- About
- Mission Statement
Education. Evidence. Regrowth.
- Education.
Prioritize knowledge. Make better choices.
- Evidence.
Sort good studies from the bad.
- Regrowth.
Get bigger hair gains.
Team MembersPhD's, resarchers, & consumer advocates.
- Rob English
Founder, researcher, & consumer advocate
- Research Team
Our team of PhD’s, researchers, & more
Editorial PolicyDiscover how we conduct our research.
ContactHave questions? Contact us.
Before-Afters- Transformation Photos
Our library of before-after photos.
- — Jenna, 31, U.S.A.
I have attached my before and afters of my progress since joining this group...
- — Tom, 30, U.K.
I’m convinced I’ve recovered to probably the hairline I had 3 years ago. Super stoked…
- — Rabih, 30’s, U.S.A.
My friends actually told me, “Your hairline improved. Your hair looks thicker...
- — RDB, 35, New York, U.S.A.
I also feel my hair has a different texture to it now…
- — Aayush, 20’s, Boston, MA
Firstly thank you for your work in this field. I am immensely grateful that...
- — Ben M., U.S.A
I just wanted to thank you for all your research, for introducing me to this method...
- — Raul, 50, Spain
To be honest I am having fun with all this and I still don’t know how much...
- — Lisa, 52, U.S.
I see a massive amount of regrowth that is all less than about 8 cm long...
Client Testimonials150+ member experiences.
 Scroll DownPopular Treatments
Scroll DownPopular Treatments- Treatments
Popular treatments. But do they work?
- Finasteride
- Oral
- Topical
- Dutasteride
- Oral
- Topical
- Mesotherapy
- Minoxidil
- Oral
- Topical
- Ketoconazole
- Shampoo
- Topical
- Low-Level Laser Therapy
- Therapy
- Microneedling
- Therapy
- Platelet-Rich Plasma Therapy (PRP)
- Therapy
- Scalp Massages
- Therapy
- More
IngredientsTop-selling ingredients, quantified.
- Saw Palmetto
- Redensyl
- Melatonin
- Caffeine
- Biotin
- Rosemary Oil
- Lilac Stem Cells
- Hydrolyzed Wheat Protein
- Sodium Lauryl Sulfate
- More
ProductsThe truth about hair loss "best sellers".
- Minoxidil Tablets
Xyon Health
- Finasteride
Strut Health
- Hair Growth Supplements
Happy Head
- REVITA Tablets for Hair Growth Support
DS Laboratories
- FoliGROWTH Ultimate Hair Neutraceutical
Advanced Trichology
- Enhance Hair Density Serum
Fully Vital
- Topical Finasteride and Minoxidil
Xyon Health
- HairOmega Foaming Hair Growth Serum
DrFormulas
- Bio-Cleansing Shampoo
Revivogen MD
- more
Key MetricsStandardized rubrics to evaluate all treatments.
- Evidence Quality
Is this treatment well studied?
- Regrowth Potential
How much regrowth can you expect?
- Long-Term Viability
Is this treatment safe & sustainable?
Free Research- Free Resources
Apps, tools, guides, freebies, & more.
- Free CalculatorTopical Finasteride Calculator
- Free Interactive GuideInteractive Guide: What Causes Hair Loss?
- Free ResourceFree Guide: Standardized Scalp Massages
- Free Course7-Day Hair Loss Email Course
- Free DatabaseIngredients Database
- Free Interactive GuideInteractive Guide: Hair Loss Disorders
- Free DatabaseTreatment Guides
- Free Lab TestsProduct Lab Tests: Purity & Potency
- Free Video & Write-upEvidence Quality Masterclass
- Free Interactive GuideDermatology Appointment Guide
- More
Articles100+ free articles.
-
Does Anavar Cause Hair Loss?
-
10 Best Shampoos for Hair Loss in 2026
-
XYON Review: Do Their Products Actually Regrow Hair?
-
Minoxidil Before and After Photos [2026] | Does It Work?
-
How to Get Finasteride: Is It Over the Counter?
-
Keeps Review: The Truth About Their Hair Loss Treatments?
-
7 Best Oils for Hair Growth
-
Hims Hair Growth Reviews: The Pros, Cons, and Real Results
PublicationsOur team’s peer-reviewed studies.
- Microneedling and Its Use in Hair Loss Disorders: A Systematic Review
- Use of Botulinum Toxin for Androgenic Alopecia: A Systematic Review
- Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia
- Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results
- A Hypothetical Pathogenesis Model For Androgenic Alopecia:Clarifying The Dihydrotestosterone Paradox And Rate-Limiting Recovery Factors
Menu- AboutAbout
- Mission Statement
Education. Evidence. Regrowth.
- Team Members
PhD's, resarchers, & consumer advocates.
- Editorial Policy
Discover how we conduct our research.
- Contact
Have questions? Contact us.
- Before-Afters
Before-Afters- Transformation Photos
Our library of before-after photos.
- Client Testimonials
Read the experiences of members
Before-Afters/ Client Testimonials- Popular Treatments
-
Articles
SRD5A1 and SRD5A2 are both part of the SRD5A gene family, encoding type I and type II 5α-reductase, respectively. With regard to hair loss, 5α-reductase is a type of enzyme that catalyzes the conversion of testosterone into dihydrotestosterone (DHT). DHT is a driving factor in androgenic alopecia (AGA) and, as a result, 5α-reductase inhibitors are a primary treatment for AGA. A collection of studies have investigated genetic variation in SRD5A1 and SRD5A2, with the results suggesting that some variants may cause differential responses to treatment with 5α-reductase inhibitors. This article will explore how relevant SRD5A1 and SRD5A2 are to hair treatment effectiveness and how to interpret your genetic results to make the correct treatment choice.
Interested in Topical Dutasteride?
Hair gains bigger than finasteride? Dutasteride makes this possible, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.

What Are the SR5DA Genes?
The Steroid 5α-Reductase (SRD5A) gene family is thought to be composed of up to five genes, the most prominent being SRD5A1, SRD5A2, and SRD5A3. Despite the name, only SRD5A1 and SRD5A2 exhibit strong 5α-reductase activity, meaning that they are highly efficient at converting testosterone to DHT.[1]Scaglione, A., Montemiglio, L.C., Parisi, G., Asteriti, I.A., Bruni, R., Cerutti, G., Testi, C., Savino, C., Mancia, F., Lavia, P. and Vallone, B. (2017). Subcellular localization of the five members … Continue reading
Both SRD5A1 and SRD5A2 are expressed throughout the body, but it is their expression in the scalp that is important for hair growth outcomes. Type I 5α-reductase (produced by SRD5A1) is only strongly expressed in the sebaceous glands, the part of the hair follicle that produces sebum and keeps the skin moisturized. In contrast, type II 5α-reductase (produced by SRD5A2) is primarily expressed in the infundibulum (upper portion), inner root sheath, and outer root sheath of the hair follicle, indicating that type I and type II 5α-reductase have distinct localization within the skin and hair follicle.[2]Bayne, Flanagan, Einstein, Ayala, Chang, Azzolina, Whiting, Mumford and Thiboutot. (1999). Immunohistochemical localization of types 1 and 2 5α‐reductase in human scalp. British Journal of … Continue reading
Although they do have other roles, the primary function of these enzymes is to convert testosterone into dihydrotestosterone (DHT). One of four androgens (steroid hormones), DHT is known to be a driving factor of androgenic alopecia (AGA) and is implicated in the miniaturization of hair follicles.[3]Marchetti, P.M. and Barth, J.H. (2013). Clinical biochemistry of dihydrotestosterone. Annals of Clinical Biochemistry, 50(2), 95-107. Available at: https://doi.org/10.1258/acb.2012.012159
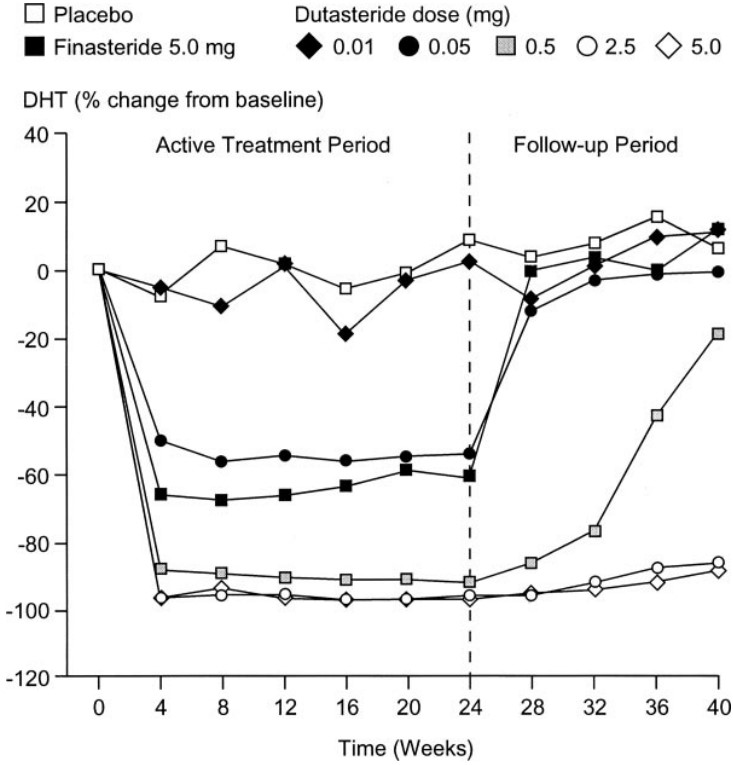
Due to the aforementioned role of DHT, 5α-reductase is a key target when it comes to the treatment of AGA. Thus, one of the main classes of AGA and hair loss treatments is 5α-reductase inhibitors. These inhibitors work by targeting the 5α-reductase enzymes, reducing their levels in order to disrupt the conversion of testosterone to DHT. Finasteride is the only FDA-approved 5α-reductase inhibitor for the treatment of AGA, which inhibits type II 5α-reductase. Dutasteride, a dual-inhibitor of type I and type II 5α-reductase, is only FDA-approved for the treatment of an enlarged prostate but is also prescribed off-label for AGA.[4]Gupta, A.K., Bamimore, M.A., Wang, T. and Talukder, M. (2024). The impact of monotherapies for male androgenetic alopecia: A network meta‐analysis study. Journal of Cosmetic Dermatology. Available … Continue reading
Other 5α-reductase inhibitors exist, including naturally occurring substances such as saw palmetto and some green tea catechins, but they have varying levels of evidence quality.
What is The Evidence For Targeting SR5DA for Hair Loss?
So, SRD5A1 and SRD5A2 are closely linked to 5α-reductase activity, DHT production, and, therefore, AGA. Owing to this, it is feasible that genetic variation in either SRD5A1 or SRD5A2 could influence the efficacy of 5α-reductase inhibitors in the treatment of hair loss.
In one study, the genotypes of 42 males with AGA were investigated. They had been using dutasteride for 6 months in a clinical trial, which had produced variable results. For the purposes of this study, patients were put into the poor responder (control) group or the good responder (cases) group, based on their increase in hair count during the original study. In their investigation, they identified a number of genetic variants that were statistically significantly associated with the strength of the response to the treatment (Figure 1).[5]Rhie, A., Son, H.Y., Kwak, S.J., Lee, S., Kim, D.Y., Lew, B.L., Sim, W.Y., Seo, J.S., Kwon, O., Kim, J.I. and Jo, S.J. (2019). Genetic variations associated with response to dutasteride in the … Continue reading
Three of these were single nucleotide polymorphisms (SNPs) within the SRD5A1 gene – rs3822430, rs8192186, and rs3736316. Each of these SNPs was positively associated with the response to dutasteride; in other words, patients with these genetic variants responded better to dutasteride treatment.

Figure 1: Genotypic landscape of 42 patients and the cumulative effect of each allele count and their positive or negative effect. Boxes represent SNPs that exhibited a positive (blue) or negative (red) effect on dutasteride response. Light-colored boxes represent heterozygous SNPs (a variation where an individual has two different versions of a specific DNA sequence at a particular location in the genome), dark-colored boxes represent homozygous SNPs (a variation where an individual has two identical versions of a specific DNA sequence at a particular location in the genome). Patient responses to dutasteride improve from left to right.[6]Rhie, A., Son, H.Y., Kwak, S.J., Lee, S., Kim, D.Y., Lew, B.L., Sim, W.Y., Seo, J.S., Kwon, O., Kim, J.I. and Jo, S.J. (2019). Genetic variations associated with response to dutasteride in the … Continue reading
Despite the positive associations, some of the patients who possessed these SNPs were still considered to be poor responders. This suggests that having a ‘positive’ SNP in SRD5A1 does not provide a definitive indication that you will respond well to dutasteride. Rather, the study’s results suggest that the combination of SNPs you possess and how they interact with each other is more important.
Interestingly, SRD5A2 was not associated with the response to dutasteride in the same study and no other studies have investigated the effects of SRD5A2 variants on the efficacy of dutasteride or finasteride treatment for hair loss, but that does not mean there are no effects.
Genetic variation in the SRD5A gene family appears to influence the efficacy of dutasteride treatment, so the question then turns to why this might happen.
In a study conducted on 57 males with type II diabetes, an association was found between the SRD5A1 HinfI SNP and the DHT/testosterone ratio, which is used as an indicator of 5α-reductase enzyme activity.[7]Ellis, J.A., Panagiotopoulos, S., Akdeniz, A., Jerums, G. and Harrap, S.B. (2005). Androgenic correlates of genetic variation in the gene encoding 5α-reductase type 1. Journal of Human Genetics, … Continue reading
HinfI is an enzyme that binds to a specific series of bases (called a restriction site) and cuts the DNA. Any changes to that sequence of bases will prevent HinfI from cutting the DNA, so it can be used to identify SNPs within known restriction sites. Individuals who lacked the SRD5A1 HinfI restriction site had a higher ratio of DHT/testosterone ratio than those with other genotypes, indicating increased activity of 5α-reductase.
In patients with increased levels of DHT, due to genetic variation, treatment with 5α-reductase inhibitors may look different. Higher concentrations of 5α-reductase inhibitors may be necessary, and it might take longer to see results, but the treatment may also have a more noticeable effect on hair loss as DHT levels can be reduced more than normal.

