- About
- Mission Statement
Education. Evidence. Regrowth.
- Education.
Prioritize knowledge. Make better choices.
- Evidence.
Sort good studies from the bad.
- Regrowth.
Get bigger hair gains.
Team MembersPhD's, resarchers, & consumer advocates.
- Rob English
Founder, researcher, & consumer advocate
- Research Team
Our team of PhD’s, researchers, & more
Editorial PolicyDiscover how we conduct our research.
ContactHave questions? Contact us.
Before-Afters- Transformation Photos
Our library of before-after photos.
- — Jenna, 31, U.S.A.
I have attached my before and afters of my progress since joining this group...
- — Tom, 30, U.K.
I’m convinced I’ve recovered to probably the hairline I had 3 years ago. Super stoked…
- — Rabih, 30’s, U.S.A.
My friends actually told me, “Your hairline improved. Your hair looks thicker...
- — RDB, 35, New York, U.S.A.
I also feel my hair has a different texture to it now…
- — Aayush, 20’s, Boston, MA
Firstly thank you for your work in this field. I am immensely grateful that...
- — Ben M., U.S.A
I just wanted to thank you for all your research, for introducing me to this method...
- — Raul, 50, Spain
To be honest I am having fun with all this and I still don’t know how much...
- — Lisa, 52, U.S.
I see a massive amount of regrowth that is all less than about 8 cm long...
Client Testimonials150+ member experiences.
 Scroll DownPopular Treatments
Scroll DownPopular Treatments- Treatments
Popular treatments. But do they work?
- Finasteride
- Oral
- Topical
- Dutasteride
- Oral
- Topical
- Mesotherapy
- Minoxidil
- Oral
- Topical
- Ketoconazole
- Shampoo
- Topical
- Low-Level Laser Therapy
- Therapy
- Microneedling
- Therapy
- Platelet-Rich Plasma Therapy (PRP)
- Therapy
- Scalp Massages
- Therapy
- More
IngredientsTop-selling ingredients, quantified.
- Saw Palmetto
- Redensyl
- Melatonin
- Caffeine
- Biotin
- Rosemary Oil
- Lilac Stem Cells
- Hydrolyzed Wheat Protein
- Sodium Lauryl Sulfate
- More
ProductsThe truth about hair loss "best sellers".
- Minoxidil Tablets
Xyon Health
- Finasteride
Strut Health
- Hair Growth Supplements
Happy Head
- REVITA Tablets for Hair Growth Support
DS Laboratories
- FoliGROWTH Ultimate Hair Neutraceutical
Advanced Trichology
- Enhance Hair Density Serum
Fully Vital
- Topical Finasteride and Minoxidil
Xyon Health
- HairOmega Foaming Hair Growth Serum
DrFormulas
- Bio-Cleansing Shampoo
Revivogen MD
- more
Key MetricsStandardized rubrics to evaluate all treatments.
- Evidence Quality
Is this treatment well studied?
- Regrowth Potential
How much regrowth can you expect?
- Long-Term Viability
Is this treatment safe & sustainable?
Free Research- Free Resources
Apps, tools, guides, freebies, & more.
- Free CalculatorTopical Finasteride Calculator
- Free Interactive GuideInteractive Guide: What Causes Hair Loss?
- Free ResourceFree Guide: Standardized Scalp Massages
- Free Course7-Day Hair Loss Email Course
- Free DatabaseIngredients Database
- Free Interactive GuideInteractive Guide: Hair Loss Disorders
- Free DatabaseTreatment Guides
- Free Lab TestsProduct Lab Tests: Purity & Potency
- Free Video & Write-upEvidence Quality Masterclass
- Free Interactive GuideDermatology Appointment Guide
- More
Articles100+ free articles.
-
Which Hormones Cause Hair Loss in Females?
-
Does Zepbound Cause Hair Loss?
-
Does Wegovy Cause Hair Loss?
-
Strut Health Review: 5 Things to Consider Before Purchasing
-
Does Tirzepatide Cause Hair Loss?
-
Musely Reviews for Hair Loss: Are They Trustworthy?
-
Best Minoxidil for Women: Top 6 Brands of 2026
-
Best Topical Finasteride: 5 Top Products of 2026
PublicationsOur team’s peer-reviewed studies.
- Microneedling and Its Use in Hair Loss Disorders: A Systematic Review
- Use of Botulinum Toxin for Androgenic Alopecia: A Systematic Review
- Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia
- Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results
- A Hypothetical Pathogenesis Model For Androgenic Alopecia:Clarifying The Dihydrotestosterone Paradox And Rate-Limiting Recovery Factors
Menu- AboutAbout
- Mission Statement
Education. Evidence. Regrowth.
