety, Efficacy and Attributes of 2.5% Selenium Sulfide Shampoo in the Treatment of Dandruff: A Single-Center Study. Cureus. 16(3). E57148. Available at: https://doi.org/10.7759/cureus.57148 ↑36 Davies, D.B., Boorman, G.C., Shuttleworth, D. (1999). Comparative efficacy of shampoos containing coal tar (4.0% w/w; Tarmed), coal tar (4.0% w/w) plus ciclopirox olamine (1.0% w/w Tarmed AF), and ketoconazole (2.0% w/w Nizoral) for the treatment of dandruff/seborrheic dermatitis. Journal of Dermatological Treatment. 10(3). 177-183. Available at: https://doi.org/10.3109/09546639909056025 ↑37, ↑39, ↑49 Ge, L., Liu, Z., Xu, S., Li, C., Jin, M., Luo, Y., Kong, Y., Meng, J., Zheng, G., Gao, J., Wang, P., Bai, W., Na, H., Zhou, X., Jin, Z., Pi, L. (2025). A Cohort Clinical Study on the Efficacy of Topical Salicylic Acid/Piroctone Olamine Dandruff Pre-Gel and Cleanser in Improving Symptoms of Moderate to Severe Seborrheic Dermatitis of the Scalp. Journal of Cosmetic Dermatology. 24(1). E16742. Available at: https://doi.org/10.1111/jocd.16742 ↑38 Marks, R., Pearse, A.D., Walker, A.P. (1985). The effects of a shampoo containing zinc pyrithione on the control of dandruff. British Journal of Dermatology. 112(4). 415-422. Available at: https://doi.org/10.1111/j.1365-2133.1985.tb02314.x. ↑40 Paula Ludmann. (2024). Seborrheic Dermatitis: Diagnosis and Treatment. American Academy of Dermatology Association. Available at: https://www.aad.org/public/diseases/a-z/seborrheic-dermatitis-treatment (Accessed: February 2025) ↑41 Dall’Oglio, F., Nasca, M.R., Gerbino, C., Micali, G. (2022). An Overview of the Diagnosis and Management of Seborrheic Dermatitis. Clinical, Cosmetic and Investigational Dermatology. 6(15). 1537-1548. Available from: https://doi.org/10.2147/CCID.S284671 ↑42 Alshaebi, M., Zahed, L., Osalyan, M., Sulaimani, S., Albahlool, A., Abduljabbar, M.H., Hariri, J. (2023). Association Between Diet and Seborrheic Dermatitis: A Case-Control Study. Cureus. 15(11). E48782. Available at: https://doi.org/10.7759/cureus.48782 ↑43 Woolhiser, E., Keime, N., Patel, A., Weber, I., Adelman, M., Dellavalle, R.P. (2024). Nutrition, Obesity, and Seborrheic Dermatitis: Systematic Review. JMIR Dermatology. E50143. Available at: https://doi.org/10.2196/50143 ↑44 Paula Ludmann. (2024). Seborrheic Dermatitis: Diagnosis and Treatment. American Academy of Dermatology Association. Available at: https://www.aad.org/public/diseases/a-z/seborrheic-dermatitis-treatment (Accessed: February 2025) ↑45 Zhang, F., Li, Y-H., Ren, W., Li, S-R., Chen, Y-C. (2023). Clinical efficacy of a combination treatment of traditional Chinese medicine for scalp seborrheic dermatitis. Journal of Cosmetic Dermatology. 22(11). 3072-3077. Available at: https://doi.org/10.1111/jocd.15818 ↑46 Goldenberg, G. (2013). Optimizing Treatment Approaches in Seborrheic Dermatitis. Journal of Clinical and Aesthetic Dermatology. 6(2). 44-49. Available at: PMID: 23441240 ↑47 Jaalouk, D., Pulumati, A., Algarin, Y.A., Kircik, L., Issa, N.T. (2024). Dermatologic Procedures for the Treatment of Seborrheic Dermatitis. Journal of Drugs in Dermatology. 23(10). 819-824. Available at: https://doi.org/10.36849/JDD.2024.8116 ↑48 Ortonne, J-P., Nikkels, A.F., Reich, K., Oliver, R.M.P., Lee., J.H., Kerrouche, N., Sidou, F., Faergemann, J. (2011). Efficacious and safe management of moderate to severe scalp seborrheic dermatitis using clobetasol propionate shampoo 0.05% combined with ketoconazole shampoo 2%: a randomized controlled study. British Journal of Dermatology. 165(1). 171-176. Available at: https://doi.org/10.1111/j.1365-2133.2011.10269.x. ↑50 University of Utah Health. (no date). Seborrheic Dermatitis. Available at: https://healthcare.utah.edu/dermatology/conditions/seborrheic-dermatitis (Accessed: February 2025) ↑51 Cleveland Clinic. (2020). Seborrheic Dermatitis. Cleveland Clinic. Available at: https://my.clevelandclinic.org/health/diseases/14403-seborrheic-dermatitis (Accessed: February 2025) ↑52 National Eczema Association. (2025). Seborrheic Dermatitis. National Eczema Association. Available at: https://nationaleczema.org/eczema/types-of-eczema/seborrheic-dermatitis/#h-management-and-treatment (Accessed: February 2025) While the medical literature clearly advises women to avoid finasteride before conception during pregnancy, and while breastfeeding, the guidance for men is less definitive. The question of whether men can safely continue using finasteride during the conception period remains a topic of debate among healthcare professionals.
However, a recent large dataset statistical analysis has sent ripples through the hair loss space and regulatory world, as it appears to show further evidence that the use of finasteride in men leads to a congenital anomaly called “cryptorchidism” (undescended testicles). But what does the data actually say? And can we link statistical association to causality? In this article, we will take a deep dive into what the paper shows (or doesn’t show) and whether we think it is a cause of major concern for men.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.

Let’s first take a look at what the study is all about.
The Study
We’ll begin by summarizing the data from the study and then go into detail about what it all means, how the statistics are analyzed, and whether this is a result to be concerned about.
The researchers analyzed data from the FDA Adverse Event Reporting System (FAERS) from 2010 to 2022 to assess potential safety concerns related to paternal drug exposure on fertility, pregnancy outcomes, and offspring health.[1]Zeng, Y., Lin, W., Zhuang, W. (2024). Safety concerns of paternal drug exposure on fertility, pregnancy, and offspring: an analysis based on the FDA adverse event reporting system. Andrology. 1-12. … Continue reading The FAERS is a computerized database that supports the FDA’s post-marketing safety surveillance program for approved drugs and therapeutic biologic products.[2]US Food and Drug Administration. (no date). FDA Adverse Events Reporting System (FAERS) Public Dashboard. US FDA. Available at: … Continue reading It collects and stores information on adverse events, medication errors, and product quality complaints that may be associated with FDA-approved products.
Reporting to FAERS can be done in two ways:
- Mandatory reporting: Manufacturers are required by law to report adverse events to FAERS within 14 days of becoming aware of them.
- Voluntary reporting: Healthcare professionals (such as physicians, pharmacists, and nurses) and consumers (including patients, family members, and lawyers) can voluntarily submit reports.
Importantly, anyone can submit to FAERS directly; it does not need to be done by a doctor. The FDA provides multiple options for voluntary reporting:
- Online submission through the FDA’s Electronic Submission Gateway (ESG) or Safety Reporting Portal (SRP).
- Using FDA Form 3500, which can be submitted electronically or by mail.[3]US Food and Drug Administration (2024). Reporting Serious Problems to FDA. MedWatch. Available at: … Continue reading
What Were The Study Results?
The researchers conducted a disproportionality analysis, specifically the Reporting Odds Ratio (ROR), to identify drugs disproportionately associated with reproductive-related adverse events.
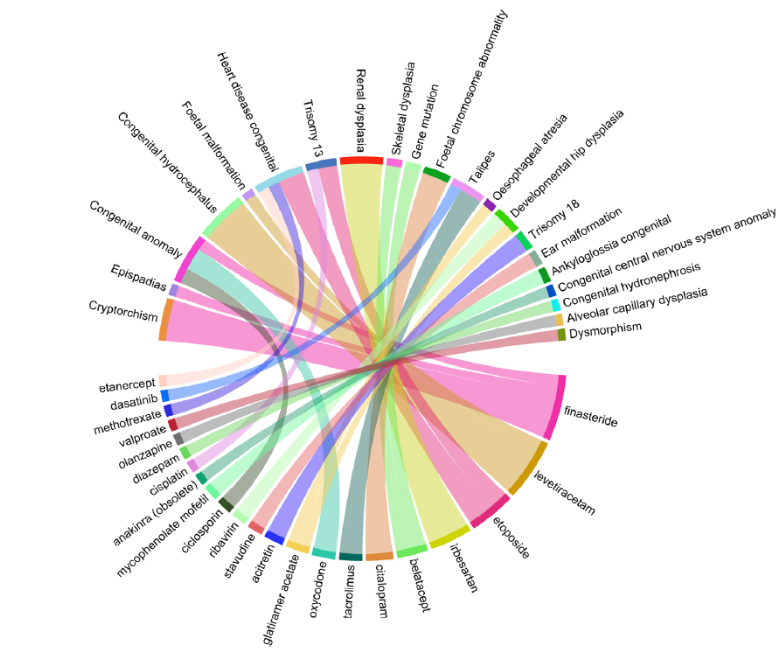
The study analyzed 16,180,533 total reports; 3,210 cases related to paternal drug exposure were identified, with 7,808 associated adverse events (e.g., spontaneous abortions and small babies). The study found that drugs used to treat rheumatoid arthritis, cancer, infections, and psychotropic conditions were the most frequently implicated.
However, one of the strongest links between treatment and adverse health events was between finasteride and cryptorchidism, with an ROR of 891.7 based on 11 reports. This suggests that cryptorchidism was reported for finasteride-exposed fathers at a much higher rate than for most other drugs in the database.

Figure 1: A graph showing the ROR of different drugs and their adverse event pairs. Finasteride and cryptorchidism appear to have a noticeably larger ROR than others.[4]Zeng, Y., Lin, W., Zhuang, W. (2024). Safety concerns of paternal drug exposure on fertility, pregnancy, and offspring: an analysis based on the FDA adverse event reporting system. Andrology. 1-12. … Continue reading
Understanding the Data
Before we go into what the data means, let’s explain some key concepts that are important to the study.
What is a Disproportionality Analysis?
A disproportionality analysis is a tool used in drug safety monitoring. It analyzes large databases of reported side effects from various medications and looks for unusual patterns – like if a particular side effect is reported much more often with one drug than others.[5]Fusaroli, M., Salvo, F., Begaud, B., AlShammari, T.M, Bate, A., Battini, V., Brueckner, A., Candore, G., Carnovale, C., Crisafulli, S., Cutroneo, P.M., Dolladille, C., Drici, M.D., Faillie, J.L., … Continue reading
Imagine a concert where five people in the front row get food poisoning after eating hotdogs from a nearby stall, while only one person in the entire back section reports feeling ill. You might suspect that the front-row hot dogs are bad—but this doesn’t prove the food stand actually caused the sickness. Maybe those five people already had food poisoning before coming. Disproportionality analysis works in a similar way: it flags patterns, i.e., five people sick in the front row, but it doesn’t prove causation.
What is the Reporting Odds Ratio (ROR)?
The ROR is a key statistical measure used in disproportionality analyses. It compares how often a specific side effect is reported for a particular drug versus all other drugs.[6]Rothman, K.J., Lanes, S., Sacks, S.T. (2004). The reporting odds ratio and its advantages over the proportional reporting ratio. Pharmacoepidemiology and Drug Safety. 13(8). 519-523. Available at: … Continue reading If the ROR is high, it means the side effects are being reported more often for that drug than you’d normally expect.
Think about flipping a coin 10 times, and imagine it lands on “heads” 7 times. You might think the coin is biased. But if you had flipped it 1,000 times, the results might have evened out to 50/50. The Reporting Odds Ratio (ROR) works similarly: when there are only a few cases, even small variations make the number seem exaggerated. A few extra reports in a small dataset can make an effect look much larger than it actually is.
Unlike incidence, which measures new cases over time, or prevalence, which measures total cases at a given time, ROR does not provide information about the actual risk of an adverse event occurring. Instead, it indicates whether there’s a disproportionate association between a drug and an adverse event in the reporting database.
The important point to remember is that ROR is primarily a hypothesis-generating tool, helping prioritize which drug-event combinations may need further investigation.
What Do The Study Results Mean?
The ROR calculation was based on reports from the FAERS, which, as we mentioned above, is a system for self-reporting adverse events that anyone can report to. This means that more severe or unusual side effects are more likely to be reported, and as such, FAERS is at risk of reporting bias. This was acknowledged as a limitation in the study.
Furthermore, unlike controlled clinical studies, FAERS does not track how many people take a drug; it only tracks how many people report an issue.
To calculate the true risk of cryptorchidism from finasteride, you need two numbers:
- The number of reported cases (numerator) – FAERS provides this (11 cases).
- The total number of fathers who took finasteride (denominator) – FAERS does not provide this.
Since FAERS does not track drug exposure rates, it is impossible to calculate the incidence or prevalence of an event. This means we can’t determine what percentage of fathers taking finasteride had children with cryptorchidism or whether this percentage is actually higher than background rates in the general population.
Think about it this way: a phone company gets 100 customer complaints in a month. Without knowing how many total customers they have, you can’t tell if that’s a serious problem. If they have 200 customers, that’s bad (50% complaint rate). However, if they have 2 million customers, it’s insignificant (0.005% complaint rate). FAERS has the same issue—it counts events but doesn’t count the total number of people taking the drug.
Furthermore, the disproportionality analysis does not compare finasteride to a control group. Instead, it compares the number of cryptorchidism reports for finasteride (11) to the number of cryptorchidism reports for all other drugs (likely much lower because most drugs do not affect male hormone pathways).
This is problematic for several reasons:
1. This is Not a Matched Control Population
-
- Fathers who took finasteride should be compared to fathers who did not take finasteride while keeping other factors (like age, lifestyle, genetics) constant.
- FAERS instead compares finasteride to all other drugs – but as we just mentioned, most drugs don’t affect male reproductive hormones, making the comparison flawed.
2. Selective Reporting Bias in FAERS
-
- Finasteride users are already aware of post-finasteride syndrome (PFS) and reproductive side effect concerns.
- If a father taking finasteride has a child with any birth defect, they may be more likely to report it than a father taking, say, an antibiotic or a painkiller.
- This could artificially inflate the number of finasteride-related reports, making cryptorchidism appear more common than it is.
3. The Numerator is Small, But the ROR is Huge:
-
- FAERS recorded only 11 cryptorchidism cases for finasteride from 2010 – 2022.
- Cryptorchidism naturally occurs in 2-3% of all full-term male births.[7]Leslie, S.W., Sajjad, H., Villanueva, C.A. (2024). In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470270/ … Continue reading
This creates a statistical illusion. If very few cryptorchidism cases are reported for other drugs, the ROR for finasteride skyrockets, even if the actual risk is low.
People fear shark attacks because they’re widely reported in the news, but statistical analyses have shown that the odds of dying from a falling vending machine are higher than being killed by a shark.[8]United States Consumer Product Safety Commission. (1995). CPSC, Soda Vending Machine Industry Labeling Campaign Warns of Deaths and Injuries. US CPSC. Available at: … Continue reading The reason we think sharks are deadlier is that their attacks make headlines while vending machine accidents don’t. Similarly, if only one case of cryptorchidism is reported for another drug, but 11 cases are reported for finasteride, the ROR can look massive—even if the actual risk is tiny.
In 2022, about 2,626,865 men in the United States were estimated to have taken finasteride.[9]ClinCalc. (no date). Finasteride Drug Usage Statistics, United States, 2013-2022. ClinCalc. Available at: https://clincalc.com/drugstats/Drugs/Finasteride (Accessed: January 2025) Even if all 11 reports of cryptorchidism were from distinct individuals and occurred solely in 2022 (instead of over 12 years), this would equate to an incidence rate of 0.00042% (or 4.2 per million users). This is notably below the background risk of cryptorchidism in the general population (2-3%), suggesting that the observed reports in FAERS are likely to be an artifact of a small sample size rather than evidence of a causal relationship.
So, to summarize, this study, while showing a statistical association between men taking finasteride and their children having cryptorchidism, does not show any causal relationship – meaning that it doesn’t actually show that finasteride causes this congenital anomaly.
Why Is This Study Even A Discussion?
Finasteride’s potential impact on reproductive health has been debated for years, largely due to animal studies and regulatory warnings for women. While the FAERS data discussed above suggest a statistical association between finasteride use in men and cryptorchidism in offspring, the underlying question is whether this link is biologically plausible or supported by stronger evidence.
Finasteride is classified as an FDA Pregnancy Category X drug, meaning that it is strictly contraindicated in pregnant women due to teratogenic effects observed in animal studies.[10]Merck & Co. Inc. (no date). Propecia Prescribing Information. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020788s020s021s023lbl.pdf (Accessed: January 2025) These concerns stem from its mechanism of action: blocking the conversion of testosterone into dihydrotestosterone (DHT) by inhibiting the 5ɑ-reductase enzyme. Since DHT is crucial for normal male fetal development, any disruption during pregnancy can result in genital abnormalities.[11]Bormann, C.L., Smith, G.D., Padmanabhan, V., Lee, T.M. (2011). Prenatal testosterone and dihydrotestosterone exposure disrupts ovine testicular development. Reproduction 142(1). Available at: … Continue reading
Studies in rodent and primate models have shown that exposure to high doses of finasteride during pregnancy can lead to:
- Hypospadias – a condition where the urethral opening is misplaced on the underside of the penis instead of at the tip.[12]An, N., Peng, J., He, G., Fan, X., Li, F., Chen, H. (2018). Involvement of activation of mitogen-activated protein kinase (MAPK)/extracellular signal-related kinase (ERK) signaling pathway in … Continue reading
- Cryptorchidism – as mentioned above, is an anomaly in which one or both testicles fail to descend into the scrotum during fetal development, a condition later associated with fertility issues and an increased risk of testicular cancer.
- Reduced anogenital distance (AGD) – a key marker of disrupted androgen signaling during development and is often used as a biomarker for endocrine disruption.[13]Clark, R.L., Anderson, C.A., Prahalada, S., Robertson, R.T., Lochry, E.A., Leonard, Y.M., Stevens, J.L., Hoberman, A.M. (1993). Critical developmental periods for effects on male rat genitalia … Continue reading
One study in rhesus monkeys found that continuous finasteride exposure throughout gestation resulted in severe genital malformations in male offspring.[14]Prahalada, S., Tarantal, A.F., Harris, G.H., Ellsworth, K.P., Clarke, A.P., Skiles, G.L., MacKenzie, K.I., Kruk, L.F., Ablin, D.S., Cukierski, M.A., Peter, C.P., vanZwieten, M.J., Hendrickx, A.G. … Continue reading This was particularly concerning because monkeys have hormonal systems that more closely resemble humans compared to rodents. Due to these findings, the FDA issued strong warnings that pregnant women should never ingest or even handle crushed finasteride tablets, as skin absorption could theoretically lead to fatal exposure.
For more information, see our article diving into the science behind finasteride & conception, and our article about how to use finasteride and minimize its exposure to your partner.
Can These Findings in Animals Be Directly Applied to Humans?
Although these studies raise legitimate concerns, there are important reasons why their findings may not directly apply to human males taking finasteride. For example, the doses used in animal studies are often much higher than those used in human treatment. The studies also involve direct maternal exposure during pregnancy, whereas paternal exposure (via sperm) results in much lower fetal exposure (we’ll discuss this further below). Furthermore, while rodents and monkeys have similar endocrine systems, their sensitivity to 5ɑ-reductase inhibition differs from that of humans.
Therefore, while animal models provide a biological basis for concern, they do not conclusively prove that paternal finasteride exposure affects offspring in humans.
Is It Biologically Plausible That Finasteride Could Cause Issues in Men?
To determine whether paternal finasteride use could biologically contribute to congenital anomalies in humans, we need to look at:
- How much finasteride reaches semen and whether these lead to enough exposure in females to impact fetal development.
- Whether finasteride alters sperm in a way that could lead to birth defects.
How Much Finasteride Reaches Semen?
One way finasteride could hypothetically impact fetal development is through semen exposure during conception or early pregnancy. However, semen levels of finasteride are extremely low.
Clinical data from GlaxoSmithKline (internal studies) measured finasteride concentrations in the semen of men taking a 50 mg dose (which is 10 x higher than the standard dose for hair loss). The result? Only 0.26 ng/mL of finasteride was detected in semen.[15]US Food and Drug Administration. (no date). Propecia (finasteride). US FDA. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/020788s017lbl.pdf (Accessed: January 2025) At the standard 1 mg dose used for hair loss, semen concentrations would likely be even lower.
How does this compare to doses known to cause fetal harm?
In the rhesus monkey studies, oral doses of finasteride given directly to pregnant females (at levels over 5,000 x higher than those found in human semen) caused genital abnormalities in male offspring. Therefore, the amount of finasteride that pregnant human women might absorb from semen exposure is likely so low that it falls below the threshold needed to affect fetal development.
Conclusion: There is no compelling evidence to suggest that the trace amounts of finasteride in semen are enough to cause congenital defects in humans.
Can Finasteride Affect Sperm Quality or DNA?
Another possible concern is whether finasteride negatively affects sperm itself, leading to:
- Reduced fertility.
- DNA damage that could increase congenital anomaly risk.
Some studies suggest finasteride can reduce sperm concentration and motility at higher doses (5 mg for prostate treatment), but these effects are reversible after stopping the medication, and studies in men taking the 1 mg dose for hair loss do not show significant sperm abnormalities.
For example, a 2013 study by Samplaski et al. found that men taking an average of 1.04 mg/day of finasteride experienced an 11.6-fold increase in sperm count after stopping the drug, with no participants experiencing a decrease in sperm count post-discontinuation.[16]Samplaski, M.K., Lo, K., Grober, E., Jarvi, K. (2013). Finasteride use in the male infertility population: effects on semen and hormone parameters. Fertility and Sterility. 100(6). 1542-1546. … Continue reading
Similarly, a 1999 study found that 1 mg/day of finasteride did not significantly affect spermatogenesis or semen production in healthy men.[17]Overstreet, J.W., Fuh, V.L., Gould, J., Howards, S.S., Lieber, M.M., Hellstrom, W., Shapiro, S., Carroll, P., Corfman, R.S., Petrous, S., Lewis, R., Toth, P., Shown, T., Roy, J., Jarow, J.P., … Continue reading
A 2007 study observed that taking 5 mg/day of finasteride exhibited mild reductions in semen volume, sperm concentration, and motility, though these parameters returned just below normal after stopping.[18]J.K., Amory., Wang, C., Swerdloff, R.S., Anawalt, B.D., Matsumoto, A.M., Bremner, W.J., Walker, S.E., Haberer, L.J., Clark, R.V. (2007). The effect of 5alpha-reductase inhibition with dutasteride and … Continue reading