Figure 2: Measurements of testosterone (T), DHT, sex hormone binding globulin (SHBG), and insulin in participants with different genotypes (AA, AB, BB). A=absence of restriction site. Presence of the restriction site. Those lacking the restriction site (AA) had a higher DHT/T ratio meaning increased 5a-reductase activity.[8]Ellis, J.A., Panagiotopoulos, S., Akdeniz, A., Jerums, G. and Harrap, S.B. (2005). Androgenic correlates of genetic variation in the gene encoding 5α-reductase type 1. Journal of Human Genetics, … Continue reading
A different study was conducted on 104 patients with metastatic prostate cancer, investigating SNPs in SRD5A1 and SRD5A2. The authors discovered that patients with the GG genotype in SRD5A2 rs523349 exhibited increased 5α-reductase enzyme activity than those with the GC or CC genotype. #
The patients did not have their DHT levels measured, however, it is possible that increased 5α-reductase enzyme activity would lead to increased levels of DHT, which might make patients with the GG genotype a better candidate for treatment with a 5α-reductase inhibitor.[9]Shiota, M., Fujimoto, N., Yokomizo, A., Takeuchi, A., Itsumi, M., Inokuchi, J., Tatsugami, K., Uchiumi, T. and Naito, S. (2015). SRD5A gene polymorphism in Japanese men predicts prognosis of … Continue reading
These findings were supported by another study, which investigated several genetic variants of the SRD5A2 gene in healthy men. The authors found that, although the expression levels of the type II 5α-reductase enzyme were similar throughout, some of the variants produced type II 5α-reductase with very different properties to the normal (wild-type) enzyme.[10]Makridakis, N.M., di Salle, E. and Reichardt, J.K. (2000). Biochemical and pharmacogenetic dissection of human steroid 5α-reductase type II. Pharmacogenetics and Genomics, 10(5), 407-413. Available … Continue reading
Importantly, the activity of the enzyme (the speed at which it catalyzes reactions) was lower than normal in some variants and higher in others suggesting that DHT production may be lower in people with some SRD5A2 variants and higher in people with others. In contrast to those with higher levels, patients with lower DHT levels than normal may require a reduced dose of 5α-reductase inhibitor, and it is possible that treatment will be less efficient as DHT levels are already low. Or, other treatments that don’t primarily target DHT might be more appropriate.
To investigate this further, the authors produced lab-grown animal cells which contained each of the genetic variants. They then tested finasteride and dutasteride on all of the cells and measured 5α-reductase activity, to determine how efficiently the 5α-reductase inhibitors worked on each variant. They found that finasteride and dutasteride could be more, less, or equally effective as normal, depending on the variant(s).
Moreover, finasteride could be more effective than normal against a variant, while dutasteride was less effective than normal, and vice versa. This suggests that genetic variation could significantly affect the outcomes of treatment with finasteride or dutasteride.
Collectively, the results of these studies suggest that genetic variation in the SRD5A family of genes should be considered when designing treatment regimens for hair loss. However, the data is not without its limitations.
For the most part, studies conducted on SRD5A (including the ones here) have only included male participants. As males and females display differences in DHT expression, it would not be surprising if there were also differences in SRD5A gene expression and 5α-reductase inhibitor activity.
Furthermore, these studies were only conducted on a small number of participants. This reduces the power of a study, as you may not have an accurate representation of the wider population, and it can lead to results being misleading. Repeating the study on a much larger scale would produce more conclusive results. Also, some of the studies were not conducted on patients with AGA or hair loss-related conditions, so the findings are not directly relevant to hair loss treatment.
The final study, which investigated 5α-reductase inhibitor activity on each variant, was performed in vitro. In other words, it was performed on cells that had been genetically modified to express each variant. Furthermore, these cells were not even human cells found in the scalp or hair follicle, but rather animal cells.
Although models such as this can be very useful, the results they produce are not definitive, as the model (cells, in this case) is not a true representation of human anatomy.
Despite these limitations, there is sufficient evidence to suggest that genetic variation in SRD5A1 or SRD5A2 may influence your response to treatment with a 5α-reductase inhibitor. Below are some of the variants which may be relevant to hair loss and treatment.
What Do Your Genetic Results Mean?
Your Result
SRD5A1 (rs248793)
Variant 1 – GG genotype
Variant 2 – CC genotype Variant 3 – GC genotype
What it means At a lower risk of presenting with higher DHT/T ratio At a slightly higher risk of presenting with an increased DHT/T ratio At a higher risk of presenting with a significant increase in DHT/T ratio The Implication You might not be a good candidate for 5α-reductase inhibitors May be a good candidate for normal/increased concentrations of 5α-reductase inhibitors May be a good candidate for increased concentrations of 5α-reductase inhibitors Your Result SRD5A1 (rs3822430)
Variant 1 – AA genotype
Variant 2 – AG genotype Variant 3 – GG genotype
What it means May be a normal/poor responder to 5α-reductase inhibitors May be a good responder to 5α-reductase inhibitors May be a good responder to 5α-reductase inhibitors The Implication May be a good candidate for typical/higher dosages of 5α-reductase inhibitors May be a good candidate for lower dosages of 5α-reductase inhibitors May be a good candidate for lower dosages of 5α-reductase inhibitors Your Result SRD5A1 (rs8192186)
Variant 1 – AA genotype
Variant 2 – AG genotype Variant 3 – GG genotype
What it means May be a good responder to 5α-reductase inhibitors May be a good responder to 5α-reductase inhibitors May be a normal/poor responder to 5α-reductase inhibitors The Implication May be a good candidate for lower dosages of 5α-reductase inhibitors May be a good candidate for lower dosages of 5α-reductase inhibitors May be a good candidate for typical/higher dosages of 5α-reductase inhibitors Your Result SRD5A2 (rs523349)
Variant 1 – GG genotype
Variant 2 – GC genotype Variant 3 – CC genotype
What it means Associated with increased 5α-reductase activity Significantly lower 5α-reductase activity Significantly lower 5α-reductase activity The Implication May be a good candidate for 5α-reductase inhibitors May not be a good candidate for 5α-reductase inhibitors May not be a good candidate for 5α-reductase inhibitors What Relevance Dose SR5DA Have for Hair Loss Treatment?
We have also created a rubric that helps to determine the relevance of a specific gene to hair loss based on the quality of the evidence in the above studies.
On a scale of 1-5, how important are these genetic results? (1 is the lowest, 5 is the highest)
This score is a rating based on evidence quality.
- Does this gene have any potential relevance for hair loss? (1 point)
Yes. Increased DHT is associated with hair follicle miniaturization and the onset of androgenic alopecia, and these genes encode enzymes that synthesize DHT (score=1)
- Does the totality of evidence implicate SRD5A1 or SRD5A2 as causal agents for hair loss? (1 point)
Yes, as mentioned above, an increase in DHT is associated with androgenic alopecia, and these genes create an enzyme that synthesizes DHT (score = 1)
- Does the totality of evidence implicate SRD5A1/SRD5A2 as predictive factors for hair loss treatment responsiveness? (2 points)
Yes, there is evidence to suggest that SRD5A1 may be a predictive factor for hair loss treatment responsiveness, however, some of the patients with the SNP’s for treatment responsiveness still performed poorly, indicating that there are a number of factors involved in responsiveness to treatments. (score = 1)
- Is this quality of evidence on (3) strong enough to influence treatment recommendations? (1 point)
No. (score = 0)
Total Score = 3
Final Thoughts
While some small studies suggest that genetic variation in SRD5A1 and SRD5A2 may influence your response to treatment with a 5α-reductase inhibitor, the evidence is not yet strong enough to make definitive treatment recommendations based solely on genotype. Larger and more robust studies are needed to confirm the true predictive value of genetic testing for SRD5A1 and SRD5A2 for personalizing hair loss treatments.
References[+]
References ↑1 Scaglione, A., Montemiglio, L.C., Parisi, G., Asteriti, I.A., Bruni, R., Cerutti, G., Testi, C., Savino, C., Mancia, F., Lavia, P. and Vallone, B. (2017). Subcellular localization of the five members of the human steroid 5α-reductase family. Biochimie open, 4, 99-106. Available at: https://doi.org/10.1016/j.biopen.2017.03.003 ↑2 Bayne, Flanagan, Einstein, Ayala, Chang, Azzolina, Whiting, Mumford and Thiboutot. (1999). Immunohistochemical localization of types 1 and 2 5α‐reductase in human scalp. British Journal of Dermatology, 141(3), 481-491. Available at: https://doi.org/10.1046/j.1365-2133.1999.03042.x ↑3 Marchetti, P.M. and Barth, J.H. (2013). Clinical biochemistry of dihydrotestosterone. Annals of Clinical Biochemistry, 50(2), 95-107. Available at: https://doi.org/10.1258/acb.2012.012159 ↑4 Gupta, A.K., Bamimore, M.A., Wang, T. and Talukder, M. (2024). The impact of monotherapies for male androgenetic alopecia: A network meta‐analysis study. Journal of Cosmetic Dermatology. Available at: https://doi.org/10.1111/jocd.16362 ↑5, ↑6 Rhie, A., Son, H.Y., Kwak, S.J., Lee, S., Kim, D.Y., Lew, B.L., Sim, W.Y., Seo, J.S., Kwon, O., Kim, J.I. and Jo, S.J. (2019). Genetic variations associated with response to dutasteride in the treatment of male subjects with androgenetic alopecia. Plos one, 14(9), e0222533. Available at: https://doi.org/10.1371/journal.pone.0222533 ↑7, ↑8 Ellis, J.A., Panagiotopoulos, S., Akdeniz, A., Jerums, G. and Harrap, S.B. (2005). Androgenic correlates of genetic variation in the gene encoding 5α-reductase type 1. Journal of Human Genetics, 50(10), 534-537. Available at: https://doi.org/10.1007/s10038-005-0289-x ↑9 Shiota, M., Fujimoto, N., Yokomizo, A., Takeuchi, A., Itsumi, M., Inokuchi, J., Tatsugami, K., Uchiumi, T. and Naito, S. (2015). SRD5A gene polymorphism in Japanese men predicts prognosis of metastatic prostate cancer with androgen deprivation therapy. European Journal of Cancer, 51(14), 1962-1969. Available at: https://doi.org/10.1016/j.ejca.2015.06.122 ↑10 Makridakis, N.M., di Salle, E. and Reichardt, J.K. (2000). Biochemical and pharmacogenetic dissection of human steroid 5α-reductase type II. Pharmacogenetics and Genomics, 10(5), 407-413. Available at: https://doi.org/10.1097/00008571-200007000-00004 SULT1A1 is a gene that encodes for sulfotransferase, an enzyme that catalyzes various reactions throughout the body. Regarding hair loss, sulfotransferase is crucial for activating minoxidil, which requires sulfonation to exert its effects.
Some studies suggest that measuring sulfotransferase levels may be possible to predict whether minoxidil will be effective. Others have claimed that the expression of a specific variant of the SULT1A1 gene can indicate whether the drug is likely to work.
This article will explore how relevant SULT1A1 is to hair treatment effectiveness and how to interpret your genetic results to make the correct treatment choice.
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is SULT1A1?
The SULT1A1 gene codes for an enzyme called sulfotransferase 1A1 (SULTS). The SULT family of enzymes catalyzes the transfer of a sulfonate (SO3-) group from the universal donor 3’-phosphoadenosine 5’-phosphosulfate (PAPS) to an acceptor molecule. This reaction is known as sulfation or sulfurylation.[1]Negishi, M., Pederson, L.G., Petrochenko, E., Shevtsov, S., Gorokhov, A., Kakuta, Y., Pederson, L.C. (2001). Structure and function of sulfotransferases. Archives of biochemistry and biophysics. … Continue reading
These reactions play a crucial role in the metabolism and detoxification of various compounds, including hormones, neurotransmitters, and drugs (including minoxidil which we will get to), increasing their water solubility and facilitating their elimination.[2]Gamage, N., Barnett, A., Hempel, N., Duggleby, R.G., Windmill, K.F., Martin, J.L., McManus, M.E. (2006). Human Sulfotransferases and Their Role in Chemical Metabolism. Toxicological Sciences. 90(1). … Continue reading
The SULT1 family in humans consists of at least nine members, including SULT1A1, SULT1A2, SULT1A3, SULT1A4, SULT1B1, SULT1C2, SULT1C3, SULT1C4, and SULT1E1. Genetic variations in SULT1A1 can influence enzyme activity and have been associated with differences in drug response, toxicity, and disease susceptibility.[3]National Library of Medicine. (2024). SULT1A1 sulfotransferase family 1A member 1 [Homo sapiens (human)]. NIH. Available at: … Continue reading
Some studies have found different variants of the SULT1A1 gene, which are associated with different activity levels. The GG variant was associated with high activity, whereas GA and AA variants were associated with low activity.[4]Ramos, P.M., Gohad, P., McCoy, J., Wambier, C., Goren, A. (2021). Minoxidil Sulfotransferase Enzyme (SULT1A1) Genetic Variants Predicts Response to Oral Minoxidil Treatment for Female Pattern Hair … Continue reading
So, we know what SULT1A1 is and about the enzyme it codes for. But how relevant is it to hair loss outcomes?
What is the Evidence For Targeting SULT1A1 for Hair Loss?
One crucial piece of evidence for targeting SULT1A1 for hair loss is the link between sulfotransferase and minoxidil. SULT1A1 codes for the sulfotransferase enzyme that catalyzes the conversion of minoxidil (a prodrug that needs activation to exert its effect) to minoxidil sulfate (the activated form of the drug). As such, some studies have evaluated the correlation between minoxidil efficacy and sulfotransferase activity.
One study was conducted with 34 patients who had been treated with minoxidil alone for a minimum of 6 months.[5]Goren, A., Castano, J.A., McCoy, J., Bermudez, F., Lotti, T. (2014). Novel enzymatic assay predicts minoxidil response in the treatment of androgenetic alopecia. Dermatologic Therapy. 27. 171-173. … Continue reading These patients were evaluated as “responders” or “non-responders” based on global photographic assessment. Hairs in the growing (anagen phase) were plucked from the border between bald and non-bald scalp areas and evaluated for sulfotransferase activity. Each patient’s sulfotransferase activity was measured and compared to their “responder” or “non-responder” status. The researchers found that most “responders” had a higher sulfotransferase activity, whereas most “non-responders” had a lower sulfotransferase activity.

Figure 1. Sulfotransferase activity compared to “responder or non-responder status”.[6]Goren, A., Castano, J.A., McCoy, J., Bermudez, F., Lotti, T. (2014). Novel enzymatic assay predicts minoxidil response in the treatment of androgenetic alopecia. Dermatologic Therapy. 27. 171-173. … Continue reading
Another study of the same group also measured sulfotransferase activity in 21 women with female pattern hair loss who had been treated with 5% minoxidil for a minimum of 6 months.[7]Roberts, J., Desai, N., McCoy, J., Goren, A. (2014). Sulfotransferase activity in plucked hair follicles predicts response to topical minoxidil in the treatment of female androgenetic alopecia. … Continue reading Fifteen “responders” and 6 “non-responders” were identified, with only two not correctly identified after the assay.
Why Do Some People Have Lower SULT1A1 Activity Levels Than Others?
Well, the SULT1A1*2 variant of the SULT1A is associated with low enzyme activity and thermal stability of SULT1A1.[8]Raftogianis, R.B., Wood, T.C., Otterness, D.M., Loon, J.A.V., Weinshilboum, R.M. (1997). Phenol Sulfotransferase Pharmacogenetics in Humans: Association of Common SULT1A1 Alleles with TS PST … Continue reading Therefore, it can be reasonably inferred that those with lower sulfotransferase activity might have this gene variant and, therefore, be less responsive to minoxidil.
SULT1A1 Gene Variants & Minoxidil: Clinical Studies
There are two studies that explore different gene variants of SULT1A1 and their effect on minoxidil efficacy.
In the first study, 17 males and 18 females with androgenic alopecia were included.[9]Raghad, N.A., Al-Gazally, M.E., Ewahd, W.A. (2017). Assessment the effect of different genotypes of sulfotransferase 1A1 gene on the response to minoxidil in patients with androgenic alopecia. … Continue reading The participants had been using topical minoxidil for at least 3 months before being assessed for response and allocated into “responder” and “non-responder” groups. The participants were then genotyped to determine what allele variant was present in the SULT1A1 gene and compared.
84% of participants who carried the G allele of the SULT1A1 gene were in the “responder” group, compared to only 16% of those with the A allele.

Figure 2. The proportion of participants in the R0 (“non-responder”) and R1 (“responder”) groups with each allele variation.[10]Raghad, N.A., Al-Gazally, M.E., Ewahd, W.A. (2017). Assessment the effect of different genotypes of sulfotransferase 1A1 gene on the response to minoxidil in patients with androgenic alopecia. … Continue reading
Furthermore, of those carrying the GG variant, 68.8% were “responders” compared to 15.8% who were “non-responders”. Conversely, 84.2% of “non-responders” had the GA genotype compared to 31.2% of “responders”.

Figure 3. The proportion of participants in the R0 (“non-responder”) and R1 (“responder”) groups with each genotype variation.[11]Raghad, N.A., Al-Gazally, M.E., Ewahd, W.A. (2017). Assessment the effect of different genotypes of sulfotransferase 1A1 gene on the response to minoxidil in patients with androgenic alopecia. … Continue reading
Interestingly, a higher proportion of “responders” were female (25.7%), indicating a potential for women to respond better to minoxidil (possibly due to more women having the GG allele variation) – however, this would need to be confirmed in further studies.

