- About
- Mission Statement
Education. Evidence. Regrowth.
- Education.
Prioritize knowledge. Make better choices.
- Evidence.
Sort good studies from the bad.
- Regrowth.
Get bigger hair gains.
Team MembersPhD's, resarchers, & consumer advocates.
- Rob English
Founder, researcher, & consumer advocate
- Research Team
Our team of PhD’s, researchers, & more
Editorial PolicyDiscover how we conduct our research.
ContactHave questions? Contact us.
Before-Afters- Transformation Photos
Our library of before-after photos.
- — Jenna, 31, U.S.A.
I have attached my before and afters of my progress since joining this group...
- — Tom, 30, U.K.
I’m convinced I’ve recovered to probably the hairline I had 3 years ago. Super stoked…
- — Rabih, 30’s, U.S.A.
My friends actually told me, “Your hairline improved. Your hair looks thicker...
- — RDB, 35, New York, U.S.A.
I also feel my hair has a different texture to it now…
- — Aayush, 20’s, Boston, MA
Firstly thank you for your work in this field. I am immensely grateful that...
- — Ben M., U.S.A
I just wanted to thank you for all your research, for introducing me to this method...
- — Raul, 50, Spain
To be honest I am having fun with all this and I still don’t know how much...
- — Lisa, 52, U.S.
I see a massive amount of regrowth that is all less than about 8 cm long...
Client Testimonials150+ member experiences.
 Scroll DownPopular Treatments
Scroll DownPopular Treatments- Treatments
Popular treatments. But do they work?
- Finasteride
- Oral
- Topical
- Dutasteride
- Oral
- Topical
- Mesotherapy
- Minoxidil
- Oral
- Topical
- Ketoconazole
- Shampoo
- Topical
- Low-Level Laser Therapy
- Therapy
- Microneedling
- Therapy
- Platelet-Rich Plasma Therapy (PRP)
- Therapy
- Scalp Massages
- Therapy
 More
More
IngredientsTop-selling ingredients, quantified.
- Saw Palmetto
- Redensyl
- Melatonin
- Caffeine
- Biotin
- Rosemary Oil
- Lilac Stem Cells
- Hydrolyzed Wheat Protein
- Sodium Lauryl Sulfate
 More
More
ProductsThe truth about hair loss "best sellers".
- Minoxidil Tablets
Xyon Health
- Finasteride
Strut Health
- Hair Growth Supplements
Happy Head
- REVITA Tablets for Hair Growth Support
DS Laboratories
- FoliGROWTH Ultimate Hair Neutraceutical
Advanced Trichology
- Enhance Hair Density Serum
Fully Vital
- Topical Finasteride and Minoxidil
Xyon Health
- HairOmega Foaming Hair Growth Serum
DrFormulas
- Bio-Cleansing Shampoo
Revivogen MD
- more
Key MetricsStandardized rubrics to evaluate all treatments.
- Evidence Quality
Is this treatment well studied?
- Regrowth Potential
How much regrowth can you expect?
- Long-Term Viability
Is this treatment safe & sustainable?
Free Research- Free Resources
Apps, tools, guides, freebies, & more.
- Free CalculatorTopical Finasteride Calculator
- Free Interactive GuideInteractive Guide: What Causes Hair Loss?
- Free ResourceFree Guide: Standardized Scalp Massages
- Free Course7-Day Hair Loss Email Course
- Free DatabaseIngredients Database
- Free Interactive GuideInteractive Guide: Hair Loss Disorders
- Free DatabaseTreatment Guides
- Free Lab TestsProduct Lab Tests: Purity & Potency
- Free Video & Write-upEvidence Quality Masterclass
- Free Interactive GuideDermatology Appointment Guide
- More
Articles100+ free articles.
-
Which Hormones Cause Hair Loss in Females?
-
Does Zepbound Cause Hair Loss?
-
Does Wegovy Cause Hair Loss?
-
Strut Health Review: 5 Things to Consider Before Purchasing
-
Does Tirzepatide Cause Hair Loss?