- Team Members
PhD's, resarchers, & consumer advocates.
- Editorial Policy
Discover how we conduct our research.
- Contact
Have questions? Contact us.
- Before-Afters
Before-Afters- Transformation Photos
Our library of before-after photos.
- Client Testimonials
Read the experiences of members
Before-Afters/ Client Testimonials- Popular Treatments
-
ArticlesDiffuse Thinning: Causes, Implications, And Steps For Regrowth (See Photos)
First Published Jan 10 2020Last Updated Sep 19 2025Miscellaneous Researched & Written By:Perfect Hair Health Team
Researched & Written By:Perfect Hair Health Team
Want help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Learn MoreArticle Summary
Diffuse thinning is a presentation of hair loss linked to androgenic alopecia, stress, and a variety of chronic conditions. If you’re dealing with diffuse hair loss, this article reveals its common causes, and a step-by-step guide toward identifying which causes are most relevant to you. The good news: diffuse hair loss is often reversible. We’ve got the reader case studies (with photos) to prove it.
Full Article
A complete guide to diffuse hair loss
Diffuse thinning isn’t a type of hair loss. Rather, it’s a term used to describe the appearance of someone’s hair loss.
When someone has diffuse hair loss, it means that they’re experiencing a decrease in hair density across the entire scalp. Many people first notice diffuse thinning as a wider part, a thinner ponytail, or after seeing more scalp skin following a haircut.
In this article, we’ll uncover what diffuse thinning is, what causes it, and what can we can do about it.
For what it’s worth, I’m intimately familiar with this presentation of hair loss. It was part of my hair loss diagnosis back in 2007. At the time, my dermatologist diagnosed me with male pattern hair loss, also known as androgenic alopecia (AGA). He also attributed my diffuse thinning exclusively to AGA.
What I didn’t learn (until years later) is that diffuse thinning isn’t just linked to AGA; it’s also associated with dozens of underlying chronic conditions – hypothyroidism, heavy metal toxicities, nutrient deficiencies, and more – each of which has a unique set of causes, and a unique set of treatments.
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.

Consequently, diffuse thinners are at a high risk of getting diagnosed with the wrong type of hair loss… because their hair loss presentation overlaps with so many different causes.
If I’d known this – and if I’d known how to troubleshoot which underlying drivers of diffuse hair loss were relevant to me – I could’ve saved myself a lot of time, money, and hair.
That’s why I’ve written this article – to help you avoid my mistakes. By the end, you’ll learn:
- The major causes of diffuse thinning (and the ones commonly missed by doctors)
- Ways to identify which causes might be relevant to your diffuse thinning
- Why it’s critical to test first, treat second (Ben M.’s story)
- How there may be an “order of operations” for reversing diffuse hair loss, at least if we suspect multiple causes
The good news? If we can properly identify and address the underlying causes of diffuse thinning, we can often see full hair loss reversals. We’ve got case reports from the scientific literature – and the case studies from readers – to prove it.
More on this below.
What is diffuse thinning?
Diffuse thinning is a term used to describe a decrease to hair density across the entire scalp. This can happen as a result of:
- Each individual hair strand getting thinner (i.e., hair follicle miniaturization). As each hair grows thinner, this creates the appearance of general thinning everywhere.
- An increase in hair shedding (i.e., a decrease in the total number of hairs on the scalp). If we’re constantly shedding more hair than we’re replacing, then over time, we lose hair density.
In either case, diffuse hair loss leads to thinner-looking hair, with more scalp showing (particularly when the hair is parted).
Diffuse thinning in a female scalp

What causes diffuse hair loss?
The causes of diffuse thinning are widespread. Here are some of the most common culprits:
- Genetics & hormonal imbalances. Diffuse hair loss can occur from due to polycystic ovarian syndrome or menopause in women, and/or pattern hair loss in both men and women.
- Stress. This includes mental, emotional, and physiological stress – childbirth, illness, surgery, chronic anxiety, and even physical exhaustion.
- Chronic conditions. Diffuse thinning is often observed alongside conditions like hypothyroidism, hyperparathyroidism, gut dysbiosis, nutrient deficiencies & surpluses, and heavy metal toxicities (more on these later).
How do I identify my unique causes of diffuse thinning?
The short-answer: it’s complicated.
There are many types of hair loss, and each type has a different set of causes, and a different set of treatments. If we apply the wrong set of treatments to the wrong set of causes, we won’t see much regrowth.
So, how can we go about identifying the causes of diffuse hair loss? In reality, there are two approaches.