Figure 4. Red: Proportion of males and females in the “responder” group (R1). Blue: Proportion of males and females in the “non-responder” group (R0).[12]Raghad, N.A., Al-Gazally, M.E., Ewahd, W.A. (2017). Assessment the effect of different genotypes of sulfotransferase 1A1 gene on the response to minoxidil in patients with androgenic alopecia. … Continue reading
A further study was conducted in 2020 in which 10 participants with female pattern hair loss were treated with 1 mg oral minoxidil daily for six months.[13]Ramos, P.M., Gohad, P., McCoy, J., Wambier, C., Goren, A. (2021). Minoxidil Sulfotransferase Enzyme (SULT1A1) genetic variants predict response to oral minoxidil treatment for female pattern hair … Continue reading Hairs were counted within a 2.2 cm2 area, with a minimum 13% increase in hair count considered as a “responder”. Genotyping was conducted alongside this. Participants with the GG allele variant showed a 13.3% average increase in hair count, while participants with the GA allele variant showed a 6.9% average increase.
The researchers concluded that this gene variant can predict response to oral minoxidil treatment, but we see some issues. There are clearly some are some exceptions to the rule (which you can see below).
One person with the GA allele variant showed a 21.8% increase in hair which is a larger increase than nearly all of the GG allele variants! Furthermore, three of the GG variants did not reach the minimum 13% increase in hair count to actually be labeled a “responder”.

Figure 5. Effect of allele variants on hair follicle growth.[14]Ramos, P.M., Gohad, P., McCoy, J., Wambier, C., Goren, A. (2021). Minoxidil Sulfotransferase Enzyme (SULT1A1) genetic variants predict response to oral minoxidil treatment for female pattern hair … Continue reading
To confirm whether the variants actually affect response rates to minoxidil treatment, larger-scale studies are needed.
Can I Get Better Results with Oral Minoxidil?
On the internet, some individuals have mentioned that if you have a variant of SULT1A1, that means you’re less likely to respond to topical minoxidil, then you should take low-dose oral minoxidil. This is because the liver has abundant sulfotransferase activity which can also convert oral minoxidil to its active form. This active form could then circulate through the bloodstream to the scalp and exert its effects that way.
But is this true?
Well, it is true that the liver has high sulfotransferase activity. This suggests that individuals with low sulfotransferase activity in their hair follicles (due to SULT1A1 gene variants) might still benefit from oral minoxidil. However, as you can see above, studies have shown mixed results regarding the efficacy of oral minoxidil in “non-responders”.
Would Switching From Topical to Oral Help?
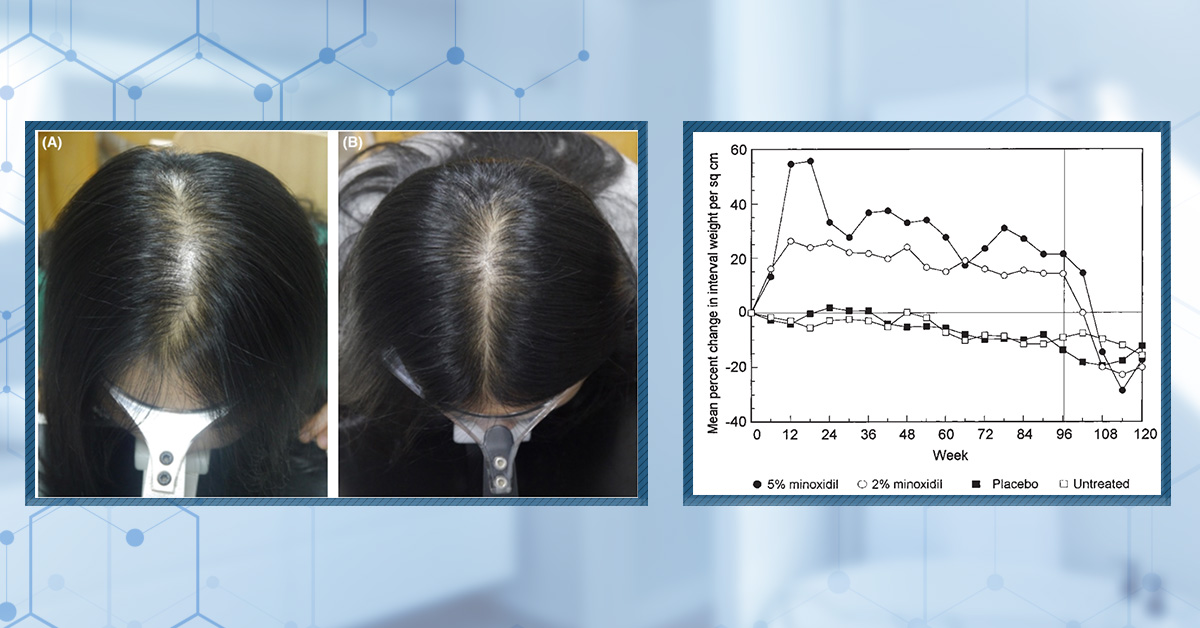
Switching to oral minoxidil may help some who don’t respond to topical minoxidil. One study by Ramos et al. found that in their study population of female patients, oral minoxidil slightly outperformed topical minoxidil in improving hair density and reducing shedding over 24 weeks.[15]Ramos, P.M., Sinclair, R.D., Kasprzak, M., Miot, H.A. (2020). Minoxidil 1 mg oral versus minoxidil 5% topical solution for the treatment of female-pattern hair loss: a randomized clinical … Continue reading
Another study, however, found that although topical minoxidil had a better overall effect than 1 mg oral minoxidil, there was no significant difference between the two groups, indicating that switching might actually just lead to the same response.[16]Asilian, A., Farmani, A., Saber, M. (2023). Clinical efficacy and safety of low-dose oral minoxidil versus topical solution in the improvement of androgenetic alopecia: a randomized controlled … Continue reading
Will Switching Make a Difference?
Not necessarily. It looks like the effectiveness of oral minoxidil can still be influenced by the same genetic factors that affect topical minoxidil response. Additionally, oral minoxidil carried potential safety risks, as it is not FDA-approved for hair loss and may have systemic side effects that need to be carefully managed.
In recent years, genetic testing companies have sprung up that claim to analyze your genotype to help you choose a personalized hair loss treatment. However, concerns remain about the accuracy of their recommendations, privacy issues regarding genetic data, and the potential for overpromising results without comprehensive clinical validation.
These companies often include the SULT1A1 gene as a predictor of responsiveness to minoxidil. So, we collated all of the potential SULT1A1 gene variants that might be relevant to hair loss and recommendations, depending on your genotype.
SULT1A1 genetic variants play a significant role in predicting the effectiveness of minoxidil for hair loss treatment. While the enzyme’s activity in hair follicles can indicate responsiveness to topical minoxidil, switching to oral minoxidil may offer limited additional benefits due to similar genetic influences on enzyme activity. Enhancing sulfotransferase activity through methods like tretinoin application and microneedling has shown promise in improving treatment outcomes for non-responders.
What Do Your Genetic Results Mean?
There are a number of variants that your genetic testing results might tell you that you have. You can see the possible variants that might come up within your own gene testing and reference these tables once you get your results to find out what they mean.
Your Result SULT1A1-1 Variant 1 SULT1A1-1 Variant 2 SULT1A1-1 Variant 3 rs9282861 GG genotype rs9282861 GA genotype rs9282861 AA genotype What it Means High sulfotransferase activity Moderate sulfotransferase activity Low sulfotransferase activity The Implication May respond well to topical minoxidil. Recommend treatment. May respond normally to topical minoxidil. May not respond well to topical minoxidil. You may want to try oral minoxidil or an alternative treatment. Your Result SULT1A1-2 Variant 1 SULT1A1-2 Variant 2 SULT1A1-2 Variant 3 rs1042028 GG genotype rs1042028 GA genotype rs1042028 AA genotype What it Means High sulfotransferase activity Moderate sulfotransferase activity Low sulfotransferase activity and low thermal stability The Implication May respond well to topical minoxidil. Recommend treatment. May respond normally to topical minoxidil. May not respond well to topical minoxidil. You may want to try oral minoxidil or an alternative treatment. Your Result SULT1A1-3 Variant 1 SULT1A1-3 Variant 2 SULT1A1-3 Variant 3 rs1042157 TT genotype rs1042157 CT genotype rs1042157 CC genotype What it Means Low sulfotransferase activity. You may want to try oral minoxidil or an alternative treatment. Moderate sulfotransferase activity High sulfotransferase activity The Implication May not respond well to topical minoxidil. You may want to try oral minoxidil or an alternative treatment. May respond normally to topical minoxidil. May respond well to topical minoxidil. Recommend treatment. Your Result SULT1A1-4 Variant 1 SULT1A1-3 Variant 2 SULT1A1-4 Variant 3 rs6839 GG genotype rs6839 AG genotype rs6839 AA genotype What it Means Low sulfotransferase activity Moderate sulfotransferase activity High sulfotransferase activity The Implication May not respond well to topical minoxidil. You may want to try oral minoxidil or an alternative treatment. May respond normally to topical minoxidil. May respond well to topical minoxidil. Recommend treatment. Table 1: Different potential allele variants of the SULT1A1 gene and the implication in terms of hair treatments.
What Relevance Does SULT1A1 Have for Hair Loss Treatment?
We have also created a rubric that helps to determine the relevance of a specific gene to hair loss based on the quality of the evidence in the above studies.
- Does this gene have any potential relevance for hair loss? (1 point)
Yes. Some studies have shown that people with variations in the SULT1A1 gene may respond differentially to minoxidil. (score = 1)
- Does the totality of evidence implicate SULT1A1 as a causal agent for hair loss? (1 point)
There is no evidence to suggest that SULT1A1 variations cause hair loss (score = 0)
- Does the totality of evidence implicate SULT1A1 as a predictive factor for hair loss treatment responsiveness? (2 points)
Yes. There are a number of studies implicating SULT1A1 as a predictive factor for minoxidil responsiveness. (score =2)
- Is this quality of evidence on (3) strong enough to influence treatment recommendations? (1 point)
No. One paper was published in a journal with a low/no impact factor. The sample sizes were small, and the results where genotyping was actually conducted were variable. (score= 0)
Total Score = 3
How Can I Improve My Sulfotransferase Activity?
So, you have tried minoxidil, but the regrowth hasn’t been as impactful as you hoped, and you find out that this is because your sulfotransferase levels are low. How can you boost it? Well, studies show that combining retinoic acid or tretinoin with minoxidil can increase sulfotransferase activity.
The topical application of tretinoin increases the expression and activity of follicular sulfotransferase enzymes. One study was conducted on 20 participants (10 males and 10 females) with androgenic alopecia.[17]Sharma, A., Goren, A., Dhurat, R., Agrawal, S., Sinclair, R., Trueb, R., Vano-Galvan, S., Chen, G., Tan, Y., Kovacevic, M., Situm, M., McCoy, J. (2019). Tretinoin enhances minoxidil response in … Continue reading
The participants’ hair follicles were analyzed using the Minoxidil Response Test and determined as “responders” or “non-responders” to minoxidil treatment. The participants then underwent 5 days of treatment with 0.1% topical tretinoin. The average sulfotransferase activity for the whole cohort did not significantly improve after the five days, however, when the cohort was separated into “responders” and “non-responders”, something interesting happened. Those predicted to be “non-responders” to topical minoxidil did show a significant increase in sulfotransferase activity, with a total of 43% of “non-responders” converted to “responders” after five days of application.

Figure 6. Sulfotransferase activity before and after five days of 0.1% topical tretinoin application. NR = Non-responder. R = Responder.[18]Sharma, A., Goren, A., Dhurat, R., Agrawal, S., Sinclair, R., Trueb, R., Vano-Galvan, S., Chen, G., Tan, Y., Kovacevic, M., Situm, M., McCoy, J. (2019). Tretinoin enhances minoxidil response in … Continue reading
Another way to improve sulfotransferase levels and, therefore, minoxidil efficacy is by undergoing microneedling. One study by Sharma et al. investigated the effect of microneedling on follicular sulfotransferase enzymes in male subjects with androgenic alopecia.[19]Sharma, A., Surve, R., Dhurat, R., Sinclair, R., Tan, Y., Zou, Y., Muller Ramos, R., Wambier, C., Verner, I., Kovacevic, M., Goren, A. (2020). Microneedling improves minoxidil response in … Continue reading Six male subjects underwent 3 weekly sessions of microneedling at 1.5 mm depth on a target area of the scalp. Sulfotransferase enzyme activity was analyzed in the hair follicle at the baseline and at the end of the three weeks. 66% of participants had an increase in sulfotransferase activity compared to the baseline, and 16% of subjects who were previously classified as “non-responders” to topical minoxidil were converted to “responder” status.