-
Musely Reviews for Hair Loss: Are They Trustworthy?
-
Best Minoxidil for Women: Top 6 Brands of 2026
-
Best Topical Finasteride: 5 Top Products of 2026
PublicationsOur team’s peer-reviewed studies.
- Microneedling and Its Use in Hair Loss Disorders: A Systematic Review
- Use of Botulinum Toxin for Androgenic Alopecia: A Systematic Review
- Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia
- Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results
- A Hypothetical Pathogenesis Model For Androgenic Alopecia:Clarifying The Dihydrotestosterone Paradox And Rate-Limiting Recovery Factors
Menu- AboutAbout
- Mission Statement
Education. Evidence. Regrowth.
- Team Members
PhD's, resarchers, & consumer advocates.
- Editorial Policy
Discover how we conduct our research.
- Contact
Have questions? Contact us.
- Before-Afters
Before-Afters- Transformation Photos
Our library of before-after photos.
- Client Testimonials
Read the experiences of members
Before-Afters/ Client Testimonials- Popular Treatments
-
ArticlesMicroneedling For Hair Loss: What’s The Best Needle Size?
First Published Nov 8 2025Last Updated Nov 9 2025Natural Remedies Researched & Written By:Perfect Hair Health Team
Researched & Written By:Perfect Hair Health Team Reviewed By:Rob English, Medical Editor
Reviewed By:Rob English, Medical Editor
Want help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Learn MoreArticle Summary
When it comes to microneedling for hair regrowth, researchers aren’t yet sure which needle size elicits the best results. In clinical studies, needle lengths of 0.6mm to 2.5mm (used once weekly or bi-weekly) have been shown to improve hair counts in men with androgenic alopecia (AGA). Even still, there’s debate over whether shorter needle lengths (used more frequently) might lead to better results. Read on to see the evidence, mechanisms, photos, theories, and results.
Full Article
Microneedling: a powerful, under-researched hair loss therapy
In the last five years, microneedling therapies have exploded in popularity – especially among hair loss sufferers.
Research now shows that microneedling can increase hair counts by 15%. And as clinical evidence for microneedling continues to grow, so do the devices available to consumers: microneedle rollers, microneedle stamps, and even automated needling devices – with needle lengths ranging from 0.25mm to 2.5mm (and higher).
But with microneedling research still in its infancy, there’s one big question that researchers have yet to answer:
When it comes to treating pattern hair loss, what’s the best microneedling needle length? 0.25mm? 0.5mm? 1.0mm? 1.5mm? 2.0mm? Higher?
Despite what microneedling manufacturers tell you, there is no clear-cut answer.
Rather, the evidence indicates that when it comes to treating pattern hair loss, the right microneedling needle length is highly contextual. It depends on (1) how frequently you plan on microneedling and (2) whether you’re combining microneedling with other treatments.
This article dives into the research to uncover the evidence, and how to best position yourself for hair regrowth if you decide to start microneedling.
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.

What is microneedling?
Microneedling is a stimulation-based therapy for hair loss. Similar to platelet-rich plasma therapy and massaging, microneedling leverages acute wounding in balding scalp skin (via medical-grade needles) to evoke growth factors. Over time, these growth factors may help to (1) promote the formation of new blood vessels, (2) reduce the appearance of scar tissue, and (3) promote hair follicle proliferation.
Yes, the therapy hurts. And yes, microneedlers look like small medieval torture devices.
A microneedle roller used for hair loss

But despite the pain involved in therapy, microneedling – when repeated once or twice-weekly, and for 3-6 months – have been shown to greatly improve hair growth in men with androgenic alopecia (AGA).{{https://link.springer.com/article/10.1007/s13555-021-00653-2}}
Just see the results of this 2017 study, which demonstrated hair count improvements of ~15% for those using microneedling devices without any other treatments.
Microneedling for AGA: results over six months (bi-weekly sessions)

Or the results of this 2013 study, which found that microneedling enhanced the regrowth achieved from 5% minoxidil by 400%.