Approach #1: visit a qualified dermatologist
The first approach is to find a qualified dermatologist who (1) specializes in hair loss disorders, and (2) conducts full health evaluations. This health examination may include self-assessment questionnaires and a range of lab tests. This would allow for a highly trained individual to vet the appearance of our hair loss against our health history – and tell us which causes of diffuse thinning might be most pertinent to us.
Unfortunately, it’s difficult to find a dermatologist who does this.
For starters, not all dermatologists are involved in the “academic” side of their field. As such, many are years behind the literature on how to best diagnose and/or treat certain hair disorders.
Secondly, dermatologists have to run a business. This means they can’t spend an hour with every patient. So, they ask patients the minimum number of questions to get them 80% of the information they need to ascertain a diagnosis. This works well for maximizing patient visits and revenue; it doesn’t always work well for the patient with a complicated case of hair loss.
Lastly, insurance companies are frugal; they limit the lab tests you can order for patients. So, even if a dermatologist wanted to get more specific in their diagnosis by ordering lab work, health insurance may not let them do so.
All of this is to the detriment of the person sitting in their chair – their patient.
I would know; I’ve personally experienced all of this during my visit with a dermatologist to investigate my diffuse thinning, and my subsequent hair loss diagnosis.
When a dermatologist falls short of the right hair loss diagnosis (my story)
In 2007, I noticed a significant amount of hair loss. I experienced very slight temple recession, but significant hair loss at the crown and to my overall hair density. So, I visited a leading dermatologist in Massachusetts to understand what was going on.
Within 15 seconds of combing through my scalp, that dermatologist diagnosed me with androgenic alopecia (AGA) – specifically, AGA in a diffuse pattern as well as crown thinning.
This dermatologist did not ask me about any underlying health questions. I wasn’t asked if I was taking any drugs or supplements; I wasn’t asked if my family had a history of chronic conditions associated with hair loss; I wasn’t given lab work to rule out the possibilities of a thyroid disorder, a vitamin D deficiency, or a heavy metal toxicity from drinking well-water my whole life. (These questions would’ve ruled out other common causes of diffuse thinning.)
Rather, I was handed a diagnosis based exclusively on the presentation of my hair loss: AGA (which happens to be the most common hair loss diagnosis in adult men). If you’re curious, you can see my diagnosis here.
Years later, after investing in thousands of dollars in lab tests, I discovered that my hair loss probably wasn’t exclusively due to AGA. Rather, I likely had AGA alongside chronic telogen effluvium (i.e., diffuse thinning) – the latter of which was linked to subclinical hypothyroidism.
No wonder why interventions for AGA – minoxidil, low-level laser therapy, and saw palmetto – didn’t work for me. I was only treating partly treating the underlying causes of my thinning hair… because I’d only received a partial diagnosis.
Can’t find a good dermatologist? There’s another way!
For those who don’t have access to a top-level dermatologist, there are still ways to help yourself identify why your hair loss is occurring in a diffuse pattern.
It all starts with education.
Specifically, we can employ a DIY-approach to (1) learn about the major causes of diffuse thinning, and then (2) see which causes apply to us as individuals.
Approach #2: learn the major causes of diffuse thinning, and then compare those causes to your own health history and hair loss situation
The rest of this article is designed to help you identify the potential drivers of your diffuse hair loss. It begins with education, and it ends with an action plan to (hopefully) help your hair.
It all starts by diving deeper than diffuse thinning’s appearance – so that we can understand its causes.
Diffuse hair loss: two categories
To reiterate, diffuse hair loss is a term to describe general thinning across the entire top of the scalp. This sort of thinning generally falls into two categories:
- Hair thinning caused by androgenic alopecia (AGA)
- Hair thinning caused by hair shedding disorders
Differentiating between these two types of hair loss is important. After all, each type of hair loss is associated with a different set of causes, and thereby a different set of treatments.
Androgenic alopecia (AGA)
Androgenic alopecia (AGA), also called pattern hair loss, is one of the most commonly diagnosed types of hair loss in the U.S. In fact, some resources estimate that AGA is responsible for up to 95% of hair loss diagnoses in adult men. This is what I was diagnosed with back in 2007.