Figure 7. Sulfotransferase enzyme activity following microneedling treatment.[20]Sharma, A., Surve, R., Dhurat, R., Sinclair, R., Tan, Y., Zou, Y., Muller Ramos, R., Wambier, C., Verner, I., Kovacevic, M., Goren, A. (2020). Microneedling improves minoxidil response in … Continue reading
Final Thoughts
While some small studies suggest that testing for SULT1A1 variants might help to predict minoxidil efficacy, the evidence is not yet strong enough to make definitive treatment recommendations based solely on genotype. Larger and more robust studies are needed to confirm the true predictive value of genetic testing for SULT1A1 for personalizing hair loss treatments.
References[+]
References ↑1 Negishi, M., Pederson, L.G., Petrochenko, E., Shevtsov, S., Gorokhov, A., Kakuta, Y., Pederson, L.C. (2001). Structure and function of sulfotransferases. Archives of biochemistry and biophysics. 390(2). 149-157. Available at: https://doi.org/10.1006/abbi.2001.2368 ↑2 Gamage, N., Barnett, A., Hempel, N., Duggleby, R.G., Windmill, K.F., Martin, J.L., McManus, M.E. (2006). Human Sulfotransferases and Their Role in Chemical Metabolism. Toxicological Sciences. 90(1). 5-22. Available at: https://doi.org/10.1093/toxsci/kfj061 ↑3 National Library of Medicine. (2024). SULT1A1 sulfotransferase family 1A member 1 [Homo sapiens (human)]. NIH. Available at: https://www.ncbi.nlm.nih.gov/gene?Cmd=DetailsSearch&Db=gene&Term=6817 (Accessed: 03 June 2024) ↑4 Ramos, P.M., Gohad, P., McCoy, J., Wambier, C., Goren, A. (2021). Minoxidil Sulfotransferase Enzyme (SULT1A1) Genetic Variants Predicts Response to Oral Minoxidil Treatment for Female Pattern Hair Loss. Journal of the European Academy of Dermatology and Venereology: JEADV. 35(1). E24-e26. Available at: https://doi.org/10.1111/jdv.16765 ↑5 Goren, A., Castano, J.A., McCoy, J., Bermudez, F., Lotti, T. (2014). Novel enzymatic assay predicts minoxidil response in the treatment of androgenetic alopecia. Dermatologic Therapy. 27. 171-173. Available at: https://doi.org/10.1111/dth.12111 ↑6 Goren, A., Castano, J.A., McCoy, J., Bermudez, F., Lotti, T. (2014). Novel enzymatic assay predicts minoxidil response in the treatment of androgenetic alopecia. Dermatologic Therapy. 27. 171-173. Available at: https://doi.org/10.1111/dth.12111 ↑7 Roberts, J., Desai, N., McCoy, J., Goren, A. (2014). Sulfotransferase activity in plucked hair follicles predicts response to topical minoxidil in the treatment of female androgenetic alopecia. Dermatologic Therapy. 27(4). 252-254. Available at https://doi.org/10.1111/dth.12130 ↑8 Raftogianis, R.B., Wood, T.C., Otterness, D.M., Loon, J.A.V., Weinshilboum, R.M. (1997). Phenol Sulfotransferase Pharmacogenetics in Humans: Association of Common SULT1A1 Alleles with TS PST Phenotype. Biochemical and Biophysical Research Communications. 239(1). 298-304. Available at: https://doi.org/10.1006/bbrc.1997.7466 ↑9 Raghad, N.A., Al-Gazally, M.E., Ewahd, W.A. (2017). Assessment the effect of different genotypes of sulfotransferase 1A1 gene on the response to minoxidil in patients with androgenic alopecia. Journal of Global Pharma Technology. 10(9). 144-149 ↑10, ↑11, ↑12 Raghad, N.A., Al-Gazally, M.E., Ewahd, W.A. (2017). Assessment the effect of different genotypes of sulfotransferase 1A1 gene on the response to minoxidil in patients with androgenic alopecia. Journal of Global Pharma Technology. 10(9). 144-149 ↑13 Ramos, P.M., Gohad, P., McCoy, J., Wambier, C., Goren, A. (2021). Minoxidil Sulfotransferase Enzyme (SULT1A1) genetic variants predict response to oral minoxidil treatment for female pattern hair loss. Journal of the European Academy of Dermatology and Venererology. 35(1). E24-e26. Available at: https://doi.org/10.1111/jdv.16765 ↑14 Ramos, P.M., Gohad, P., McCoy, J., Wambier, C., Goren, A. (2021). Minoxidil Sulfotransferase Enzyme (SULT1A1) genetic variants predict response to oral minoxidil treatment for female pattern hair loss. Journal of the European Academy of Dermatology and Venererology. 35(1). E24-e26. Available at: https://doi.org/10.1111/jdv.16765 ↑15 Ramos, P.M., Sinclair, R.D., Kasprzak, M., Miot, H.A. (2020). Minoxidil 1 mg oral versus minoxidil 5% topical solution for the treatment of female-pattern hair loss: a randomized clinical trial. Journal of the American Academy of Dermatology. 82(1): 252-253. Available at: https://doi.org/10.1016/j.jaad.2019.08.060 ↑16 Asilian, A., Farmani, A., Saber, M. (2023). Clinical efficacy and safety of low-dose oral minoxidil versus topical solution in the improvement of androgenetic alopecia: a randomized controlled trial. Journal of Cosmetic Dermatology. 23(3). 949-957. Available at: https://doi/org/10.1111/jocd.16086 ↑17 Sharma, A., Goren, A., Dhurat, R., Agrawal, S., Sinclair, R., Trueb, R., Vano-Galvan, S., Chen, G., Tan, Y., Kovacevic, M., Situm, M., McCoy, J. (2019). Tretinoin enhances minoxidil response in androgenetic alopecia patients by upregulating follicular sulfotransferase enzymes. Dermatologic Therapy. 32(3). e12915. Available at: https://doi.org/10.1111/dth.12915 ↑18 Sharma, A., Goren, A., Dhurat, R., Agrawal, S., Sinclair, R., Trueb, R., Vano-Galvan, S., Chen, G., Tan, Y., Kovacevic, M., Situm, M., McCoy, J. (2019). Tretinoin enhances minoxidil response in androgenetic alopecia patients by upregulating follicular sulfotransferase enzymes. Dermatologic Therapy. 32(3). e12915. Available at: https://doi.org/10.1111/dth.12915 ↑19 Sharma, A., Surve, R., Dhurat, R., Sinclair, R., Tan, Y., Zou, Y., Muller Ramos, R., Wambier, C., Verner, I., Kovacevic, M., Goren, A. (2020). Microneedling improves minoxidil response in androgenetic alopecia patients by upregulating follicular sulfotransferase enzymes. Journal of Biological Regulators & Homeostatic Agents. 34(2). 659-661. Available at: 10.23812/19-385-L-51 ↑20 Sharma, A., Surve, R., Dhurat, R., Sinclair, R., Tan, Y., Zou, Y., Muller Ramos, R., Wambier, C., Verner, I., Kovacevic, M., Goren, A. (2020). Microneedling improves minoxidil response in androgenetic alopecia patients by upregulating follicular sulfotransferase enzymes. Journal of Biological Regulators & Homeostatic Agents. 34(2). 659-661. Available at: 10.23812/19-385-L-51 GPR44 is a gene that encodes the G-protein-coupled receptor 44, also known as the prostaglandin D2 receptor (DP2). This receptor plays a pivotal role in various physiological processes, including inflammation and immune responses.
GPR44 is considered significant in the context of hair loss because some believe it is involved in hair growth inhibition.
Early studies evaluating prostaglandin activity in the hair follicle found that elevated levels of prostaglandin D2 (PGD2) have been found in the scalps of individuals with androgenic alopecia. PGD2 exerts its effects through the GPR44 receptor.
This article will delve into the importance of the GPR44 gene in hair loss, its potential as a therapeutic target, and the significant role that understanding your genetic makeup can play in making informed treatment decisions.
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is GPR44?
The GPR44 gene (also called CRTh2) codes for the expression of a type of receptor for prostaglandins, specifically PGD2.[1]National Library of Medicine. (2024). PTGDR2 Prostaglandin D2 Receptor 2 [Homo sapiens (human)]. NIH. Available at: https://www.ncbi.nlm.nih.gov/gene/11251 (Accessed: 12 July 2024.) Prostaglandin D2 is a bioactive lipid compound that belongs to the family of prostaglandins, which are derived from arachidonic acid. Prostaglandins are involved in various physiological processes, including inflammation, allergic reactions, and regulation of sleep-wake cycles. PGD2 is produced by several types of cells, including mast cells, dendritic cells, and other types of immune cells.
Studies suggest that PGD2 has been found to inhibit hair growth in isolated human hair follicles and mice. Furthermore, PGD2 has been found to be elevated in the scalps of balding men diagnosed with androgenetic alopecia.[2]Nieves, A., Garza, L.A. (2014). Does Prostaglandin D2 Hold the Cure to Male Pattern Baldness? Experimental Dermatology. 23(4). 224-227. Available at: https://doi.org/10.1111/exd.12348[3]Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). … Continue reading
What is the Evidence for Targeting GPR44 for Hair Loss?
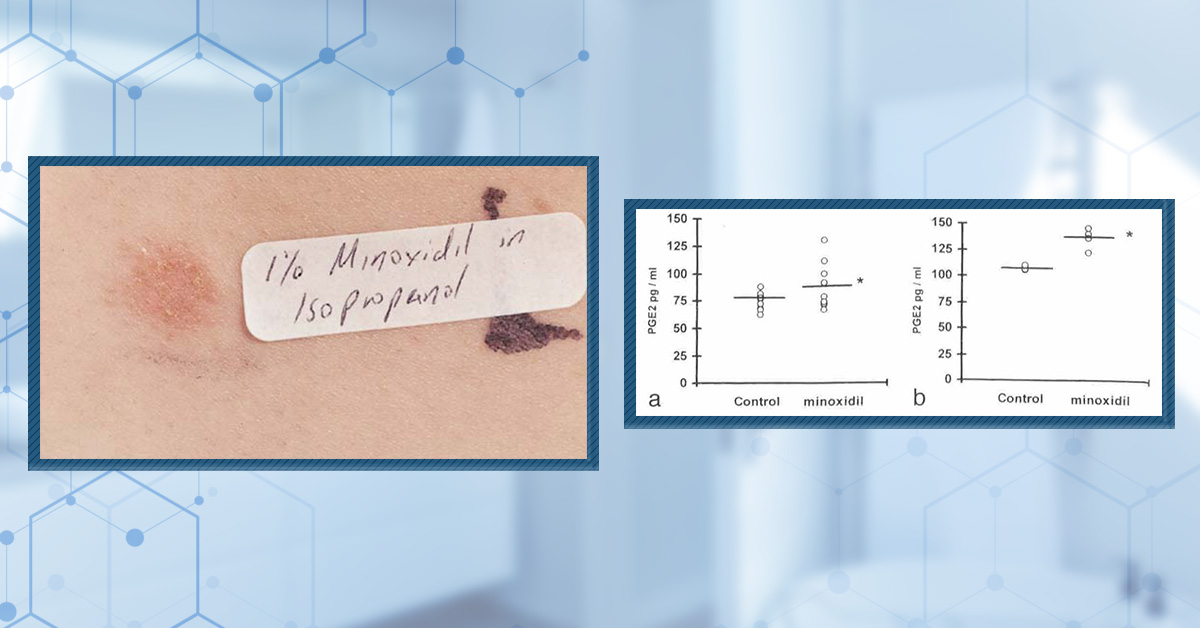
As mentioned above, PGD2 binds to its receptor, GPR44, to exert its effects. Studies on human scalp samples from the bald and haired areas of balding men found that the level of PGD2 was significantly higher in the scalps of the balding areas (Figure 1). Furthermore, PGE2, which has been linked to human hair growth, was found to be significantly lower in the bald scalp (Figure 1).[4]Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). … Continue reading

Figure 1: Fold change in PGD2, 15-dPGJ2, and PGE2 expression in the bald scalp compared to the haired scalp. *P<0.05; **P<0.01.[5]Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). … Continue reading
The same study evaluated the effect of high levels of PGD2 in mouse skin, hypothesizing that it might lead to the initiation of features of androgenic alopecia. The researchers used K14-Ptgs2 transgenic mice that are genetically modified to overexpress the Ptgs2 gene (also known as COX-2) specifically in the skin. These mice are often used in prostaglandin signaling studies as these specific genetic modifications increase levels of PGD2, PGE2, and 15-dPGJ2.
The mice overexpressing this gene were found to have hair follicles that entered premature catagen with subsequent development of alopecia.[6]Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). … Continue reading
In a series of experiments, researchers investigated the effects of prostaglandin D2 (PGD2) on hair growth using C57Bl/6 mice, a common laboratory strain. They topically applied PGD2 to the shaved backs of these mice and measured hair length 20 days after depilation.
The results showed a significant inhibition of hair growth in the treated areas. To further explore the mechanism, the team used a separate mouse model with the GPR44 gene (which encodes a PGD2 receptor) knocked out. Interestingly, these GPR44-deficient mice demonstrated resistance to hair loss when PGD2 was applied topically, indicating that PGD2’s effect on hair loss was through the GPR44 receptor.[7]Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). … Continue reading