Microneedling + 5% minoxidil for AGA: results over three months (weekly sessions)

In short: microneedling is effective at improving pattern hair loss (AGA) in men. But questions still remain as to its best practices. Questions like:
- How far apart should we space our sessions? Daily? Weekly? Monthly?
- How long should our sessions be? Five minutes? Ten? Twenty?
- What’s the best needle count? 192 needles? 540 needles? More?
- What’s the best needle length? 0.25 mm? 1.0 mm? 2.0 mm? More?
…and many more.
The truth is that it’s impossible to answer any one of these questions without answering the others. After all, these questions are all interlinked. The smaller the needle length, the quicker your healing, the more frequently you can microneedle. And the higher your number of needles, the more inflammation you can evoke, and the shorter your sessions can be.
Having said that, the best needle length debate might be answerable by itself. Why? Because at different needle lengths, microneedling has different effects.
Here’s why.
Microneedling needle lengths: different puncture depths, different effects on the hair follicles
Our scalp skin consists of three main layers: the epidermis, dermis, and hypodermis (i.e., subcutaneous layer).
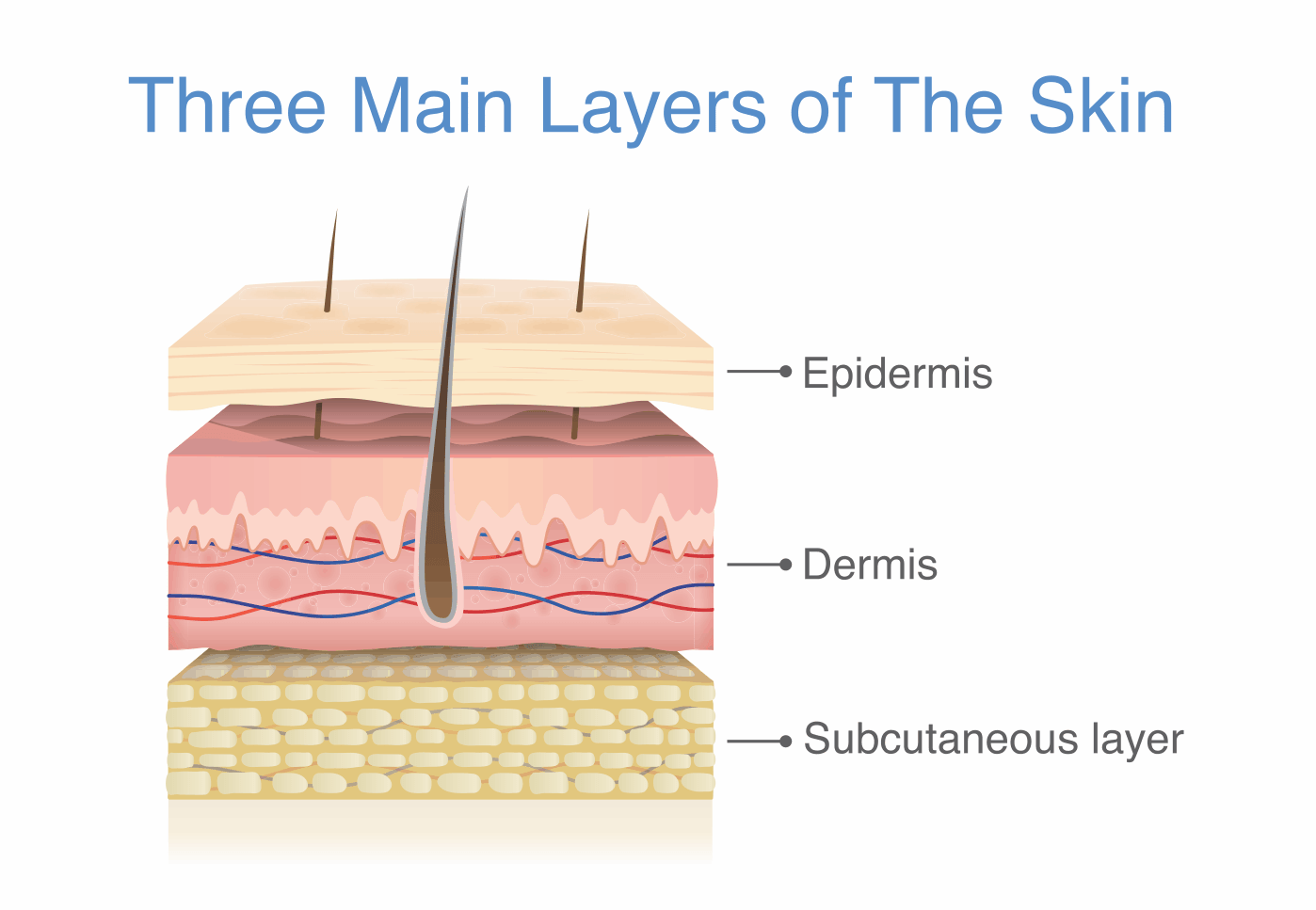
The thickness of our scalp (and its subcomponents) is influenced by our age, gender, and degree of balding. But in general, our scalp skin is just 5mm to 6mm thick.