Figure 2: Percent changes in sperm count, semen volume, sperm concentration, motility, and morphology at weeks 26 and 52 of treatment with finasteride or dutasteride and at the follow-up after stopping.[19]J.K., Amory., Wang, C., Swerdloff, R.S., Anawalt, B.D., Matsumoto, A.M., Bremner, W.J., Walker, S.E., Haberer, L.J., Clark, R.V. (2007). The effect of 5alpha-reductase inhibition with dutasteride and … Continue reading
Could Finasteride Cause Epigenetic Changes to Sperm?
Some scientists have speculated that finasteride could cause epigenetic modifications to sperm, meaning it might alter gene expression without changing the DNA sequence. However, no studies have directly confirmed this in humans. Animal studies suggest some potential for altered gene expression, but these findings haven’t been replicated in human sperm research.[20]Kolasa, A., Roginska, D., Rzeszotek, S., Machalinski, B., Wiszniewska, B. (2021). Paternal finasteride treatment can influence the testicular transcriptome profile of male offspring – … Continue reading
In 2011 and 2012, two separate case reports documented men struggling with fertility issues after long-term finasteride use. While their sperm morphology appeared normal, both had elevated sperm DNA fragmentation-a marker of DNA damage. After stopping finasteride, one saw fragmentation drop from 30% to 16.5% within six months, while the other improved and successfully conceived.[21]Salvarci, A., Istanbulluoglu, O. (2012). Secondary infertility due to use of low-dose finasteride. International urology and nephrology. 45(1). 83-85. Available at: … Continue reading,[22]Tu, H.Y.V., Zini, A. (2011). Finasteride-induced secondary infertility associated with sperm DNA damage. Fertility and sterility. 95(6). e13-4. Available at: … Continue reading
These reports suggest finasteride may contribute to sperm DNA damage, but since they lack controls, other lifestyle changes such as diet, exercise, or better sleep could also explain the improvements. You can read more about our thoughts on these case studies here.
The bottom line is that:
- Finasteride can mildly impact sperm quality, but this effect is reversible and not linked to congenital anomalies.
- No strong evidence exists that finasteride causes long-term DNA changes that could harm offspring.
So, is it biologically plausible that finasteride causes birth defects when taken by men? We think the current evidence for paternal risk is weak.
Is There Any Other Evidence That Finasteride Causes Congenital Anomalies?
To date, no large-scale, well-controlled studies have confirmed an increased risk of congenital anomalies from paternal finasteride use.
Danish Nationwide Study (2017)
Study Type: A large-scale epidemiological study using data from national birth registries.[23]Anderson, J.T., Jenson, T.B., Horwitz, H., Clausen, S.S. (2019). Paternal exposure to finasteride – Before and during pregnancy. Pharmacoepidemiology and Drug Safety. 28(16). Conference … Continue reading
Findings: No increased risk of congenital anomalies in children of men who had taken finasteride before conception. The risk of miscarriage was also not elevated.
Conclusion: No strong evidence linking paternal finasteride use to birth defects.
Case Reports and Small Studies
Some isolated case reports have suggested a potential association between paternal finasteride use and reproductive issues in offspring.[24]Ahn, K.H., Shin, J., Hong, S.C., Han, JY., Lee, E.H., Lee, J.S., Oh, M.J., Kim, H.J. (2015). Pregnancy Outcomes with Paternal Exposure to Finasteride, a Synthetic 5-Alpha-Reductase Inhibitor: A Case … Continue reading However, these reports often lack proper controls and fail to rule out other factors such as genetics, environmental exposures, or maternal health conditions.
Final Thoughts
While the study we have discussed in this article highlights a statistical association between paternal finasteride exposure and cryptorchidism, it does not establish causation. The limitations of FAERS data, including reporting bias and the absence of a control population, make it difficult to draw firm conclusions. Additionally, biological plausibility remains weak, given the extremely low levels of finasteride in semen and the lack of strong evidence linking paternal exposure to congenital anomalies. Ultimately, while more research is warranted, current data does not suggest a major cause for concern. Men using finasteride should, however, discuss any reproductive concerns with their healthcare provider before making any decisions.
References[+]
References ↑1 Zeng, Y., Lin, W., Zhuang, W. (2024). Safety concerns of paternal drug exposure on fertility, pregnancy, and offspring: an analysis based on the FDA adverse event reporting system. Andrology. 1-12. Advance online publication. Available at: https://doi.org/10.1111/andr.13790 ↑2 US Food and Drug Administration. (no date). FDA Adverse Events Reporting System (FAERS) Public Dashboard. US FDA. Available at: https://fis.fda.gov/extensions/FPD-FAQ/FPD-FAQ.html#:~:text=Healthcare%20professionals%2C%20consumers%2C%20and%20manufacturers,members%2C%20lawyers%20and%20others). (Accessed: January 2025) ↑3 US Food and Drug Administration (2024). Reporting Serious Problems to FDA. MedWatch. Available at: https://www.fda.gov/safety/medwatch-fda-safety-information-and-adverse-event-reporting-program/reporting-serious-problems-fda (Accessed: January 2025) ↑4 Zeng, Y., Lin, W., Zhuang, W. (2024). Safety concerns of paternal drug exposure on fertility, pregnancy, and offspring: an analysis based on the FDA adverse event reporting system. Andrology. 1-12. Advance online publication. Available at: https://doi.org/10.1111/andr.13790 ↑5 Fusaroli, M., Salvo, F., Begaud, B., AlShammari, T.M, Bate, A., Battini, V., Brueckner, A., Candore, G., Carnovale, C., Crisafulli, S., Cutroneo, P.M., Dolladille, C., Drici, M.D., Faillie, J.L., Goldman, A., Hauben, M., Herdeiro, M.T., Mahaux, O., Manlik, K., Montastruc, F., Noguchi, Y., Noren, G.N., Noseda, R., Onakpoya, I.J., Pariente, A., Poluzzi, E., Salem, M., Sartori, D., Trinh, N.T.H., Tuccori, M., van Hunsel, F., van Puijenbroek., E, Raschi, E., Jhouri, C. (2024). The Reporting of Disproportionality Analysis for Drug Safety Signal Detection Using Individual Case Safety Reports in PharmacoVigilance (READUS-PV): Development and Statement. Drug Safety. 47(6). 575-584. Available at: https://doi.org/10.1007/s40264-024-01421-9 ↑6 Rothman, K.J., Lanes, S., Sacks, S.T. (2004). The reporting odds ratio and its advantages over the proportional reporting ratio. Pharmacoepidemiology and Drug Safety. 13(8). 519-523. Available at: https://doi.org/10.1002/pds.1001 ↑7 Leslie, S.W., Sajjad, H., Villanueva, C.A. (2024). In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470270/ (Accessed: January 2025) ↑8 United States Consumer Product Safety Commission. (1995). CPSC, Soda Vending Machine Industry Labeling Campaign Warns of Deaths and Injuries. US CPSC. Available at: https://www.cpsc.gov/Newsroom/News-Releases/1996/CPSC-Soda-Vending-Machine-Industry-Labeling-Campaign-Warns-Of-Deaths-And-Injuries (Accessed: January 2025) ↑9 ClinCalc. (no date). Finasteride Drug Usage Statistics, United States, 2013-2022. ClinCalc. Available at: https://clincalc.com/drugstats/Drugs/Finasteride (Accessed: January 2025) ↑10 Merck & Co. Inc. (no date). Propecia Prescribing Information. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020788s020s021s023lbl.pdf (Accessed: January 2025) ↑11 Bormann, C.L., Smith, G.D., Padmanabhan, V., Lee, T.M. (2011). Prenatal testosterone and dihydrotestosterone exposure disrupts ovine testicular development. Reproduction 142(1). Available at: https://doi.org/10.1530/REP-10-0210 ↑12 An, N., Peng, J., He, G., Fan, X., Li, F., Chen, H. (2018). Involvement of activation of mitogen-activated protein kinase (MAPK)/extracellular signal-related kinase (ERK) signaling pathway in proliferation of urethral plate fibroblasts in finasteride-induced rat hypospadias. Medical Science Monitor. 24. 8984-8992. Available at: https://doi.org/10.12659/MSM.911271 ↑13 Clark, R.L., Anderson, C.A., Prahalada, S., Robertson, R.T., Lochry, E.A., Leonard, Y.M., Stevens, J.L., Hoberman, A.M. (1993). Critical developmental periods for effects on male rat genitalia induced by finasteride, a 5 alpha-reductase inhibitor. Toxicology and Applied Pharmacology. 119(1). 34-40. Available at: https://doi.org/10.1006/taap.1993.1041 ↑14 Prahalada, S., Tarantal, A.F., Harris, G.H., Ellsworth, K.P., Clarke, A.P., Skiles, G.L., MacKenzie, K.I., Kruk, L.F., Ablin, D.S., Cukierski, M.A., Peter, C.P., vanZwieten, M.J., Hendrickx, A.G. (1997). Effects of finasteride, a type 2 5-alpha reductase inhibitor, on fetal development in the rhesus monkey (Macaca mulatta) 55(2). 119-131. Available at: 10.1002/(SICI)1096-9926(199702)55:2<119::AID-TERA1>3.0.CO;2-Z. ↑15 US Food and Drug Administration. (no date). Propecia (finasteride). US FDA. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/020788s017lbl.pdf (Accessed: January 2025) ↑16 Samplaski, M.K., Lo, K., Grober, E., Jarvi, K. (2013). Finasteride use in the male infertility population: effects on semen and hormone parameters. Fertility and Sterility. 100(6). 1542-1546. Available at: https://doi.org/10.1016/j.fertnstert.2013.07.2000 ↑17 Overstreet, J.W., Fuh, V.L., Gould, J., Howards, S.S., Lieber, M.M., Hellstrom, W., Shapiro, S., Carroll, P., Corfman, R.S., Petrous, S., Lewis, R., Toth, P., Shown, T., Roy, J., Jarow, J.P., Bonilla, J., Jacobsen, C.A., Wang, D.Z. Kaufman, K.D. (1999). Chronic treatment with finasteride daily does not affect spermatogenesis or semen production in young men. Journal of Urology. 162(4). 11295-300. Available at: PMID: 10492183 ↑18 J.K., Amory., Wang, C., Swerdloff, R.S., Anawalt, B.D., Matsumoto, A.M., Bremner, W.J., Walker, S.E., Haberer, L.J., Clark, R.V. (2007). The effect of 5alpha-reductase inhibition with dutasteride and finasteride on semen parameters and serum hormones in healthy men. The Journal of Clinical Endocrinology & Metabolism. 92(5). 1659-1665. Available at: https://doi.org/10.1210/jc.2006-2203 ↑19 J.K., Amory., Wang, C., Swerdloff, R.S., Anawalt, B.D., Matsumoto, A.M., Bremner, W.J., Walker, S.E., Haberer, L.J., Clark, R.V. (2007). The effect of 5alpha-reductase inhibition with dutasteride and finasteride on semen parameters and serum hormones in healthy men. The Journal of Clinical Endocrinology & Metabolism. 92(5). 1659-1665. Available at: https://doi.org/10.1210/jc.2006-2203 ↑20 Kolasa, A., Roginska, D., Rzeszotek, S., Machalinski, B., Wiszniewska, B. (2021). Paternal finasteride treatment can influence the testicular transcriptome profile of male offspring – preliminary study. Current issues in molecular biology. 43(2). 868-886. Available at: https://doi.org/10.3390/cimb43020062 ↑21 Salvarci, A., Istanbulluoglu, O. (2012). Secondary infertility due to use of low-dose finasteride. International urology and nephrology. 45(1). 83-85. Available at: https://doi.org/10.1007/s11255-012-0315-9 ↑22 Tu, H.Y.V., Zini, A. (2011). Finasteride-induced secondary infertility associated with sperm DNA damage. Fertility and sterility. 95(6). e13-4. Available at: https://doi.org/10.1016/j.fertnstert.2010.12.061 ↑23 Anderson, J.T., Jenson, T.B., Horwitz, H., Clausen, S.S. (2019). Paternal exposure to finasteride – Before and during pregnancy. Pharmacoepidemiology and Drug Safety. 28(16). Conference Abstract. Available at: https://doi.org/10.1002/pds.4864 ↑24 Ahn, K.H., Shin, J., Hong, S.C., Han, JY., Lee, E.H., Lee, J.S., Oh, M.J., Kim, H.J. (2015). Pregnancy Outcomes with Paternal Exposure to Finasteride, a Synthetic 5-Alpha-Reductase Inhibitor: A Case Series. Journal of Clinical Toxicology. 5(2). Available at: https://doi.org/https://doi.org/10.1002/pds.4864 Imagine if your genes could predict how much hair you’ll regrow from minoxidil… or whether you could get side effects from finasteride. This would be a breakthrough in hair loss treatments. And yet, according to some genetic testing companies, this breakthrough is already here and available (for a price).
Certain telehealth companies now offer to sequence your DNA to help you create a more tailored, personalized treatment plan for your hair loss.[1]TrichoTest. (no date). Personalizing alopecia treatment. Fagron Genomics. Available at: https://gxsciences.com/trichotest/. (Accessed: October 2024) Depending on your genetics, they might recommend substituting finasteride for dutasteride, oral over topical minoxidil, or adding corticosteroids – all based on the latest scientific data.
Who wouldn’t want to do this? It would enable you to create the highest-value and lowest-risk treatment plan for yourself.
However, the quality of the evidence surrounding this approach isn’t so cut and dry. That’s why we conducted a four-month research project in which we identified 12 genes that some companies say are associated with treatment efficacy. We looked at the available literature to determine what the science says, the quality behind it, and whether it is even relevant to hair loss.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
Single Nucleotide Polymorphisms (SNPs)
SNPs are changes at a single position in a DNA sequence. They can occur within genes or in the regions between genes. SNPs are the most common type of genetic variation in humans, occurring once in every 100-300 nucleotides in the human genome.[2]Nelson, M.R., Marnellos, G., Kammerer, S., Hoyal, C.R., Shi, M.M., Cantor, C.R., Braun, A. (2004). Large-scale validation of single nucleotide polymorphisms in gene regions. Genome Research. … Continue reading
In coding regions of genes, SNPs can be:
- Synonymous, i.e., they do not affect the protein sequence
- Nonsynonymous, i.e., they change the protein’s amino acid sequence [3]Sun, Y., Zhang, Y., Zhang, X. (2019). Synonymous SNPs of viral genes facilitate virus to escape host antiviral RNAi immunity. RNA Biology. 16(12). 1697-1710. Available at: … Continue reading
SNPs in non-coding regions of genes can affect gene expression, gene splicing, or other regulatory processes.[4]Degtyareva, A.O., Antontseva, E.V., Merkulova, T.I. (2021). Regulatory SNPs: Altered Transcription Factor Binding Sites Implicated in Complex Traits and Diseases. International Journal of Molecular … Continue reading Like genes, SNPs are inherited from parents to their children and contribute to genetic differences between people.
SNPs in certain genes may increase susceptibility to specific diseases. For example, a large-scale genome-wide association study identified 71 significantly associated loci for male pattern baldness, indicating a genetic aspect to the pathogenesis of androgenic alopecia.[5]Pirastu, N., Joshi, P.K., deVries, P.S., Cornerlis, M.C., McKeigue, P.M., Keum, N., Franceschini, N., Colombo, M., Giovannucci, E.L., Spiliopoulou, A., Franke, L., North, K.E., Kraft, Morrison, A.C., … Continue reading
So, now that we’ve discussed genes and SNPs, let’s examine what we found.
We’ve created a table of every gene we analyzed to give you an overview of the articles. Below, we will summarize each gene and its potential for advising treatment efficacy.
Gene SNP What the Genetic Testing Companies Say What the Evidence Says Treatment Relevance (1-5) ACE rs4341 People with a deletion variant of this polymorphism (CG or GG) may want to try treatments that improve blood flow to the scalp. The deletion allele (G) is associated with increased ACE activity, which leads to vasoconstriction and reduced blood flow. No studies show an association between this polymorphism and the response to hair treatments that may improve blood flow.
1 rs4343 People with a deletion variant of this polymorphism (AG or GG) may want to try treatments that improve blood flow to the scalp. The deletion allele (G) is associated with increased ACE activity, which leads to vasoconstriction and reduced blood flow. No studies show an association between this polymorphism and the response to hair treatments that may improve blood flow.
BTD rs13078881 People with the CC or CG variants may be good candidates for biotin supplementation. The CC and CG genotypes were associated with biotinidase deficiency in a study of 19 children. Adults with this polymorphism exhibited biotinidase deficiency but presented no symptoms.
No studies show an association between this polymorphism and hair loss or the response to biotin supplementation.
1 COL1A1 rs1800012 People with the GT variant may benefit from supplementation that supports collagen formation. People with the GT variant were found to have an increased ratio of α1 to α2 chains, which could lead to instability of the collagen molecules. No studies show an association between this polymorphism and the response to supplements that support collagen formation.
1 CRABP2 rs12724719 People with the AA variant may not benefit from standard retinoic acid supplementation and may require an increased dose or alternative treatment. Newborn babies with the AA variant were found to have increased retinoic acid levels in their umbilical cord blood. It is not known if the same effect is seen in adults. No studies show an association between this polymorphism and the response to retinoic acid supplementation.
1 CYP19A1 rs2470152 People with the TC variant may benefit from treatment with replacement hormones (e.g., estradiol) or anti-androgens. People with the TC variant were found to exhibit increased testosterone levels and a reduced ratio of estradiol to testosterone. No studies show an association between this polymorphism and hair loss or the response to replacement hormones and anti-androgens.
1 rs700519 People with the CC variant may be a good candidate for the typical or higher dosages of 5α-reductase inhibitors. People with the CT or TT variants may be good candidates for lower dosages of 5α-reductase inhibitors.
People with the CT or TT variant were shown to respond better to treatment with dutasteride. However, some people with CT or TT were still classified as being poor responders to dutasteride treatment. GPR44 rs533116 People with the AA variant may be good candidates for treatment with PGD2 inhibitors. People with the AA variant exhibited increased GPR44 expression in their white blood cells, which may increase sensitivity to PGD2. No studies show an association between this polymorphism and the response to treatment with PGD2 inhibitors.
1 rs545659 People with the GG variant may be good candidates for treatment with PGD2 inhibitors. People with the GG variants exhibited greater GPR44 mRNA stability, which may increase PGD2 activity. No studies show an association between this polymorphism and the response to treatment with PGD2 inhibitors.
GRα/GRꞵ (NR3C1) rs6198 People with the GG variant may not respond as well to glucocorticoid treatment. People with the GG variant exhibited a form of the glucocorticoid receptor that does not bind as well to glucocorticoids. No studies show an association between this polymorphism and the response to glucocorticoid treatment for hair loss.
1 IGF1R rs2229765 People carrying at least one A allele may be good candidates for IGF-1 supplementation. People with the AG or AA genotype were found to exhibit lower levels of IGF-1 in their plasma. No studies show an association between this polymorphism and the response to supplementation with IGF-1.
1 PGTFR rs10782665 People carrying at least one T allele have an increased probability of a positive response to treatment with Latanoprost. The presence of a G allele was found to increase the probability of a positive response to Latanoprost treatment for intraocular pressure in mice. No studies show an association between this polymorphism and hair loss response to treatment with Latanoprost.
2 rs1328441 People carrying at least one G allele have an increased probability of a positive response to treatment with Latanoprost. The presence of a G allele was found to increase the probability of a positive response to Latanoprost treatment for intraocular pressure in mice. No studies show an association between this polymorphism and hair loss response to treatment with Latanoprost.
rs6686438 People carrying at least one G allele have an increased probability of a positive response to treatment with Latanoprost. The presence of a G allele was found to increase the probability of a positive response to Latanoprost treatment for intraocular pressure in mice. No studies show an association between this polymorphism and hair loss response to treatment with Latanoprost.
PTGES2 rs13283456 People with the CT variant have reduced PTGES2 enzymatic activity, which reduces PGE2 levels. This makes them better candidates for treatment with minoxidil, which increases PGE2 levels. The CT variant is associated with reduced BMI in males. However, no direct evidence exists that it is associated with PTGES2 activity or PGE2 levels. There are no studies that show an association between this polymorphism and the response to treatment with minoxidil.
1 SRD5A1 &
SRD5A2
rs248793 People carrying at least one C allele have increased levels of DHT, which may make them good candidates for treatment with 5α-reductase inhibitors. The presence of a C allele in adults was found to be associated with an increased DHT/T ratio. No studies show an association between this polymorphism and the response to treatment with 5α-reductase inhibitors.
2 rs523349 People with the GG variant have increased 5α-reductase activity, which may make them good candidates for treatment with 5α-reductase inhibitors. The GG variant is associated with increased 5α-reductase activity, which may increase DHT levels. No studies show an association between this polymorphism and the response to treatment with 5α-reductase inhibitors.
SULT1A1 rs9282861 People carrying at least one A allele have reduced sulfotransferase activity, which may alter their response to minoxidil. Sulfotransferase activity was reduced in people with the GA variant and further in those with the AA variant. Sulfotransferase catalyzes the conversion of minoxidil to its active form, minoxidil sulfate.
Small-scale human studies have shown that people with the GG variant may respond better to minoxidil treatment for hair loss.
3 Angiotensin-converting enzyme (ACE)
ACE is a key enzyme in blood pressure regulation. It converts angiotensin I to angiotensin II, causing vasoconstriction. The ACE gene has an insertion/deletion (I/D) polymorphism that affects enzyme activity, with the deletion (D) allele associated with higher ACE levels and increased vasoconstrictions.[6]Wong, M. K. S. (2016). Angiotensin Converting Enzymes. In Handbook of Hormones. pp. 263-e29D-4. Elsevier. Available at: https://doi.org/10.1016/B978-0-12-801028-0.00254-3
Some research suggests a link between ACE gene polymorphisms and androgenic alopecia (AGA). Certain genetic testing companies propose that individuals with specific ACE polymorphisms may benefit from treatments that improve scalp blood flow. The theory is that higher ACE activity leads to increased vasoconstriction, potentially reducing blood flow to hair follicles. Therefore, treatments like minoxidil or caffeine, which may work partly through vasodilation, could be more effective for individuals with these genetic variants.

Figure 1: Comparison between AGA patients and controls regarding ACE genotypes. The insertion/deletion (ID) and deletion/deletion (DD) genotypes were significantly increased in AGA patients compared to controls.[7]Ibrahim, M.A., Ezzat, I.S., Mostafa, G.Y., Fathy, A.H.N., Eman, F., Samir, E.S.O. (2021). Association between angiotensin-converting enzyme gene insertion-deletion polymorphism and androgenetic … Continue reading
However, while this hypothesis is intriguing, no direct evidence demonstrates that people with particular ACE polymorphisms respond differently to hair loss treatments that improve blood flow.
Read our ACE gene article here.
Biotinidase (BTD)
The BTD gene encodes biotinidase, an enzyme crucial for recycling and utilizing biotin (Vitamin B7) in the body. Biotin is vital in various biological functions, including hair health, through its involvement in protein synthesis and keratin production.[8]Leon‐Del‐Rio, A. (2019). Biotin in metabolism, gene expression, and human disease. Journal of Inherited Metabolic Disease, 42(4), 647-654. Available at: https://doi.org/10.1002/jimd.12073
Mutations in BTD can lead to biotinidase deficiency, which can cause biotin deficiency or dependency. This condition can result in various symptoms, including hair abnormalities and alopecia.
According to some, certain BTD polymorphisms might predict the efficacy of biotin treatment for hair loss. However, the evidence supporting this claim is limited and inconclusive.[9]Bhattarai, D., Banday, A. Z., Sadanand, R., Arora, K., Kaur, G., Sharma, S., & Rawat, A. (2021). Hair microscopy: an easy adjunct to diagnosis of systemic diseases in children. Applied … Continue reading Studies have shown conflicting results regarding the impact of this polymorphism on biotinidase activity in adults and children, and none specifically address hair loss.
Read our BTD gene article here.
Collagen Type 1 Alpha 1 Chain (COL1A1)
COL1A1 encodes one of the chains of type I collagen, the most abundant collagen in the body. Type I collagen is crucial in supporting tissue structure throughout the body.[10]Ricard-Blum, S. (2011). The collagen family. Cold Spring Harbor perspectives in biology, 3(1), a004978. Available at: https://doi.org/10.1101/cshperspect.a004978
COL1A1 gene expression is upregulated in people with AGA.[11]Michel, L., Reygagne, P., Benech, P., Jean‐Louis, F., Scalvino, S., Ly Ka So, S., Hamidou, Z., Bianovici, S., Pouch, J., Ducos, B. and Bonnet, M., 2017. Study of gene expression alteration in male … Continue reading Furthermore, studies have shown the SNPs in the COL1A1 gene can affect collagen stability.[12]Mann, V., Hobson, E.E., Li, B., Stewart, T.L., Grant, S.F., Robins, S.P., Aspden, R.M. and Ralston, S.H. (2001). A COL1A1 Sp1 binding site polymorphism predisposes to osteoporotic fracture by … Continue reading

Figure 2: Collagen protein and mRNA levels in osteoblasts (cells that form new bones) cultured from patients with different genotypes. Different genotypes of the rs1800012 polymorphism are shown. SS genotype = GG genotype; Ss genotype = GT genotype.[13]Mann, V., Hobson, E.E., Li, B., Stewart, T.L., Grant, S.F., Robins, S.P., Aspden, R.M. and Ralston, S.H. (2001). A COL1A1 Sp1 binding site polymorphism predisposes to osteoporotic fracture by … Continue reading
While these findings suggest a potential role for COL1A1 in hair growth and loss, the exact mechanisms are not fully understood. More research is needed to clarify how variations in COL1A1 might influence hair loss and treatment responses. Currently, limited evidence supports targeting COL1A1 specifically for hair loss treatments.
Read our COL1A1 gene article here.
CRAPB2
CRABP2 is one of two genes in the cellular retinoic acid-binding protein family and is crucial for regulating retinoic acid by transporting it within cells and aiding its metabolism. Retinoic acid is important for hair health, but its deficiency and excess can lead to hair loss, indicating a dose-dependent relationship.[14]Wei, L. N. (2016). Cellular retinoic acid binding proteins: Genomic and non-genomic functions and their regulation. The Biochemistry of Retinoid Signaling II: The Physiology of Vitamin A-Uptake, … Continue reading
This gene is highly expressed in dermal papilla cells, which are vital for hair follicle growth and development.[15]He, M., Lv, X., Cao, X., Yuan, Z., Quan, K., Getachew, T., Mwacharo, J.M., Haile, A., Li, Y., Wang, S. and Sun, W. (2023). CRABP2 Promotes the Proliferation of Dermal Papilla Cells via the … Continue reading Overexpression of CRABP2 promotes cell growth, suggesting a positive role in hair maintenance. However, increased CRABP2 expression and elevated retinoic acid levels have also been associated with hair loss conditions like alopecia areata and AGA.[16]Duncan, F.J., Silva, K.A., Johnson, C.J., King, B.L., Szatkiewicz, J.P., Kamdar, S.P., Ong, D.E., Napoli, J.L., Wang, J., King Jr, L.E. and Whiting, D.A. (2013). Endogenous retinoids in the … Continue reading
Despite this paradox, treatments using tretinoin have shown promise, stimulating hair regrowth in over half of patients, with further improvements observed after combination with minoxidil.[17]Bazzano, G. S., Terezakis, N., & Galen, W. (1986). Topical tretinoin for hair growth promotion. Journal of the American Academy of Dermatology, 15(4), 880-893. Available at: … Continue reading

Figure 3: Level of hair regrowth after treatment with either a placebo, minoxidil (0.5%), tretinoin (0.025%), or a combination of tretinoin and minoxidil.[18]Bazzano, G. S., Terezakis, N., & Galen, W. (1986). Topical tretinoin for hair growth promotion. Journal of the American Academy of Dermatology, 15(4), 880-893. Available at: … Continue reading
One large study involving over 25,000 AGA patients found an association between this polymorphism and AGA, suggesting that genetic differences in CRABP2 could impact hair health and treatment efficacy.[19]Francès, M. P., Vila-Vecilla, L., Russo, V., Caetano Polonini, H., & de Souza, G. T. (2024). Utilising SNP Association Analysis as a Prospective Approach for Personalising Androgenetic Alopecia … Continue reading Ultimately, further research is needed to show exactly how it might affect treatment efficacy.
Read our CRABP2 gene article here.
CYP19A1
CYP19A1 encodes the enzyme aromatase, which converts androgens like testosterone into estrogens like estradiol. Reduced expression of CYP19A1 and lower enzyme activity have been associated with female pattern hair loss (FPHL) and AGA. Aromatase levels are higher in non-balding scalp regions and significantly higher in women than men, possibly explaining gender differences in hair loss patterns.[20]Nebert, D. W., Wikvall, K., & Miller, W. L. (2013). Human cytochromes P450 in health and disease. Philosophical Transactions of the Royal Society B: Biological Sciences, 368(1612), 20120431. … Continue reading
Aromatase helps decrease levels of DHT, and aromatase inhibitors have been linked to hair thinning, indicating a role for the enzyme in hair health. Treatments like minoxidil may increase aromatase activity, which can improve hair growth by increasing estradiol and reducing DHT levels.[21]Gallicchio, L., Calhoun, C., & Helzlsouer, K. J. (2013). Aromatase inhibitor therapy and hair loss among breast cancer survivors. Breast cancer research and treatment, 142, 435-443. Available at: … Continue reading
While certain genetic variations have been associated with better response to treatments like dutasteride, the study also showed that some people with this SNP can be poor responders, indicating that it is probably a combination of SNPs that affects treatment response.