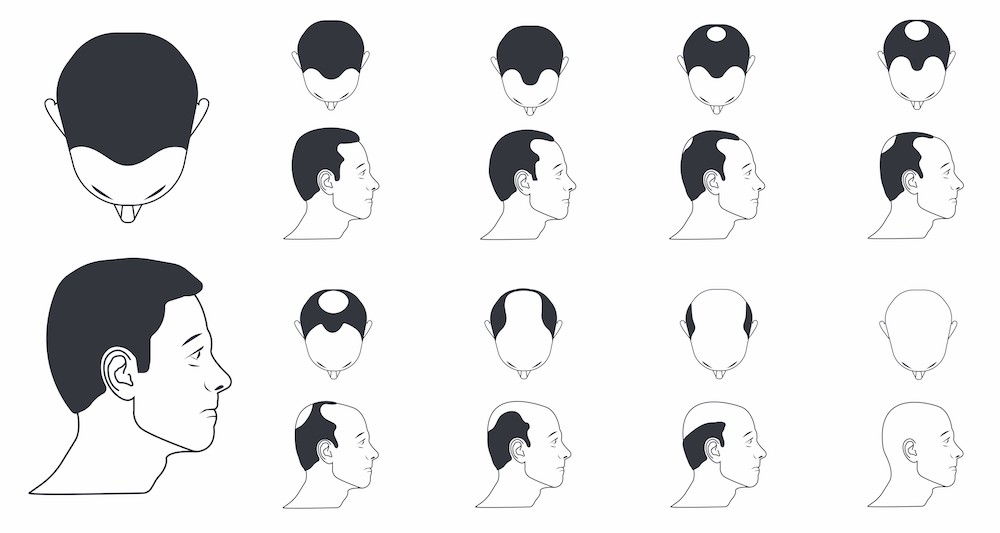
Male pattern hair loss
In men, AGA usually starts from the hair line and/or the crown. This is the reason why terms like “receding hairline” and “bald spots” are common for men with hair loss. This can occur as early as the teen years or early 20s.
Androgenic Alopecia (AGA) Norwood Scale: how AGA progresses in men

But not all AGA cases follow this exact pattern. According to our survey data, 20-40% of men with early-stage pattern hair loss also notice diffuse thinning. So, it’s not uncommon to notice general decreases to hair density that coincide with AGA.
Female pattern hair loss
In contrast to men, the overwhelming majority of women with AGA (female pattern hair loss) don’t notice hairline recession or a bald spot. Rather, they notice an even thinning of hair throughout the top part of the scalp.
Ludwig scale: how AGA progresses in women

The defining characteristic of pattern hair loss: hair follicle miniaturization
Hair follicle miniaturization is when an individual hair strand, over a series of years, gets thinner and thinner. Researchers mainly attribute this phenomenon to a hormone called dihydrotestosterone, or DHT. When DHT comes into contact with scalp hair follicles that are genetically prone hair follicle miniaturization, these hairs begin to shed, and with each hair cycle, come back thinner and thinner.
Hair follicle miniaturization: each hair strand gets thinner

This is important! Why? Because if you’re noticing that when you shed hair, certain hair strands look thinner and wispier than others, then it likely means that you’re dealing with hair follicle miniaturization. By association, this also means that you’re likely dealing with (at least) some degree of androgenic alopecia.
One thing to note about androgenic alopecia: without treatment, this type of hair loss is chronic and progressive. That means that unless you do something about it, it generally will only get worse.
Summary: one way someone can experience diffuse thinning is through hair follicle miniaturization. This is when each hair strand slowly gets thinner over time. Hair follicle miniaturization is almost always caused by androgenic alopecia: a hormonally- and genetically-driven hair loss disorder. Without treatment, hair follicle miniaturization typically only worsens.
Interestingly, hair follicle miniaturization from androgenic alopecia is just one way diffuse thinning can take place. One other way is through a hair shedding disorder. With hair shedding disorders, you’re not losing hair density due to miniaturization; you’re losing hair density due to excessive hair shedding.
More on this below.
Hair shedding disorders
Hair shedding disorders are when there is an imbalance in the hair cycle; specifically, when too many hairs are shedding, and too few hairs are growing in to replace them.
Throughout the course of a day, it’s normal to shed 100-150+ hairs – even in the absence of a hair loss problem. This is because 10-15% of our hair follicles are constantly in a state of shedding, and after shedding, these hair follicles are then replaced by newer, healthier hairs that will grow in.
Under normal circumstances, our scalps maintain a “homeostasis” between the number of shedding versus growing hairs. This way, we never really notice any changes to hair density – as any hairs shed are quickly replaced.
However, hair shedding disorders occur when this balance becomes out-of-whack. Specifically, when too many hairs start shedding and/or too few hairs start growing in to replace them. Under these circumstances, we see a decrease to overall hair density – and due to hair shedding (rather than hair follicle miniaturization).
On that note, there are two main types of hair shedding disorders: telogen effluvium and chronic telogen effluvium.
Telogen effluvium
Telogen effluvium can occur in men and women, but its the most common type of hair shedding disorder in adult women.