Figure 2. Hair length 10 days after topical PGD2 (1 ug), 15-dPGJ2 (1 ug) or vehicle treatment.[8]Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). … Continue reading
Clinical studies have found an association between the rs533116 and rs545659 polymorphisms of the GPR44 gene that enhances the expression of GPR44 in the lungs, resulting in an increase in asthma severity.[9]Campos Alberto, E., Maclean, E., Davidson, C., Palikhe, N.S., Storie, J., Tse, C., Brenner, D., Mayers, I., Vliagoftis, H., El-Sohemy, A., Cameron, L. (2012). The Single Nucleotide Polymorphism CRTh2 … Continue reading[10]Huang, J.L., Gao, P.S., Mathias, R.A., Yao, T.C., Chen, L.C., Kuo, M.L., Hsu, S.C., Plunkett, B., Togias, A., Barnes, K.C., Stellato, C., Beaty, T.H., Huang, S.K. Sequence Variants of the Gene … Continue reading
This increase in the expression of receptors like GPR44 may increase responsiveness to PGD2, so it’s possible that these findings may also apply to people with androgenic alopecia.
What is the Evidence Against Targeting GPR44 for Hair Loss?
In 2012, a study from the University of Pennsylvania and Johns Hopkins University generated a lot of excitement about a potential new treatment avenue for hair loss. The researchers found that PGD2 was elevated in the balding scalp but not in non-balding areas of the scalp of men with hair loss. Furthermore, they found that PGD2 inhibits hair growth.[11]Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). … Continue reading. This sparked an interest in prostaglandins as hair growth inhibitors.
Unfortunately, follow-up studies showed conflicting results – thanks to poorly controlled variables – and it is still unclear whether there is a causal relationship between prostaglandins and androgenetic alopecia.[12]English, R., Ruiz, S. (2021). Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia: Are Biopsy Location, Hair Diameter Diversity, and Relative Hair Follicle … Continue reading
A randomized, double-blind, placebo-controlled Phase 2a trial on setipiprant, a drug designed to bind to GPR44 and block PGD2 from exerting its effect, was conducted on males aged 18-49 with androgenic alopecia. The study found that setipiprant at 1000 mg twice daily for 24 weeks did not demonstrate efficacy compared to a placebo in improving hair growth, as measured by target area hair count and participant self-assessment. While setipiprant was safe and well-tolerated, it failed to show significant improvements indicating that targeting PGD2 alone is not sufficient to treat male pattern hair loss.[13]DuBois, J., Bruce, S., Stewart, D., Kempers, S., Harutunian, C., Boodhoo, T., Weitzenfeld, A, Chang-Lin, J.E. (2021). Setipiprant for Androgenetic Alopecia in Males: Results from a Randomized, … Continue reading
What Do Your Genetic Results Mean?
Your Result GPR44-1 Variant 1 GPR44-2 Variant 2 Rs545659 TT Rs545659 AA What it means May be at a lower risk of having elevated levels of PGD2 in the lungs/scalp. May be at an increased risk of having higher levels of GPR44 in the lungs/scalp. The Implication You might not be a good candidate for PGD2 inhibitors as a treatment for hair loss You might be a better candidate for PGD2 inhibitors as a treatment for hair loss Your Result GPR44-1 Variant 1 GPR44-2 Variant 2 GPR44-2 Variant 3 Rs533116 AA Rs533116 GG Rs533116 GA What it means May be at a lower risk of having elevated levels of PGD2 In the lungs/scalp. May be at moderate risk of having higher levels of GPR44 in the lungs/scalp. May be at an increased risk of having higher levels of GPR44 in the lungs/scalp. The Implication You might not be a good candidate for PGD2 inhibitors as a treatment for hair loss You might be an average candidate for PGD2 inhibitors as a treatment for hair loss You might be a better candidate for PGD2 inhibitors as a treatment for hair loss What Relevance Does GPR44 Have for Hair Loss Treatment?
We have also created a rubric that helps to determine the relevance of a specific gene to hair loss based on the quality of the evidence in the above studies.
- Does this gene have any potential relevance for hair loss? (1 point)
Yes, initial studies have shown that PGD2 levels are increased in the scalps of balding men. Experiments in mice suggest that PGD2 may inhibit hair growth. (score = 1)
- Does the totality of evidence implicate GPR44 as a causal agent for hair loss? (1 point)
There is not enough consistency of evidence to support the relationship between prostaglandin activity and androgenetic alopecia, due to further results conflicting with initial results. (score = 0)
- Does the totality of evidence implicate GPR44 as a predictive factor for hair loss treatment responsiveness? (2 points)
Although earlier studies showed that PGD2 is elevated in balding scalps, targeting this has not shown to be effective at treating hair loss. (score = 0)
- Is this quality of evidence on (3) strong enough to influence treatment recommendations? (1 point)
No score on number (3). (score = 0)
Total Score = 1
Final Thoughts
While early research has highlighted the potential involvement of the GPR44 gene in hair loss through its interaction with prostaglandin D2 (PGD2), the current evidence is not robust enough to make definitive treatment recommendations based solely on the GPR44 genotype. Therefore, more comprehensive and consistent research is needed to validate the role of GPR44 in hair loss and its potential as a predictive factor for treatment responsiveness.
References[+]
References ↑1 National Library of Medicine. (2024). PTGDR2 Prostaglandin D2 Receptor 2 [Homo sapiens (human)]. NIH. Available at: https://www.ncbi.nlm.nih.gov/gene/11251 (Accessed: 12 July 2024.) ↑2 Nieves, A., Garza, L.A. (2014). Does Prostaglandin D2 Hold the Cure to Male Pattern Baldness? Experimental Dermatology. 23(4). 224-227. Available at: https://doi.org/10.1111/exd.12348 ↑3, ↑4, ↑6, ↑7 Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). Prostaglandin D2 Inhibits Hair Growth and is Elevated in Bald Scalp of Men with Androgenetic Alopecia. Science Translational Medicine. 4(126). 1-21. Available at: https://doi.org/10.1126/scitranslmed.3003122 ↑5, ↑8, ↑11 Garza, L.A., Liu, Y., Alagesan, B., Lawson, J.A., Norberg, S.M., Loy, D.R., Zhao, T., Blatt, H.B., Stanton, D.C., Carrasco, L., Ahluwalia, G., Fischer, S.M., Fitzgerald, G.A., Cotsarelis, G. (2012). Prostaglandin D2 Inhibits Hair Growth and is Elevated in Bald Scalp of Men with Androgenetic Alopecia. Science Translational Medicine. 4(126). 1-21. Available at: https://doi.org/10.1126/scitranslmed.3003122 ↑9 Campos Alberto, E., Maclean, E., Davidson, C., Palikhe, N.S., Storie, J., Tse, C., Brenner, D., Mayers, I., Vliagoftis, H., El-Sohemy, A., Cameron, L. (2012). The Single Nucleotide Polymorphism CRTh2 rs533116 is Associated with Allergic Asthma and Increased Expression of CRTh2. Allergy. 67(11). 1357-1364. Available at: https://doi.org/10.1111/all.12003 ↑10 Huang, J.L., Gao, P.S., Mathias, R.A., Yao, T.C., Chen, L.C., Kuo, M.L., Hsu, S.C., Plunkett, B., Togias, A., Barnes, K.C., Stellato, C., Beaty, T.H., Huang, S.K. Sequence Variants of the Gene Encoding Chemoattractant Receptor Expressed on Th2 Cells (CRTH2) are Associated with Asthma and Differentially Influence mRNA Stability. Human Molecular Genetics. 13(21). 2691-2697. Available at: https://doi.org/10.1093/hmg/ddh279 ↑12 English, R., Ruiz, S. (2021). Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia: Are Biopsy Location, Hair Diameter Diversity, and Relative Hair Follicle Miniaturization Partly to Blame? Clinical, Cosmetic, and Investigational Dermatology. 14. 357-365. Available at: https://doi.org/10.2147/CCID.S306157 ↑13 DuBois, J., Bruce, S., Stewart, D., Kempers, S., Harutunian, C., Boodhoo, T., Weitzenfeld, A, Chang-Lin, J.E. (2021). Setipiprant for Androgenetic Alopecia in Males: Results from a Randomized, Double-Blind, Placebo-Controlled Phase 2a Trial. Clinical Cosmetic and Investigative Dermatology. 14. 1507-1517. Available at: https://doi.org/10.2147/CCID.S319676 HMI-115 is a potential new treatment for hair loss that is licensed by Hope Medicine Inc. HMI-115 has been used in a phase 1 clinical trial for hair loss and has been approved by the FDA for phase 2 trials. This treatment is also in phase 2 clinical trials for use in endometriosis. HMI-115 is gathering media attention as a treatment that may come to the market within the next few years.
HMI-115 belongs to a class of drugs known as prolactin (PRL) receptor antagonists – it works by blocking the effects of prolactin within the hair follicle by binding to and blocking the prolactin receptor. In this article, we will take a look at what HMI-115 and prolactin are and then consider how prolactin might be involved in hair follicle biology and hair loss disorders. Furthermore, we will investigate the potential impact of HMI-115 in treating androgenetic alopecia and determine whether it is likely that phase 2 clinical trials for HMI-115 will return positive results.
Key Takeaways
- Drug. HMI-115 is a drug that comes under a class of therapeutics called prolactin receptor antagonists. This drug is licensed by Bayer, which is investigating its use as a drug treatment for endometriosis. HMI-115 is also licensed by Hope Medicine Inc., which used the drug in a phase 1 clinical trial for patients with androgenetic alopecia. The FDA has also approved HMI-115 for phase 2 trials for treating hair loss, although these trials have not yet started.
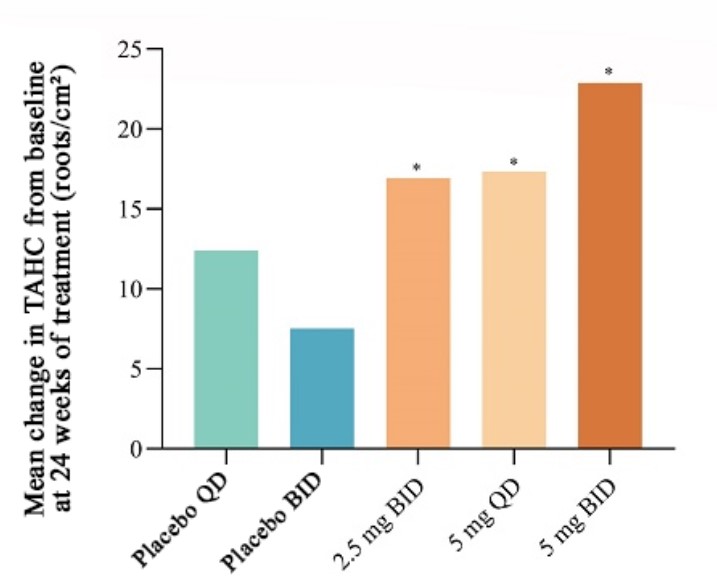
- Clinical Data. In a press release, Hope Medicine Inc. reported results from its phase 1 trial, which included a significant increase in the mean non-vellus total area hair count across the 12 males in the trial—an increase of 14 hairs/cm2 after 24 weeks. The study has not been peer-reviewed, nor have the full results been published. Furthermore, no data was provided for the 4 women included in the study.
- Safety. There was a phase 1 safety trial completed by Bayer (who licensed HMI-115 to Hope Medicine Inc.) in which up to 90 mg of the drug, delivered via subcutaneous injections every 2 weeks, was found to be well tolerated. This study, however, aimed toward using HMI-115 to treat endometriosis. The phase 1 clinical trial on hair loss, sponsored by Hope Medicine Inc., delivered 240mg of HMI-115 via subcutaneous injection every two weeks; they reported it to be safe and tolerable, though no supporting data was provided.
- Evidence Quality. HMI-115 serum scored 21/100 for evidence quality, by our metrics (this is subject to change depending on the results of clinical trials currently being undertaken).
All-Natural Hair Supplement + Topical
The top natural ingredients for hair growth, all in one serum & supplement.
Take the next step in your hair growth journey with a world-class natural serum & supplement. Ingredients, doses, & concentrations built by science.

What is HMI-115?
HMI-115 (also known as BAY1158061) is a new pharmaceutical drug developed by a biopharmaceutical company called Bioinvent and licensed by Bayer – a German multinational pharmaceutical and biotechnology company. HMI-115 has been subsequently licensed from Bayer by Hope Medicine Inc. for use as a hair loss treatment. So far, research around HMI-115 is geared toward treating endometriosis and male and female pattern hair loss. In terms of administration, HMI-115 is delivered via subcutaneous injection.
HMI-115 is a prolactin receptor antagonistic antibody.[1]Hope Medicine, (no date). Clinical Development. Research and Development. Available at: https://www.hopemedinc.com/research-platform?tp2 (Accessed: 21 April 2023) This is a type of therapeutic antibody that binds to the prolactin receptor, thereby inhibiting its activity by stopping prolactin from binding to its receptor.[2]Ferraris, J., Bernichten, S., Pisera, D., Goffin, V. (2013). Use of prolactin receptor antagonists to better understand prolactin regulation of pituitary homeostasis. Neuroendocrinology. 98. 171-179. … Continue reading Prolactin is a type of hormone produced by the pituitary gland. As indicated by its name, prolactin is a hormone that promotes lactation (milk production). In reality, prolactin is a pleiotropic hormone with many different functions in both men and women. We will go into more detail below about prolactin, its potential role in hair loss, and how HMI-115 might work to restore hair growth by inhibiting prolactin.
What is Hope Medicine Incorporated?
Hope Medicine Inc. is a Chinese biopharmaceutical company founded by Professor Rui Ping Xiao of Peking University. According to their website, Hope Medicine Inc. was founded on the basis of a thorough understanding of disease biology and the practical application of medical research.[3]Hope Medicine, (no date), About Hope Medicine. Available at: https://www.hopemedinc.com/ (Accessed: 21 April 2023) Hope Medicine Inc. focuses on developing small molecule drugs that target specific proteins or pathways involved in disease.
In 2019, Hope Medicine Inc. announced a license agreement with Bayer AG in which Hope Medicine will develop and commercialize HMI-115 as a treatment for male and female pattern hair loss, endometriosis, and other conditions.[4]Cision, (no date), Hope Medicine announces global license agreement with Bayer AG to advance the development and commercialization of the monoclonal antibody directed against prolactin (PRL) … Continue reading
In 2022, Hope Medicine announced that the US Food and Drug Administration (FDA) had approved an application for HMI-115 to be used as an investigational new drug for the treatment of androgenetic alopecia or pattern hair loss, meaning that phase 2 clinical trials can begin in the US. Hope Medicine stated that the company’s plans for its phase 2 trial for androgenetic alopecia would be an international multi-center, randomized, double-blind, placebo-controlled study. Participating countries include the US, Australia, and others. [5]Cision, (no date), Hope Medicine announces a global license agreement with Bayer AG to advance the development and commercialization of the monoclonal antibody directed against prolactin (PRL) … Continue reading
Are these trials likely to work? Let’s get into the science of how this prolactin receptor antagonist, HMI-115, might function. First, we’ll take a deep dive into what prolactin is and how it might affect hair follicle biology.
What is Prolactin?
Prolactin is a hormone produced and secreted by the anterior pituitary gland. Prolactin is named for its stimulatory effect on lactation (milk production), but in actuality, prolactin has many different functions in both men and women.[6]Freeman, M.A., Kanyicska, B., Lerant, A., Nagy, Gyorgy. (2000). Prolactin: structure, function, and regulation of secretion. Physiological Reviews. 80(4), 1523-1631. Available at: … Continue reading The normal range of prolactin in non-pregnant women is below 25 ng/ml and in men, below 20 ng/ml.[7]Majumdar, A., Mangal, N.S. (2013). Hyperprolactinemia. Journal of Human Reproductive Sciences. 6(3). 168-175. Available at: https://doi.org/10.4103/0974-1208.121400
High levels of prolactin can lead to a medical condition called hyperprolactinemia. Symptoms of hyperprolactinemia can include irregular menstrual periods/loss of menstrual periods in women, decreased sex drive and erectile dysfunction in men, infertility, overproduction of breast milk in non-pregnant or non-breastfeeding women, and also osteoporosis.[8]Capozzi, A., Scambia, G., Pontecorvi, A., Lello, S. (2015). Hyperprolactinemia: pathophysiology and therapeutic approach. Gynecological Endocrinology. 31(7). 506-510. Available at: … Continue reading
It is also thought that high prolactin levels may also be involved in hair loss (more on that below).[9]Schmidt, J.B. (1994). Hormonal basis of male and female androgenic alopecia: clinical relevance. Skin Pharmacology. 7. 61-66. Available at: https://doi.org/10.1159/000211275
How is Prolactin Involved in Hair Cycling and Loss?
Prolactin upregulates several molecular signaling pathways that are associated with hair loss. For example, the Janus kinase-signal transducer and activator of transcription (JAK/STAT) pathway is activated by prolactin.[10]Ma, F.Y., Anderson, G.M., Gunn, T.D., Goffin, V., Grattan, D.R., Bunn, S.J. (2005). Prolactin specifically activates signal transducer and activator of transcription 5b in neuroendocrine dopaminergic … Continue reading The JAK/STAT pathway is known to be involved in hair loss in patients with alopecia areata; therefore, elevated prolactin levels may subsequently enhance the JAK/STAT pathway, leading to worse severity of the disease.
Prolactin and prolactin receptors are expressed at both the mRNA and protein levels in the hair follicle. Furthermore, both of these appear to be up-regulated in the late growing stage (anagen) into the transitional stage (catagen) of the hair follicle cycle.[11]Foitzik, K., Krause, K., Conrad, F., Nakamura, M., Funk, W., Paus, R. (2006). Human scalp hair follicles are both a target and a source of prolactin, which serves as an autocrine and/or paracrine … Continue reading The researchers also found that treatment of isolated human hair follicles with high doses of prolactin (around 400 ng/ml) resulted in significant inhibition of hair growth and premature transition into catagen compared to control hair follicles. Additionally, markers for cell growth and cell death were reduced and increased, respectively, following prolactin treatment. Hair follicles were also staged for the hair cycle following prolactin treatment, and there was a significant increase in the number of treated follicles in the catagen stage. These findings indicate that prolactin can impact hair follicle biology and that prolactin may function as an inducer of catagen.

Figure 1: Effect of 400 ng/ml of prolactin on (LEFT): hair follicle growth and (RIGHT): stage of the hair follicle cycle.[12]Foitzik, K., Krause, K., Conrad, F., Nakamura, M., Funk, W., Paus, R. (2006). Human scalp hair follicles are both a target and a source of prolactin, which serves as an autocrine and/or paracrine … Continue reading
In another study, in mice, it was found that prolactin is closely involved in regulating the hair follicle cycle. Prolactin levels increased in mice at 3 weeks, just before the onset of anagen (Figure 2), with a subsequent increase in the prolactin receptor at the start of the anagen stage. This increase in prolactin levels was associated with a concomitant increase in levels of prolactin receptors in the hair follicle. Suppression of prolactin secretion (through oral treatment of a known inhibitor of prolactin called bromocriptine) from the pituitary gland induced hair growth 3-5 days earlier, which was returned to normal by treating the mice with prolactin for 3 days. Increasing the duration of treatment had an inhibitory effect on hair growth.[13]Craven, A.J., Nixon, A.J., Ashby, M.G., Ormandy, C.J., Blazek, K., Wilkins, R.J., Pearson, A.J. (2006). Prolactin delays hair regrowth in mice. Journal of Endocrinology. 191. 415-425. Available at: … Continue reading

Figure 2: Levels of circulating prolactin in mice. Prolactin levels appear to increase at around 21 days (3 weeks) of age – around one week before the mice enter the anagen stage of the hair follicle cycle.[14]Craven, A.J., Nixon, A.J., Ashby, M.G., Ormandy, C.J., Blazek, K., Wilkins, R.J., Pearson, A.J. (2006). Prolactin delays hair regrowth in mice. Journal of Endocrinology. 191. 415-425. Available at: … Continue reading
There is some evidence demonstrating that prolactin is involved in regulating hair follicle cycling. However, is prolactin relevant to hair loss disorders in humans?
In women, hyperprolactinemia was found to be associated with androgenetic alopecia-pattern hair loss, as well as hirsutism (excess facial hair).[15]Schmidt, J.B. (1994). Hormonal basis of male and female androgenic alopecia: clinical relevance. Skin Pharmacology. 7. 61-66. Available at: https://doi.org/10.1159/000211275 A study involving 65 males (mean age of 24) and 46 females (mean age of 34) with androgenetic alopecia was conducted, and levels of different hormones were measured in comparison to 58 male and 45 female healthy controls. Prolactin, however, was only measured in the females in the study. Using a TRH test – which stimulates prolactin release from the pituitary – the researchers measured the levels of TRH-induced prolactin in both hair loss patients and controls (Figure 3). The researchers wanted to see whether the total stores of prolactin were increased in those with hair loss or whether the prolactin system was hypersensitive in some way. The female Patients were administered 0.2 mg of TRH and then had blood taken after 0 minutes, 20 minutes, and 40 minutes of treatment. Prolactin levels were then measured. This was taken during the luteal phase of the menstrual cycle (around day 14 to 28) when prolactin levels were higher than normal. It is important to note, however, that prolactin levels can be highly dynamic.
The researchers found an increase in prolactin levels at minute 0 and minute 20 following TRH administration in patients with androgenetic alopecia compared to the control patients, but these results were not statistically significant. However, there was a significant increase in prolactin levels after 40 minutes of TRH administration (p=<0.05). In conclusion, the findings of this study suggest that prolactin levels may be elevated in patients with androgenetic alopecia.