Figure 4: Genotypic landscape of 42 patients, the cumulative effect of each allele count, and their positive or negative effect. Boxes represent SNPs that exhibited a positive (blue) or negative (red) effect on the patient’s response to dutasteride. Light-colored boxes represent heterozygous SNPs (a variation where an individual has two different versions of a specific DNA sequence at a particular location in the genome), dark-colored boxes represent homozygous SNPs (a variation where an individual has two identical versions of a specific DNA sequence at a particular location in the genome). Patient responses to dutasteride improve from left to right.[22]Rhie, A., Son, H.Y., Kwak, S.J., Lee, S., Kim, D.Y., Lew, B.L., Sim, W.Y., Seo, J.S., Kwon, O., Kim, J.I. and Jo, S.J. (2019). Genetic variations associated with response to dutasteride in the … Continue reading
So, while there is evidence that CYP19A1 SNPs can affect treatment efficacy, studies have not been done to determine the relationship between these and hair growth.
Read our CYP19A1 gene article here.
GPR44
The GPR44 gene encodes G-protein-coupled receptor 44 (the prostaglandin D2 receptor or DP2). GPR44 is significant because it mediates the effects of prostaglandin D2, a lipid compound involved in inflammation and the immune response.[23]National Library of Medicine. (2024). PTGDR2 Prostaglandin D2 Receptor 2 [Homo sapiens (human)]. NIH. Available at: https://www.ncbi.nlm.nih.gov/gene/11251 (Accessed: 12 July 2024.)
PGD2 levels are elevated in balding scalps compared to haired scalps. Additionally, PGD2 inhibits hair growth in isolated human hair follicles and mouse models. Overexpression of PGD2 has been shown to lead to premature hair follicle regression and alopecia in mice. Furthermore, mice lacking the GPR44 receptor did not exhibit hair loss when exposed to PGD2, indicating that GPR44 is important for PGD2’s hair growth inhibition.[24]Nieves, A., Garza, L.A. (2014). Does Prostaglandin D2 Hold the Cure to Male Pattern Baldness? Experimental Dermatology. 23(4). 224-227. Available at: https://doi.org/10.1111/exd.12348,[25]Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). … Continue reading

Figure 5: Figure 2. Hair length 10 days after topical PGD2 (1 ug), 15-dPGJ2 (1 ug) or vehicle treatment.[26]Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). Prostaglandin D2 Inhibits Hair Growth and is Elevated in Bald Scalp of Men with Androgenetic … Continue reading
However, one clinical trial using setipiprant, a GPR44 antagonist, showed no significant improvement in hair growth compared to a placebo in men with AGA, indicating that PGD2 signaling through GPR44 alone might not be sufficient for treating hair loss.[27]DuBois, J., Bruce, S., Stewart, D., Kempers, S., Harutunian, C., Boodhoo, T., Weitzenfeld, A, Chang-Lin, J.E. (2021). Setipiprant for Androgenetic Alopecia in Males: Results from a Randomized, … Continue reading
SNPs in GPR44 have been associated with increased receptor expression and asthma severity, hinting that similar mechanisms might affect hair loss.[28]Campos Alberto, E., Maclean, E., Davidson, C., Palikhe, N.S., Storie, J., Tse, C., Brenner, D., Mayers, I., Vliagoftis, H., El-Sohemy, A., Cameron, L. (2012). The Single Nucleotide Polymorphism CRTh2 … Continue reading,[29]Huang, J.L., Gao, P.S., Mathias, R.A., Yao, T.C., Chen, L.C., Kuo, M.L., Hsu, S.C., Plunkett, B., Togias, A., Barnes, K.C., Stellato, C., Beaty, T.H., Huang, S.K. Sequence Variants of the Gene … Continue reading
Nonetheless, conflicting study results and poorly controlled variables make it unclear whether targeting GPR44 is effective for treating hair loss.
Read our GPR44 gene article here.
IGF1R
IGF1R encodes the insulin-like growth factor-1 receptor, which mediates the effects of IGF-1, a protein crucial for hair follicle development and the hair growth cycle. IGF-1 promotes cell growth, division, and survival in hair follicles and regulates the transition between the growth (anagen) and red (catagen) phases.[30]Ahn, S. Y., Pi, L. Q., Hwang, S. T., & Lee, W. S. (2012). Effect of IGF-I on hair growth is related to the anti-apoptotic effect of IGF-I and up-regulation of PDGF-A and PDGF-B. Annals of … Continue reading
Studies have linked low levels of IGF-1 to AGA and hair loss. For instance, individuals with Laron syndromes, characterized by deficient IGF-1 production, often experience thinner hair and alopecia in adulthood.[31]Lurie, R., Ben-Amitai, D., & Laron, Z. (2004). Laron syndrome (primary growth hormone insensitivity): a unique model to explore the effect of insulin-like growth factor 1 deficiency on human … Continue reading IGF-1 is also significantly reduced in balding compared to non-balding scalps.[32]Panchaprateep, R., & Asawanonda, P. (2014). Insulin‐like growth factor‐1: roles in androgenetic alopecia. Experimental dermatology, 23(3), 216-218. Available at: … Continue reading Additionally, middle-aged women with lower circulating IGF-1 levels have a higher risk of developing hair loss.[33]Noordam, R., Gunn, D. A., Drielen, K. V., Westgate, G., Slagboom, P. E., Craen, A. D., & Heemst, D. V. (2016). Both low circulating insulin‐like growth factor‐1 and high‐density lipoprotein … Continue reading
Genetic variation in IGF1R influences plasma IGF-1 levels, with some maintaining normal levels and some exhibiting reduced levels. This suggests a potential role of IGF-1 supplementation in those with lower IGF-1 levels.[34]Bonafè, M., Barbieri, M., Marchegiani, F., Olivieri, F., Ragno, E., Giampieri, C., Mugianesi, E., Centurelli, M., Franceschi, C. and Paolisso, G. (2003). Polymorphic variants of insulin-like growth … Continue reading

Figure 6: Plasma IGF-1 levels depending on IGF1R gene variation. The AA and AG genotypes are associated with lower plasma IGF-1 levels. In contrast, the GG genotype is associated with normal IGF-1 levels.[35]Bonafè, M., Barbieri, M., Marchegiani, F., Olivieri, F., Ragno, E., Giampieri, C., Mugianesi, E., Centurelli, M., Franceschi, C. and Paolisso, G. (2003). Polymorphic variants of insulin-like growth … Continue reading
However, no direct link has been established between the rs2229765 SNP and specific hair loss disorders.
Read the full IGF1R gene article here.
NR3C1
NR3C1 encodes the glucocorticoid receptor (GR), which mediates the action of glucocorticoids, impacting metabolism, immune response, and stress response. There are two main isoforms: GRɑ, which binds glucocorticoids, and GRβ, which can inhibit GRɑs activity.[36]Oakley, R.H., Cidlowski, J.A. (2013). The Biology of the Glucocorticoid Receptor: New Signaling Mechanisms in Health and Disease. Journal of Allergy and Clinical Immunology. 132(5). 1033-1044. … Continue reading
GRs regulate the transitions between different phases of the hair cycle. They can influence the transition from anagen (active growth) to catagen (regression) phases. Furthermore, GRs are expressed in various components of the hair follicle, including dermal papilla cells, outer root sheath keratinocytes, and hair matrix cells.[37]Kwack, M.H., Hamida, O.B., Moon, K.K., Kim, J.C., Sung, Y.K. (2022). Dexamethasone, a Synthetic Glucocorticoid, Induces the Activity of Androgen Receptor in Human Dermal Papilla Cells. Skin … Continue reading
Certain genetic variants in NR3C1 have been linked to glucocorticoid resistance due to altered mRNA stability, affecting GR function. While these variations do impact glucocorticoid activity, there is no evidence to connect these effects to responsiveness to corticosteroids in hair loss, as the study was conducted in children with acute lymphoblastic leukemia.[38]Gasic, V., Zukic, B., Stankovic, B., Janic, D., Dokmanovic, L., Lazic, J., Krstovski, N., Dolzan, V., Jazbec, J., Pavlovic, S., Kotur, N. (2018). Pharmacogenomic Markers of Glucocorticoid Response in … Continue reading

Figure 7: Genotype frequencies associated with glucocorticoid response. The bold numbers indicate a significant difference. NR3C1 6198 shows a significant association with glucocorticoid resistance.[39]Gasic, V., Zukic, B., Stankovic, B., Janic, D., Dokmanovic, L., Lazic, J., Krstovski, N., Dolzan, V., Jazbec, J., Pavlovic, S., Kotur, N. (2018). Pharmacogenomic Markers of Glucocorticoid Response in … Continue reading
Read more about the NR3C1 gene here.
PGTFR
The PGTFR gene encodes the prostaglandin F2 alpha receptor and plays a key role in hair follicle health and pigmentation. This receptor also involves broader physiological processes, including reproduction, inflammation, and cancer. Still, its influence on hair growth has made it a target in hair loss research.[40]Ricciotti, E., FitzGerald, G.A. (2011). Prostaglandins and Inflammation. Arteriosclerosis, Thrombosis, and Vascular Biology. 31(5). 986-1000. Available at: … Continue reading Studies in animal models have shown that PGF2ɑ and its analogs, such as latanoprost, stimulate the hair follicle and melanocyte growth, hinting at potential therapeutic benefits for hair loss treatments.
Genetic variants within PGTFR have been linked to varied responses to latanoprost in glaucoma treatment. Those with one genotype have been associated with greater response to latanoprost, while others were associated with reduced effectiveness.[41]Sakurai, M., Higashide, T., Takahashi, M., Sugiyama, K. (2007). Association between Genetic Polymorphisms of the Prostaglandin F2ɑ Receptor Gene and Response to Latanoprost. Ophthalmology. 114(6). … Continue reading Similarly, other SNPs have corresponded with lower receptor activity, indicating decreased response to PGF2ɑ analogs.

Figure 8: Latanoprost responsiveness based on single nucleotide polymorphism.[42]↑4 Sakurai, M., Higashide, T., Takahashi, M., Sugiyama, K. (2007). Association between Genetic Polymorphisms of the Prostaglandin F2ɑ Receptor Gene and Response to Latanoprost. Ophthalmology. … Continue reading
In the context of hair loss, we know that some evidence exists to show that latanoprost might benefit hair regrowth.[43]Blume-Peytavi, U., Lonngors, S., Hillmann, K., Bartels, N.G. (2012). A Randomized, Double-Blind, Placebo-Controlled Pilot Study to Assess the Efficacy of a 24-Week Topical Treatment by Latanoprost … Continue reading However, no studies have linked any SNPs to treatment efficacy in the hair follicle.
Read the PGTFR gene article here.
PTGES2
The PTGES2 gene encodes prostaglandin E synthase 2, an enzyme that converts prostaglandin H2 (PGH2) to prostaglandin E2 (PGE2). This enzyme is critical in the prostaglandin synthesis pathway and plays a role in inflammation and hair growth. PGE2 levels are higher in non-balding scalp regions than in balding ones, suggesting that PTGES2 and its product PGE2 might contribute to hair preservation and growth.[44]Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). … Continue reading
Studies on AGA patients have found that PTGES2 expression increases in balding areas, likely as a compensatory response.[45]Villareal-Villareal, C.D., Sinclair, R.D., Martinez-Jacobo, L., Garza-Rodriguez, V., Rodriguez-Leon, S.A., Lamadrid-Zertuche, A.C., Rodriguez-Gutierrez, R., Ortiz-Lopez, R., Rojas-Martinez, A., … Continue reading Genetic association studies have also linked a PTGES2 SNP to AGA. However, this does not appear to correlate with the severity of hair loss.[46]Frances, M.P., Vila-Vecilla, L., Russo, V., Polonini, H.C., de Souza, G.T. (2024). Utilizing SNP Association Analysis as a Prospective Approach for Personalising Androgenetic Alopecia Treatment. … Continue reading

Figure 9: Prostaglandin mean levels (ng/g tissue) in patients with AGA comparing bald areas with non-balding.[47]Chovarda, E., Sotiriou, E., Lazaridoi, E., Vakirlis, E., Ioannides, D. (2021). The Role of Prostaglandins in Androgenetic Alopecia. International Journal of Dermatology. 60. 730-735. Available at: … Continue reading
Interestingly, some research suggests PTGES2 could influence responses to minoxidil as it has been shown to increase PGE2 production in hair follicle cells.[48]Michelet, J.F., Commo, S., Billoni, N., Mahe, Y.F., Bernard, B.A. (1997). Activation of cytoprotective prostaglandin synthase-1 by minoxidil as a possible explanation for its hair growth-stimulating … Continue reading This indicates that individuals with PTGES2 variants possibly associated with lower enzyme activity might benefit more from minoxidil, as the treatment could help elevate PGE2 levels. However, general genetic findings should be interpreted carefully, as gene expression patterns in hair follicles may differ significantly from those in other tissues.
Read the PTGES2 gene article here.
SRD5A1 & SRD5A2
The SRD5A1 and SRD5A2 genes encode type I and type II 5ɑ-reductase enzymes, which are crucial for converting testosterone into dihydrotestosterone (DHT).[49]Scaglione, A., Montemiglio, L.C., Parisi, G., Asteriti, I.A., Bruni, R., Cerutti, G., Testi, C., Savino, C., Mancia, F., Lavia, P. and Vallone, B. (2017). Subcellular localization of the five members … Continue reading Inhibitors targeting these enzymes, particularly finasteride, and dutasteride, are central to AGA treatment. Genetic variations in SRD5A1 and SRD5A2 have shown potential in influencing the effectiveness of these treatments.
In a study of AGA patients treated with dutasteride, certain SNPs in SRD5A1 were positively associated with treatment response, meaning individuals with these variants responded better. However, even patients with these SNPs displayed varied responses, suggesting that the overall genetic profile, rather than individual SNPs alone, likely plays a role in treatment efficacy.[50]Rhie, A., Son, H.Y., Kwak, S.J., Lee, S., Kim, D.Y., Lew, B.L., Sim, W.Y., Seo, J.S., Kwon, O., Kim, J.I. and Jo, S.J. (2019). Genetic variations associated with response to dutasteride in the … Continue reading Interestingly, no SRD5A2 SNPs were found to significantly impact dutasteride response in this study, although variations in SRD5A2 may still affect DHT production and, consequently, treatment outcomes.
Additional research hints that SRD5A gene variants influence enzyme activity. In particular, individuals with higher DHT levels due to SRD5A1 or SRD5A2 variants might require higher doses or longer treatment durations for 5ɑ-reductase inhibitors to show efficacy. Lab studies have further suggested that specific variants of SRD5A2 might respond differently to finasteride versus dutasteride, emphasizing that personalized treatment approaches could optimize hair loss management.[51]Makridakis, N.M., di Salle, E., and Reichardt, J.K. (2000). Biochemical and pharmacogenetic dissection of human steroid 5α-reductase type II. Pharmacogenetics and Genomics, 10(5), 407-413. Available … Continue reading
While further clinical studies are needed to confirm these findings, early data suggest that SRD5A1 and SRD5A2 genotyping could improve the efficacy of 5ɑ-reductase inhibitor treatments.
Read the full SRD5A1 and SRD5A2 gene article here.
SULT1A1
The SULT1A1 gene encodes the enzyme sulfotransferase 1A1, part of the sulfotransferase family. This enzyme plays a critical role in the metabolism and detoxification of various compounds. In hair loss treatment, SULT1A1 is especially important because it activates minoxidil through sulfonation, converting it into minoxidil sulfate, the active form needed to stimulate hair growth.[52]Goren, A., Castano, J.A., McCoy, J., Bermudez, F., Lotti, T. (2014). Novel enzymatic assay predicts minoxidil response in the treatment of androgenetic alopecia. Dermatologic Therapy. 27. 171-173. … Continue reading
Evidence suggests that specific SULT1A1 gene variants correlate with varying levels of enzyme activity and minoxidil responsiveness. Some genetic variations have been shown to lead to higher sulfotransferase activity and greater hair growth response after minoxidil treatment, whereas those with other genotypes exhibited lower enzyme activity and may have a weaker response to the drug.[53]Raghad, N.A., Al-Gazally, M.E., Ewahd, W.A. (2017). Assessment the effect of different genotypes of sulfotransferase 1A1 gene on the response to minoxidil in patients with androgenic alopecia. … Continue reading