Unlike AGA, telogen effluvium is not due to hair miniaturization; it’s due to a disruption in our hair cycle, which leads to an increase in hair shedding, and thereby a decrease to overall hair density. This can occur quickly or slowly, and it can be temporary or chronic.
In any of these scenarios, diffuse thinning might be the way that telogen effluvium presents.
Acute telogen effluvium
Acute telogen effluvium is a kind of telogen effluvium that is temporary, and generally lasts for less than six months. When its triggers are identified and removed, the hair begins to grow back again and its as if the hair shedding never took place.
So, what are these potential triggers? There are several:
- Mental/physical stress. Studies using animals have shown that physical or mental stress can exert inflammation on hair follicles and massive increases to hair shedding. In humans, this stress is often the loss of a loved one (mental/emotional), or giving birth to a child (physical) – both of which can lead to temporary but dramatic increases to hair shedding.
- Crash diets/weight loss. Hair requires both micronutrients and macronutrients to grow. Severe caloric deficits (as in, crash dieting or prolonged calorie restriction for weight loss) can make it difficult to get enough micronutrients and macronutrients to support hair growth – which can trigger hair shedding. In other words, the hair follicles shut down to conserve nutrients for other places in the body that are more necessary for survival than growing hair.
- Medications. The following medications may interfere with the hair follicle’s natural cycling, and have been linked to acute telogen effluvium:
- Antithyroid drugs
- Tricyclic antidepressants such as amitriptyline
- Bromocriptine
- Levodopa
- Cimetidine
- Amphetamines
- Non-steroidal anti-inflammatory drugs (NSAIDs)
- Hormonal contraceptives / hormone replacement therapies
- Anticoagulant medications (rare)
- Beta-blockers (metoprolol and atenolol)
- ACE inhibitors
Now, these are common triggers of temporary hair shedding that lasts for less than six months. So, what about for hair shedding that has lasted longer for six months?
Well, this isn’t always indicative of acute telogen effluvium. Sometimes it can be the beginning of something known as chronic telogen effluvium (or a combination of both). More on this below.
Chronic telogen effluvium
If you find yourself struggling with diffuse shedding for more than six months, and you don’t see signs of hair follicle miniaturization, then you could be suffering from chronic telogen effluvium.
This is the same premise as acute telogen effluvium: the hair follicle changes its normal hair cycling due to some sort of trigger. However, in these cases, the shedding persists for much longer.
If you haven’t experienced diffuse shedding for 6+ months, it doesn’t necessarily mean you have acute telogen effluvium and not chronic telogen effluvium. It’s just the 6-month mark is when most clinicians start to differentiate between the two.
The causes of chronic telogen effluvium are widespread, and oftentimes tied to underlying chronic conditions. We’ll discuss these below (you may also notice some overlap with the causes of acute telogen effluvium, too).
Hypothyroidism
The thyroid is a gland in the next that plays a role in many, many, many different functions of the body. When the thyroid function begins to slow, meaning it produces less thyroid hormone, one of the consequences can be chronic telogen effluvium.
This study found that thyroid hormone (the production of which is impaired in hypothyroidism) interacts with the hair follicle to participate in stem cell function. Thus, it has a direct impact on the follicle’s ability to produce a hair shaft.
It comes as no surprise, then, that many hypothyroidism patients report suffering from varying degrees of hair loss.
Hyperparathyroidism
The parathyroid, which is located near the thyroid, is responsible for secreting a hormone called parathyroid hormone. Its main role is to regulate calcium levels in the body, however, it also acts as a negative regulator of the hair cycle.
This means that, when the parathyroid hormone binds to parathyroid receptors in the hair follicle, hair growth is inhibited. Suffice it to say, too much parathyroid hormone (in a condition called hyperparathyroidism) can precipitate chronic telogen effluvium.
So, if you find yourself suffering from a hair shedding disorder, hyperparathyroidism could be a possible cause.