Figure 3: Median basal and stimulated levels of prolactin (PRL) and thyroid stimulating hormone (TSH), 0 minutes, 20 minutes, and 40 minutes after stimulation with TRH in female hair loss patients and controls. Adapted from:[16]Schmidt, J.B. (1994). Hormonal basis of male and female androgenic alopecia: clinical relevance. Skin Pharmacology. 7. 61-66. Available at: https://doi.org/10.1159/000211275
Another study looked at 40 women (aged between 30 and 65) with moderately increased prolactin levels, alongside androgenetic alopecia or diffuse hair loss, to determine the effects that prolactin might have on hair loss.[17]Lutz, G. (2011). Hair loss and hyperprolactinemia in women. Dermato-Endocrinology. 4(1). 70-76. Available at: https://doi.org/10.4161/der.19472 Prolactin levels varied widely in these patients, with the lowest level being 25.1 ng/ml and the highest being 1390 ng/ml. Interestingly, there did not appear to be any correlation between the number of non-growing hairs and prolactin levels, leading the researchers to conclude that it was not likely that elevated prolactin levels were the cause of diffuse or androgenetic alopecia (Figures 4 & 5).

Figure 4: Prolactin levels in patients with either diffuse or androgenetic alopecia. Adapted from:[18]Lutz, G. (2011). Hair loss and hyperprolactinemia in women. Dermato-Endocrinology. 4(1). 70-76. Available at: https://doi.org/10.4161/der.19472

Figure 5: Number of telogen hairs of patients with either diffuse or androgenetic alopecia. Vertical axis = the number of telogen hairs; Horizontal axis = patient. Adapted from: [19]Lutz, G. (2011). Hair loss and hyperprolactinemia in women. Dermato-Endocrinology. 4(1). 70-76. Available at: https://doi.org/10.4161/der.19472
A case-control study of 30 patients (16 men and 14 women) aged between 18-46 with alopecia areata (AA) and 20 controls (9 males and 11 females) aged between 18-45 was undertaken.[20]Tahlawi, S.M.E., Eishi, N.H.E., Kahhal, R.K., Hegazy, R.A., Hanafy, G.M.E., Hay, R.M.A., Shaker, O.G. (2018). Do prolactin and its receptor play a role in alopecia areata? Indian Journal of … Continue reading When comparing the serum prolactin level between AA patients and controls using an ELISA assay, no significant differences were found. PCRs were then completed with RNA harvested from biopsies taken from the lesional skin of AA patients and the occipital scalp skin of controls. An increase in the level of prolactin receptors was observed in the AA patients compared to the control patients (Figure 6). This indicates a potential hypersensitivity to prolactin in patients with AA rather than excess prolactin.

Figure 6: Comparison of the mean serum prolactin level and mean tissue prolactin receptor levels in AA patients vs. control patients. Adapted from:[21]Tahlawi, S.M.E., Eishi, N.H.E., Kahhal, R.K., Hegazy, R.A., Hanafy, G.M.E., Hay, R.M.A., Shaker, O.G. (2018). Do prolactin and its receptor play a role in alopecia areata? Indian Journal of … Continue reading
Furthermore, the levels of prolactin receptors correlate with the SALT score (Severity of Alopecia Tool) – a common score used in studies to assess the extent of scalp hair loss.
Overall, some evidence implicates prolactin in the pathogenesis of androgenetic alopecia. However, there are some contradicting findings about whether prolactin is involved in the pathogenesis of hair loss. Moreover, one might expect there to be more of a concrete link between pregnancy and hair loss, given the large changes in prolactin that occur during late pregnancy and throughout breastfeeding. However, there is little evidence of changes in hair loss and ratios of anagen/telogen hairs between different stages of pregnancy or breastfeeding status.[22]Mirallas, O., Grimalt, R. (2016). The postpartum telogen effluvium fallacy. 1(4), 198-201. Available at: https://doi.org/10.1159/000445385
However, given the caveats above, let us assume for a moment that prolactin is a definitive cause of hair loss, so why not just use already-known treatments for hyperprolactinemia, such as the drug cabergoline?
A major mechanism regulating prolactin levels is dopamine secretion by neurons in the hypothalamus. Dopamine then inhibits the secretion of prolactin from the pituitary. Cabergoline is a dopamine agonist and so promotes the action of dopamine. Some case studies have indicated that dopamine agonists like cabergoline may cause hair loss in some people. One such study included a 71-year-old woman with Parkinson’s disease who experienced progressive hair loss after taking 3 mg of cabergoline for one month. After 4 months of decreasing the dose, however, (from 3 mg to 1 mg), the patient’s hair was completely re-grown.[23]Miwa, H., Kondo, T. (2003). Hair loss induced by dopamine agonist: case report and review of the literature. Parkinsonism & Related Disorders. 10. 51-52. Available at: … Continue reading An earlier study also reports two women suffering from diffuse alopecia as a result of taking levodopa (dopamine replacement) as a treatment for Parkinson’s.[24]Marshall, A., Williams M.J. (1971). Alopecia and levodopa. British Medical Journal. 2(5752), 47. Available at: https://doi.org/10.1136/bmj.2.5752.47 Whether dopaminergic drugs could benefit hair loss in otherwise healthy people is unclear. In any case, given the widespread importance of dopamine in regulating mood and behavior, targeting this system as a therapy for hair loss may not be a wise strategy. Therefore, other pharmaceutical approaches, like the blockade of prolactin receptors, may be a better method. That is if prolactin is indeed related to hair loss.
So, let’s have a look at whether there is any evidence currently to suggest that the prolactin receptor antagonist HMI-115 might benefit those with hair loss.
Could HMI-115 work for Patients with Androgenetic Alopecia?
Recent data showing the potential effects of HMI-115 in humans has been released, but let’s first look at the published animal data.
Animals
Bayer AG did complete a study using a primate model of androgenetic alopecia, which Bayer AG goes into detail about in their patent application.[25]Ekkehard, M., Joachim, S., Jorn, K., Christiane, O. (2017). Prolactin receptor antibody for male and female pattern hair loss. World Intellectual Property Organization. Available at: … Continue reading Unfortunately, this study does not appear to be published anywhere other than in the patent application that we found on Google (such as in a peer-reviewed scientific journal).
This study attempted to leverage an apparent phenomenon of spontaneous post-adolescence scalp hair loss in stump-tailed macaques as a model system to test the effects of HIM-115. Over a period of 6 months, the macaques were treated with HMI-115. The researchers claim that terminal hairs nearly doubled throughout the treatment. Unfortunately, the data is only given in terms of change from baseline, and there does not seem to be an untreated control group, which makes it difficult to conclude whether HMI-115 is doing anything (Figure 7).