Figure 10: (Top) The proportion of participants in the R0 (“non-responder”) and R1 (“responder”) groups with each allele variation. (Bottom) The proportion of participants in the R0 (“non-responder”) and R1 (“responder”) groups with each genotype variation.[54]Raghad, N.A., Al-Gazally, M.E., Ewahd, W.A. (2017). Assessment the effect of different genotypes of sulfotransferase 1A1 gene on the response to minoxidil in patients with androgenic alopecia. … Continue reading
Recent studies have begun using SULT1A1 genotyping as a tool to optimize minoxidil treatment, especially in female-pattern hair loss. However, some people with the “favorable” gene variations still fail to respond, while others with “less favorable” gene variations show substantial hair regrowth. This highlights the need for larger validation studies..[55]Ramos, P.M., Gohad, P., McCoy, J., Wambier, C., Goren, A. (2021). Minoxidil Sulfotransferase Enzyme (SULT1A1) genetic variants predict response to oral minoxidil treatment for female pattern hair … Continue reading
Read more about these studies in the SULT1A1 gene article here.
Should We Be Targeting Genes for Hair Loss Treatment Efficacy?
Based on the evidence in the articles, SULT1A1 currently has the most evidential support. This is especially true as it is one of (if not the only) gene that we have examined that actually examined these SNPs in the hair follicles of people with hair loss.
Aside from this, we don’t see the utility in using our genes to predict hair loss treatment efficacy. That is not to say that we won’t eventually see a use for this, however. As the research evolves, new information might come to light, which we will keep you updated on.
References[+]
References ↑1 TrichoTest. (no date). Personalizing alopecia treatment. Fagron Genomics. Available at: https://gxsciences.com/trichotest/. (Accessed: October 2024) ↑2 Nelson, M.R., Marnellos, G., Kammerer, S., Hoyal, C.R., Shi, M.M., Cantor, C.R., Braun, A. (2004). Large-scale validation of single nucleotide polymorphisms in gene regions. Genome Research. 14(8).1664-1668. Available at: https://doi.org/10.1101/gr.2421604 ↑3 Sun, Y., Zhang, Y., Zhang, X. (2019). Synonymous SNPs of viral genes facilitate virus to escape host antiviral RNAi immunity. RNA Biology. 16(12). 1697-1710. Available at: https://doi.org/10.1080/15476286.2019.1656026 ↑4 Degtyareva, A.O., Antontseva, E.V., Merkulova, T.I. (2021). Regulatory SNPs: Altered Transcription Factor Binding Sites Implicated in Complex Traits and Diseases. International Journal of Molecular Sciences. 22(12). 6454. Available at: https://doi.org/10.3390/ijms22126454 ↑5 Pirastu, N., Joshi, P.K., deVries, P.S., Cornerlis, M.C., McKeigue, P.M., Keum, N., Franceschini, N., Colombo, M., Giovannucci, E.L., Spiliopoulou, A., Franke, L., North, K.E., Kraft, Morrison, A.C., Esko, T., Wilson, J.F. (2017). GWAS for male-pattern baldness identifies 71 susceptibility loci, explaining 38% of the risk. Nature Communications. 8. 1584. Available at: https://doi.org/10.1038/s41467-017-01490-8 ↑6 Wong, M. K. S. (2016). Angiotensin Converting Enzymes. In Handbook of Hormones. pp. 263-e29D-4. Elsevier. Available at: https://doi.org/10.1016/B978-0-12-801028-0.00254-3 ↑7 Ibrahim, M.A., Ezzat, I.S., Mostafa, G.Y., Fathy, A.H.N., Eman, F., Samir, E.S.O. (2021). Association between angiotensin-converting enzyme gene insertion-deletion polymorphism and androgenetic alopecia susceptibility among Egyptian patients: A preliminary case-controlled study. Journal of Cosmetic Dermatology. 21(6). 2629-2634. Available at: https://doi.org/10.1111/jocd.14434 ↑8 Leon‐Del‐Rio, A. (2019). Biotin in metabolism, gene expression, and human disease. Journal of Inherited Metabolic Disease, 42(4), 647-654. Available at: https://doi.org/10.1002/jimd.12073 ↑9 Bhattarai, D., Banday, A. Z., Sadanand, R., Arora, K., Kaur, G., Sharma, S., & Rawat, A. (2021). Hair microscopy: an easy adjunct to diagnosis of systemic diseases in children. Applied Microscopy, 51, 1-12. Available at: https://doi.org/10.1186/s42649-021-00067-6 ↑10 Ricard-Blum, S. (2011). The collagen family. Cold Spring Harbor perspectives in biology, 3(1), a004978. Available at: https://doi.org/10.1101/cshperspect.a004978 ↑11 Michel, L., Reygagne, P., Benech, P., Jean‐Louis, F., Scalvino, S., Ly Ka So, S., Hamidou, Z., Bianovici, S., Pouch, J., Ducos, B. and Bonnet, M., 2017. Study of gene expression alteration in male androgenetic alopecia: evidence of predominant molecular signalling pathways. British Journal of Dermatology, 177(5), 1322-1336. Available at: https://doi.org/10.1111/bjd.15577 ↑12 Mann, V., Hobson, E.E., Li, B., Stewart, T.L., Grant, S.F., Robins, S.P., Aspden, R.M. and Ralston, S.H. (2001). A COL1A1 Sp1 binding site polymorphism predisposes to osteoporotic fracture by affecting bone density and quality. The Journal of Clinical Investigation, 107(7), 899-907. Available at: https://doi.org/10.1172/JCI10347 ↑13 Mann, V., Hobson, E.E., Li, B., Stewart, T.L., Grant, S.F., Robins, S.P., Aspden, R.M. and Ralston, S.H. (2001). A COL1A1 Sp1 binding site polymorphism predisposes to osteoporotic fracture by affecting bone density and quality. The Journal of clinical investigation, 107(7), 899-907. Available at: https://doi.org/10.1172/JCI10347 ↑14 Wei, L. N. (2016). Cellular retinoic acid binding proteins: Genomic and non-genomic functions and their regulation. The Biochemistry of Retinoid Signaling II: The Physiology of Vitamin A-Uptake, Transport, Metabolism and Signaling, 163-178. Available at: https://doi.org/10.1007/978-94-024-0945-1_6 ↑15 He, M., Lv, X., Cao, X., Yuan, Z., Quan, K., Getachew, T., Mwacharo, J.M., Haile, A., Li, Y., Wang, S. and Sun, W. (2023). CRABP2 Promotes the Proliferation of Dermal Papilla Cells via the Wnt/β-Catenin Pathway. Animals, 13(12), 2033. Available at: https://doi.org/10.3390/ani13122033 ↑16 Duncan, F.J., Silva, K.A., Johnson, C.J., King, B.L., Szatkiewicz, J.P., Kamdar, S.P., Ong, D.E., Napoli, J.L., Wang, J., King Jr, L.E. and Whiting, D.A. (2013). Endogenous retinoids in the pathogenesis of alopecia areata. Journal of Investigative Dermatology, 133(2), 334-343. Available at: https://doi.org/10.1038/jid.2012.344 ↑17 Bazzano, G. S., Terezakis, N., & Galen, W. (1986). Topical tretinoin for hair growth promotion. Journal of the American Academy of Dermatology, 15(4), 880-893. Available at: https://doi.org/10.1016/S0190-9622(86)80024-X ↑18 Bazzano, G. S., Terezakis, N., & Galen, W. (1986). Topical tretinoin for hair growth promotion. Journal of the American Academy of Dermatology, 15(4), 880-893. Available at: https://doi.org/10.1016/S0190-9622(86)80024-X ↑19 Francès, M. P., Vila-Vecilla, L., Russo, V., Caetano Polonini, H., & de Souza, G. T. (2024). Utilising SNP Association Analysis as a Prospective Approach for Personalising Androgenetic Alopecia Treatment. Dermatology and Therapy, 14(4), 971-981. Available at: https://doi.org/10.1007/s13555-024-01142-y ↑20 Nebert, D. W., Wikvall, K., & Miller, W. L. (2013). Human cytochromes P450 in health and disease. Philosophical Transactions of the Royal Society B: Biological Sciences, 368(1612), 20120431. Available at: https://doi.org/10.1098/rstb.2012.0431 ↑21 Gallicchio, L., Calhoun, C., & Helzlsouer, K. J. (2013). Aromatase inhibitor therapy and hair loss among breast cancer survivors. Breast cancer research and treatment, 142, 435-443. Available at: https://doi.org/10.1007/s10549-013-2744-2 ↑22 Rhie, A., Son, H.Y., Kwak, S.J., Lee, S., Kim, D.Y., Lew, B.L., Sim, W.Y., Seo, J.S., Kwon, O., Kim, J.I. and Jo, S.J. (2019). Genetic variations associated with response to dutasteride in the treatment of male subjects with androgenetic alopecia. Plos one, 14(9), e0222533. Available at: https://doi.org/10.1371/journal.pone.0222533 ↑23 National Library of Medicine. (2024). PTGDR2 Prostaglandin D2 Receptor 2 [Homo sapiens (human)]. NIH. Available at: https://www.ncbi.nlm.nih.gov/gene/11251 (Accessed: 12 July 2024.) ↑24 Nieves, A., Garza, L.A. (2014). Does Prostaglandin D2 Hold the Cure to Male Pattern Baldness? Experimental Dermatology. 23(4). 224-227. Available at: https://doi.org/10.1111/exd.12348 ↑25 Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). Prostaglandin D2 Inhibits Hair Growth and is Elevated in Bald Scalp of Men with Androgenetic Alopecia. Science Translational Medicine. 4(126). 1-21. Available at: https://doi.org/10.1126/scitranslmed.3003122 ↑26 Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). Prostaglandin D2 Inhibits Hair Growth and is Elevated in Bald Scalp of Men with Androgenetic Alopecia. Science Translational Medicine. 4(126). 1-21. Available at: https://doi.org/10.1126/scitranslmed.3003122 ↑27 DuBois, J., Bruce, S., Stewart, D., Kempers, S., Harutunian, C., Boodhoo, T., Weitzenfeld, A, Chang-Lin, J.E. (2021). Setipiprant for Androgenetic Alopecia in Males: Results from a Randomized, Double-Blind, Placebo-Controlled Phase 2a Trial. Clinical Cosmetic and Investigative Dermatology. 14. 1507-1517. Available at: https://doi.org/10.2147/CCID.S319676 ↑28 Campos Alberto, E., Maclean, E., Davidson, C., Palikhe, N.S., Storie, J., Tse, C., Brenner, D., Mayers, I., Vliagoftis, H., El-Sohemy, A., Cameron, L. (2012). The Single Nucleotide Polymorphism CRTh2 rs533116 is Associated with Allergic Asthma and Increased Expression of CRTh2. Allergy. 67(11). 1357-1364. Available at: https://doi.org/10.1111/all.12003 ↑29 Huang, J.L., Gao, P.S., Mathias, R.A., Yao, T.C., Chen, L.C., Kuo, M.L., Hsu, S.C., Plunkett, B., Togias, A., Barnes, K.C., Stellato, C., Beaty, T.H., Huang, S.K. Sequence Variants of the Gene Encoding Chemoattractant Receptor Expressed on Th2 Cells (CRTH2) are Associated with Asthma and Differentially Influence mRNA Stability. Human Molecular Genetics. 13(21). 2691-2697. Available at: https://doi.org/10.1093/hmg/ddh279 ↑30 Ahn, S. Y., Pi, L. Q., Hwang, S. T., & Lee, W. S. (2012). Effect of IGF-I on hair growth is related to the anti-apoptotic effect of IGF-I and up-regulation of PDGF-A and PDGF-B. Annals of dermatology, 24(1), 26-31. Available at: https://doi.org/10.5021/ad.2012.24.1.26 ↑31 Lurie, R., Ben-Amitai, D., & Laron, Z. (2004). Laron syndrome (primary growth hormone insensitivity): a unique model to explore the effect of insulin-like growth factor 1 deficiency on human hair. Dermatology, 208(4), 314-318. Available at: https://doi.org/10.1159/000077839 ↑32 Panchaprateep, R., & Asawanonda, P. (2014). Insulin‐like growth factor‐1: roles in androgenetic alopecia. Experimental dermatology, 23(3), 216-218. Available at: https://doi.org/10.1111/exd.12339 ↑33 Noordam, R., Gunn, D. A., Drielen, K. V., Westgate, G., Slagboom, P. E., Craen, A. D., & Heemst, D. V. (2016). Both low circulating insulin‐like growth factor‐1 and high‐density lipoprotein cholesterol are associated with hair loss in middle‐aged women. British Journal of Dermatology, 175(4), 728-734. Available at: https://doi.org/ 10.1111/bjd.14529 ↑34, ↑35 Bonafè, M., Barbieri, M., Marchegiani, F., Olivieri, F., Ragno, E., Giampieri, C., Mugianesi, E., Centurelli, M., Franceschi, C. and Paolisso, G. (2003). Polymorphic variants of insulin-like growth factor I (IGF-I) receptor and phosphoinositide 3-kinase genes affect IGF-I plasma levels and human longevity: cues for an evolutionarily conserved mechanism of life span control. The Journal of Clinical Endocrinology & Metabolism, 88(7), 3299-3304. Available at: https://doi.org/10.1210/jc.2002-021810 ↑36 Oakley, R.H., Cidlowski, J.A. (2013). The Biology of the Glucocorticoid Receptor: New Signaling Mechanisms in Health and Disease. Journal of Allergy and Clinical Immunology. 132(5). 1033-1044. Available at: https://doi.org/10.1016/j.jaci.2013.09.007 ↑37 Kwack, M.H., Hamida, O.B., Moon, K.K., Kim, J.C., Sung, Y.K. (2022). Dexamethasone, a Synthetic Glucocorticoid, Induces the Activity of Androgen Receptor in Human Dermal Papilla Cells. Skin Pharmacology and Physiology. 35(5). 299-304. Available at: https://doi.org/10.1159/000525067 ↑38 Gasic, V., Zukic, B., Stankovic, B., Janic, D., Dokmanovic, L., Lazic, J., Krstovski, N., Dolzan, V., Jazbec, J., Pavlovic, S., Kotur, N. (2018). Pharmacogenomic Markers of Glucocorticoid Response in The Initial Phase of Remission Induction Therapy in Childhood Acute Lymphoblastic Leukemia. Radiology and Oncology. 52(3). 296-306. Available at: https://doi.org/10.2478/raon-2018-0034 ↑39 Gasic, V., Zukic, B., Stankovic, B., Janic, D., Dokmanovic, L., Lazic, J., Krstovski, N., Dolzan, V., Jazbec, J., Pavlovic, S., Kotur, N. (2018). Pharmacogenomic Markers of Glucocorticoid Response in The Initial Phase of Remission Induction Therapy in Childhood Acute Lymphoblastic Leukemia. Radiology and Oncology. 52(3). 296-306. Available at: https://doi.org/10.2478/raon-2018-0034 ↑40 Ricciotti, E., FitzGerald, G.A. (2011). Prostaglandins and Inflammation. Arteriosclerosis, Thrombosis, and Vascular Biology. 31(5). 986-1000. Available at: https://doi.org/10.1161/ATVBAHA.110.207449. ↑41 Sakurai, M., Higashide, T., Takahashi, M., Sugiyama, K. (2007). Association between Genetic Polymorphisms of the Prostaglandin F2ɑ Receptor Gene and Response to Latanoprost. Ophthalmology. 114(6). 1039-1045. Available at: https://doi.org/10.1016/j.ophtha.2007.03.025. ↑42 ↑4 Sakurai, M., Higashide, T., Takahashi, M., Sugiyama, K. (2007). Association between Genetic Polymorphisms of the Prostaglandin F2ɑ Receptor Gene and Response to Latanoprost. Ophthalmology. 114(6). 1039-1045. Available at: https://doi.org/10.1016/j.ophtha.2007.03.025. ↑43 Blume-Peytavi, U., Lonngors, S., Hillmann, K., Bartels, N.G. (2012). A Randomized, Double-Blind, Placebo-Controlled Pilot Study to Assess the Efficacy of a 24-Week Topical Treatment by Latanoprost 0.1% on Hair Growth and Pigmentation in Healthy Volunteers with Androgenetic Alopecia. Journal of the American Academy of Dermatology. 66(5). 797-800. Available at: https://doi.org/10.1016/j.jaad.2011.05.026. ↑44 Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). Prostaglandin D2 Inhibits Hair Growth and is Elevated in Bald Scalp of Men with Androgenetic Alopecia. Science Translational Medicine. 4(126). 1-21. Available at: https://doi.org/10.1126/scitranslmed.3003122 ↑45 Villareal-Villareal, C.D., Sinclair, R.D., Martinez-Jacobo, L., Garza-Rodriguez, V., Rodriguez-Leon, S.A., Lamadrid-Zertuche, A.C., Rodriguez-Gutierrez, R., Ortiz-Lopez, R., Rojas-Martinez, A., Ocampo-Candiani, J. (2019). Prostaglandins in androgenetic alopecia in 12 men and four female. Journal of the European Academy of Dermatology and Venereology. 33(5). E214-e215. Available at: https://doi.org/10.1111/jdv.15479 ↑46 Frances, M.P., Vila-Vecilla, L., Russo, V., Polonini, H.C., de Souza, G.T. (2024). Utilizing SNP Association Analysis as a Prospective Approach for Personalising Androgenetic Alopecia Treatment. Dermatology and Therapy (Heidelb). 14(4). 971-981. Available at: https://doi.org/10.1007/s13555-024-01145-y ↑47 Chovarda, E., Sotiriou, E., Lazaridoi, E., Vakirlis, E., Ioannides, D. (2021). The Role of Prostaglandins in Androgenetic Alopecia. International Journal of Dermatology. 60. 730-735. Available at: https://doi.org/10.1111/ijd.15378 ↑48 Michelet, J.F., Commo, S., Billoni, N., Mahe, Y.F., Bernard, B.A. (1997). Activation of cytoprotective prostaglandin synthase-1 by minoxidil as a possible explanation for its hair growth-stimulating effect. Journal of Investigative Dermatology. 108(2). 205-209. Available at: https://doi.org/10.1111/1523-1747.ep12334249 ↑49 Scaglione, A., Montemiglio, L.C., Parisi, G., Asteriti, I.A., Bruni, R., Cerutti, G., Testi, C., Savino, C., Mancia, F., Lavia, P. and Vallone, B. (2017). Subcellular localization of the five members of the human steroid 5α-reductase family. Biochimie open, 4, 99-106. Available at: https://doi.org/10.1016/j.biopen.2017.03.003 ↑50 Rhie, A., Son, H.Y., Kwak, S.J., Lee, S., Kim, D.Y., Lew, B.L., Sim, W.Y., Seo, J.S., Kwon, O., Kim, J.I. and Jo, S.J. (2019). Genetic variations associated with response to dutasteride in the treatment of male subjects with androgenetic alopecia. Plos one, 14(9), e0222533. Available at: https://doi.org/10.1371/journal.pone.0222533 ↑51 Makridakis, N.M., di Salle, E., and Reichardt, J.K. (2000). Biochemical and pharmacogenetic dissection of human steroid 5α-reductase type II. Pharmacogenetics and Genomics, 10(5), 407-413. Available at: https://doi.org/10.1097/00008571-200007000-00004 ↑52 Goren, A., Castano, J.A., McCoy, J., Bermudez, F., Lotti, T. (2014). Novel enzymatic assay predicts minoxidil response in the treatment of androgenetic alopecia. Dermatologic Therapy. 27. 171-173. Available at: https://doi.org/10.1111/dth.12111 ↑53 Raghad, N.A., Al-Gazally, M.E., Ewahd, W.A. (2017). Assessment the effect of different genotypes of sulfotransferase 1A1 gene on the response to minoxidil in patients with androgenic alopecia. Journal of Global Pharma Technology. 10(9). 144-149 ↑54 Raghad, N.A., Al-Gazally, M.E., Ewahd, W.A. (2017). Assessment the effect of different genotypes of sulfotransferase 1A1 gene on the response to minoxidil in patients with androgenic alopecia. Journal of Global Pharma Technology. 10(9). 144-149 ↑55 Ramos, P.M., Gohad, P., McCoy, J., Wambier, C., Goren, A. (2021). Minoxidil Sulfotransferase Enzyme (SULT1A1) genetic variants predict response to oral minoxidil treatment for female pattern hair loss. Journal of the European Academy of Dermatology and Venererology. 35(1). E24-e26. Available at: https://doi.org/10.1111/jdv.16765 Progesterone is a steroid hormone with a wide range of physiological and medical effects. It is linked to female fertility and pregnancy, and it plays roles in neuro- and immunoprotection and various gynecological treatments. Studies have linked changes in progesterone levels to androgenic alopecia and postpartum telogen effluvium. Still, mixed evidence, limited research, and potential side effects have led to this treatment not being widely adopted.
In this article, we will explore the association between progesterone and hair loss, particularly female pattern hair loss (FPHL), and determine whether supplementation with progesterone can improve hair loss outcomes.
Key Takeaways
- What Is It? Progesterone is a steroid hormone that is essential for a wide range of physiological processes. Deficiencies are associated with menstrual irregularities, fertility and pregnancy issues, mood and sleep disturbance, and physical symptoms. Other signs can include dry skin and thinning hair.
- Evidence Quality: The evidence quality is 31/100 based on our metrics.
- Clinical Data: There is very limited evidence supporting using progesterone to improve hair loss outcomes.
- Study 1: 10 male patients with AGA were treated with a lotion containing 11a-hydroxyprogesterone. Improvements were observed in the “cranial” region of the scalp but not the left temporal region.
- Study 2: 6 male patients with AGA were treated with 100 mg of progesterone for 6 months. Improvements were observed in new hair growth and the transition from vellus to terminal hairs.
- Dosing & Formulation Considerations: Know your progestins! Many synthetic progesterone formulations are actually androgenic in nature rather than anti-androgenic. While some have more recently been developed to behave more closely to natural progesterone, there is data lacking in their efficacy to improve hair regrowth. We recommend sticking with natural progesterone until further research is available. If you are using natural progesterone, micronized allows for better systemic absorption especially when taken orally. It is typically prescribed at 200 mg daily for 12 days per 28-day cycle. However, it has not been tested for hair loss. If you decide to use non-micronized progesterone, a topical formulation may be more beneficial as oral is heavily metabolized and, therefore, may not reach the strength needed to affect hair growth outcomes. If you decide to take synthetic progestins, you might find results with cyproterone acetate or drospirenone (Slynd); however, once again, data is limited.
All-Natural Hair Supplement + Topical
The top natural ingredients for hair growth, all in one serum & supplement.
Take the next step in your hair growth journey with a world-class natural serum & supplement. Ingredients, doses, & concentrations built by science.
What Is Progesterone?
Progesterone is an important steroid hormone that plays several key roles in the female reproductive system. It is primarily produced by the corpus luteum in the ovaries after ovulation in women. For men, progesterone is produced in smaller amounts by the adrenal glands and is associated with sperm development.[1]Nio-Kobayashi, J., Miyazaki, K., Hashiba, K., Okuda, K., Iwanaga, T. (2016). Histological analysis of arteriovenous anastomosis-like vessels established in the corpus luteum of cows during … Continue reading,[2]Mirihagelle, S., Hughes, J.R., Miller, D.J. (2022). Progesterone-induced sperm release from the oviduct sperm reservoir. Cells. 11(10). 1622. Available at: https://doi.org/10.3390/cells11101622

Figure 1. Progesterone molecule.
The association between progesterone and hair health is multifaceted, involving direct hormonal effects and indirect influences.
Studies have shown that progesterone, due to its 5-alpha-reductase (5-AR) inhibiting properties, can help balance the potentially negative effects of androgens like testosterone. When progesterone levels decline, increased conversion of testosterone to dihydrotestosterone by 5-AR can occur, leading to hair follicle miniaturization and hair thinning.[3]Grymowicz, M., Rudnicka, E., Podfigurna, A., Napierała, P., Smolarczyk, R., Smolarczyk, K., Męczekalski, B. (2020). Hormonal effects on hair follicles. International Journal of Molecular Sciences. … Continue reading
Significant hormonal changes occur in menopausal women, including a decrease in estrogen and progesterone levels. Estrogen prolongs the growing (anagen) phase of the hair follicle cycle, and progesterone indirectly supports this through its androgen-inhibiting activity. Therefore, a reduction in both estrogen and progesterone can leave menopausal women vulnerable to increased androgen levels and subsequent hair loss.
Changes in progesterone levels can also affect postpartum women. During pregnancy, progesterone levels are significantly elevated but drop sharply after childbirth. This sudden decrease in progesterone and estrogen is believed to contribute to postpartum telogen effluvium (PPTE). However, unlike the other examples mentioned above, PPTE is generally self-limiting. It occurs 2-4 months after delivery and resolves typically within 6-24 weeks (although in rare cases, it can persist up to 15 months).[4]Cleveland Clinic. (no date). Postpartum Hair Loss. Cleveland Clinic. Available at: https://my.clevelandclinic.org/health/diseases/23297-postpartum-hair-loss (Accessed: September 2024)
So, we know how progesterone deficits might lead to hair loss, but does progesterone supplementation improve hair loss outcomes?
Can Progesterone Improve Hair Loss Outcomes?
As previously mentioned, progesterone has some 5-AR inhibitory properties. However, there is limited evidence to show that it can improve hair loss outcomes.
One 1987 study treated ten male patients with AGA with a lotion containing 1% 11a-hydroxyprogesterone (a progesterone derivative) for one year, and 8 patients were treated with a control.[5]Van der Willigen, A.H., Peereboom-Wynia, J.D.R., van Joost, TH., Stolz, E. (1987). A preliminary study of the effect of 11a hydroxyprogesterone on hair growth in men suffering from androgenetic … Continue reading Those treated with the progesterone derivative showed an increase in the number of anagen hairs (45 to 51) and mean hair shaft diameter (69.6 μm to 71.6 μm) in the “cranial” region of the scalp. Further improvements were seen with reduced regressing/non-growing (catagen/telogen) hairs (46-40). Unfortunately, without images, we can’t see if these improvements led to a clinically significant outcome.
Furthermore, the study also analyzed hair counts on the left temporal side of the scalp. Here, the number of anagen hairs reduced from 67 to 62, and the number of catagen/telogen hairs increased from 21 to 30, indicating a varied response to the treatment.

Figure 2: Hair counts after topical application of a progesterone derivative.[6]Van der Willigen, A.H., Peereboom-Wynia, J.D.R., van Joost, TH., Stolz, E. (1987). A preliminary study of the effect of 11a hydroxyprogesterone on hair growth in men suffering from androgenetic … Continue reading
Another small study was conducted with 6 males with AGA, acne, and benign prostatic hyperplasia (BPH).[7]Kalinchenko, S., Nikiforov, I., Samburskaya, O. (2022). BPH, Androgenic Alopecia, and Acne – Markers of Progesterone Deficiency. Journal of the Endocrine Society. 6. 431-432. Available at: … Continue reading The participants were treated with Vitamin D and 100 mg progesterone daily for 6 months. After this period, the authors reported that the patients had reduced hair loss, new hair growth, and increased vellus transition to terminal hairs. Unfortunately, the authors didn’t report the specific values or show any photos. Furthermore, it is not possible to know if the positive effects were due to supplementing with Vitamin D.
While there is a logical reasoning behind the use of progesterone for women undergoing menopause suffering from female pattern hair loss, there is no clinical evidence demonstrating its efficacy.
Progesterone Formulations
There are a number of formulations of progesterone, but how effective might they be at improving hair loss outcomes?
Oral
Oral progesterone is typically prescribed for hormone replacement therapy (HRT). However, due to its metabolism, oral progesterone may only have limited benefits for hair loss. It undergoes extensive first-pass metabolism in the liver, leading to significant degradation of the hormone before it reaches the systemic circulation, meaning that limited amounts of the hormone may reach the scalp.[8]Coombes, Z., Plant, K., Freire, C., Basit, A.W., Butler, P., Conlan, R.S., Gonzalez, D. (2021). Progesterone metabolism by human and rat hepatic and intestinal tissue. Pharmaceutics. 13(10). 1707. … Continue reading
Topical
Topical progesterone has a few potential benefits, including:
- Localized application
- Fewer systemic side effects
- Bypass first pass metabolism, so more is reaching the target area
According to one source, the most common strength of progesterone applied topically is around 2%. However, this appears to be based on clinical experience rather than published studies.[9]Roseway Labs. (2020). Topicals for Hair Loss. Roseway Labs. Available at: https://rosewaylabs.com/topicals-for-hair-loss/ (Accessed: September 2024)
Injection
While some clinics use injected progesterone combined with other treatments, like platelet-rich plasma (you can find videos of these if you search on YouTube) to treat hair thinning, there is no peer-reviewed, published clinical evidence to suggest that it improves hair loss outcomes.
Micronized
Recently, there has been interest in using micronized progesterone and its potential as a hair growth treatment. This formulation may offer improved absorption and efficacy in balancing hormone levels, potentially aiding hair growth.
Micronized progesterone is a formulation of progesterone that has been processed to create very small particles smaller than 10 μm in size. This process increases the surface area of progesterone particles, allowing for better systemic absorption, especially when taken orally.[10]Hargrove, J.T., Maxson, W.S., Wentz, A.C. (1989). Absorption of oral progesterone is influenced by vehicle and particle size. American Journal of Obstetrics and Gynecology. 161(4). 948-951. Available … Continue reading
Micronized progesterone is chemically identical to the progesterone that is naturally produced in the human body, meaning it should work similarly.[11]de Lignieres, B. (1999). Oral micronized progesterone. Clinical Therapeutics. 21(1). 41-60. Available at: https://doi.org/10.1016/S0149-2917(00)88267-3 It is currently used as an HRT for menopausal symptoms, to support pregnancy and fertility, and to treat gynecological disorders.[12]Memi, E., Pavli, P., Papagianni, M., Vrachnis, N., Mastorakos, G. (2024). Diagnostic and therapeutic use of oral micronized progesterone in endocrinology. Reviews in endocrine and metabolic … Continue reading
While we have recently been getting a lot of emails from members about micronized progesterone, there is a significant gap in the literature about its potential efficacy in treating hair loss in menopausal women or people with AGA.
Synthetic Progesterone
We have discussed natural progesterone in-depth, so let’s also examine synthetic progesterone (progestins) and how it differs from natural progesterone.
Progestins differ from natural progesterone in their chemical structure, which results in different physiological effects. Some common synthetic progestins include norethindrone, medroxyprogesterone acetate (MPA), norethisterone (NET-A), and levonorgestrel. Unlike natural progesterone, many synthetic progestins can increase androgen activity. This is critical to keep in mind when choosing whether to take progestins if you suffer from hair loss. Furthermore, progestins can cause other unwanted side effects like acne, excessive hair growth in unwanted areas, and changes in skin texture, alongside more serious increased risks such as cardiovascular events (heart attacks and strokes) and cancers.
One study published in 2017 examined the androgenic and estrogenic properties of various progestins, including MPA and NET-A. The findings indicated that these progestins bind to the androgen receptor (AR) with affinities comparable to dihydrotestosterone (DHT), suggesting that they can exert androgenic effects in vivo (in cells).[13]Louw-du Toit, R., Perkins, M.S., Hapgood, J.P., Africander, D. (2017). Comparing the androgenic and estrogenic properties of progestins used in contraception and hormone therapy. Biochemical and … Continue reading
Research on hormonal contraceptives highlighted that synthetic progestins can lead to hair loss. One review conducted on data on alopecia associated with the levonorgestrel IUD found a number of women who had the IUD implanted between 2000-2001 experienced hair loss. Furthermore, in some of these cases, when the IUD was removed, women recovered their hair loss, indicating a direct effect of levonorgestrel on hair loss for some people. Unfortunately, this study is limited in many ways, including being a retrospective study and only having 73 total reports of alopecia (in New Zealand and using World Health Organization data).[14]Paterson, H., Clifton, J., Miller, D., Ashton, J., Harrison-Woolrych, M. (2007(. Hair loss with use of the levonorgestrel intrauterine device. Contraception 76. 306-309. Available at: … Continue reading
A case study from 2002, this time conducted on a woman taking a combination low-dose oral contraceptive (norethindrone and ethinyl estradiol), found shortly after starting, she experienced hair loss, which abated when stopped.[15]Yokoyama, Y., Sato, S., Saito, Y. (2002). Alopecia related to low-dose oral contraceptives. Archives of Gynecology and Obstetrics. 47. 266-246. Available at: https://doi.org/10.1007/pl00007489
So, it seems like if you have AGA, you might want to avoid synthetic progestins. But are there exceptions to the rule? There might be.
Cyproterone Acetate
While cyproterone acetate is a progestin, it has shown potential in improving hair regrowth in women with androgenic alopecia. In a study involving 80 women with FPHL treated with either 200 mg spironolactone, 50 mg of cyproterone acetate, or 100 mg daily for 10 days per month if menopausal, 44% of those treated with cyproterone acetate experienced hair regrowth. However, another 44% saw no change, and 12% continued to lose hair. There was also no significant difference between the cyproterone acetate and spironolactone groups.[16]Sinclair, R., Wewerinke, M., Jolley, D. (2005). Treatment of female pattern hair loss with oral antiandrogens. British Journal of Dermatology. 152(3). 466-473. Available at: … Continue reading
Another study reported that 77.1% of 35 women with androgenic alopecia observed hair regrowth after three months of treatment with the combined cyproterone acetate and ethinyl estradiol pill (2mg). 42.8% of participants had slight regrowth, 34.3% had moderate regrowth after trichoscopic assessment, and 22.8% showed no regrowth at all.[17]Coneac, A., Muresan, A., Orasan, M.S. (2014). Antiandrogenic therapy with ciproterone acetate in female patients who suffer from both androgenic alopecia and acne vulgaris. Clujul Medical. 87(4). … Continue reading