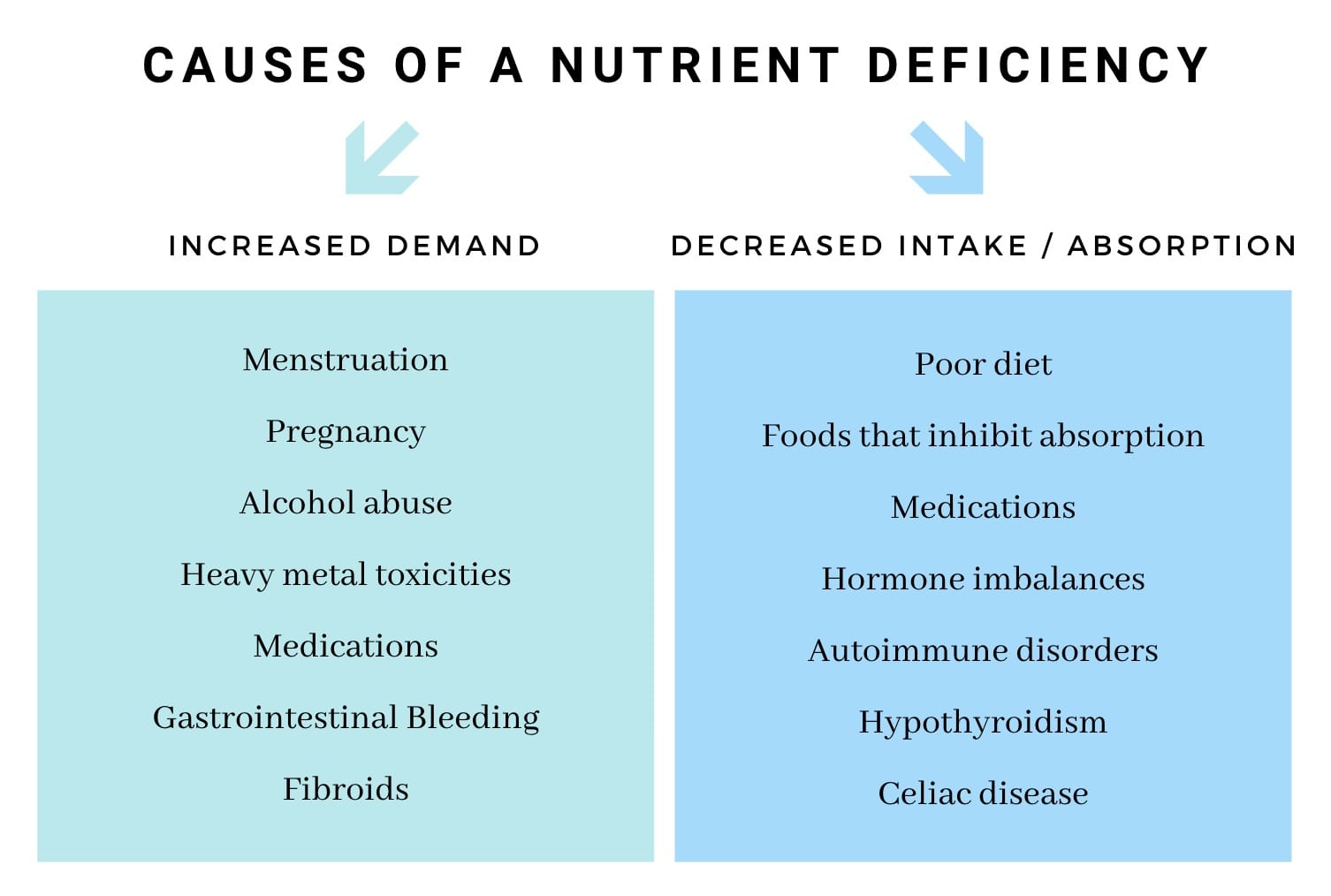
Nutrient deficiencies / surpluses / imbalances
Nutrient deficiencies, surpluses, and imbalances are something that can trigger bouts of hair shedding – particularly when prolonged and severe.
There are a variety of causes of nutrient imbalances, and in general, they all boil down to an imbalance between changed demand for nutrients versus changed supply of nutrients.

Interestingly, there’s a difference between nutrient imbalances that cause acute telogen effluvium versus nutrient imbalances that cause chronic telogen effluvium.
In acute telogen effluvium, these nutrient imbalances are often the result of poor dietary choices. In chronic telogen effluvium, these nutrient imblances are often the result of underlying conditions: malabsorption, copper IUDs, chronic illnesses which increase the demand for nutrients, etc.
In either scenario, you can end up with hair loss. So it’s important to understand (and rule out) whether a nutrient deficiency is relevant to your specific hair loss case (we’ll reveal steps on how to do this later).
Small intestinal bacterial overgrowth (SIBO)
Small intestinal bacterial overgrowth (SIBO) is a condition whereby the pathogenic bacteria begin overgrow in the small intestine.
This creates issues with nutrient absorption – as these bacteria begin to compete with the nutrients that otherwise would’ve been absorbed by the small intestine and transported elsewhere in the body. Moreover, SIBO also triggers intestinal inflammation – the consequences of which we’re only beginning to understand.
There are currently no studies that tease out the connection between SIBO and hair loss. However, in my experience working with females who have diffuse hair loss, an overwhelming percentage of them who test for SIBO come back with a positive result. So, given the mechanistic links between SIBO and nutrient deficiencies, it’s worth mentioning this chronic condition as a potential trigger to chronic telogen effluvium.