Within that skin, our epidermis is usually less than 0.5mm thick, our dermis is 1-2mm thick, and our subcutaneous layer is 3mm thick.
This has significant relevance to microneedling needle lengths. Why? Because the depths at which these needles puncture our scalps has a direct influence over which regions of the hair follicles we will stimulate.
Needle lengths of 0.25 mm to 0.5 mm may improve topical absorption
At shorter needle depths (i.e., 0.25mm to 0.5mm), microneedling only wounds the top layers of the skin (the epidermis). This will improve the absorption of topicals (i.e., minoxidil). However, these shallower depths likely won’t evoke the growth factors necessary to encourage hair follicle proliferation. For this effect to occur, we need to incur wounds deeper – specifically, we need to wound the dermis.
Needle lengths of 1.5 mm to 2.5 mm may evoke growth factors for hair follicle proliferation
At longer needle depths (i.e., 1.5mm to 2.5mm), microneedling needles will puncture the dermis of our scalp skin. This has important ramifications to hair follicle proliferation, because the dermis is where the hair follicle stem cell bulge resides. It’s also where there are vascular networks – such that punctures at this depth ofte lead to swelling and/or pinpoint bleeding.
What is the hair follicle stem cell bulge?
The hair follicle stem cell bulge is located 1.0 mm to 1.8 mm deep in our scalp skin near the isthmus (upper third) of the hair follicle – and can usually be found at the base of the arrector pili muscle.
This hair follicle stem cell bulge is sort of like the “source material” for a hair follicle. These stem cells help replenish and repopulate the cells that constitute each hair follicle. If a hair follicle’s stem cell population is completely depleted, hair follicles can no longer replace old cells, and the hair follicles will stop proliferating (or growing).