Figure 3. Effect of cyproterone acetate on hair regrowth. [18]Coneac, A., Muresan, A., Orasan, M.S. (2014). Antiandrogenic therapy with ciproterone acetate in female patients who suffer from both androgenic alopecia and acne vulgaris. Clujul Medical. 87(4). … Continue reading
A 12-month randomized trial found that cyproterone acetate was more effective than minoxidil at treating hair loss in women with signs of hyperandrogenism, which may be worth considering when considering hair loss treatments.[19]Vexiau, P., Chaspoux, C., Boudou, P., Fiet, J., Jouanique, C., Hardy, N., Reygagne, P. (2002). Effects of minoxidil 2% vs. cyproterone acetate treatment on female androgenetic alopecia: a controlled, … Continue reading
Drospirenone
Drospirenone (also known under the brand name Slynd) is a newer synthetic progesterone that has a unique profile. It is derived from spironolactone, a drug you may be familiar with, as it also has anti-androgenic properties. Like cyproterone acetate, Slynd does not increase androgenic activity. Instead, it has androgenic properties similar to natural progesterone, which makes it an attractive potential treatment.[20]Regidor, P.A., Mueller, A., Mayr, M. (2023). Pharmacological and metabolic effects of drospirenone as a progestin-only pill compared to combined formulations with estrogen. Womens Health (Lond). 19. … Continue reading
However, the data on hair loss is limited. One study evaluated the efficacy of oral finasteride therapy combined with an oral contraceptive containing drosperinone and ethinyl estradiol in premenopausal women with FPHL. The study found that 62% of patients showed some improvement in hair loss, but it was unclear whether the improvement was due to the higher dosage of finasteride or the combination with the oral contraceptive.[21]Iorizzo, M., Vincenzi, C., Voudouris, S., Piraccini, B.M., Tosti, A. (2006). Finasteride treatment of female pattern hair loss. Archives of Dermatology. 142(3). 298-302. Available at: … Continue reading
Furthermore, if you are sensitive or respond poorly to spironolactone, you might also experience side effects with Slynd. Another factor is that as a synthetic progestin, it might also carry elevated cardiovascular and cancer risks.
Other “new” progestins have also been developed and designed to be closer in mechanism of action to progesterone than other synthetics. These are dienogest, nestorone, nomegestrol acetate, and trimegestone, which have anti-androgenic activity, that may benefit those with hair loss, but again, they haven’t been tested.[22]Sitruk-Ware, R. (2006). New progestagens for contraceptive use. Human Reproduction Update. 12(2). 169-178. Available at: https://doi.org/10.1093/humupd/dmi046
Dosing Considerations
Oral micronized progesterone is typically prescribed at 200 mg daily for 12 days per 28-day cycle for postmenopausal women or 400 mg daily for 10 days for women who have not had a period for at least three consecutive months.[23]Memi, E., Pavli, P., Papagianni, M., Vrachnis, N., Mastorakos, G. (2024). Diagnostic and therapeutic use of oral micronized progesterone in endocrinology. Reviews in endocrine and metabolic … Continue reading It may be beneficial for women with female pattern hair loss.
Topical progesterone creams are often used in doses ranging from 20 to 40 mg, applied once or twice daily. For example, one study conducted with post-menopausal women used 40 mg daily or 20 mg twice daily for 42 days.[24]Carey, B.J., Carey, A.H., Patel, S., Carter, G., Studd, J.W. (2000). A study to evaluate serum and urinary hormone levels following short and long term administration of two regimens of progesterone … Continue reading
Injectable progesterone is injected primarily at around 150 mg every 12 weeks.[25]Nelson, A., (2002). Merits of DMPA relative to other reversible contraceptive methods. Journal of Reproductive Medicine. 47(9). 781-784. PMID: 12380406
Based on the research above, the dose for cyproterone acetate is around 50 – 100 mg, but this was given with ethinyl estradiol. For Slynd, the standard contraceptive dose of 4 mg orally once daily for 24 days followed by 4 inactive days may have potential benefits.
Dosing should be individualized based on the patient’s age, health status, and specific hormonal imbalances. Patients should report any concerning side effects to their doctor straight away. Close monitoring and adjustment of dosage by a healthcare provider are important, as effects can vary between individuals.
Best Practices
- Premenopausal Women: Progesterone supplementation may be used to address hormonal imbalances contributing to hair thinning.
- Postmenopausal Women: HRT with progesterone is more common, particularly in combination with estrogen, to combat hair loss linked to reduced hormone levels during menopause.
- Individuals with Androgenic Hair Loss: Progesterone as an adjunct to other anti-androgen therapies (e.g., spironolactone) for hair loss management (if you are pre-menopausal).[26]Brough, K.R., Torgerson, R.R. (2017). Hormonal therapy in female pattern hair loss. International Journal of Women’s Dermatology. 3. 53-57. Available at: … Continue reading
- Key Considerations: Before starting progesterone therapy, it is important to undergo individualized hormone testing and consult with a healthcare provider. Monitor for side effects such as mood changes, weight gain, or changes in menstrual patterns
Ultimately, due to the lack of evidence, we believe that steering clear of synthetic progestins, for the most part, would be best until newer data comes out supporting their use in hair growth. As it stands there may be some promising candidates, but its clear from our research that there is a gap in the evidence.
Final Thoughts
While progesterone, particularly in topical and micronized formulations, may benefit women suffering from FPHL or other hormonally influenced hair loss, more high-quality research is needed. If you are thinking about using progesterone, consult with your doctor or healthcare professional to ensure that it is tailored to your needs.
References[+]
References ↑1 Nio-Kobayashi, J., Miyazaki, K., Hashiba, K., Okuda, K., Iwanaga, T. (2016). Histological analysis of arteriovenous anastomosis-like vessels established in the corpus luteum of cows during luteolysis. Journal of Ovarian Research. 9(67). 1-14. Available at: https://doi.org/10.1186/s13048-016-0277-0 ↑2 Mirihagelle, S., Hughes, J.R., Miller, D.J. (2022). Progesterone-induced sperm release from the oviduct sperm reservoir. Cells. 11(10). 1622. Available at: https://doi.org/10.3390/cells11101622 ↑3 Grymowicz, M., Rudnicka, E., Podfigurna, A., Napierała, P., Smolarczyk, R., Smolarczyk, K., Męczekalski, B. (2020). Hormonal effects on hair follicles. International Journal of Molecular Sciences. 21(15). 5342. Available at: https://doi.org/10.3390/ijms21155342 ↑4 Cleveland Clinic. (no date). Postpartum Hair Loss. Cleveland Clinic. Available at: https://my.clevelandclinic.org/health/diseases/23297-postpartum-hair-loss (Accessed: September 2024) ↑5, ↑6 Van der Willigen, A.H., Peereboom-Wynia, J.D.R., van Joost, TH., Stolz, E. (1987). A preliminary study of the effect of 11a hydroxyprogesterone on hair growth in men suffering from androgenetic alopecia. Acta dermato-venereologica. 67(1). 82-85. PMID: 2436423 ↑7 Kalinchenko, S., Nikiforov, I., Samburskaya, O. (2022). BPH, Androgenic Alopecia, and Acne – Markers of Progesterone Deficiency. Journal of the Endocrine Society. 6. 431-432. Available at: https://doi.org/10.1210/jendso/bvac150 ↑8 Coombes, Z., Plant, K., Freire, C., Basit, A.W., Butler, P., Conlan, R.S., Gonzalez, D. (2021). Progesterone metabolism by human and rat hepatic and intestinal tissue. Pharmaceutics. 13(10). 1707. Available at: https://doi.org/10.3390/pharmaceutics13101707 ↑9 Roseway Labs. (2020). Topicals for Hair Loss. Roseway Labs. Available at: https://rosewaylabs.com/topicals-for-hair-loss/ (Accessed: September 2024) ↑10 Hargrove, J.T., Maxson, W.S., Wentz, A.C. (1989). Absorption of oral progesterone is influenced by vehicle and particle size. American Journal of Obstetrics and Gynecology. 161(4). 948-951. Available at: https://doi.org/10.1016/0002-9378(89)90759-x ↑11 de Lignieres, B. (1999). Oral micronized progesterone. Clinical Therapeutics. 21(1). 41-60. Available at: https://doi.org/10.1016/S0149-2917(00)88267-3 ↑12, ↑23 Memi, E., Pavli, P., Papagianni, M., Vrachnis, N., Mastorakos, G. (2024). Diagnostic and therapeutic use of oral micronized progesterone in endocrinology. Reviews in endocrine and metabolic disorders. 25(4). 751-772. Available at: https://doi.org/10.1007/s11154-024-09882-0 ↑13 Louw-du Toit, R., Perkins, M.S., Hapgood, J.P., Africander, D. (2017). Comparing the androgenic and estrogenic properties of progestins used in contraception and hormone therapy. Biochemical and Biophysical Research Communications. (491)1. 140-146. Available at: https://doi.org/10.1016/j.bbrc.2017.07.063 ↑14 Paterson, H., Clifton, J., Miller, D., Ashton, J., Harrison-Woolrych, M. (2007(. Hair loss with use of the levonorgestrel intrauterine device. Contraception 76. 306-309. Available at: https://doi.org/10.1016/j.contraception.2007.06.015 ↑15 Yokoyama, Y., Sato, S., Saito, Y. (2002). Alopecia related to low-dose oral contraceptives. Archives of Gynecology and Obstetrics. 47. 266-246. Available at: https://doi.org/10.1007/pl00007489 ↑16 Sinclair, R., Wewerinke, M., Jolley, D. (2005). Treatment of female pattern hair loss with oral antiandrogens. British Journal of Dermatology. 152(3). 466-473. Available at: https://doi.org/10.1111/j.1365-2133.2005.06218.x ↑17 Coneac, A., Muresan, A., Orasan, M.S. (2014). Antiandrogenic therapy with ciproterone acetate in female patients who suffer from both androgenic alopecia and acne vulgaris. Clujul Medical. 87(4). 226-234. Available at: https://doi.org/10.15386/cjmed-386 ↑18 Coneac, A., Muresan, A., Orasan, M.S. (2014). Antiandrogenic therapy with ciproterone acetate in female patients who suffer from both androgenic alopecia and acne vulgaris. Clujul Medical. 87(4). 226-234. Available at: https://doi.org/10.15386/cjmed-386 ↑19 Vexiau, P., Chaspoux, C., Boudou, P., Fiet, J., Jouanique, C., Hardy, N., Reygagne, P. (2002). Effects of minoxidil 2% vs. cyproterone acetate treatment on female androgenetic alopecia: a controlled, 12-month randomized trial. British Journal of Dermatology. 146(6). 992-999. Available at: https//doi.org/10.1046/j.1365-2133.2002.04798.x ↑20 Regidor, P.A., Mueller, A., Mayr, M. (2023). Pharmacological and metabolic effects of drospirenone as a progestin-only pill compared to combined formulations with estrogen. Womens Health (Lond). 19. 1-10. Available at: https://doi.org/10.1177/17455057221147388 ↑21 Iorizzo, M., Vincenzi, C., Voudouris, S., Piraccini, B.M., Tosti, A. (2006). Finasteride treatment of female pattern hair loss. Archives of Dermatology. 142(3). 298-302. Available at: https://doi.org/10.1001/archderm.142.3.298 ↑22 Sitruk-Ware, R. (2006). New progestagens for contraceptive use. Human Reproduction Update. 12(2). 169-178. Available at: https://doi.org/10.1093/humupd/dmi046 ↑24 Carey, B.J., Carey, A.H., Patel, S., Carter, G., Studd, J.W. (2000). A study to evaluate serum and urinary hormone levels following short and long term administration of two regimens of progesterone creams in postmenopausal women. BJOG. 107(6). 722-726. Available at: https://doi.org/10.1111/j.1471-0528.2000.tb13331.x ↑25 Nelson, A., (2002). Merits of DMPA relative to other reversible contraceptive methods. Journal of Reproductive Medicine. 47(9). 781-784. PMID: 12380406 ↑26 Brough, K.R., Torgerson, R.R. (2017). Hormonal therapy in female pattern hair loss. International Journal of Women’s Dermatology. 3. 53-57. Available at: https://doi.org/10.1016/j.ijwd.2017.01.001 CRABP2 is one of two genes found within the CRABP family alongside CRABP1. CRABP2 is a key regulator of retinoic acid, a vitamin A derivative, transporting it around the cell and helping its metabolism. Both CRABP2 and retinoic acid have been suggested in the literature to have roles in the maintenance of hair health. This is particularly evident for retinoic acid, which has been suggested to regulate hair health in a dose-dependent manner. A few studies have also investigated genetic variation in CRABP2, suggesting that some variants may be linked to hair loss. This article will explore how relevant CRABP2 is to hair loss treatment effectiveness and how to interpret your genetic results to make the correct treatment choice.
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is CRABP2?
The cellular retinoic acid binding protein (CRABP) gene family is very small, consisting of just two members – cellular retinoic acid binding protein 1 (CRABP1) and cellular retinoic acid binding protein 2 (CRABP2). CRABP1 is expressed throughout the body, whereas CRABP2 expression is restricted to certain tissues, such as the skin. Both CRABP genes are high-affinity binding proteins of retinoic acid, which is a derivative of vitamin A. Although research has yet to fully elucidate their exact functions, it is understood that CRABP1 and CRABP2 both play a role in the transport and metabolism of retinoic acid.[1]Wei, L. N. (2016). Cellular retinoic acid binding proteins: Genomic and non-genomic functions and their regulation. The Biochemistry of Retinoid Signaling II: The Physiology of Vitamin A-Uptake, … Continue reading
In sheep, it has been shown that CRABP2 is highly expressed in dermal papilla cells (DPCs), which play a key role in the growth and development of hair follicles. Moreover, they showed that CRABP2 regulates the proliferation of DPCs and that the overexpression of CRABP2 promoted increased DPC proliferation. Although this research was conducted in cells taken from sheep, it does suggest that CRABP2 may play a role in the maintenance of hair.[2]He, M., Lv, X., Cao, X., Yuan, Z., Quan, K., Getachew, T., Mwacharo, J.M., Haile, A., Li, Y., Wang, S. and Sun, W. (2023). CRABP2 Promotes the Proliferation of Dermal Papilla Cells via the … Continue reading
These results suggest that increased expression of CRABP2 could be beneficial for hair loss. However, the association between CRABP2 and hair maintenance is slightly more complex than it first appears. In tissue taken from a mouse model of alopecia areata (AA), the expression of CRABP2 (both the gene and protein) was increased compared to control mice. Similarly, CRABP2 protein expression was higher in tissue taken from humans with AA. Ultimately, the findings of the paper suggest that increased retinoic acid synthesis may contribute to the pathogenesis of AA.[3]Duncan, F.J., Silva, K.A., Johnson, C.J., King, B.L., Szatkiewicz, J.P., Kamdar, S.P., Ong, D.E., Napoli, J.L., Wang, J., King Jr, L.E. and Whiting, D.A. (2013). Endogenous retinoids in the … Continue reading
Conversely, it has also been shown that a reduction in retinoic acid signaling may be associated with hair loss. Mice lacking a key retinoic acid receptor exhibited impaired anagen initiation within their hair follicles (the growing phase), which was likely a contributory factor in the progressive alopecia that these mice developed.[4]Li, M., Chiba, H., Warot, X., Messaddeq, N., Gérard, C., Chambon, P., & Metzger, D. (2001). RXRα ablation in skin keratinocytes results in alopecia and epidermal alterations. Development, … Continue reading
Further evidence has been added to support these findings, suggesting that retinoic acid signaling may contribute to AGA similarly to androgens. It is widely accepted that androgens drive the pathogenesis of AGA and lead to the miniaturization of hair follicles. However, a study conducted in 30 male patients with AGA revealed that genes involved in retinoic acid signaling are upregulated, suggesting that retinoic acid signaling may promote follicle miniaturization.[5]Ho, B.S.Y., Vaz, C., Ramasamy, S., Chew, E.G.Y., Mohamed, J.S., Jaffar, H., Hillmer, A., Tanavde, V., Bigliardi-Qi, M. and Bigliardi, P.L. (2019). Progressive expression of PPARGC1α is associated … Continue reading
Despite appearing contradictory, it is possible that all of these studies are accurate and that both a deficiency and excess of retinoic acid can contribute to hair loss. Indeed, the literature suggests that retinoic acid may regulate hair health in a dose-dependent manner, whereby the optimal and ‘healthy’ level of retinoic acid sits somewhere between low and high.[6]VanBuren, C. A., & Everts, H. B. (2022). Vitamin A in skin and hair: an update. Nutrients, 14(14), 2952. Available at: https://doi.org/10.3390/nu14142952
This leads to a somewhat paradoxical situation, as retinoic acid is necessary for hair growth, but it can also cause hair loss when present in high concentrations. Thus, the therapeutic use of retinoic acid in treating hair loss is a challenging prospect.[7]Sadgrove, N. J., & Simmonds, M. S. (2021). Topical and nutricosmetic products for healthy hair and dermal antiaging using “dual‐acting”(2 for 1) plant‐based peptides, hormones, and … Continue reading
That said, several studies have shown that the application of tretinoin, a type of retinoic acid, has beneficial effects in treating hair loss. One study was conducted on 56 patients with AGA, who were treated with either a placebo, 0.5% minoxidil, 0.025% tretinoin, or a combination of minoxidil and tretinoin.[8]Bazzano, G. S., Terezakis, N., & Galen, W. (1986). Topical tretinoin for hair growth promotion. Journal of the American Academy of Dermatology, 15(4), 880-893. Available at: … Continue reading Tretinoin treatment alone was shown to stimulate some hair regrowth in more than half of the patients who received the treatment. Further positive results were observed with combination treatment.

Figure 1: Level of hair regrowth after treatment with either a placebo, minoxidil (0.5%), tretinoin (0.025%), or a combination of tretinoin and minoxidil.[9]Bazzano, G. S., Terezakis, N., & Galen, W. (1986). Topical tretinoin for hair growth promotion. Journal of the American Academy of Dermatology, 15(4), 880-893. Available at: … Continue reading
This was also shown in a study conducted on 31 male patients with AGA. The study showed that once-daily application of tretinoin and minoxidil, in combination, was as effective at treating hair loss as twice-daily minoxidil on its own (Figure 1).[10]Shin, H. S., Won, C. H., Lee, S. H., Kwon, O. S., Kim, K. H., & Eun, H. C. (2007). Efficacy of 5% minoxidil versus combined 5% minoxidil and 0.01% tretinoin for male pattern hair loss: a … Continue reading