Figure 7: Effect of HMI-115 treatment on Hair Growth in Stump-Tailed Macaques with Androgenetic Alopecia over 24 weeks. Adapted from:[26]Ekkehard, M., Joachim, S., Jorn, K., Christiane, O. (2017). Prolactin receptor antibody for male and female pattern hair loss. World Intellectual Property Organization. Available at: … Continue reading
Humans
There are two clinical trials currently recruiting for HMI-115: one phase 2 trial for endometriosis-associated pain and another phase 2 trial for treating male androgenetic alopecia over 24 weeks.[27]Clinical Trials, (no date). HMI-115. Available at: https://clinicaltrials.gov/ct2/results?cond=&term=HMI-115&cntry=&state=&city=&dist= (Accessed: 02 May 2024) The latter of the two follows on from a now complete phase 1 trial, whereby HMI-115 was tested as a treatment for male and female androgenetic alopecia.[28]Hope Medicine. (2023). An Open Label Study, to Evaluate Safety, Tolerability, and Efficacy in Male and Female With Androgenetic Alopecia Treated With HMI-115 Over a 24-Week Treatment Period (Clinical … Continue reading Importantly, this means that we have some information regarding the efficacy and safety of HMI-115 in humans – here’s what they found.
The study investigated the potential of HMI-115 as a treatment for both male and female androgenetic alopecia. 12 male and 4 female participants were given 240mg of HMI-115 every two weeks by subcutaneous injection for 24 weeks. The primary measurement was a change in target area hair count (TAHC) of non-vellus hair from baseline (week 0) to week 24.
In a press release, Hope Medicine Inc. (the sponsor of the trial) stated that “HMI-115 demonstrated positive efficacy results. It is also safe and well-tolerated”.[29]Hope Medicine. (No date). Positive Outcome from a Phase Ib Study in Australia Treating Patients with Androgenic Alopecia. Hope Medicine Available at: https://www.hopemedinc.com/company-release-37 … Continue reading. The press release also showed that the mean non-vellus TAHC increased by 14 hairs/cm2 in the male group, which was reported as a statistically significant increase. Hope Medicine Inc. acknowledges that this is the first indication that a prolactin blockade receptor may promote hair growth in patients with androgenetic alopecia, potentially opening the door for its use as a novel therapeutic.
While this does sound promising, there are several drawbacks. First and foremost, these results have (at the time of writing) only been shared as a press release. This means that the study and the results have not been peer-reviewed. In other words, no external reviewers have evaluated the study and ensured its integrity.[30]Kelly, J., Sadeghieh, T., Khosrow, A. (2014). Peer Review in Scientific Publications: Benefits, Critiques, & A Survival Guide. eJIFCC. 25(3). 227-243. PMID: 27683470 The lack of peer review means that we can’t be sure that unwanted results have not been omitted. Of the single measurement that has been reported, change in non-vellus TAHC, it is difficult to contextualize an increase of 14 hairs/cm2 – is that a large, moderate, or small change?
Furthermore, the study was conducted on a small number of participants. Generally speaking, the greater the sample size, the more reliable the results. In testing just 12 males and 4 females, the statistical power is low, and there is a risk of obtaining false-positive and false-negative results.[31]Andrade, C., (2020). Sample Size and its Importance in Research. Indian Journal of Psychological Medicine. 42(1). 102-103. Available at: https://doi.org/10.4103/IJPSYM.IJPSYM_504_19
On the one hand, it can be difficult to determine outliers, subjects who differ greatly from the average. For example, a few hyper-responders could see huge increases in their TAHC and cause the mean change of the group to be significant, while the majority of the subjects see no change. On the other hand, small sample sizes can obscure meaningful changes and smaller positive effects that do not reach significance. In either case, small sample sizes do not offer a good estimation of how the treatment may perform in the wider population. Furthermore, Hope Medicine didn’t include any results for the 4 women included, but it is unlikely that there would have been any statistically significant differences anyway.
With that said, HMI-115 does seem to have produced some positive effects, and the phase 2 trial should address some of the issues that hold back its phase 1 counterpart.
What are the Chances of HMI-115 Making it Through Phase 2 Clinical Trials?
So, as mentioned, Hope Medicine Inc. has been approved by the FDA to conduct Phase 2 clinical trials, and they are currently attempting to recruit 180 males with androgenetic alopecia for another 24-week study.
This may sound promising, but, in actual fact, phase 2 trials are generally considered to be the biggest milestone in drug development. The biggest reasons that phase 2 testing might fail are:
- Previously unknown serious side effects occur
- The trial shows insufficient efficacy – i.e., it doesn’t work as well as the researchers initially thought
- Poor commercial viability
It should also be noted that more than 30% of drugs entering phase 2 studies fail to progress, and more than 58% of drugs that do progress then go on to fail in phase 3 trials.[32]Norman, G.A.V. (2019). Phase II trials in drug development and adaptive trial design. JACC Basic to Translational Science. 4(3). 428-437. Available at: https://doi.org/10.1016/j.jacbts.2019.02.005
While the odds are stacked against anyone trying to get their drug through phase 2 clinical trials, the phase 1 trial did provide some hope for HMI-115. Although the study has a number of drawbacks, if the positive effect seen in the males is true (and that’s a big ‘if’), then it provides the best (and only) indication thus far that prolactin receptor blockades may be compatible as a treatment for androgenetic alopecia.
Is HMI-115 Safe?
A safety study was conducted by Bayer AG in a randomized controlled trial with 29 healthy postmenopausal women.[33]Nave, R., Jodi, S., Hoffman, A., Gashaw, I., Zollmann, F., Berse, M., Hochel, J., Kratzschmar, J., Rohde, B. (2019). Monoclonal antibody against prolactin receptor: a randomized placebo-controlled … Continue reading
Participants were split into four groups and administered either HMI-115 or a placebo via subcutaneous injection. Treatments were administered either once every two weeks or once every 3 weeks. The treatment doses were 30 mg (14-day interval), 60 mg (28-day interval), or 90 mg (14-day interval) of HMI-115 or a placebo control on three occasions.
The most frequently occurring adverse events in more than 10% of all study participants (including placebo) were headache, nasopharyngitis (common cold), nausea, lower abdominal pain, injection site bruises, general weakness, back pain, hot flush, oral herpes, temperature increase, and pain in extremities. The adverse events in more than 10% of participants that were associated with HMI-115 were headache, lower abdominal pain, hot flush, and nausea. Compared to the placebo, the frequency of adverse events was not increased with HMI-115, and no dose-dependent increase in adverse event frequency was observed.
Furthermore, the treatment was slowly absorbed, reaching peak concentrations approximately 5 – 11 days after dosing. After the final 90 mg dose, HMI-115 was eliminated from the blood plasma around 16 days later. The researchers determined that the three different dosages of HMI-115 were well-tolerated in healthy postmenopausal women, with no allergic reactions seen.
It remains to be seen if HMI-115 is safe in the long term, or across a larger, more representative group of patients. Furthermore, this study was completed in the context of treating endometriosis; therefore, the number of treatments, the concentration of the drug, and the duration of treatment time may differ from those who may be administered this drug for hair loss disorders.
For comparison, the completed phase 1 clinical trial, which Hope Medicine Inc. sponsored, treated patients with androgenetic alopecia 240 mg of HMI-115 every 2 weeks via subcutaneous injection, which is much higher than the concentrations used in the safety study completed by Bayer.[34]Clinical Trials, (no date). HMI-115. Available at: https://clinicaltrials.gov/ct2/results?cond=&term=HMI-115&cntry=&state=&city=&dist= (Accessed: 21 April 2023) Hope Medicine Inc. reported that this delivery of HMI-115 proved safe and tolerable, though they did not provide any data to support this statement.
Is HMI-115 for Me?
Well, HMI-115 is not yet available, and it looks like it won’t be available for another few years, at least as we look to the beginning of the phase 2 trials. While it’s still too early to tell if this product will make it to the market, we look forward to seeing the full results from the phase 1 trial and those from further trials to come.
References[+]
References ↑1 Hope Medicine, (no date). Clinical Development. Research and Development. Available at: https://www.hopemedinc.com/research-platform?tp2 (Accessed: 21 April 2023) ↑2 Ferraris, J., Bernichten, S., Pisera, D., Goffin, V. (2013). Use of prolactin receptor antagonists to better understand prolactin regulation of pituitary homeostasis. Neuroendocrinology. 98. 171-179. Available at: https://doi.org/10.1159/000354701 ↑3 Hope Medicine, (no date), About Hope Medicine. Available at: https://www.hopemedinc.com/ (Accessed: 21 April 2023) ↑4 Cision, (no date), Hope Medicine announces global license agreement with Bayer AG to advance the development and commercialization of the monoclonal antibody directed against prolactin (PRL) receptor. CISION PR Newswire. Available at: https://en.prnasia.com/releases/apac/hope-medicine-announced-global-license-agreement-with-bayer-ag-to-advance-the-development-and-commercialization-of-the-monoclonal-antibody-directed-against-prolactin-prl-receptor-242094.shtml (Accessed: 21 April 2023) ↑5 Cision, (no date), Hope Medicine announces a global license agreement with Bayer AG to advance the development and commercialization of the monoclonal antibody directed against prolactin (PRL) receptor. CISION PR Newswire. Available at: https://en.prnasia.com/releases/apac/hope-medicine-announced-global-license-agreement-with-bayer-ag-to-advance-the-development-and-commercialization-of-the-monoclonal-antibody-directed-against-prolactin-prl-receptor-242094.shtml (Accessed: 21 April 2023) ↑6 Freeman, M.A., Kanyicska, B., Lerant, A., Nagy, Gyorgy. (2000). Prolactin: structure, function, and regulation of secretion. Physiological Reviews. 80(4), 1523-1631. Available at: https://doi.org/10.1152/physrev.2000.80.4.1523 ↑7 Majumdar, A., Mangal, N.S. (2013). Hyperprolactinemia. Journal of Human Reproductive Sciences. 6(3). 168-175. Available at: https://doi.org/10.4103/0974-1208.121400 ↑8 Capozzi, A., Scambia, G., Pontecorvi, A., Lello, S. (2015). Hyperprolactinemia: pathophysiology and therapeutic approach. Gynecological Endocrinology. 31(7). 506-510. Available at: https://doi.org/10.3109/09513590.2015.1017810 ↑9, ↑15, ↑16 Schmidt, J.B. (1994). Hormonal basis of male and female androgenic alopecia: clinical relevance. Skin Pharmacology. 7. 61-66. Available at: https://doi.org/10.1159/000211275 ↑10 Ma, F.Y., Anderson, G.M., Gunn, T.D., Goffin, V., Grattan, D.R., Bunn, S.J. (2005). Prolactin specifically activates signal transducer and activator of transcription 5b in neuroendocrine dopaminergic neurons. Endocrinology. 146(12). 5112-5119. Available at: https://doi.org/10.1210/en.2005-0770 ↑11, ↑12 Foitzik, K., Krause, K., Conrad, F., Nakamura, M., Funk, W., Paus, R. (2006). Human scalp hair follicles are both a target and a source of prolactin, which serves as an autocrine and/or paracrine promoter of apoptosis-driven hair follicle regression. The American Journal of Pathology. 168(3). 748-756. Available at: https://doi.org/10.2353/ajpath.2006.050468 ↑13, ↑14 Craven, A.J., Nixon, A.J., Ashby, M.G., Ormandy, C.J., Blazek, K., Wilkins, R.J., Pearson, A.J. (2006). Prolactin delays hair regrowth in mice. Journal of Endocrinology. 191. 415-425. Available at: https://doi.org/10.1677/joe.1.06685 ↑17, ↑18, ↑19 Lutz, G. (2011). Hair loss and hyperprolactinemia in women. Dermato-Endocrinology. 4(1). 70-76. Available at: https://doi.org/10.4161/der.19472 ↑20 Tahlawi, S.M.E., Eishi, N.H.E., Kahhal, R.K., Hegazy, R.A., Hanafy, G.M.E., Hay, R.M.A., Shaker, O.G. (2018). Do prolactin and its receptor play a role in alopecia areata? Indian Journal of Dermatology. 63(3), 241-245. https://doi.org/10.4103/ijd.IJD_590_17 ↑21 Tahlawi, S.M.E., Eishi, N.H.E., Kahhal, R.K., Hegazy, R.A., Hanafy, G.M.E., Hay, R.M.A., Shaker, O.G. (2018). Do prolactin and its receptor play a role in alopecia areata? Indian Journal of Dermatology. 63(3), 241-245. https://doi.org/10.4103/ijd.IJD_590_17 ↑22 Mirallas, O., Grimalt, R. (2016). The postpartum telogen effluvium fallacy. 1(4), 198-201. Available at: https://doi.org/10.1159/000445385 ↑23 Miwa, H., Kondo, T. (2003). Hair loss induced by dopamine agonist: case report and review of the literature. Parkinsonism & Related Disorders. 10. 51-52. Available at: https://doi.org/10.1016/S1353-8020(03)00058-0 ↑24 Marshall, A., Williams M.J. (1971). Alopecia and levodopa. British Medical Journal. 2(5752), 47. Available at: https://doi.org/10.1136/bmj.2.5752.47 ↑25 Ekkehard, M., Joachim, S., Jorn, K., Christiane, O. (2017). Prolactin receptor antibody for male and female pattern hair loss. World Intellectual Property Organization. Available at: https://patentimages.storage.googleapis.com/56/cc/a3/7d3ac32f1537b2/WO2019011719A1.pdf (Accessed: 23 April 2023) ↑26 Ekkehard, M., Joachim, S., Jorn, K., Christiane, O. (2017). Prolactin receptor antibody for male and female pattern hair loss. World Intellectual Property Organization. Available at: https://patentimages.storage.googleapis.com/56/cc/a3/7d3ac32f1537b2/WO2019011719A1.pdf (Accessed: 23 April 2023) ↑27 Clinical Trials, (no date). HMI-115. Available at: https://clinicaltrials.gov/ct2/results?cond=&term=HMI-115&cntry=&state=&city=&dist= (Accessed: 02 May 2024) ↑28 Hope Medicine. (2023). An Open Label Study, to Evaluate Safety, Tolerability, and Efficacy in Male and Female With Androgenetic Alopecia Treated With HMI-115 Over a 24-Week Treatment Period (Clinical Trial Registration NCT05324293). Clinical Trials. (Accessed: 02 May 2024) ↑29 Hope Medicine. (No date). Positive Outcome from a Phase Ib Study in Australia Treating Patients with Androgenic Alopecia. Hope Medicine Available at: https://www.hopemedinc.com/company-release-37 (Accessed 2 May 2024) ↑30 Kelly, J., Sadeghieh, T., Khosrow, A. (2014). Peer Review in Scientific Publications: Benefits, Critiques, & A Survival Guide. eJIFCC. 25(3). 227-243. PMID: 27683470 ↑31 Andrade, C., (2020). Sample Size and its Importance in Research. Indian Journal of Psychological Medicine. 42(1). 102-103. Available at: https://doi.org/10.4103/IJPSYM.IJPSYM_504_19 ↑32 Norman, G.A.V. (2019). Phase II trials in drug development and adaptive trial design. JACC Basic to Translational Science. 4(3). 428-437. Available at: https://doi.org/10.1016/j.jacbts.2019.02.005 ↑33 Nave, R., Jodi, S., Hoffman, A., Gashaw, I., Zollmann, F., Berse, M., Hochel, J., Kratzschmar, J., Rohde, B. (2019). Monoclonal antibody against prolactin receptor: a randomized placebo-controlled study evaluating safety, tolerability, and pharmacokinetics of repeated subcutaneous administrations in postmenopausal women. Reproductive Sciences. 26(4). 523-531. Available at: https://doi.org/10.1177/1933719118776806 ↑34 Clinical Trials, (no date). HMI-115. Available at: https://clinicaltrials.gov/ct2/results?cond=&term=HMI-115&cntry=&state=&city=&dist= (Accessed: 21 April 2023) Pyrilutamide, also known as KX826, is an anti-androgenic drug with a mechanism of action similar to that of flutamide, albeit with potentially fewer side effects. Developed as a treatment for both androgenic alopecia and acne vulgaris, pyrilutamide is currently in phase III clinical trials in China and phase II clinical trials in the US. KX-826 is also included as the core ingredient of an anti-hair loss “cosmetic”, which is now being sold globally. In this ultimate guide, we’ll examine the available data on pyrilutamide: what it is, how it works, what the clinical studies show, and whom it might benefit.
Key Takeaways
- Drug. Pyrilutamide is an androgen receptor antagonist developed for treating androgenic alopecia and acne vulgaris. Topical pyrilutamide has completed phase III trials in China and phase II trials in the US and has recently gained approval for a trial using pyrilutamide in combination with minoxidil in China.
- Clinical Data. There have been five as yet unpublished trials that were conducted in either China or the US. We only have information about these trials from press releases or conference poster presentations. The key information we do have is bulleted below:
- A 24-week trial with 160 women with female pattern hair loss was conducted in China. The participants were randomized to six treatment groups (0.25% pyrilutamide applied once daily, 0.25% applied twice daily, 0.5% applied once daily, 0.5% applied twice daily, or two placebo groups – once daily and twice daily treatments). The 0.5% once-daily treatment appeared to perform the best, with an increase of 11.39 hairs per cm2 from the baseline compared to the placebo groups.
- A 24-week trial with 120 men with male-pattern hair loss was conducted in China. During the trial, the participants were randomized to four treatment groups (0.25% pyrilutamide applied twice daily, 0.5% applied once daily, 0.5% applied twice daily, or a placebo). This time, the 0.5% twice-daily treatment appeared to perform the best by the end of the 24 weeks, with an increase of 15.34 hairs per cm2 from the baseline compared to the placebo groups.
- A 24-week phase 1 trial investigating the safety, tolerability, and pharmacokinetics of pyrilutamide was conducted in the US. 40 men aged 18-60 with male-pattern hair loss were treated with ascending dose treatments of pyrilutamide (0.3%, 1.2%, 4.8%, and 9.6%). The study showed that the only reported adverse effects were mild contact dermatitis. Furthermore, pyrilutamide treatment was found to have a low risk of systemic effects, with low concentrations found in the blood after treatment.
- A 24-week phase 2 trial investigating the efficacy and safety of pyrilutamide was conducted in the US. 123 male patients with male-pattern hair loss were treated with either 0.25% once daily, 0.5% once daily, or 0.5% twice daily. The study showed that pyrilutamide improved hair counts by 10 hairs per cm2; however, no significant improvement was observed compared to the placebo.
- A 24-week phase 3 trial investigating the efficacy and safety of pyrilutamide was conducted in China. The participants were treated with either 0.5% pyrilutamide or a placebo. Similar to the phase 2 trial above, the study showed that pyrilutamide significantly improved hair counts compared to the baseline, however, no significant improvement was observed compared to the placebo.
- Evidence Quality. Pyrilutamide scored 37/100 for evidence quality by our metrics.
- Safety. Based on the information available, topical pyrilutamide treatment appears to be well-tolerated. However, none of the studies have been published, and there is the possibility that important information might have been omitted from the data that is available.
- Best Practices. From the limited data available, a concentration of 0.5% pyrilutamide (once daily for women and twice daily for men) appears to be the most effective pyrilutamide treatment regimen. It appears to be a well-tolerated treatment for androgenic alopecia.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is Pyrilutamide?
Pyrilutamide (also known as KX-826) is a topical nonsteroidal antiandrogen (NSAA) drug developed by Kintor Pharmaceuticals. It was developed as a treatment for androgenic alopecia and acne vulgaris, and the drug is currently undergoing phase III trials in China and phase II trials in the US.

Figure 1: Pyrilutamide molecular structure. Adapted from:[1]Pubchem, (no date). Pyrilutamide. NIH. Available at: https://pubchem.ncbi.nlm.nih.gov/substance/469676781 (Accessed: 04 May 2023)
What is the Link Between Pyrilutamide and Pattern Hair Loss?
Testosterone and dihydrotestosterone (or DHT) are androgens that have been implicated in pattern hair loss. To exert their effects, androgens must bind to the androgen receptor, and although the exact mechanisms are unknown, activating the androgen receptor in certain types of hair follicles appears to cause them to undergo miniaturization and eventually cause total hair loss.[2]Trueb, R.M., (2021). Understanding pattern hair loss-hair biology impacted by genes, androgens, prostaglandins, and epigenetic factors. Indian Journal of Plastic Surgery, 54(4). 385-392. Available … Continue reading Because pyrilutamide binds to and blocks the androgen receptor, in theory, it should help to prevent the negative effects of androgens on hair follicles.
How Does Pyrilutamide Work?
Pyrilutamide works in a different way than other anti-androgenic drugs, such as finasteride or dutasteride. Instead of inhibiting the enzyme 5α-reductase that catalyzes the conversion of testosterone to dihydrotestosterone, it competitively binds to the androgen receptor. This stops dihydrotestosterone and testosterone from binding to the receptor and exerting their effects.[3]Kintor, (2021), Kintor Pharmaceuticals Announced Successful Dosing of the First Batch of Patients for Acne Vulgaris Phase I/II Clinical Trial of Pyrilutamide. News Center. Available at: … Continue reading
Does Pyrilutamide Work to Regrow Hair?
There are currently no published data demonstrating the effects of pyrilutamide on hair loss; however, Kintor Pharmaceuticals has made some press announcements where they mention results from their clinical trials.
Study 1
The first study, looking at female androgenic alopecia, was a 24-week, multi-center, randomized, double-blind, placebo-controlled phase II trial conducted in China.[4]Cision PR Newswire, (2022), Kintor Pharma Announced the Primary Endpoint of Phase II Clinical Study for KX-826’s Treatment of Female Androgenetic Alopecia in China was Met. Available at: … Continue reading 160 female participants were randomly assigned to six treatment groups, including 0.25% pyrilutamide applied once daily, 0.25% applied twice daily, 0.5% applied once daily, and 0.5% applied twice daily, or placebo groups (one group for once daily, and one group for twice daily). The primary measured outcome was the change in hair growth, as measured by target area non-vellus hair count (TAHC). Essentially, the researchers were counting the number of thick, pigmented hairs (or ‘terminal’ hairs) in a given area, as opposed to the number of fine, unpigmented (vellus) hairs.
The researchers determined that the recommended dose for their phase III trial in China is 0.5% once daily, as it increased hairs by 11.39 counts per cm2 from baseline, compared to the placebo group. Furthermore, the researchers said that efficacy was seen as early as the end of week 12 of treatment. When it came to safety, the researchers mentioned that it was well tolerated, with mild adverse events seen that were similar to the placebo. Unfortunately, they do not mention what these adverse effects were.
Study 2
Another 24-week, randomized, double-blind, placebo-controlled, multi-regional study was conducted to evaluate the efficacy and safety of pyrilutamide in 120 men with androgenic alopecia.[5]Cision PR Newswire, (2023), Kintor Pharma Announces Completion of Subject Enrollment in Phase III Clinical Trial of KX-826 for Treatment of Male Androgenetic Alopecia in China. Available at: … Continue reading For this study, the researchers presented a poster at the 6th National Hair Academic Conference in China and it has since been translated to English online.
The participants were randomized into four groups:
- 0.25% pyrilutamide applied twice daily
- 0.5% pyrilutamide applied once daily
- 0.5% pyrilutamide twice daily
- Placebo (most likely treatment with just the cream or emollient that pyrilutamide is suspended in).
The researchers found that the participants that used 0.5% pyrilutamide twice daily showed improvement in total hair count at the end of the 24 weeks, with an increase of 15.34 hairs per cm2 compared to the placebo-treated groups (Figure 2).[6]Kintor Pharmaceutical Limited, (2022). Interim Results Announcement for the six months ended 30 June 2022. Kintor Pharmaceutical. 1-50. Available at: … Continue reading
It’s worth noting that the study reports that all the treatment groups demonstrated significant improvement compared to the placebo groups, but it does not provide details on statistical testing or variability in each group.