Hair follicle stem cell bulge
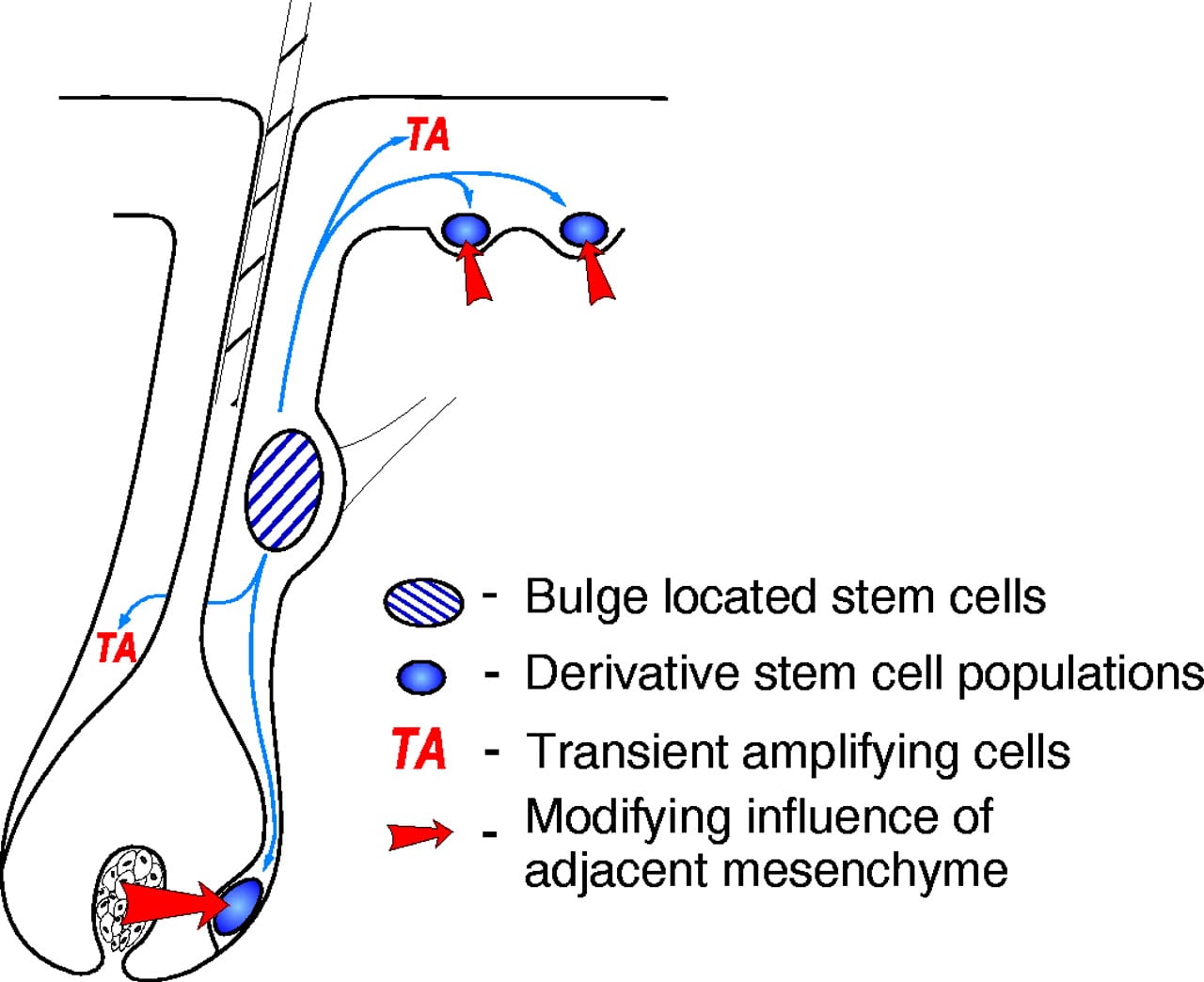
Interestingly, we can stimulate these stem cells via wounding. If wounds are incurred surrounding these stem cell bulges, the growth factors stimulated during wounding can even signal to these hair follicle stem cells to initiate a new anagen phase of the hair cycle.
For pattern hair loss sufferers, this often means increases to hair counts within the realms of 15% – and that’s without any other therapies. That’s an impressive improvement. But again, it bears repeating…
We only see these hair count increases from studies using microneedling devices (by themselves) that puncture 1.5mm to 2.5mm deep. In other words, we only see these hair count increases at microneedling lengths that stimulate the hair follicle stem cell bulge.
Long-story short: we likely need to microneedle at depths of 1.5mm to 2.5mm if we’re to expect appreciable stimulation of the hair follicle stem cell bulge, and thereby appreciable hair follicle proliferation (i.e., hair regrowth).
Now, it’s worth noting that studies testing microneedling as a monotherapy have only ever investigated needle lengths of 1.5mm and greater. So, the absence of evidence should not imply evidence against shorter needle lengths. But we also have to make recommendations based on what is known, not postulated. So, consider these limitations as you keep reading.
So, should we all microneedling at needle lengths of 1.5mm or greater?
Not necessarily.