Figure 2: The effect of combined minoxidil and tretinoin or minoxidil alone on hair growth parameters.[11]Shin, H. S., Won, C. H., Lee, S. H., Kwon, O. S., Kim, K. H., & Eun, H. C. (2007). Efficacy of 5% minoxidil versus combined 5% minoxidil and 0.01% tretinoin for male pattern hair loss: a … Continue reading
What is the Evidence for Targeting CRABP2 for Hair Loss?
Collectively, the evidence does suggest that CRABP2 and retinoic acid are key factors in hair loss. Owing to this, it is feasible that genetic variation in CRABP2 could influence the efficacy of hair loss treatments.
In a study conducted on newborn babies, it was found that the rs12724719 polymorphism was linked to retinoic acid levels. Specifically, those with the AA genotype had a greater concentration of retinoic acid in the blood of their umbilical cord than those with the GA or GG genotypes. It is believed that such an increase in retinoic acid may have been caused by reduced CRABP2 expression, impairing its ability to transport retinoic acid into the nucleus of the cell.[12]Manolescu, D. C., El-Kares, R., Lakhal-Chaieb, L., Montpetit, A., Bhat, P. V., & Goodyer, P. (2010). Newborn serum retinoic acid level is associated with variants of genes in the retinol … Continue reading
Although this study was conducted in newborn umbilical cord blood, and so is probably not representative of how the genetic variant affects adults or hair, the results are still interesting. If adults with the AA genotype also exhibit increased levels of retinoic acid, then therapeutic supplementation with retinoic acid to treat hair loss may be less effective in those individuals. Moreover, given that retinoic acid levels are already high, increasing levels further may increase the risk of those individuals experiencing retinoic acid-induced hair loss, as discussed earlier.
A separate study was conducted on over 25,000 patients with AGA, a mix of both males and females. Interestingly, their analysis revealed an association between the rs12724719 polymorphism and AGA. Unfortunately, the authors did not specifically state which of the genotypes were linked to AGA and which were not. However, this is yet another indication that genetic variation in CRABP2 and the rs12724719 polymorphism may influence hair health and treatments.[13]Francès, M. P., Vila-Vecilla, L., Russo, V., Caetano Polonini, H., & de Souza, G. T. (2024). Utilising SNP Association Analysis as a Prospective Approach for Personalising Androgenetic Alopecia … Continue reading
What Do Your Genetic Results Mean?
Your Result CRABP2 (rs12724719)
Variant 1 – GG genotype
Variant 2 – GA genotype Variant 3 – AA genotype
What it Means Associated with normal levels of retinoic acid in the blood Associated with normal levels of retinoic acid in the blood Associated with elevated levels of retinoic acid in the blood The Implication May benefit from retinoic acid supplementation May benefit from retinoic acid supplementation May not benefit from retinoic acid treatment (i.e, vitamin A supplementation or retinoid topicals) What Relevance Does CRABP2 Have for Hair Loss Treatment?
We have also created a rubric that helps to determine the relevance of a specific gene to hair loss based on the quality of the evidence in the above studies.
On a scale of 1-5, how important are these genetic results? (1 is the lowest, 5 is the highest)
This score is a rating based on evidence quality.
- Does this gene have any potential relevance for hair loss? (1 point)
Yes. CRABP2 has been found to be upregulated in patients with alopecia areata (score = 1)
- Does the totality of evidence implicate CRABP2 as a causal agent for hair loss? (1 point)
No. There is very little published literature that indicates CRABP2 causes hair loss. (score = 0)
- Does the totality of evidence implicate CRABP2 as a predictive factor for hair loss treatment responsiveness? (2 points)
No. There is no published literature that shows that CRABP2 polymorphisms affect hair loss treatments (score = 0)
- Is this quality of evidence on (3) strong enough to influence treatment recommendations? (1 point)
Since CRABP2 fails question #3, it cannot be awarded points for question #4 (score = 0)
Total Score = 1
Final Thoughts
While there is evidence that genetic variation in CRABP2 is associated with AGA and may affect retinoic acid levels, the evidence is not yet sufficient to make definitive treatment recommendations based solely on genotype. Importantly, no studies have yet explored how genetic variation in CRABP2 affects treatment with retinoic acid or any other therapeutic. Additional studies that seek to answer this question must be conducted to confirm the true predictive value of testing CRABP2 variants to personalize hair treatments.
References[+]
References ↑1 Wei, L. N. (2016). Cellular retinoic acid binding proteins: Genomic and non-genomic functions and their regulation. The Biochemistry of Retinoid Signaling II: The Physiology of Vitamin A-Uptake, Transport, Metabolism and Signaling, 163-178. Available at: https://doi.org/10.1007/978-94-024-0945-1_6 ↑2 He, M., Lv, X., Cao, X., Yuan, Z., Quan, K., Getachew, T., Mwacharo, J.M., Haile, A., Li, Y., Wang, S. and Sun, W. (2023). CRABP2 Promotes the Proliferation of Dermal Papilla Cells via the Wnt/β-Catenin Pathway. Animals, 13(12), 2033. Available at: https://doi.org/10.3390/ani13122033 ↑3 Duncan, F.J., Silva, K.A., Johnson, C.J., King, B.L., Szatkiewicz, J.P., Kamdar, S.P., Ong, D.E., Napoli, J.L., Wang, J., King Jr, L.E. and Whiting, D.A. (2013). Endogenous retinoids in the pathogenesis of alopecia areata. Journal of Investigative Dermatology, 133(2), 334-343. Available at: https://doi.org/10.1038/jid.2012.344 ↑4 Li, M., Chiba, H., Warot, X., Messaddeq, N., Gérard, C., Chambon, P., & Metzger, D. (2001). RXRα ablation in skin keratinocytes results in alopecia and epidermal alterations. Development, 128(5), 675-688. Available at: https://doi.org/10.1242/dev.128.5.675 ↑5 Ho, B.S.Y., Vaz, C., Ramasamy, S., Chew, E.G.Y., Mohamed, J.S., Jaffar, H., Hillmer, A., Tanavde, V., Bigliardi-Qi, M. and Bigliardi, P.L. (2019). Progressive expression of PPARGC1α is associated with hair miniaturization in androgenetic alopecia. Scientific reports, 9(1), 8771. Available at: https://doi.org/10.1038/s41598-019-43998-7 ↑6 VanBuren, C. A., & Everts, H. B. (2022). Vitamin A in skin and hair: an update. Nutrients, 14(14), 2952. Available at: https://doi.org/10.3390/nu14142952 ↑7 Sadgrove, N. J., & Simmonds, M. S. (2021). Topical and nutricosmetic products for healthy hair and dermal antiaging using “dual‐acting”(2 for 1) plant‐based peptides, hormones, and cannabinoids. FASEB BioAdvances, 3(8), 601. Available at: https://doi.org/10.1096/fba.2021-00022 ↑8, ↑9 Bazzano, G. S., Terezakis, N., & Galen, W. (1986). Topical tretinoin for hair growth promotion. Journal of the American Academy of Dermatology, 15(4), 880-893. Available at: https://doi.org/10.1016/S0190-9622(86)80024-X ↑10, ↑11 Shin, H. S., Won, C. H., Lee, S. H., Kwon, O. S., Kim, K. H., & Eun, H. C. (2007). Efficacy of 5% minoxidil versus combined 5% minoxidil and 0.01% tretinoin for male pattern hair loss: a randomized, double-blind, comparative clinical trial. American journal of clinical dermatology, 8, 285-290. Available at: https://doi.org/10.2165/00128071-200708050-00003 ↑12 Manolescu, D. C., El-Kares, R., Lakhal-Chaieb, L., Montpetit, A., Bhat, P. V., & Goodyer, P. (2010). Newborn serum retinoic acid level is associated with variants of genes in the retinol metabolism pathway. Pediatric research, 67(6), 598-602. Available at: https://doi.org/10.1203/PDR.0b013e3181dcf18a ↑13 Francès, M. P., Vila-Vecilla, L., Russo, V., Caetano Polonini, H., & de Souza, G. T. (2024). Utilising SNP Association Analysis as a Prospective Approach for Personalising Androgenetic Alopecia Treatment. Dermatology and Therapy, 14(4), 971-981. Available at: https://doi.org/10.1007/s13555-024-01142-y CYP19A1 is a gene within the cytochrome P450 superfamily, a large network of genes that regulate various critical processes throughout the body. CYP19A1 encodes the protein aromatase, which is involved in the conversion of androgens, such as testosterone, into estrogens. Aromatase is believed to play a key role in regulating hair growth, and several studies have also linked aromatase activity to hair loss. A handful of studies have also investigated genetic variation in CYP19A1, suggesting that some variants may cause differential responses to hair loss treatments. This article will explore how relevant CYP19A1 is to hair treatment effectiveness and how to interpret your genetic results to make the correct treatment choice.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What Is CYP19A1?
Cytochrome P450 Family 19 Subfamily A Member 1, known as CYP19A1, is part of the cytochrome P450 superfamily. The human genome contains at least 57 genes that belong to various CYP sub-families, collectively regulating several critical roles throughout the body. CYP19A1 encodes the protein aromatase, an enzyme involved in converting androgens to estrogens, such as androgen, into estradiol. For this reason, aromatase is also known as estrogen synthase.[1]Nebert, D. W., Wikvall, K., & Miller, W. L. (2013). Human cytochromes P450 in health and disease. Philosophical Transactions of the Royal Society B: Biological Sciences, 368(1612), 20120431. … Continue reading
Many studies have linked aromatase as a key regulatory factor in hair growth for several years. One such study was conducted on growing (anagen) phase hairs taken from female participants with and without female pattern hair loss (FPHL). Analysis of the hairs revealed that CYP19A1 expression was significantly lower in the participants with FPHL.[2]Sánchez, P., Serrano-Falcón, C., Torres, J. M., Serrano, S., & Ortega, E. (2018). 5α-Reductase isozymes and aromatase mRNA levels in plucked hair from young women with female pattern hair … Continue reading
Similarly, another study measured the aromatase levels in the hair follicles of men and women with androgenic alopecia (AGA). The follicles were taken from different regions of the head, revealing that aromatase levels were higher in the occipital (non-balding) region than in the frontal (balding) region. This difference was identified in both males and females. Still, interestingly, it was also found that aromatase levels were six times higher in the frontal hair follicles of women than in men. This could explain the differences in male and female hair loss patterns.[3]Sawaya, M. E., & Price, V. H. (1997). Different levels of 5α-reductase type I and II, aromatase, and androgen receptor in hair follicles of women and men with androgenetic alopecia. Journal of … Continue reading

Figure 1: Differences in aromatase activity in men and women.[4]Sawaya, M. E., & Price, V. H. (1997). Different levels of 5α-reductase type I and II, aromatase, and androgen receptor in hair follicles of women and men with androgenetic alopecia. Journal of … Continue reading
Associations between aromatase and hair loss have been underlined by the discovery that aromatase inhibitors can lead to the thinning and loss of hair. An analysis of 851 female breast cancer survivors revealed that those who underwent aromatase inhibitor therapy were significantly more likely to report hair loss and hair thinning than those who did not. Moreover, this association was independent of factors such as chemotherapy and radiotherapy, highlighting the importance of aromatase.[5]Gallicchio, L., Calhoun, C., & Helzlsouer, K. J. (2013). Aromatase inhibitor therapy and hair loss among breast cancer survivors. Breast cancer research and treatment, 142, 435-443. Available at: … Continue reading
Although not yet fully understood, the role of aromatase in hair loss is thought to be based on its influence on estrogen, testosterone, and dihydrotestosterone (DHT). In converting testosterone to estradiol, aromatase reduces testosterone levels and, importantly, reduces the amount of testosterone converted to DHT. High levels of DHT have been implicated in the pathogenesis of AGA. These interactions could explain the association between reduced aromatase activity and hair loss.[6]Rossi, A., Caro, G., Magri, F., Fortuna, M. C., & Carlesimo, M. (2021). Clinical aspect, pathogenesis and therapy options of alopecia induced by hormonal therapy for breast cancer. Exploration of … Continue reading
Indeed, it has been shown that aromatase inhibition in mice led to decreased levels of estradiol (a form of estrogen) and increased levels of DHT.[7]Iqbal, R., Jain, G. K., Siraj, F., & Vohora, D. (2018). Aromatase inhibition by letrozole attenuates kainic acid-induced seizures but not neurotoxicity in mice. Epilepsy Research, 143, 60-69. … Continue reading Similar results were reported in men, with aromatase inhibition leading to increased levels of testosterone and DHT. However, it should be noted that this study was conducted on older men who generally have lower levels of testosterone, so the results may not be representative of testosterone modulation in the wider population.[8]Leder, B. Z., Rohrer, J. L., Rubin, S. D., Gallo, J., & Longcope, C. (2004). Effects of aromatase inhibition in elderly men with low or borderline-low serum testosterone levels. The Journal of … Continue reading

Figure 2: Effect of anastrozole (an aromatase inhibitor) on serum testosterone, free testosterone, and dihydrotestosterone in men aged 62-74 years.[9]Leder, B. Z., Rohrer, J. L., Rubin, S. D., Gallo, J., & Longcope, C. (2004). Effects of aromatase inhibition in elderly men with low or borderline-low serum testosterone levels. The Journal of … Continue reading
A recent study has even suggested that Minoxidil, the first FDA-approved treatment for AGA, may exert its effects via interaction with aromatase. They found that Minoxidil increases the activity of aromatase, suggesting that Minoxidil may help to treat AGA by increasing the production of estradiol and decreasing the production of DHT.[10]Shen, Y., Zhu, Y., Zhang, L., Sun, J., Xie, B., Zhang, H., & Song, X. (2023). New target for minoxidil in the treatment of androgenetic alopecia. Drug Design, Development and Therapy, 2537-2547. … Continue reading

Figure 3: Human epidermal-dermal papilla cells treated with minoxidil showed an increase in mRNA levels of CYP19A1, indicating that it enhances the activity of aromatase.[11]Shen, Y., Zhu, Y., Zhang, L., Sun, J., Xie, B., Zhang, H., & Song, X. (2023). New target for minoxidil in the treatment of androgenetic alopecia. Drug Design, Development and Therapy, 2537-2547. … Continue reading
What Is The Evidence for Targeting CYP19A1 For Hair Loss?
Collectively, a significant amount of evidence suggests that aromatase is a key factor in hair loss. Owing to this, it is feasible that genetic variation in CYP19A1 could influence the efficacy of hair loss treatments.
In a study conducted on patients with polycystic ovary syndrome (PCOS), the rs2470152 single nucleotide polymorphism (SNP) in CYP19A1 was suggested to be associated with decreased aromatase activity. Namely, participants with PCOS and the TC genotype were found to exhibit increased levels of testosterone and a reduced ratio of estradiol to testosterone. In participants without PCOS, those with the TC genotype also exhibited a lower ratio of estradiol to testosterone.[12]Zhang, X.L., Zhang, C.W., Xu, P., Liang, F.J., Che, Y.N., Xia, Y.J., Cao, Y.X., Wu, X.K., Wang, W.J., Yi, L. and Gao, Q. (2012). SNP rs2470152 in CYP19 is correlated to aromatase activity in Chinese … Continue reading

Figure 4: Characteristics and serum hormone concentrations in different genotypes of women with and without PCOS. Of interest is the TC genotype; participants exhibited an increased level of estradiol (E2) and a decreased E2/T ratio (meaning increased testosterone and decreased estradiol).[13]Zhang, X.L., Zhang, C.W., Xu, P., Liang, F.J., Che, Y.N., Xia, Y.J., Cao, Y.X., Wu, X.K., Wang, W.J., Yi, L. and Gao, Q. (2012). SNP rs2470152 in CYP19 is correlated to aromatase activity in Chinese … Continue reading
People with the TC genotype may benefit from treatment with estradiol or anti-androgen drugs, given the associations between low estrogen levels, high androgen levels, and hair loss. However, it should be noted that this study was conducted on participants with PCOS; the rs2470152 SNP has not been linked to AGA or other types of hair loss, meaning it may not affect their treatment.
Furthermore, as stated earlier, the relationship between estrogen androgen levels and hair loss is still not understood. Although associations between low estrogen levels and hair loss have been identified, so too have associations between high estrogen levels and hair loss. A study involving 955 females discovered that participants with the rs4646 SNP CC genotype had an increased risk of developing FPHL.[14]Yip, L., Zaloumis, S., Irwin, D., Severi, G., Hopper, J., Giles, G., Harrap, S., Sinclair, R. and Ellis, J. (2009). Gene‐wide association study between the aromatase gene (CYP19A1) and female … Continue reading
Interestingly, the rs4646 SNP CC genotype had previously been shown to be associated with higher estrogen levels in postmenopausal females.[15]Haiman, C.A., Dossus, L., Setiawan, V.W., Stram, D.O., Dunning, A.M., Thomas, G., Thun, M.J., Albanes, D., Altshuler, D., Ardanaz, E. and Boeing, H. (2007). Genetic variation at the CYP19A1 locus … Continue reading The suggestion that higher estrogen levels may increase the risk of developing FPHL contradicts previous literature on the subject, indicating that genetics alone are not sufficient to make treatment recommendations.
Another study investigated the effects of genetic variation on dutasteride treatment, a drug used off-label in treating hair loss. They identified a positive association between the rs700519 SNP in CYP19A1 and the efficacy of dutasteride; in other words, people with this genetic variant responded better to treatment.[16]Rhie, A., Son, H.Y., Kwak, S.J., Lee, S., Kim, D.Y., Lew, B.L., Sim, W.Y., Seo, J.S., Kwon, O., Kim, J.I. and Jo, S.J. (2019). Genetic variations associated with response to dutasteride in the … Continue reading

Figure 5: Genotypic landscape of 42 patients, the cumulative effect of each allele count, and their positive or negative effect. Boxes represent SNPs that exhibited a positive (blue) or negative (red) effect on the patient’s response to dutasteride. Light-colored boxes represent heterozygous SNPs (a variation where an individual has two different versions of a specific DNA sequence at a particular location in the genome), dark-colored boxes represent homozygous SNPs (a variation where an individual has two identical versions of a specific DNA sequence at a particular location in the genome). Patient responses to dutasteride improve from left to right.[17]Rhie, A., Son, H.Y., Kwak, S.J., Lee, S., Kim, D.Y., Lew, B.L., Sim, W.Y., Seo, J.S., Kwon, O., Kim, J.I. and Jo, S.J. (2019). Genetic variations associated with response to dutasteride in the … Continue reading
Despite this positive association, some patients classified as ‘poor responders’ also had the rs700519 SNP. This indicates that having a ‘positive’ SNP in CYP19A1 does not guarantee that you will respond well to dutasteride. Rather, the study presents the likelihood that the combination of SNPs that one possesses is more important.
What Do Your Genetic Results Mean?
Your Result CYP19A1 (rs2470152)
Variant 1 – TT genotype Variant 2 – CC genotype Variant 3 – TC genotype
What it means Not associated with a change in testosterone or estrogen levels Not associated with a change in testosterone or estrogen levels Associated with reduced expression of CYP19A1 and, therefore, an increase in testosterone levels/decrease in estrogen levels The Implication May not benefit from estradiol or anti-androgens May not benefit from estradiol or anti-androgens May benefit from treatment with estradiol as a replacement hormone or anti-androgen drugs Your Result CYP19A1 (rs700519)
Variant 1 – CC genotype
Variant 2 – CT genotype Variant 3 – TT genotype
What it means May be a normal/poor responder to 5α-reductase inhibitors May be a good responder to 5α-reductase inhibitors May be a good responder to 5α-reductase inhibitors The Implication May be a good candidate for typical/higher dosages of 5α-reductase inhibitors May be a good candidate for lower dosages of 5α-reductase inhibitors May be a good candidate for lower dosages of 5α-reductase inhibitors What Relevance Does CYp19A1 Have For Hair Loss Treatment?
We have also created a rubric that helps to determine the relevance of a specific gene to hair loss based on the quality of the evidence in the above studies.
On a scale of 1-5, how important are these genetic results? (1 is the lowest, 5 is the highest)
This score is a rating based on evidence quality.
- Does this gene have any potential relevance for hair loss? (1 point)
Yes. A decrease in aromatase may lead to an increase in testosterone and, subsequently, DHT, which are linked with androgenetic alopecia. (score=1)
- Does the totality of evidence implicate CYP19A1 as a causal agent for hair loss? (1 point)
While there are some hypotheses about how SNPs in CYP19A1 may lead to hair loss, there is no published evidence showing this possible association. (score = 0)
- Does the totality of evidence implicate CYP19A1 as a predictive factor for hair loss treatment responsiveness? (2 points)
No, the data does not suggest that CYP19A1 can be used as a predictor for hair loss treatment responsiveness. (score = 0)
- Is this quality of evidence on (3) strong enough to influence treatment recommendations? (1 point)
Since CYP19A1 fails question #3, it cannot be awarded points for question #4 (score = 0)
Total Score = 1
Final Thoughts
While one small study suggests that genetic variation in CYP19A1 may influence your response to treatment with a 5α-reductase inhibitor, the evidence is not yet strong enough to make definitive treatment recommendations based solely on genotype. Furthermore, some evidence regarding CYP19A1 and its associations with hair loss conditions is contradictory. Larger and more robust studies are needed to confirm the true predictive value of genetic testing for CYP19A1 variants to personalize hair loss treatments.
References[+]
References ↑1 Nebert, D. W., Wikvall, K., & Miller, W. L. (2013). Human cytochromes P450 in health and disease. Philosophical Transactions of the Royal Society B: Biological Sciences, 368(1612), 20120431. Available at: https://doi.org/10.1098/rstb.2012.0431 ↑2 Sánchez, P., Serrano-Falcón, C., Torres, J. M., Serrano, S., & Ortega, E. (2018). 5α-Reductase isozymes and aromatase mRNA levels in plucked hair from young women with female pattern hair loss. Archives of dermatological research, 310, 77-83. Available at: https://doi.org/10.1007/s00403-017-1798-0 ↑3, ↑4 Sawaya, M. E., & Price, V. H. (1997). Different levels of 5α-reductase type I and II, aromatase, and androgen receptor in hair follicles of women and men with androgenetic alopecia. Journal of Investigative Dermatology, 109(3), 296-300. Available at: https://doi.org/10.1111/1523-1747.ep12335779 ↑5 Gallicchio, L., Calhoun, C., & Helzlsouer, K. J. (2013). Aromatase inhibitor therapy and hair loss among breast cancer survivors. Breast cancer research and treatment, 142, 435-443. Available at: https://doi.org/10.1007/s10549-013-2744-2 ↑6 Rossi, A., Caro, G., Magri, F., Fortuna, M. C., & Carlesimo, M. (2021). Clinical aspect, pathogenesis and therapy options of alopecia induced by hormonal therapy for breast cancer. Exploration of Targeted Anti-tumor Therapy, 2(5), 490. Available at: https://doi.org/10.37349/etat.2021.00059 ↑7 Iqbal, R., Jain, G. K., Siraj, F., & Vohora, D. (2018). Aromatase inhibition by letrozole attenuates kainic acid-induced seizures but not neurotoxicity in mice. Epilepsy Research, 143, 60-69. Available at: https://doi.org/10.1016/j.eplepsyres.2018.04.004 ↑8, ↑9 Leder, B. Z., Rohrer, J. L., Rubin, S. D., Gallo, J., & Longcope, C. (2004). Effects of aromatase inhibition in elderly men with low or borderline-low serum testosterone levels. The Journal of Clinical Endocrinology & Metabolism, 89(3), 1174-1180. Available at: https://doi.org/10.1210/jc.2003-031467 ↑10, ↑11 Shen, Y., Zhu, Y., Zhang, L., Sun, J., Xie, B., Zhang, H., & Song, X. (2023). New target for minoxidil in the treatment of androgenetic alopecia. Drug Design, Development and Therapy, 2537-2547. Available at: https://doi.org/10.2147/DDDT.S427612 ↑12, ↑13 Zhang, X.L., Zhang, C.W., Xu, P., Liang, F.J., Che, Y.N., Xia, Y.J., Cao, Y.X., Wu, X.K., Wang, W.J., Yi, L. and Gao, Q. (2012). SNP rs2470152 in CYP19 is correlated to aromatase activity in Chinese polycystic ovary syndrome patients. Molecular Medicine Reports, 5(1), 245-249. Available at: https://doi.org/10.3892/mmr.2011.616 ↑14 Yip, L., Zaloumis, S., Irwin, D., Severi, G., Hopper, J., Giles, G., Harrap, S., Sinclair, R. and Ellis, J. (2009). Gene‐wide association study between the aromatase gene (CYP19A1) and female pattern hair loss. British Journal of Dermatology, 161(2), 289-294. Available at: https://doi.org/10.1111/j.1365-2133.2009.09186.x ↑15 Haiman, C.A., Dossus, L., Setiawan, V.W., Stram, D.O., Dunning, A.M., Thomas, G., Thun, M.J., Albanes, D., Altshuler, D., Ardanaz, E. and Boeing, H. (2007). Genetic variation at the CYP19A1 locus predicts circulating estrogen levels but not breast cancer risk in postmenopausal women. Cancer research, 67(5), 1893-1897. Available at: https://doi.org/10.1158/0008-5472.CAN-06-4123 ↑16, ↑17 Rhie, A., Son, H.Y., Kwak, S.J., Lee, S., Kim, D.Y., Lew, B.L., Sim, W.Y., Seo, J.S., Kwon, O., Kim, J.I. and Jo, S.J. (2019). Genetic variations associated with response to dutasteride in the treatment of male subjects with androgenetic alopecia. Plos one, 14(9), e0222533. Available at: https://doi.org/10.1371/journal.pone.0222533 COL1A1 is a gene within the collagen superfamily, a large network that comprises at least 44 genes and 28 proteins. The collagen proteins have a variety of roles, with perhaps their most crucial being to support the structure of tissues throughout the body. COL1A1 and COL1A2 produce the protein chains that combine to form type 1 collagen, the most abundant type of collagen in the body, which has also been linked to regulating hair growth. Moreover, some studies have suggested that genetic variation in COL1A1 may cause differential responses to hair loss treatment.
This article will explore how relevant COL1A1 is to hair treatment effectiveness and how to interpret your genetic results to make the correct treatment choice.
All-Natural Hair Supplement
The top natural ingredients for hair growth, all in one supplement.
Take the next step in your hair growth journey with a world-class natural supplement. Ingredients, doses, & concentrations built by science.

What Is COL1A1?
Collagen Type I Alpha 1 Chain, or COL1A1, is part of the collagen superfamily. There are 44 genes encoding the proteins that make up the 28 different types of collagen, with some collagen types consisting of more than one protein (α chain).[1]Ricard-Blum, S. (2011). The collagen family. Cold Spring Harbor perspectives in biology, 3(1), a004978. Available at: https://doi.org/10.1101/cshperspect.a004978 Collagens have a variety of key roles throughout the body, foremost of which is the promotion of cell growth and supporting the structure and organization of tissues.[2]Sun, H., Wang, Y., Wang, S., Xie, Y., Sun, K., Li, S., Cui, W. and Wang, K. (2023). The involvement of collagen family genes in tumor enlargement of gastric cancer. Scientific Reports, 13(1), 100. … Continue reading
Type 1 collagen (COL1) is the most abundant of all collagen types within the body, representing over a quarter of the total protein content in mammals. It consists of two α1 chains, produced by COL1A1, and one α2 chain, produced by Collagen Type I Alpha 2 Chain (COL1A2). The three α chains assemble into a single procollagen and undergo multiple rounds of modification, with several molecules eventually assembling into a longer collagen fibril and, finally, a type 1 collagen fiber (Figure 1).[3]Kruger, T. E., Miller, A. H., & Wang, J. (2013). Collagen scaffolds in bone sialoprotein‐mediated bone regeneration. The Scientific World Journal, 2013(1), 812718. Available at: … Continue reading

Figure 1: How Type I Collagen is Made in the Body. (a) The process starts with three protein chains: two identical α1(I) chains and one α2(I) chain. (b) These three chains twist together to form a structure called procollagen. (c) An enzyme called procollagen peptidase comes along and snips off the loose ends of the procollagen.(d) After the trimming, what’s left is called a tropocollagen molecule. This is the basic building block of collagen. (e) Multiple tropocollagen molecules then line up and stick together, forming a thin strand called a collagen fibril. This fibril keeps growing as more tropocollagen molecules join in. (f) Finally, many of these collagen fibrils bundle together to create a sturdy collagen fiber. This is the form of collagen that gives strength to our skin, bones, and other tissues.[4]Kruger, T. E., Miller, A. H., & Wang, J. (2013). Collagen scaffolds in bone sialoprotein‐mediated bone regeneration. The Scientific World Journal, 2013(1), 812718. Available at: … Continue reading
Given its abundance within the body, it is hardly surprising that COL1 has been detected in the scalp. Specifically, the connective tissue sheath surrounding the hair follicle was found to be a major source of type 1 procollagen, expressing greater amounts than other parts of the follicle. Moreover, they showed that the expression of type 1 collagen changes throughout the hair cycle, collectively indicating that type 1 collagen may play a key role in the growth and structure of hair follicles.[5]Oh, J.K., Kwon, O.S., Kim, M.H., Jo, S.J., Han, J.H., Kim, K.H., Eun, H.C. and Chung, J.H. (2012). Connective tissue sheath of hair follicle is a major source of dermal type I procollagen in human … Continue reading
These results support an earlier study that found that Col1 levels in mice also changed based on the stage of the hair cycle. They found that levels of Col1 were approximately two-fold higher in the dermis of the skin in the anagen (growing) phase than skin in the telogen (resting) phase. Furthermore, they found that Col1 molecules underwent more modifications during the anagen phase. This indicates that the remodeling of collagen is more active in anagen skin, which may support the growth and migration of hair follicles.[6]Yamamoto, & Yamauchi. (1999). Characterization of dermal type I collagen of C3H mouse at different stages of the hair cycle. British Journal of Dermatology, 141(4), 667-675. Available at: … Continue reading
What is the Evidence for Targeting COL1A1 For Hair Loss?
Although only a few studies have investigated COL1 in relation to hair health, the evidence they have provided is robust and certainly suggests that COL1 may well be an important factor in regulating hair growth. Owing to this, it is feasible that genetic variation in COL1A1 could influence hair loss treatments.
Research into the rs1800012 polymorphism of Col1 revealed that people with the GT genotype had a higher ratio of COL1A1:COL1A2 gene expression and α1:α2 chains than the GG genotype. Generally existing in a 2:1 ratio, due to the structure of COL1, any increase in this ratio would lead to an imbalance between the two types of α chain.[7]Mann, V., Hobson, E.E., Li, B., Stewart, T.L., Grant, S.F., Robins, S.P., Aspden, R.M. and Ralston, S.H. (2001). A COL1A1 Sp1 binding site polymorphism predisposes to osteoporotic fracture by … Continue reading
This could lead to instability of the collagen molecules, indicating that it may be useful for people who exhibit this genotype to take supplements that might support collagen synthesis, such as silicon, cysteine, or collagen.