Heavy metal toxicities
Heavy metals – like lead, cadmium, thallium, mercury, arsenic, aluminum, and copper – are often toxic at varying levels of exposure. And unfortunately, many of these heavy metals are linked to hair loss.
The mechanisms by which these metals trigger hair loss differ from one to another. For instance, mercury and thallium bind to proteins that build the hair shafts thus disrupting the proliferation of the hair follicle. Mercury also has a specific affinity for the thyroid. When absorbed into the body, it can downregulate the production of thyroid hormones, leading to hypothyroidism.
Another mechanism by which heavy metals may disrupt hair cycling is through the displacement of essential minerals – like magnesium, calcium, zinc, and iron. Heavy metals can knock essential minerals out of their binding sites – interfering with transport to tissues as well as disrupting the roles these minerals play in cellular activity. This is why heavy metal toxicities can mimic a nutrient deficiency – even in the presence of adequate nutrient consumption and absorption – because the problem is not necessarily in getting the nutrients where they’re supposed to be; it’s keeping them there.
While severe heavy metal toxicity is uncommon in developed countries, we are consistently exposed to heavy metals through our water supply, food, and air as a result of modern manufacturing practices. So, for people who present the symptoms of a heavy metal toxicity, and who have an elevated environmental risk of exposure, it’s usually a good idea to do further testing.
Which brings us to our next step: moving beyond education, and toward action.
What can we do about diffuse hair loss?
Now that we’ve learned of the major common causes of diffuse hair loss, we can go about identifying which ones are relevant to us. There are two ways to do this.
First, we can order laboratory work to test for all of the above “causes” linked to diffuse thinning. This would rule out which causes are relevant to us. Unfortunately, this method of testing is cost-prohibitive. It would cost tens of thousands of dollars to order each and every lab test to give us the insights we need to determine which ones are relevant to our unique hair loss case, and which ones aren’t.
If that doesn’t sound like a worth investment to you, don’t worry. There is another way.
The best approach (aside from working with a doctor)? Compare your environment, health history, and hair loss case against the major causes of diffuse thinning
Now that we’ve handled the educational component of this article, this may be easier than you think.
Simply ask yourself the following questions:
- Is my diffuse hair loss from hair follicle miniaturization, hair shedding, or both? The answers to these questions will help you determine if your diffuse thinning is related to androgenic alopecia, telogen effluvium, or both. And that, in turn, will tell you whether the causes are related to androgens, genetics, temporary stressors, or chronic conditions.
- Do I have any health symptoms in addition to hair loss? And do these symptoms overlap with any chronic conditions linked to hair shedding disorders? This might include things like poor digestion, skin problems, brain fog, cold hands/feet, and beyond.