When it comes to needle depths, there is an upper limit. Specifically, we want to avoid puncturing something called an emissary vein.
Emissary veins are bi-directional blood vessels that run from the scalp’s hypodermis (i.e., muscle tissues) through the cranium (i.e., skull bone) and into the brain. When brain infections occur following scalp injuries, they are almost always the result of a puncture to the emissary vein – as an open emissary vein can allow pathogenic bacteria from the epidermis to bypass the skull plate and migrate directly into brain tissues. This can cause serious health ramifications, and even death.
Emissary veins aren’t everywhere on the scalp. And in general, they’re located at depths deeper than 5mm – at the bottom edges of the hypodermis.
There’s no reason for us to risk wounding an emissary vein via microneedling – especially because we can stimulate the hair follicle stem cell bulge at shallower depths (i.e., 1.5 mm to 2.5 mm).
Moreover, the studies that we do have on microneedling for pattern hair loss don’t test needle lengths above 2.5mm. So, don’t deviate from what is clinically supported; don’t go deeper than needle lengths of 2.5mm.
So, now that we’ve established a lower and upper limit for mironeedling needle lengths, let’s revisit that question: which needle length is best for regrowing hair?
Microneedling for hair growth: what’s the best needle length?
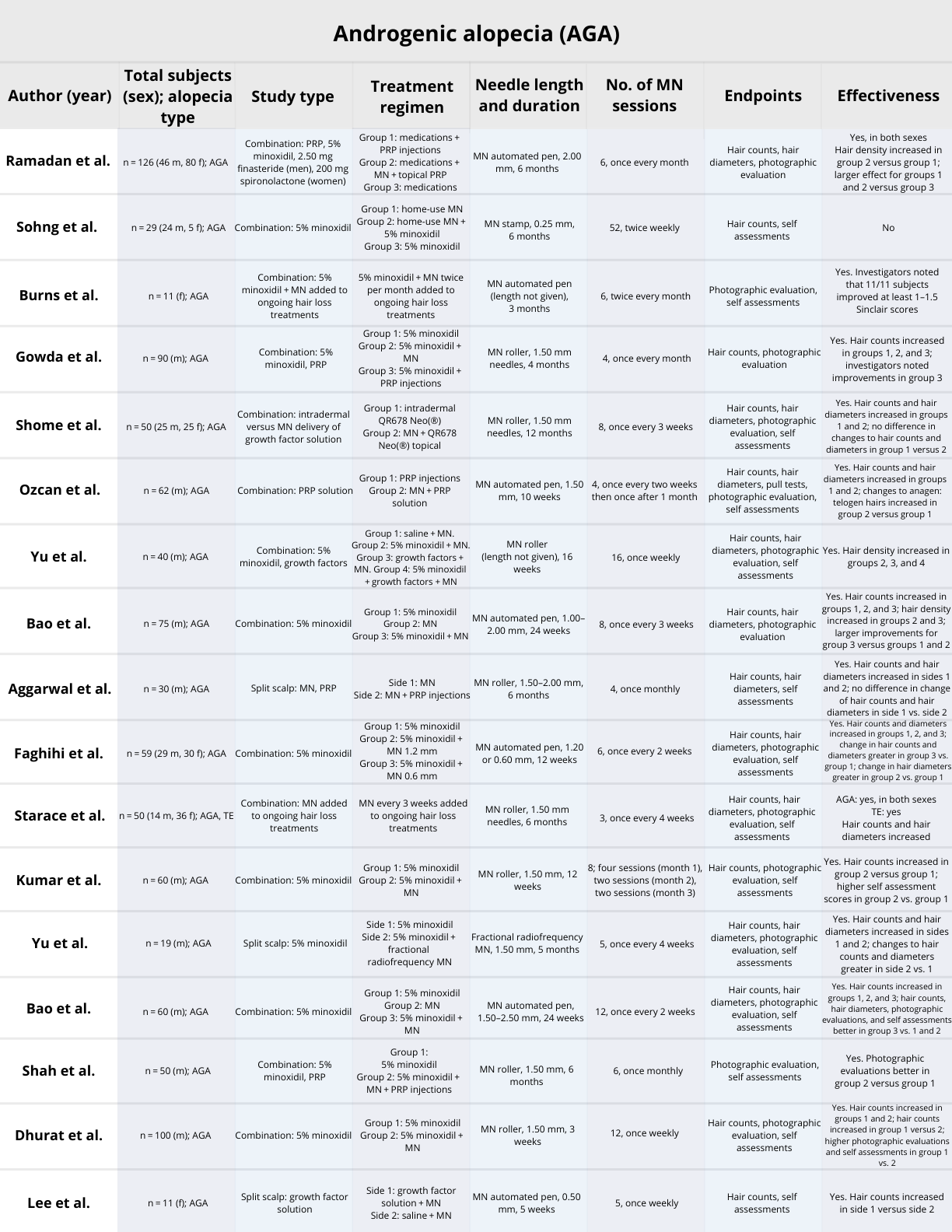
Since microneedling research is still in its infancy, we don’t yet know the best needle length. But we can give you a general idea of the best needle lengths based on the clinical studies on microneedling published so far.{{https://link.springer.com/article/10.1007/s13555-021-00653-2}}
- In a 2013 study, participants used 5% minoxidil twice-daily alongside microneedling with a 1.5mm needle roller once-weekly. Over three months, the author (Dr. Dhurat) found that the 1.5mm needle roller improved hair regrowth from minoxidil by 400%.
- In a 2015 study, participants used minoxidil and finasteride daily alongside microneedling with a 1.5mm needler roller either once-weekly or twice-weekly. After six months, the researchers found significant increases to hair counts. (5)
- In a 2017 study, participants used 5% minoxidil alongside a 1.5mm to 2.5mm automated needler once every two weeks. Over six months, the investigators found comparable hair count increases to that of Dr. Dhurat’s 2013 study. They also found that microneedling alone improved hair counts by ~15%.