Figure 2: Collagen protein and mRNA levels in osteoblasts (cells that form new bones) cultured from patients with different genotypes. Different genotypes of the rs1800012 polymorphism are shown. SS genotype = GG genotype; Ss genotype = GT genotype.[8]Mann, V., Hobson, E.E., Li, B., Stewart, T.L., Grant, S.F., Robins, S.P., Aspden, R.M. and Ralston, S.H. (2001). A COL1A1 Sp1 binding site polymorphism predisposes to osteoporotic fracture by … Continue reading
Furthermore, in an analysis of over 26,000 people, it was found that the rs1800012 polymorphism is associated with AGA. Unfortunately, the study does not state which specific genotypes are associated with AGA, but this does suggest that the rs1800012 polymorphism and COL1A1 play a role in hair loss. [9]Francès, M. P., Vila-Vecilla, L., Russo, V., Caetano Polonini, H., & de Souza, G. T. (2024). Utilising SNP Association Analysis as a Prospective Approach for Personalising Androgenetic Alopecia … Continue reading
It has also been found that COL1A1 expression is upregulated in people with AGA. However, the upregulation of COL1A1 was not linked to the rs1800012 polymorphism. Moreover, the same study also showed that the expression of COL1A2 is upregulated in people with AGA, which may cause the α1:α2 chain ratio to remain unchanged.[10]Michel, L., Reygagne, P., Benech, P., Jean‐Louis, F., Scalvino, S., Ly Ka So, S., Hamidou, Z., Bianovici, S., Pouch, J., Ducos, B. and Bonnet, M., 2017. Study of gene expression alteration in male … Continue reading
Together, although these studies do suggest that COL1A1 and the rs1800012 polymorphism may be involved in hair loss, they also indicate that the underlying mechanism is not understood. Further studies are required to understand how the expression of COL1A1 and COL1A2, the rs1800012 polymorphism, and the α1:α2 chain ratio link to hair loss and AGA.
What Do Your Genetic Results Mean?
Your Result
COL1A1 (rs1800012) Variant 1 – GG genotype Variant 2 – GT genotype What it means Normal α1 chain synthesis Increased α1 chain synthesis The Implication May not benefit from supplementation that supports collagen formation May benefit from supplementation that supports collagen formation, such as adenosine or cysteine
What Relevance Does COL1A1 Have for Hair Loss Treatment?
We have also created a rubric that helps to determine the relevance of a specific gene to hair loss based on the quality of the evidence in the above studies.
On a scale of 1-5, how important are these genetic results? (1 is the lowest, 5 is the highest)
This score is a rating based on evidence quality.
- Does this gene have any potential relevance for hair loss? (1 point)
Yes, COL1A1 and COL1A2 have been found to be overexpressed in patients with androgenetic alopecia (score=1)
- Does the totality of evidence implicate COL1A1 as a causal agent for hair loss? (1 point)
No, there is no published evidence to suggest that COL1A1 polymorphisms can cause hair loss (score = 0)
- Does the totality of evidence implicate COL1A1 as a predictive factor for hair loss treatment responsiveness? (2 points)
No, there is no data to suggest that COL1A1 polymorphisms can be used as a predictor for hair loss treatment responsiveness (score = 0)
- Is this quality of evidence on (3) strong enough to influence treatment recommendations? (1 point)
Since COL1A1 fails question #3, it cannot be awarded points for question #4 (score = 0)
Total Score = 1
Final Thoughts
While there is some evidence to suggest that genetic variation in COL1A1 may influence your response to treatment with collagen supplements, there is not yet strong enough evidence to make definitive treatment recommendations based solely on genotype. Furthermore, it is evident that the association(s) between COL1A1, rs1800012, and hair loss are not yet understood. Larger and more robust studies are needed to confirm the true predictive value of genetic testing for COL1A1 variants to personalize hair loss treatments.
References[+]
References ↑1 Ricard-Blum, S. (2011). The collagen family. Cold Spring Harbor perspectives in biology, 3(1), a004978. Available at: https://doi.org/10.1101/cshperspect.a004978 ↑2 Sun, H., Wang, Y., Wang, S., Xie, Y., Sun, K., Li, S., Cui, W. and Wang, K. (2023). The involvement of collagen family genes in tumor enlargement of gastric cancer. Scientific Reports, 13(1), 100. Available at: https://doi.org/10.1038/s41598-022-25061-0 ↑3, ↑4 Kruger, T. E., Miller, A. H., & Wang, J. (2013). Collagen scaffolds in bone sialoprotein‐mediated bone regeneration. The Scientific World Journal, 2013(1), 812718. Available at: https://doi.org/10.1155/2013/812718 ↑5 Oh, J.K., Kwon, O.S., Kim, M.H., Jo, S.J., Han, J.H., Kim, K.H., Eun, H.C. and Chung, J.H. (2012). Connective tissue sheath of hair follicle is a major source of dermal type I procollagen in human scalp. Journal of Dermatological Science, 68(3), 194-197. Available at: https://doi.org/10.1016/j.jdermsci.2012.09.006 ↑6 Yamamoto, & Yamauchi. (1999). Characterization of dermal type I collagen of C3H mouse at different stages of the hair cycle. British Journal of Dermatology, 141(4), 667-675. Available at: https://doi.org/10.1046/j.1365-2133.1999.03105.x ↑7 Mann, V., Hobson, E.E., Li, B., Stewart, T.L., Grant, S.F., Robins, S.P., Aspden, R.M. and Ralston, S.H. (2001). A COL1A1 Sp1 binding site polymorphism predisposes to osteoporotic fracture by affecting bone density and quality. The Journal of Clinical Investigation, 107(7), 899-907. Available at: https://doi.org/10.1172/JCI10347 ↑8 Mann, V., Hobson, E.E., Li, B., Stewart, T.L., Grant, S.F., Robins, S.P., Aspden, R.M. and Ralston, S.H. (2001). A COL1A1 Sp1 binding site polymorphism predisposes to osteoporotic fracture by affecting bone density and quality. The Journal of clinical investigation, 107(7), 899-907. Available at: https://doi.org/10.1172/JCI10347 ↑9 Francès, M. P., Vila-Vecilla, L., Russo, V., Caetano Polonini, H., & de Souza, G. T. (2024). Utilising SNP Association Analysis as a Prospective Approach for Personalising Androgenetic Alopecia Treatment. Dermatology and Therapy, 14(4), 971-981. Available at: https://doi.org/10.1007/s13555-024-01142-y ↑10 Michel, L., Reygagne, P., Benech, P., Jean‐Louis, F., Scalvino, S., Ly Ka So, S., Hamidou, Z., Bianovici, S., Pouch, J., Ducos, B. and Bonnet, M., 2017. Study of gene expression alteration in male androgenetic alopecia: evidence of predominant molecular signalling pathways. British Journal of Dermatology, 177(5), 1322-1336. Available at: https://doi.org/10.1111/bjd.15577 Angiotensin-converting enzyme facilitates the conversion of angiotensin I to angiotensin II. This, alongside the degradation of bradykinin, leads to vasoconstriction (the tightening of blood vessels). As hair follicles require an adequate supply of blood for growth and health, it is thought that increased ACE activity can contribute to hair loss. In this article, we will explore the evidence (or lack thereof) linking ACE to hair loss and whether targeting changes in medication to single nucleotide polymorphisms (SNPs) in the ACE gene can improve hair growth outcomes.
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is ACE?
Angiotensin-converting enzyme (ACE) is an enzyme that catalyzes the conversion of angiotensin I to angiotensin II (as well as degrading bradykinin), which are important factors in the regulation of blood pressure.[1]Wong, M. K. S. (2016). Angiotensin Converting Enzymes. In Handbook of Hormones. pp. 263-e29D-4. Elsevier. Available at: https://doi.org/10.1016/B978-0-12-801028-0.00254-3 Angiotensin II is known as a vasoconstrictor – i.e., it constricts blood vessels, reducing blood flow. Some research has implicated ACE activity and its gene polymorphisms have been associated with increased susceptibility to androgenic alopecia (AGA), and to the pathogenesis of alopecia areata.[2]Ibrahim, M.A., Ezzat, I.S., Mostafa, G.Y., Fathy, A.H.N., Eman, F., Samir, E.S.O. (2021). Association between angiotensin-converting enzyme gene insertion-deletion polymorphism and androgenetic … Continue reading,[3]Fahim, S., Montazer, F., Tohidinik, H.R., Naraghi, Z.S., Abedini, R., Nasimi, M., Ghandi, N. (2019). Serum and tissue angiotensin-converting enzyme in patients with alopecia areata. Indian Journal … Continue reading
Can Targeting ACE Help Hair Loss?
Insertion or deletion changes in the ACE gene can affect its activity, with the insertion typically leading to reduced ACE activity and the deletion leading to increased ACE activity (and, therefore, increased vasoconstriction).
Characterizing single nucleotide polymorphisms (SNPs) in the ACE gene may help predict responses to treatments that can affect blood flow, such as minoxidil or caffeine.Evidence Supporting Targeting ACE Polymorphisms For Hair Loss
ACE plays a key role in regulating blood pressure, converting angiotensin I to angiotensin II, and constricting blood vessels. Research in androgenic alopecia (AGA) indicates that the insertion/deletion gene mutation in the ACE gene is associated with increased susceptibility to AGA. The researchers found that the deletion/deletion and insertion/deletion genotypes were more frequently found in AGA patients, suggesting a genetic predisposition linked to ACE activity.[4]Mustafa, A.I., Ibrahim, S.E., Gohary, Y.M., Al-Husseini, N.F., Fawzy, E., El-Shimi, O.S. (2022). Association between angiotensin-converting enzyme gene insertion-deletion polymorphism and … Continue reading

Figure 1: Comparison between AGA patients and controls regarding ACE genotypes. The insertion/deletion (ID) and deletion/deletion (DD) genotypes were significantly increased in AGA patients compared to controls.[5]Ibrahim, M.A., Ezzat, I.S., Mostafa, G.Y., Fathy, A.H.N., Eman, F., Samir, E.S.O. (2021). Association between angiotensin-converting enzyme gene insertion-deletion polymorphism and androgenetic … Continue reading
Another study also found a link between ACE activity and the pathogenesis of alopecia areata (AA). In a study conducted on 49 people (25 with alopecia areata and 24 controls), researchers found no significant difference in serum ace activity but a significantly lower ace activity in the tissue. Furthermore, among patients with alopecia areata, higher ACE activity was associated with more severe disease and non-patchy alopecia areata.[6]Fahim, S., Montazer, F., Tohidinik, H.R., Naraghi, Z.S., Abedini, R., Nasimi, M., Ghandi, N. (2019). Serum and tissue angiotensin-converting enzyme in patients with alopecia areata. Indian Journal … Continue reading
While there appears to be a link between ACE and AGA, and AA, there are no studies linking ACE activity or gene polymorphisms to treatment efficacy in hair loss. Some genetic testing companies, however, believe that if you have the deletion polymorphisms of rs4343 or rs4341, you may want to try treatments that improve blood flow to the scalp.
The single nucleotide polymorphisms (SNP) rs4343 and rs4341 are variations in the ACE gene, part of the renin-angiotensin system (RAS). The RAS plays an important role in blood pressure regulation and fluid balance.
The G allele of rs4343 corresponds to the deletion allele of the ACE gene, which has been associated with higher ACE activity.[7]Tsantes, A.E., Kopterides, P., Bonovas, S., Bagos, P., Antonakos, G., Nikolopoulos, G.K., Gialeraki, A., Kapsimali, V., Kyriakou, E., Kokori, S., Dima, K., Armagandis, A., Tsangaris, I. (2013).Effect … Continue readingHigher ACE levels lead to increased production of angiotensin II, which leads to vasoconstriction. Some think that hair loss treatments (such as caffeine or minoxidil), which are thought to work at least in part through vasodilation, might improve hair loss outcomes.
Evidence Against Targeting ACE Polymorphisms For Hair Loss
While it is thought that minoxidil works by increasing blood flow to the hair follicle, no literature suggests that people with particular ACE polymorphisms will respond differently to hair treatments that may improve blood flow, such as caffeine or minoxidil.
Your Genetic Results
Your Result ACE (rs4343)
Variant 1 – AA genotype (insertion/insertion) Variant 2 – AG genotype (insertion/deletion) Variant 3 – GG genotype (deletion/deletion) What it means May have no abnormal vasoconstriction due to normal ACE activity May have moderately elevated vasoconstriction in the scalp due to a slight increase in ACE activity May have elevated vasoconstriction in the scalp due to increased ACE activity The Implication May not benefit from treatments that target blood flow, such as minoxidil or caffeine May want to try managing hair loss with treatments targeting blood flow, such as minoxidil or caffeine May want to try managing hair loss with treatments targeting blood flow, such as minoxidil or caffeine Your Result
ACE (rs4341)
Variant 1 – CC genotype Variant 2 – CG genotype Variant 3 – GG genotype What it means May have no abnormal vasoconstriction due to normal ACE activity May have moderately elevated vasoconstriction in the scalp due to a slight increase in ACE activity May have elevated vasoconstriction in the scalp due to increased ACE activity The Implication May not benefit from treatments that target blood flow, such as minoxidil or caffeine May want to try managing hair loss with treatments targeting blood flow, such as minoxidil or caffeine May want to try managing hair loss with treatments targeting blood flow, such as minoxidil or caffeine Treatment Relevance
We have also created a rubric that helps to determine the relevance of a specific gene to hair loss based on the quality of the evidence in the above studies.
On a scale of 1-5, how important are these genetic results? (1 is the lowest, 5 is the highest)
This score is a rating based on evidence quality.
- Does this gene have any potential relevance for hair loss? (1 point)
There is no evidence to support its significance in hair loss treatments (score=0)
-
- Does the totality of evidence implicate ACE as a causal agent for hair loss? (1 point)
No, there is no published evidence to suggest that ACE polymorphisms can cause hair loss (score = 0)
- Does the totality of evidence implicate ACE as a predictive factor for hair loss treatment responsiveness? (2 points)
No, there is no data to suggest that ACE polymorphisms can be used as a predictor for hair loss treatment responsiveness (score = 0)
- Is this quality of evidence on (3) strong enough to influence treatment recommendations? (1 point)
Since ACE fails question #3, it cannot be awarded points for question #4 (score = 0)
Total Score = 0
Final Thoughts
ACE is essential in maintaining circulation throughout the body and may play some role in the pathogenesis of AGA. However, no evidence supports targeting it as a predictor of treatment efficacy.
References[+]
References ↑1 Wong, M. K. S. (2016). Angiotensin Converting Enzymes. In Handbook of Hormones. pp. 263-e29D-4. Elsevier. Available at: https://doi.org/10.1016/B978-0-12-801028-0.00254-3 ↑2 Ibrahim, M.A., Ezzat, I.S., Mostafa, G.Y., Fathy, A.H.N., Eman, F., Samir, E.S.O. (2021). Association between angiotensin-converting enzyme gene insertion-deletion polymorphism and androgenetic alopecia susceptibility among Egyptian patients: A preliminary case-controlled study. Journal of Cosmetic Dermatology. 21(6). 2629-2634. Available at: https://doi.org/10.1111/jocd.14434 ↑3, ↑6 Fahim, S., Montazer, F., Tohidinik, H.R., Naraghi, Z.S., Abedini, R., Nasimi, M., Ghandi, N. (2019). Serum and tissue angiotensin-converting enzyme in patients with alopecia areata. Indian Journal of Dermatology, Venerology and Leprology. (85)3. 295-299 Available at: https://doi.org/10.4103/ijdvl.IJDVL_158_17. ↑4 Mustafa, A.I., Ibrahim, S.E., Gohary, Y.M., Al-Husseini, N.F., Fawzy, E., El-Shimi, O.S. (2022). Association between angiotensin-converting enzyme gene insertion-deletion polymorphism and androgenetic alopecia susceptibility among Egyptian patients: a preliminary case-controlled study. Journal of Cosmetic Dermatology. 21(60). 2629-2634. Available at: https://doi.org/10.1111/jocd ↑5 Ibrahim, M.A., Ezzat, I.S., Mostafa, G.Y., Fathy, A.H.N., Eman, F., Samir, E.S.O. (2021). Association between angiotensin-converting enzyme gene insertion-deletion polymorphism and androgenetic alopecia susceptibility among Egyptian patients: A preliminary case-controlled study. Journal of Cosmetic Dermatology. 21(6). 2629-2634. Available at: https://doi.org/10.1111/jocd.14434 ↑7 Tsantes, A.E., Kopterides, P., Bonovas, S., Bagos, P., Antonakos, G., Nikolopoulos, G.K., Gialeraki, A., Kapsimali, V., Kyriakou, E., Kokori, S., Dima, K., Armagandis, A., Tsangaris, I. (2013).Effect of angiotensin-converting enzyme gene I/D polymorphism and its expression on clinical outcome in acute respiratory distress syndrome. Minerva anestesiologica. 79(8). 861-870. Available at: PMID 23635999 The NR3C1 gene encodes the glucocorticoid receptor, which is essential for mediating the effects of glucocorticoids in various physiological processes, including metabolism, immune response, and stress regulation. This receptor plays a critical role in the body’s ability to respond to glucocorticoid medications, making it a key factor in conditions treated with these drugs.
This article will delve into the role of NR3C1 in glucocorticoid responsiveness and the evidence (or lack thereof) supporting it as a target for hair loss.
What is NR3C1?
The NR3C1 gene codes for the glucocorticoid receptor (GR). This receptor is involved in various physiological processes, including metabolism regulation, immune response, and stress response.[1]GeneCards. (no date). NR3C1 Gene – Nuclear Receptor Subfamily 3 Group C Member 1. GeneCards. Available at: … Continue reading. Glucocorticoids are a type of steroid used to treat inflammatory and autoimmune diseases as well as cancer.[2]Strehl, C., Ehlers, L., Gaber, T., Butthereit, F. (2019). Glucocorticoids – All Rounders Tackling the Versatile Players of the Immune System. Frontiers in Immunology. 10 GR is necessary for … Continue reading
All-Natural Hair Topical
The top natural ingredients for hair growth, all in one serum.
Take the next step in your hair growth journey with a world-class natural serum. Ingredients, doses, & concentrations built by science.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is the Evidence for Targeting NR3C1 for Hair Loss?
GR is essential for glucocorticoids to exert their effects. There are two isoforms of GR encoded by the NR3C1 gene: GRα and GRβ. GRα is the classic GR protein, mediating the action of glucocorticoids.
GRβ contains a unique extra sequence that gives it several distinct properties: GRβ does not bind to activators of glucocorticoids, resides in the nucleus of the cells, and is by itself inactive. However, when expressed alongside GRα, GRβ inhibits the activity of GRα.[3]Oakley, R.H., Cidlowski, J.A. (2013). The Biology of the Glucocorticoid Receptor: New Signaling Mechanisms in Health and Disease. Journal of Allergy and Clinical Immunology. 132(5). 1033-1044. … Continue reading
Simply put, if GRꞵ binds to GRɑ, it stops it from working correctly. This can lead to reduced sensitivity or even resistance to glucocorticoids in tissues expressing GRβ at higher levels.
In one retrospective study involving 122 children with acute lymphoblastic leukemia, researchers found that a specific genetic variant, called rs6198, can affect how the body responds to glucocorticoid medications.[4]Gasic, V., Zukic, B., Stankovic, B., Janic, D., Dokmanovic, L., Lazic, J., Krstovski, N., Dolzan, V., Jazbec, J., Pavlovic, S., Kotur, N. (2018). Pharmacogenomic Markers of Glucocorticoid Response in … Continue reading
When a patient had the GG allele variant, it was found that it stabilized the messenger RNA (mRNA), which is the molecule that carries instructions from DNA to make proteins. This stabilization leads to more of a particular form of the glucocorticoid receptor, which doesn’t bind to the medication as well as the normal form.
Because this receptor doesn’t bind well, the treatment may not work as effectively, which could explain why some patients developed resistance to glucocorticoid therapy. This means their bodies don’t respond as well to the treatment, making it less effective in controlling their condition.