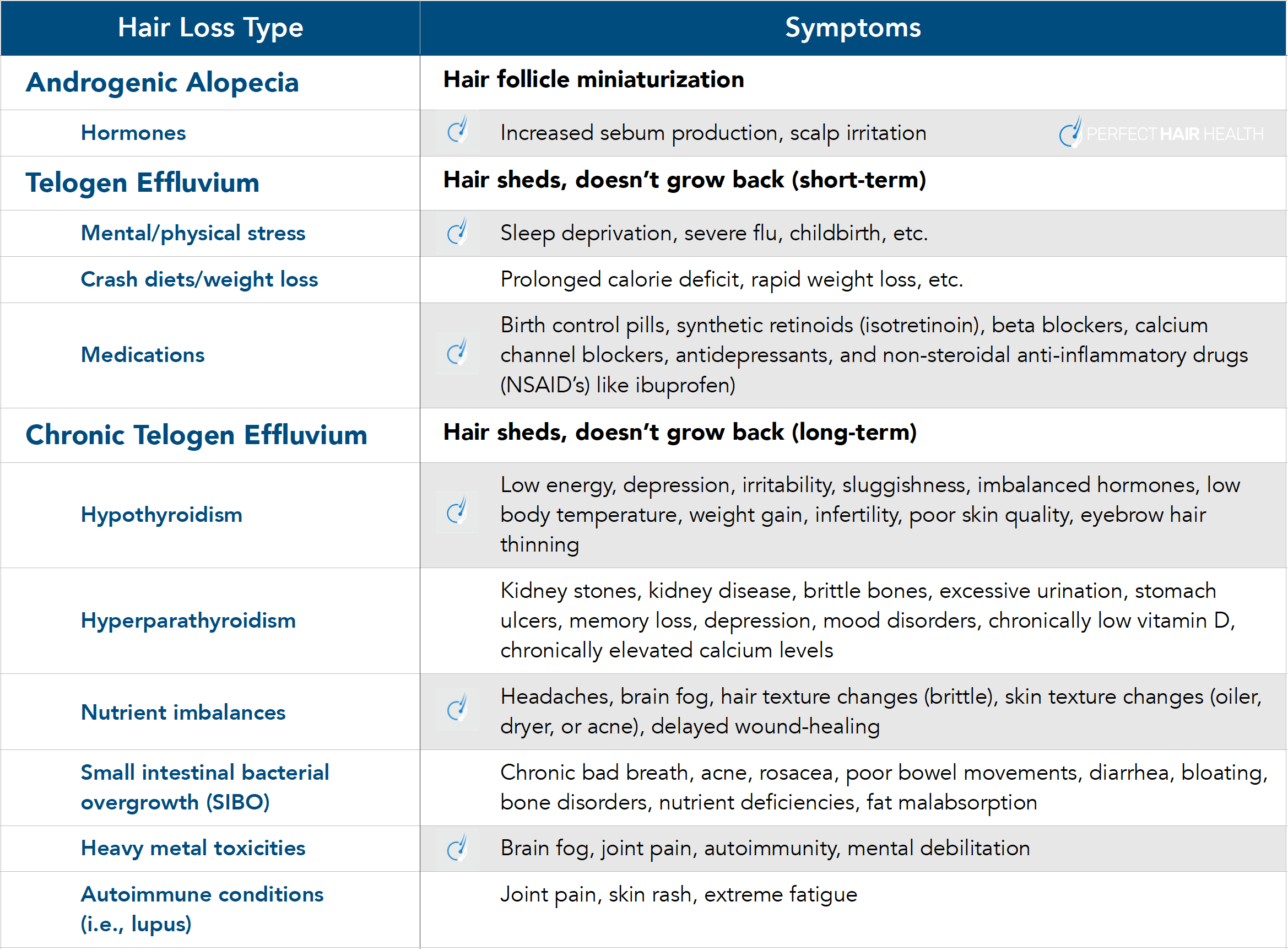
On that note, we’ve compiled a list of the conditions linked to diffuse hair loss, their symptoms, and how this hair loss might look in the scalp (its speed of onset and presentation). Using this list, it’s likely that you can narrow down your lists of relevant lab tests to just a few orders (if any).

Take that list, and start using it to your advantage! And keep in mind that a huge percentage of hair loss sufferers have multiple forms of hair loss. So, if you fall into multiple categories, that’s okay. You’re just identifying your own potential causes, so can seek more robust treatment options.
The power of identifying your hair loss causes (reader case study)
Here’s a reader case study of someone with whom I’ve worked for years: Ben M.
Ben M. is a male who began experiencing diffuse hair loss in his early twenties. In his first attempts to treat his hair loss, Ben M. only followed treatments for androgenic alopecia – which he’d initially suspected was a problem for him. They only worked to slow or stop his hair loss – if that.
A deeper analysis into his diet, lifestyle, stress levels, and environment revealed that Ben M. was also likely dealing with a hair shedding disorder – specifically, telogen effluvium related to a variety of causes (stress and nutrient deficiencies). So, we began to tackle those causes in addition to continuing to pursue interventions for AGA.
Six months later, Ben M. recovered nearly all of the hair that he’d lost.

If you’re curious to see his photos and full case study write-up, you can do so here.
Note: these results happened only after Ben took the time to evaluate his hair loss presentation alongside his health history, identify additional underlying causes, and then take a multifactorial approach to resolving his hair loss.
Once he targeted all of the underlying causes to his hair thinning, his regrowth skyrocketed. And according to him, it’s remained ever since we worked together.
The bottom line? Identify first, treat second
If you’re dealing with hair loss in a diffuse pattern, it pays dividends to systematically identify which causes of diffuse thinning relate to you. Then, you can prioritize testing for these contributors, and in doing so, fast-track yourself to better hair recovery.
Questions? Comments? Please reach out in the comments section below.
Want help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Learn More
Perfect Hair Health Team
"... Can’t thank @Rob (PHH) and @sanderson17 enough for allowing me to understand a bit what was going on with me and why all these [things were] happening ... "
— RDB, 35, New York, U.S.A."... There is a lot improvement that I am seeing and my scalp feel alive nowadays... Thanks everyone. "
— Aayush, 20’s, Boston, MA"... I can say that my hair volume/thickness is about 30% more than it was when I first started."
— Douglas, 50’s, Montréal, CanadaWant help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Join Now - Mission Statement
 Scroll Down
Scroll Down More
More More
More