- In a 2020 study, participants applied 5% minoxidil twice daily and microneedled once every two weeks with either a 0.6mm or 1.2mm needle length roller for 12 weeks. They found that microneedling with either length was more effective than 5% minoxidil twice daily by itself. In terms of statistical significance, the study showed that there was no statistical difference between the two lengths with respect to improved hair counts: in conjunction with minoxidil, the 1.2mm needle improved hair counts by about 15% while the 0.6mm needle improved hair counts by about 19%.
But these aren’t the only studies done on microneedling for hair loss. There are many more, which we’ve discussed in our systematic review on the subject (recently published in Dermatology and Therapy).{{https://link.springer.com/article/10.1007/s13555-021-00653-2}}
What do all of the studies tell us?
- So far, we’ve clinically tested microneedle lengths from 0.25mm to 2.5mm for men with androgenic alopecia (AGA).
- However, only needle lengths of 1.5mm to 2.5mm were tested as a monotherapy (i.e., not in conjuction with minoxidil or other treatments).
- At depths of 0.6mm to 2.5mm, microneedling is suspected to increase both topical absorption (with minoxidil) and hair follicle proliferation (as a standalone treatment).
And while the 2020 study demonstrates shorter needle lengths may produce results comparable to longer needle lengths (at least with respect to hair counts), the majority of evidence still supports the use of a 1.5mm to 2.5mm needle length.
The rationale? There are two factors to the depth of penetration when using microneedles: needle length and applied pressure. In earlier studies, 1.5mm needles were used to evoke erythema (skin redness) whereas, in the 2020 study, the authors aimed to evoke bleeding.
This is an important distinction to make.
Because evoking bleeding involves more pressure than just evoking erythema, it’s possible that both the 2020 study (using 0.6mm and 1.2mm needles) and the earlier studies (using 1.5mm needle lengths) penetrated to similar depths — simply due to differences in applied pressure.
The equation also gets more complicated when we evaluate not just “session endpoints”, but also the fact that microneedling rollers versus automated pens puncture at different depths in the scalp skin… even when controlling for the same exact needle length.