Figure 1: Genotype frequencies associated with glucocorticoid response. The bold numbers indicate a significant difference. NR3C1 6198 shows a significant association with glucocorticoid resistance.[5]Gasic, V., Zukic, B., Stankovic, B., Janic, D., Dokmanovic, L., Lazic, J., Krstovski, N., Dolzan, V., Jazbec, J., Pavlovic, S., Kotur, N. (2018). Pharmacogenomic Markers of Glucocorticoid Response in … Continue reading
What is the Evidence Against Targeting NR3C1 for Hair Loss?
Some companies that test your genotype to suggest treatments use this gene as a marker for glucocorticoid sensitivity. While the evidence suggests that variations of NR3C1 can negatively affect glucocorticoid receptor activity, there is no published evidence showing that there are subsequent effects on corticosteroid treatment responsiveness in hair.
What Do Your Genetic Results Mean?
Your Result NR3C1 (rs6198)
Variant 1 GG genotype
Variant 2 GA genotype Variant 3 AA genotype
What it means Increased expression of the GRβ isoform Moderate expression of the GRβ isoform Normal expression of GR and less expression of the GRβ isoform The Implication You may want to avoid glucocorticoid treatment You may respond less well to glucocorticoid treatment You may respond normally to glucocorticoid treatment What Relevance Does NR3C1 Have For Hair Loss Treatment?
We have also created a rubric that helps to determine the relevance of a specific gene to hair loss based on the quality of the evidence in the above studies.
On a scale of 1-5, how important are these genetic results? (1 is the lowest, 5 is the highest)
This score is a rating based on evidence quality.
- Does this gene have any potential relevance for hair loss? (1 point)
Yes. Due to the inhibitory effect of GRβ on GR activity, this variation may affect response to glucocorticoid treatment in cases of hair loss. (score = 1)
- Does the totality of evidence implicate GRα as a causal agent for hair loss? (1 point)
No, there doesn’t appear to be any evidence implicating GRα in hair loss.
- Does the totality of evidence implicate GRα as a predictive factor for hair loss treatment responsiveness? (2 points)
While there is evidence to suggest that the activity of GRα may be affected by this variation, there is no published evidence to indicate that it can predict responsiveness to glucocorticoid treatment. (score = 0)
- Is this quality of evidence on (3) strong enough to influence treatment recommendations? (1 point)
No, the quality of evidence is not strong enough to influence treatment recommendations due to the lack of published evidence. (score = 0)
Total Score = 1
Final Thoughts
The NR3C1 gene, which encodes the glucocorticoid receptor, plays a crucial role in various physiological processes, including stress response and inflammation. While variations in the gene, particularly the rs6198 variant, have been linked to altered glucocorticoid sensitivity, the evidence for its role in hair loss remains inconclusive. Therefore, more research is needed to determine its relevance and utility in predicting or treating hair loss.
References[+]
References ↑1 GeneCards. (no date). NR3C1 Gene – Nuclear Receptor Subfamily 3 Group C Member 1. GeneCards. Available at: https://www.genecards.org/cgi-bin/carddisp.pl?gene=NR3C1#:~:text=This%20gene%20encodes%20glucocorticoid%20receptor,regulator%20of%20other%20transcription%20factors. (Accessed: July 2024) ↑2 Strehl, C., Ehlers, L., Gaber, T., Butthereit, F. (2019). Glucocorticoids – All Rounders Tackling the Versatile Players of the Immune System. Frontiers in Immunology. 10 GR is necessary for glucocorticoids to bind to and exert their biological effects. 10. 1-20. Available at: https://doi.org/10.3389/fimmu.2019.01744 ↑3 Oakley, R.H., Cidlowski, J.A. (2013). The Biology of the Glucocorticoid Receptor: New Signaling Mechanisms in Health and Disease. Journal of Allergy and Clinical Immunology. 132(5). 1033-1044. Available at: https://doi.org/10.1016/j.jaci.2013.09.007 ↑4 Gasic, V., Zukic, B., Stankovic, B., Janic, D., Dokmanovic, L., Lazic, J., Krstovski, N., Dolzan, V., Jazbec, J., Pavlovic, S., Kotur, N. (2018). Pharmacogenomic Markers of Glucocorticoid Response in The Initial Phase of Remission Induction Therapy in Childhood Acute Lymphoblastic Leukemia. Radiology and Oncology. 52(3). 296-306. Available at: https://doi.org/10.2478/raon-2018-0034 ↑5 Gasic, V., Zukic, B., Stankovic, B., Janic, D., Dokmanovic, L., Lazic, J., Krstovski, N., Dolzan, V., Jazbec, J., Pavlovic, S., Kotur, N. (2018). Pharmacogenomic Markers of Glucocorticoid Response in The Initial Phase of Remission Induction Therapy in Childhood Acute Lymphoblastic Leukemia. Radiology and Oncology. 52(3). 296-306. Available at: https://doi.org/10.2478/raon-2018-0034 The PGFTR gene encodes the prostaglandin F2 alpha (PGF2α) receptor, a critical component in various physiological processes. PGFTR is particularly significant in the context of hair loss due to its involvement in hair follicle and melanocyte growth. Studies have shown that PGF2α and its analogs, such as latanoprost, can stimulate hair growth and treat eyelash and eyebrow growth issues like hypotrichosis.
This article will explore the importance of the PGFTR gene in hair loss, its potential as a therapeutic target, and how understanding your genetic makeup could inform more effective treatment decisions.
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is PGTFR?
The PGTFR gene encodes the prostaglandin F2 alpha (PGF2α) receptor, which plays an important role in various physiological processes, including reproductive physiology, inflammation, and cancer progression.[1]Ricciotti, E., FitzGerald, G.A. (2011). Prostaglandins and Inflammation. Arteriosclerosis, Thrombosis, and Vascular Biology. 31(5). 986-1000. Available at: https://doi.org/10.1161/ATVBAHA.110.207449.
Studies have suggested that PGF2α and its analogs, like latanoprost, stimulate the hair follicle and melanocyte growth in mice.[2]Sasaki, S., Hozumi, Y., Kondo, S. (2005). Influence of Prostaglandin F2 alpha and its Analogues on Hair Regrowth and Follicular Melanogenesis in a Murine Model. Experimental Dermatology. 14(5). … Continue reading
Can Targeting PGTFR Help Hair Loss?
Latanoprost is an analog of PGF2α and is commonly used as a treatment for an eye condition called glaucoma. Some clinical studies looking at the responsiveness of patients to latanoprost have uncovered multiple gene variants that can either increase or decrease responsiveness to the drug.
One study involved 100 volunteers who applied latanoprost eye drops to one eye once daily for seven days. Intraocular pressure was measured at the beginning and end of the study.[3]Sakurai, M., Higashide, T., Takahashi, M., Sugiyama, K. (2007). Association between Genetic Polymorphisms of the Prostaglandin F2ɑ Receptor Gene and Response to Latanoprost. Ophthalmology. 114(6). … Continue reading
Two key single nucleotide polymorphisms (SNPs) in the PGTFR gene were found to be associated with response to latanoprost treatment. SNPs are single-base pair gene changes. These single changes can have varied effects, from dramatic impacts on gene function or protein structure to no noticeable effect at all.
The results showed that within the rs3753380 SNP, the CC genotype was associated with a greater response to latanoprost, and the CT and TT genotypes were significantly associated with a lesser response. The rs3766355 SNP also found specific genotypes associated with lower latanoprost response. The study also found that the C allele of rs3766355 and the T allele of rs3753380 were associated with lower transcriptional activity of PGTFR, which suggests that these alleles may lead to reduced expression of PGTFR, resulting in a decreased response to latanoprost.

Figure 1: Latanoprost responsiveness based on single nucleotide polymorphism.[4]Sakurai, M., Higashide, T., Takahashi, M., Sugiyama, K. (2007). Association between Genetic Polymorphisms of the Prostaglandin F2ɑ Receptor Gene and Response to Latanoprost. Ophthalmology. 114(6). … Continue reading
This has been repeated in several studies that have evaluated various SNPs associated with the PGTFR gene for latanoprost’s effectiveness in treating glaucoma.
No studies have demonstrated whether SNPs in the PGTFR gene affect treatment responsiveness in relation to hair loss; however, PGF2ɑ analogs have been shown to improve hair growth outcomes.One randomized, double-blind, placebo-controlled study involving 16 men with androgenic alopecia was conducted over 24 weeks. It found that daily application of latanoprost 0.1% significantly increased hair density compared to baseline and placebo-treated areas of the scalp, suggesting that latanoprost can stimulate hair growth.[5]Blume-Peytavi, U., Lonngors, S., Hillmann, K., Bartels, N.G. (2012). A Randomized, Double-Blind, Placebo-Controlled Pilot Study to Assess the Efficacy of a 24-Week Topical Treatment by Latanoprost … Continue reading

Figure 2: number and percentage of anagen and telogen hairs per cm2 at baseline and week 24.[6]Blume-Peytavi, U., Lonngors, S., Hillmann, K., Bartels, N.G. (2012). A Randomized, Double-Blind, Placebo-Controlled Pilot Study to Assess the Efficacy of a 24-Week Topical Treatment by Latanoprost … Continue reading
Furthermore, a recent paper explored the genetic factors associated with androgenic alopecia.[7]Frances, M.P., Vila-Vecilla, L., Russo, V., Polonini, H.C., de Souza, G.T. (2024). Utilizing SNP Association Analysis as a Prospective Approach for Personalising Androgenetic Alopecia Treatment. … Continue reading The study analyzed data from 26,607 patients, examining 26 SNPs and their correlation with AGA diagnosis. Eight SNPs were found to show a statistically significant association with AGA, one of which was PTGFR (rs10782665). However, there was no correlation found between these SNPs and the severity of AGA.
While the studies above suggest an effect of PGTFR gene variants on latanoprost effectiveness, no studies have determined this in the context of hair growth.
What Do Your Genetic Results Mean?
Your Result PGTFR (rs10782665)
Variant 1 – TT genotype Variant 2 – GT genotype Variant 3 – GG genotype What it means Associated with a higher percentage of responders to latanoprost treatment Associated with a moderately higher percentage of responders to latanoprost treatment Associated with a higher percentage of non-responders to latanoprost treatment The Implication May benefit from latanoprost treatment May benefit from latanoprost treatment May benefit from treatments other than latanoprost Your Result PGTFR (rs6686438)
Variant 1 – TT genotype Variant 2 – GT genotype Variant 3 – GG genotype What it means Associated with a higher percentage of responders to latanoprost treatment Associated with a higher percentage of responders to latanoprost treatments Associated with a higher percentage of non-responders to latanoprost treatment The Implication May benefit from latanoprost treatment May benefit from latanoprost treatment May benefit from treatments other than latanoprost Your Result PGTFR (rs1328441)
Variant 1 – AA genotype Variant 2 – AG genotype Variant 3 – GG genotype What it means Associated with a higher percentage of responders to latanoprost treatment Not associated with either responsiveness or non-responsiveness to latanoprost Associated with a higher percentage of non-responders to latanoprost treatment The Implication May benefit from latanoprost treatment May benefit from latanoprost treatment May benefit from treatments other than latanoprost Treatment Relevance
We have created a rubric that helps to determine the relevance of a specific gene to hair loss based on the quality of the evidence in the above studies.
On a scale of 1-5, how important are these genetic results? (1 is the lowest, 5 is the highest)
This score is a rating based on evidence quality.
Does this gene have any potential relevance for hair loss? (1 point)
- Yes. Initial studies have indicated that latanoprost could work as a treatment for hair loss. (score = 1)
Does the totality of evidence implicate PGTFR as a causal agent for hair loss? (1 point)
- There is no literature to suggest that PGTFR is a causal agent for hair loss. (score = 0)
Does the totality of evidence implicate PGTFR as a predictive factor for hair loss treatment responsiveness? (2 points)
- Although some studies have shown that PGTFR gene variations can affect latanoprost treatment responsiveness for patients with glaucoma, this has not also been shown to be true in the hair follicle. (score = 0)
Is this quality of evidence on (3) strong enough to influence treatment recommendations? (1 point)
- It may be worth trying or avoiding latanoprost treatments if you have certain gene variations. (score = 1)
Total Score = 2
Final Thoughts
While some small studies suggest that genetic variation in the PGTFR gene may influence responsiveness to treatments like latanoprost, the evidence is not yet strong enough to make definitive treatment recommendations based solely on genotype. Larger and more robust studies are needed to confirm the true predictive value of genetic testing for PGTFR in personalizing hair loss treatments. Understanding the genetic underpinnings of hair loss and treatment responsiveness could eventually lead to more effective and tailored therapeutic approaches, but current data is insufficient to guide clinical decisions at this time.
References[+]
References ↑1 Ricciotti, E., FitzGerald, G.A. (2011). Prostaglandins and Inflammation. Arteriosclerosis, Thrombosis, and Vascular Biology. 31(5). 986-1000. Available at: https://doi.org/10.1161/ATVBAHA.110.207449. ↑2 Sasaki, S., Hozumi, Y., Kondo, S. (2005). Influence of Prostaglandin F2 alpha and its Analogues on Hair Regrowth and Follicular Melanogenesis in a Murine Model. Experimental Dermatology. 14(5). 323-328. Available at: https://doi.org/10.1111/j.0906-6705.2005.00270.x. ↑3, ↑4 Sakurai, M., Higashide, T., Takahashi, M., Sugiyama, K. (2007). Association between Genetic Polymorphisms of the Prostaglandin F2ɑ Receptor Gene and Response to Latanoprost. Ophthalmology. 114(6). 1039-1045. Available at: https://doi.org/10.1016/j.ophtha.2007.03.025. ↑5, ↑6 Blume-Peytavi, U., Lonngors, S., Hillmann, K., Bartels, N.G. (2012). A Randomized, Double-Blind, Placebo-Controlled Pilot Study to Assess the Efficacy of a 24-Week Topical Treatment by Latanoprost 0.1% on Hair Growth and Pigmentation in Healthy Volunteers with Androgenetic Alopecia. Journal of the American Academy of Dermatology. 66(5). 797-800. Available at: https://doi.org/10.1016/j.jaad.2011.05.026. ↑7 Frances, M.P., Vila-Vecilla, L., Russo, V., Polonini, H.C., de Souza, G.T. (2024). Utilizing SNP Association Analysis as a Prospective Approach for Personalising Androgenetic Alopecia Treatment. Dermatology and Therapy (Heidelb). 14(4). 971-981. Available at: https://doi.org/10.1007/s13555-024-01145-y The PTGES2 gene encodes the enzyme prostaglandin E synthase 2, which plays a crucial role in converting prostaglandin H2 to prostaglandin E2 (PGE2). This enzyme is significant in various physiological processes, including inflammation and hair growth. Notably, studies have identified higher levels of PGE2 in non-balding scalps compared to balding ones, highlighting the potential relevance of PTGES2 in hair loss.
This article will delve into the role of PTGES2 in hair loss, its potential as a therapeutic target, and how genetic insights can guide more personalized and effective treatments.
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is PTGES2?
Prostaglandin E synthase 2 (PTGES2) gene encodes the enzyme prostaglandin E synthase 2. This enzyme catalyzes the conversion of prostaglandin H2 (PGH2) to prostaglandin E2 (PGE2). It is a key enzyme in the prostaglandin synthesis pathway and plays a crucial role in various physiological processes, including inflammation and hair growth.
The PTGES2 gene codes for the prostaglandin E synthase enzyme, which is a key element in the synthesis of PGE2. Studies on human scalp samples have found PGE2 to be more abundant in non-balding scalps compared to balding scalps.[1]Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). … Continue reading
Can Targeting PTGES2 Help Hair Loss?
There is some evidence to suggest that PTGES2 might be worth targeting:
Elevated PGE2 levels in haired scalp
Multiple studies have consistently shown that PGE2 levels are diminished in balding scalp areas compared to haired areas. For instance, measurements in patients with AGA have shown that PGE2 and PGF2ɑ were significantly lower in bald areas, while PGD2 and prostacyclin were elevated.[2]Chovarda, E., Sotiriou, E., Lazaridoi, E., Vakirlis, E., Ioannides, D. (2021). The Role of Prostaglandins in Androgenetic Alopecia. International Journal of Dermatology. 60. 730-735. Available at: … Continue reading

Figure 1: Prostaglandin mean levels (ng/g tissue) in patients with AGA comparing bald areas with non-balding.[3]Chovarda, E., Sotiriou, E., Lazaridoi, E., Vakirlis, E., Ioannides, D. (2021). The Role of Prostaglandins in Androgenetic Alopecia. International Journal of Dermatology. 60. 730-735. Available at: … Continue reading
PTGES2 Expression in Androgenic Alopecia
A study on 16 Hispanic males with androgenic alopecia (AGA) found that PTGES2 expression was significantly increased in the balding scalp compared to 16 control participants. This overexpression of PTGES2 in early male pattern hair loss is hypothesized to be the body’s attempt to counteract hair loss.[4]Villareal-Villareal, C.D., Sinclair, R.D., Martinez-Jacobo, L., Garza-Rodriguez, V., Rodriguez-Leon, S.A., Lamadrid-Zertuche, A.C., Rodriguez-Gutierrez, R., Ortiz-Lopez, R., Rojas-Martinez, A., … Continue reading

Figure 2: Comparison of relative gene expression of PTGES in patients with AGA and control patients.[5]Villareal-Villareal, C.D., Sinclair, R.D., Martinez-Jacobo, L., Garza-Rodriguez, V., Rodriguez-Leon, S.A., Lamadrid-Zertuche, A.C., Rodriguez-Gutierrez, R., Ortiz-Lopez, R., Rojas-Martinez, A., … Continue reading
Furthermore, a recent study delved into the genetic factors associated with AGA. The researchers analyzed genetic data from 26,607 patients, focusing on 26 SNPS and their correlation with a diagnosis of AGA. Eight SNPs were found to show a statistically significant association with AGA, one of which was PTGES2 (rs13283456).[6]Frances, M.P., Vila-Vecilla, L., Russo, V., Polonini, H.C., de Souza, G.T. (2024). Utilizing SNP Association Analysis as a Prospective Approach for Personalising Androgenetic Alopecia Treatment. … Continue reading However, it should be noted that no correlation was found between the SNP and AGA severity.
Moreover, the study does not mention the samples from which the genetic information was gained. Genetic analyses of human scalp hair follicles have found unique gene expression profiles not found in other tissues.[7]Wu, S., Yu, Y., Liu, C., Zhang, X., Zhu, P., Peng, Y., Yan, X., Li, Y., Hua, P., Li, Q., Wang, S., Zhang, L. (2022). Single-cell transcriptomics reveals lineage trajectory of human scalp hair … Continue reading So, PTGES2 gene expression may not have the same association in tissue taken from the scalp.
Therefore, while general genetic studies do provide insights, they should be approached with caution when extrapolating these findings to hair growth processes.
Some believe that this SNP could affect responsiveness to minoxidil when targeting a gene for treatment efficacy. One study conducted on human dermal papilla cells found that minoxidil increased PGE2 production.[8]Michelet, J.F., Commo, S., Billoni, N., Mahe, Y.F., Bernard, B.A. (1997). Activation of cytoprotective prostaglandin synthase-1 by minoxidil as a possible explanation for its hair growth-stimulating … Continue readingSo, if you have the gene variant leading to lower activity of PGE2 synthase, minoxidil may be more beneficial.
What Do Your Genetic Results Mean?
Your Result PTGES2 (rs13283456) Variant 1 – CC genotype Variant 2 – TT genotype Variant 3 – CT genotype What it means Normal enzymatic activity of PGE2 synthase Normal enzymatic activity of PGE2 synthase Lower enzymatic activity of PGE2 synthase The Implication Will not affect the efficacy of minoxidil Will not affect the efficacy of minoxidil May be more beneficial to use minoxidil as a treatment for hair loss What Relevance Does PTGES2 Have for Hair Loss Treatment?
We have also created a rubric that helps to determine the relevance of a specific gene to hair loss based on the quality of the evidence in the above studies.
On a scale of 1-5, how important are these genetic results? (1 is the lowest, 5 is the highest)
This score is a rating based on evidence quality.
- Does this gene have any potential relevance for hair loss? (1 point)
Yes. Studies have found that PGE2 levels are elevated in scalps of patients with a normal amount of hair compared to those with hair loss. (score = 1)
- Does the totality of evidence implicate PTGES2 as a causal agent for hair loss? (1 point)
Whilst this may be a causal agent for hair loss, there doesn’t appear to be literature to support this yet. Furthermore, there have been no studies to determine if a lack of PGE2 leads to the development of hair loss disorders. (0 = score)
- Does the totality of evidence implicate PTGES2 as a predictive factor for hair loss treatment responsiveness? (2 points)
No, the studies show that the gene variant that leads to reduced PTGES2 activity does not have any predictive value in determining patient response to hair loss treatment. (0 = score)
- Is this quality of evidence on (3) strong enough to influence treatment recommendations? (1 point)
Since PTGES2 fails question #3, it cannot be awarded points for question #4 (score = 0)
Total Score = 1
Final Thoughts
The PTGES2 gene has shown potential in hair loss treatment. However, current evidence is not sufficient to make definitive treatment recommendations based on PTGES2 genotypes. Research indicates that PGE2 levels are higher in non-balding scalps, and PTGES2 expression is increased in balding areas. Yet, there is still no conclusive proof that PTGES2 is a causal factor in hair loss. Moreover, the genetic variant rs13283456 associated with PTGES2 does not appear to predict treatment responsiveness effectively. Further research is necessary to better understand the role of PTGES2 in hair growth and to determine its potential as a target for hair loss treatments.
References[+]
References ↑1 Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). Prostaglandin D2 Inhibits Hair Growth and is Elevated in Bald Scalp of Men with Androgenetic Alopecia. Science Translational Medicine. 4(126). 1-21. Available at: https://doi.org/10.1126/scitranslmed.3003122 ↑2, ↑3 Chovarda, E., Sotiriou, E., Lazaridoi, E., Vakirlis, E., Ioannides, D. (2021). The Role of Prostaglandins in Androgenetic Alopecia. International Journal of Dermatology. 60. 730-735. Available at: https://doi.org/10.1111/ijd.15378 ↑4, ↑5 Villareal-Villareal, C.D., Sinclair, R.D., Martinez-Jacobo, L., Garza-Rodriguez, V., Rodriguez-Leon, S.A., Lamadrid-Zertuche, A.C., Rodriguez-Gutierrez, R., Ortiz-Lopez, R., Rojas-Martinez, A., Ocampo-Candiani, J. (2019). Prostaglandins in androgenetic alopecia in 12 men and four female. Journal of the European Academy of Dermatology and Venereology. 33(5). E214-e215. Available at: https://doi.org/10.1111/jdv.15479 ↑6 Frances, M.P., Vila-Vecilla, L., Russo, V., Polonini, H.C., de Souza, G.T. (2024). Utilizing SNP Association Analysis as a Prospective Approach for Personalising Androgenetic Alopecia Treatment. Dermatology and Therapy (Heidelb). 14(4). 971-981. Available at: https://doi.org/10.1007/s13555-024-01145-y ↑7 Wu, S., Yu, Y., Liu, C., Zhang, X., Zhu, P., Peng, Y., Yan, X., Li, Y., Hua, P., Li, Q., Wang, S., Zhang, L. (2022). Single-cell transcriptomics reveals lineage trajectory of human scalp hair follicle and informs mechanisms of hair graying. Cell Discovery. 8(49). 1-20. Available at: https://doi.org/10.1038/s41421-022–00394-2 ↑8 Michelet, J.F., Commo, S., Billoni, N., Mahe, Y.F., Bernard, B.A. (1997). Activation of cytoprotective prostaglandin synthase-1 by minoxidil as a possible explanation for its hair growth-stimulating effect. Journal of Investigative Dermatology. 108(2). 205-209. Available at: https://doi.org/10.1111/1523-1747.ep12334249 IngredientsPharmaceuticalsNatural RemediesCompany Reviews
By Perfect Hair Health TeamNov 8, 2025Hims vs Keeps vs Roman: Which Hair Growth Subscription Service Wins?
Hair growth subscription services are sprouting up everywhere online. Among them, three companies have emerged from the pack: Hims, Keeps, and Roman. Each company offers two FDA-approved hair loss treatments, as well as other add-on products (supplements, gummies, etc). In this post, the Perfect Hai...
By Perfect Hair Health TeamNov 8, 2025Vitamin B1 for Hair Loss: Good or Bad for Hair Loss?
Vitamin B1 – also known as thiamine (or thiamin) – is part of the B-complex of vitamins. In mouse models, severe vitamin B1 deficiencies lead to rapid weight loss, neurological decline, and hair loss. However, thiamine repletion studies (as well as studies on humans) suggest that this hair loss seem...
By Perfect Hair Health TeamNov 8, 2025Nutrafol Review: Half-Truths, Cherrypicked Data, & Misleading Study Results
Nutrafol is a hair loss supplement praised by media, endorsed by doctors, and supported by clinical studies. At first glance, it seems like the perfect option for anyone interesting in fighting hair loss naturally. Unfortunately, during our investigation, we found that (1) Nutrafol’s 2018 clin...
By Perfect Hair Health TeamNov 8, 2025Microneedling For Hair Loss: What’s The Best Needle Size?
When it comes to microneedling for hair regrowth, researchers aren’t yet sure which needle size elicits the best results. In clinical studies, needle lengths of 0.6mm to 2.5mm (used once weekly or bi-weekly) have been shown to improve hair counts in men with androgenic alopecia (AGA). Even sti...
By Perfect Hair Health TeamNov 8, 2025Oral Minoxidil: What’s The Best Dose (mg) For Men With Pattern Hair Loss?
Oral minoxidil improves hair growth in men with androgenic alopecia (AGA), with dosages of 0.25mg, 2.5mg, and 5.0mg showing positive effects. But the higher the dose, the higher your risk of side effects: namely, body hair growth and lower limb edema (swelling). So, which dose is best for you? While...
By Perfect Hair Health TeamNov 8, 2025Rosemary Oil For Hair Loss? Not So Fast… (See Photos)
In 2015, a clinical study showed that rosemary oil improved pattern hair loss and was just as effective as 2% minoxidil (Rogaine®). Since then, interest in rosemary oil has exploded – with many hair loss sufferers switching from Rogaine® to rosemary as a more natural solution. But is this a good mov...
By Perfect Hair Health TeamNov 4, 20255 Natural DHT Blockers… But Should You Use Them?
Natural DHT blockers are popular among hair loss sufferers who want to lower DHT without the use of drugs. Unfortunately, most natural DHT reducers lack enough DHT-reducing capabilities to regrow hair. This article separates fact from fiction to reveal the best (and worst) natural DHT blockers for p...
By Perfect Hair Health TeamSep 24, 2025Topical Dutasteride Before and After: 10 Successes
Recent clinical data show that topical dutasteride offers promising hair regrowth and reduced side effects, but results vary widely, and more research is needed. Learn how to interpret anecdotal stories, set realistic goals, and combine therapies for the best outcomes....
By Sarah King, PhDSep 18, 2025Does Topical Dutasteride Work?
Topical dutasteride is gaining attention as a potent alternative to oral dutasteride (and finasteride) in treating androgenic alopecia, aiming to deliver robust DHT suppression at the scalp with fewer systemic side effects. But does topical dutasteride work? In this article, we break down how topica...
By Sarah King, PhDSep 16, 2025Where to Buy Topical Finasteride?
Topical finasteride is gaining traction as a lower-risk alternative to oral finasteride, especially for those concerned about systemic side effects. In the U.S., providers like Ulo and Strut stand out for customization and lab-tested purity. Canadian options include Xyon Health and Essential Clinic,... - Mission Statement
 Scroll Down
Scroll Down More
More More
More