Why? Because microneedling rollers “roll” the needles onto the skin. That means the depth those needles actually penetrate is subject to angulation changes and user pressure variability (i.e., how hard someone presses down). However, with automated microneedling pens, studies suggest that needling penetration depths near-perfectly match needle lengths (up to 1.5mm, at least).
Resultantly, the best data we have suggest that microneedling rollers penetrate, on average, just 50-75% of their actual needle length. This makes it even more difficult to make needle length recommendations, because the actual microneedling device influences the answer.
What can be gleaned from all of the data?
Taking into account session endpoints, device differences, hypothetical mechanisms, and clinical outcomes from our latest systematic literature review on microneedling for hair loss, here are the needle lengths we currently recommend:
- Microneedling roller. Use a 1.0-1.5mm needle length.
- Microneedling automated pen. Use a 0.6-0.8mm needle length.
These recommendations will hopefully improve topical absorption, stimulate growth factors linked to hair follicle proliferation, and minimize any concerns over infection or the puncturing of short an emissary vein.
Moreover, stick with needling once weekly, or once every two weeks. Again, it’s clinically effective. Other recommendations on other websites are theoretical, anecdotal, and generally unsubstantiated.
What about microneedling every day with a 0.25 mm or 0.5 mm needle length?
As stated earlier, it’s important to note that the absence of evidence does not imply evidence against any treatment protocol.
In other words, just because we don’t have studies trialing needle lengths smaller than 1.5mm for pattern hair loss (as a standalone treatment), this does not mean that smaller needle lengths are ineffective. It’s just that evidence supporting smaller needle lengths is unsubstantiated.
There are some YouTube personalities claiming to see great microneedling results from microneedling nightly with a 0.25mm and then immediately applying topicals. There are some men on HairLossTalk who are demonstrating results from microneedling every night with a 1.0mm roller.
There may be some benefits to microneedling more frequently – particularly if you’re also using a topical. For example, due to the relatively short half-life of topical minoxidil, users must apply minoxidil twice-daily in order to elicit a significant effect on miniaturizing hair follicles. Microneedlers with needle lengths of 0.25mm to 0.5mm help to increase topical absorption. Moreover, because these needle lengths typically only puncture the epidermis, they can be used more frequently (i.e., once daily) versus microneedlers with needle lengths of 1.5mm+ (i.e., once every week or more).
Thus, some might argue that daily microneedling with a smaller needle length might help to more regularly promote topical absorption, and that this benefit might outweigh the stimulation of growth factors elicited from needle depths of 1.5mm and beyond.
But again, these stories are just anecdotes; and the rationales behind shorter needle lengths and more frequent needling are just hypothetical. While we do have people trialing augmented microneedling lengths and schedules in our membership community (with great success), we can’t yet extrapolate their results to what all pattern hair loss sufferers should expect.
Long story short: until these anecdotes stand the test of a clinical trial, we must make our recommendations based on the evidence already available… and that means recommending a 1.5mm to 2.5mm needle length.
The bottom line: for now, stick with 0.6-0.8mm needle lengths for automated pens, and 1.0-1.5mm needle lengths for rollers
These needle lengths are what worked in clinical trials, and they seem to be working well for the people inside of our membership site.
Questions? Comments? Please reach out in the comments section.
Want help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Learn More
Perfect Hair Health Team
"... Can’t thank @Rob (PHH) and @sanderson17 enough for allowing me to understand a bit what was going on with me and why all these [things were] happening ... "

 — RDB, 35, New York, U.S.A.
— RDB, 35, New York, U.S.A."... There is a lot improvement that I am seeing and my scalp feel alive nowadays... Thanks everyone. "

 — Aayush, 20’s, Boston, MA
— Aayush, 20’s, Boston, MA"... I can say that my hair volume/thickness is about 30% more than it was when I first started."

 — Douglas, 50’s, Montréal, Canada
— Douglas, 50’s, Montréal, CanadaWant help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Join Now - Mission Statement