Figure 2: Mean change from the baseline in the number of non-vellus hairs in the target area (TAHC) after 24 weeks of treatment. * = p<0.05 compared to the baseline. QD = once daily, BID = twice daily. Adapted from:[7]Follicle Thought, (2022). Kintor Pharmaceutical KX-826 Phase 2 Results with Poster. Follicle Thought Hair Growth Treatment News. Available at: … Continue reading
According to the researchers, the safety profile was good in all dose groups with:
- 5.9% of participants reported pruritus (itchy skin)
- 2.5% of participants reported contact dermatitis
- 2 patients showing hypertriglyceridemia (high volume of fats in the blood)
Study 3
A randomized, double-blind, placebo-controlled, dose-escalation phase 1 trial was completed in the US over 24 weeks to evaluate the safety, tolerability, and pharmacokinetics of different concentrations of pyrilutamide.[8]Kintor Pharmaceuticals, (2020), Results of Kintor’s Phase 1b Clinical Trials of Pyrilutamide in America. News Center. Available at: https://en.kintor.com.cn/news/129.html (Accessed: 03 May 2023) The participants included 40 healthy male patients, 18-60 years old with androgenic alopecia, who were treated with multiple ascending dose applications of 0.3%, 1.2%, 4.8%, and 9.6% pyrilutamide.[9]Clinical Trials, (2019), Safety, tolerability, and pharmacokinetics of KX826 in healthy male subjects with androgenetic alopecia following topical single ascending dose administration. NIH. Available … Continue reading
The study showed no “severe” adverse drug events, with all adverse events relating to the drug application being mild contact dermatitis that healed in a short time.[10]Kintor Pharma, (no date), Developing Novel Drugs and Commercialization Platform. Available at: https://docs.publicnow.com/viewDoc?hash_primary=BFD6444A4669BD4BE0683A8BCC8B5E80F3D7E430 (Accessed: 03 … Continue reading Unfortunately, the amount of time taken to heal was not given.
Furthermore, the researchers measured the concentration of the drug in the blood to measure the risk of any systemic effects. While we do not have the specific numbers, the researchers do mention that the concentration of pyrilutamide in the blood was low, indicating that the topical concentrations used were not enough to cause a systemic accumulation (i.e., it may not lead to effects around the rest of the body after being topically applied, at these concentrations and frequency).
Study 4
A subsequent phase 2 study was next conducted in the US, with results announced in May 2023. The randomized, double-blind, placebo-controlled, and parallel-group clinical study was conducted in 123 male AGA patients who were classified as stage III vertex, IV, or V using the Hamilton-Norwood scale. 93 patients were randomly assigned to either 0.25% once daily (“QD”), 0.5% QD, and 0.5% twice daily (“BID”) pyrilutamide. 30 patients were randomly assigned to placebo groups for each dose.[11]Kintor Pharma, (2023). Voluntary Announcement. Successful Completion of Phase II Clinical Trial of KX-826 for Treatment of AGA in the United States. Available at: … Continue reading
According to Kintor, the 0.5% BID KX-826 group hair count increased by around 10 hairs per cm2 compared to the baseline after 24 weeks, which was statistically significant. An improvement was seen over the placebo. However, this was not found to be statistically significant. Similar to Study 3, a favorable safety profile was observed, with the only adverse events being mild and local scalp sensitivity.
Study 5
After a number of promising results, the next study showed a missed primary endpoint for a phase 3 study. This was a multicenter, randomized, double-blind, placebo-controlled study to evaluate the twice-daily use of 0.5% KX-826 in men with AGA in China.[12]Kintor Pharma, (2023). Results of KX-826 Phase III Clinical Trial for Treatment of Male AGA in China. Available at: … Continue reading Unfortunately, Kintor did not mention the number of participants in this study.
Pyrilutamide was found to be safe, with no serious adverse events reported. After 24 weeks, the total area hair count was statistically improved compared to the baseline (although no numbers were given), but once again, there was no significant change compared to the placebo.
A few months later, Kintor announced that the NMPA in China had approved a trial for the combination treatment of pyrilutamide and minoxidil in male AGA patients. We will have to wait and see whether combination treatment leads to better results.
UPDATE SEPTEMBER 2024:
Kintor Pivoted to Selling KX826 as a CosmeticDespite not achieving the primary endpoint in their most recently completed trial, Kintor announced in July of 2024 that cosmetic products containing KX-826 were to be launched for sale.[13]Kintor Pharma, (2024). Cosmetics with KX-826 as the core ingredient launched for sale. News Center. Available at: https://en.kintor.com.cn/news_details/3.html (Accessed: 09 September 2024)
Through Koshine, a subsidiary of Kintor, which was established in 2009, they have released the first of these cosmetics – Koshine 826 Anti Hair Loss Solution. It appears to have been listed on Amazon.com by Koshine Biomedica, although there has not yet been confirmation from Kintor or Koshine that this is the official product.[14]Amazon, (no date). KX-826 DHT Blocker Hair Thickening,3 Days Oil Control 1-2 Weeks Hair Loss Reduction 4-6 Weeks New Hair Visible, Hair Regrowth Spray for Men and Women -1 Month Supply 60ml. … Continue reading

Figure 3: KOSHINE 826, the cosmetic version of KX-826 currently being sold.
Koshine 826 is on sale for $69, which buys you a 60ml bottle for a ‘one-month supply’. 1 ml of solution is to be applied each morning and evening, constituting approximately 6-8 sprays from the bottle. The solution should be sprayed onto the exposed scalp within the region of hair loss, followed by a 3-minute scalp massage. Unfortunately, the concentration of KX-826 contained within the product is not stated, so it is not possible to predict how well this product may perform based on clinical studies. However, the product information claims that customers can expect oil control after 3 days of use, reduced hair loss after 1-2 weeks, and visible hair growth after 4-6 weeks.
So, how has Kintor gone from failing the primary endpoint for their most recent study to selling a product containing its KX-826? It all appears to be in the terminology.
To sell a drug in the USA – “articles intended for use in the diagnosis, cure, mitigation, treatment, or prevention of disease” – a company must demonstrate that the product is safe and effective, amongst other factors. This information is generally provided through several rounds of successful clinical trials. However, to sell a cosmetic – “articles intended to be rubbed, poured, sprinkled, or sprayed on, introduced into, or otherwise applied to the human body…for cleansing, beautifying, promoting attractiveness, or altering the appearance” – there is no requirement for FDA approval.[15]U.S. Food & Drug Administration, (2024). Cosmetics & U.S. Law. Available at: https://www.fda.gov/cosmetics/cosmetics-laws-regulations/cosmetics-us-law (Accessed: 09 September 2024)
In other words, cosmetics need not have proven efficacy because they are not used for ‘treating’ anything. Manufacturers don’t even need to prove the safety of a cosmetic before selling it, with action only taken if the FDA receives reliable information that suggests the product may be unsafe.[16]U.S. Food & Drug Administration, (2022). Cosmetic Products. Available at: https://www.fda.gov/cosmetics/cosmetic-products-ingredients/cosmetic-products (Accessed: 09 September 2024)
As Koshine 826 is being marketed as a cosmetic, it can be sold despite clinical trials not (yet) showing sufficient evidence to gain FDA approval. This situation will only change if the product is deemed to be unsafe or the FDA believes that Koshine 826 should also be defined as a drug, which would create the need for FDA approval. Only the FDA can truly define which products are cosmetics and which are drugs, and Kintor must be careful with their wording to ensure that Koshine 826 is not also being marketed as a drug. For now, though, Koshine 826 can be sold without the need for FDA approval.
UPDATE MARCH 2025
Kintor Announces Most Recent Phase 3 Trial Has Met its Primary Endpoint
Kintor Pharma has continued to conduct clinical trials even since launching the product as a cosmetic. The latest? A 16 center open-label trial in China including men and women with AGA.[17]Kintor Pharma. (2025). Long-Term Safety Phase III Clinical Trial Of KX-826 For The Treatment Of AGA Reached Primary Endpoint. Available at: https://en.kintor.com.cn/news_details/9.html (Accessed: … Continue reading
The primary endpoint was safety (incidence of treatment-emergent adverse events). Secondary endpoints included change in target non-vellus hair counts (TAHC), change in target non-vellus hair width (TAHW) and hair growth assessment (HGA) score.
Participants used 0.5% KX-826 twice daily for 52 weeks.
According to the press release, KX-826 showed good safety and tolerability in a clinical trial, with a low incidence of adverse effects, and no drug-related sexual dysfunction adverse events.
TAHC – At 52 weeks, 46% of patients showed ≥10 hairs/cm2 change from the baseline and 20% showed ≥20 hairs/cm2 change from the baseline.
TAHW – Showed a statistically significant increase from the baseline.
HGA – 53% of male participants and 48.4% of female participants showed an HGA score of ≥1.
Press Releases vs. Peer Reviewed Data, Can We Trust Kintor’s Results?
Kintor has conducted multiple studies to explore the efficacy and safety of KX-826, presenting promising results in press releases. However, none of these findings have been published in peer-reviewed journals, which limits the ability to independently verify the data. Peer-reviewed publications are essential for ensuring transparency, as they subject research to rigorous scrutiny by independent experts. Without this process, the information provided by Kintor reflects only what the company has chosen to disclose, raising concerns about potential biases or omitted data.
In contrast, certain natural supplements have published data, albeit often of limited quality. Even when evidence for supplements is weak, peer-reviewed studies provide a more complete picture by detailing methodologies, statistical analyses, and limitations. This transparency allows readers to critically assess claims and understand their clinical significance. For example, if a supplement claims to improve health outcomes, published studies might reveal whether these improvements are substantial or merely marginal.
Non-peer-reviewed data, such as press releases from pharmaceutical companies like Kintor, should be interpreted with caution for several reasons:
-
Lack of Independent Verification: Peer review ensures that findings are evaluated by unbiased experts who can identify flaws or inconsistencies. Without this step, data may be selectively presented to emphasize positive outcomes while downplaying adverse effects or inconclusive results.
-
Conflict of Interest Risks: Companies have a vested interest in promoting their products and may prioritize marketing over scientific integrity. This can lead to exaggerated claims or omission of unfavorable data.
-
Limited Methodological Transparency: Press releases often lack detailed information about study design, statistical analyses, and participant demographics, making it difficult to assess the robustness of the findings.
While natural supplements are not without issues—such as inconsistent ingredient quality or weak regulatory oversight—they often benefit from published studies that allow for critical evaluation. Until Kintor publishes its findings in reputable journals, it remains challenging to fully trust the reported efficacy and safety of KX-826. Independent peer-reviewed research is important for determining whether the claims made in press releases translate into meaningful clinical benefits.
What’s In the Future For KX-826?
Based on the July press release, Koshine 826 may be the first of many products to use KX-826. Kintor stated that they will continue exploring the use of KX-826 for androgenic alopecia and acne.
In their most recent press release, posted in August 2024, Kintor provided further details regarding the upcoming phase II/III clinical trial of KX-826 in the treatment of androgenic alopecia. Dermatology teams from more than 20 domestic hospitals are set to be involved, with over 750 participants expected to be enrolled. Enrollment will commence in early 2025. The trial itself will treat participants with 1% KX-826, which Kintor claims to have performed significantly better in preclinical studies than 0.5% KX-826. This would be the largest KX-826 trial to date, and if the 1% solution does significantly outperform the 0.5% solution, the results could be one to keep an eye on.[18]Kintor Pharma. (2024). Starting Again! Pioneer Pharmaceuticals KX-826 Tincture Registrational Clinical Trial Investigators Meeting Successfully Held. Kintor Pharma. Available at: … Continue reading
What are the Side Effects of Pyrilutamide?
As mentioned above, pyrilutamide treatment does not appear to lead to any serious side effects, with mild contact dermatitis being the only adverse event reported by the researchers. However, because we do not have the full study details or outcomes, we do not know if any other side effects were omitted.
If this is the only side effect, however, pyrilutamide may present an alternative to oral androgen receptor antagonists like flutamide (which you can read about here) that have limited safety profiles in both men and women. Furthermore, because pyrilutamide is a topical treatment instead of an oral treatment this may reduce the risk of systemic effects.
However, as yet, we have no information on whether pyrilutamide can build up in the body and potentially cause systemic effects. Pyrilutamide is an anti-androgen, and therefore it is not unreasonable to hypothesize that, if present at a high enough concentration, pyrilutamide will be associated with side effects like those of other anti-androgens (like erectile dysfunction and loss of sexual interest).
Is Pyrilutamide Right for Me?
You may want to experiment with pyrilutamide if:
- You accept the risk of potential side effects associated with the use of anti-androgen drugs
- You suffer from male or female pattern hair loss
- Are ok buying a product with no published (in peer-reviewed journals) data available for it
- Want to try a topical androgen receptor antagonist
Where Can I Get Pyrilutamide?
Although this product is still in its clinical trial phase, you can buy it online at certain retailers. However, if you do decide to try it, it will set you back around $100 – $110 for a 2 FL OZ bottle.
It is also the core ingredient within Koshine 826, a cosmetic product that has recently begun global sales. A one-month supply, 60ml, costs $69.
Final Thoughts
At a dose of 0.5% once daily in women and twice daily in men, topical pyrilutamide appears to be well-tolerated and may lead to an increase in hair number compared to the baseline. However, few of the studies that used a placebo found any statistically significant differences between the two groups. At this point in time, we would recommend not buying this product until more information from the currently ongoing trials is published.
References[+]
References ↑1 Pubchem, (no date). Pyrilutamide. NIH. Available at: https://pubchem.ncbi.nlm.nih.gov/substance/469676781 (Accessed: 04 May 2023) ↑2 Trueb, R.M., (2021). Understanding pattern hair loss-hair biology impacted by genes, androgens, prostaglandins, and epigenetic factors. Indian Journal of Plastic Surgery, 54(4). 385-392. Available at: https://doi.org/10.1055/s-0041-1739252 ↑3 Kintor, (2021), Kintor Pharmaceuticals Announced Successful Dosing of the First Batch of Patients for Acne Vulgaris Phase I/II Clinical Trial of Pyrilutamide. News Center. Available at: https://en.kintor.com.cn/news/172.html (Accessed: 03 May 2023) ↑4 Cision PR Newswire, (2022), Kintor Pharma Announced the Primary Endpoint of Phase II Clinical Study for KX-826’s Treatment of Female Androgenetic Alopecia in China was Met. Available at: https://www.prnewswire.com/news-releases/kintor-pharma-announced-the-primary-endpoint-of-phase-ii-clinical-study-for-kx-826s-treatment-of-female-androgenetic-alopecia-in-china-was-met-301691321.html (Accessed: 02 May 2023) ↑5 Cision PR Newswire, (2023), Kintor Pharma Announces Completion of Subject Enrollment in Phase III Clinical Trial of KX-826 for Treatment of Male Androgenetic Alopecia in China. Available at: https://www.prnewswire.com/news-releases/kintor-pharma-announces-completion-of-subject-enrollment-in-phase-iii-clinical-trial-of-kx-826-for-treatment-of-male-androgenetic-alopecia-in-china-301783455.html (Accessed: 03 May 2023) ↑6 Kintor Pharmaceutical Limited, (2022). Interim Results Announcement for the six months ended 30 June 2022. Kintor Pharmaceutical. 1-50. Available at: https://www1.hkexnews.hk/listedco/listconews/sehk/2022/0829/2022082902004.pdf (Accessed: 03 May 2023) ↑7 Follicle Thought, (2022). Kintor Pharmaceutical KX-826 Phase 2 Results with Poster. Follicle Thought Hair Growth Treatment News. Available at: https://folliclethought.com/kintor-pharmaceutical-kx-826-phase-2-results-with-poster/ (Accessed: 04 May 2023) ↑8 Kintor Pharmaceuticals, (2020), Results of Kintor’s Phase 1b Clinical Trials of Pyrilutamide in America. News Center. Available at: https://en.kintor.com.cn/news/129.html (Accessed: 03 May 2023) ↑9 Clinical Trials, (2019), Safety, tolerability, and pharmacokinetics of KX826 in healthy male subjects with androgenetic alopecia following topical single ascending dose administration. NIH. Available at: https://clinicaltrials.gov/ct2/show/NCT04984707 (Accessed: 03 May 2023) ↑10 Kintor Pharma, (no date), Developing Novel Drugs and Commercialization Platform. Available at: https://docs.publicnow.com/viewDoc?hash_primary=BFD6444A4669BD4BE0683A8BCC8B5E80F3D7E430 (Accessed: 03 May 2023) ↑11 Kintor Pharma, (2023). Voluntary Announcement. Successful Completion of Phase II Clinical Trial of KX-826 for Treatment of AGA in the United States. Available at: https://staticpacific.blob.core.windows.net/press-releases-attachments/1520008/HKEX-EPS_20230511_10734339_0.PDF (Accessed: 09 May 2024) ↑12 Kintor Pharma, (2023). Results of KX-826 Phase III Clinical Trial for Treatment of Male AGA in China. Available at: https://staticpacific.blob.core.windows.net/press-releases-attachments/1591631/HKEX-EPS_20231127_10979479_0.PDF (Accessed: 09 May 2024) ↑13 Kintor Pharma, (2024). Cosmetics with KX-826 as the core ingredient launched for sale. News Center. Available at: https://en.kintor.com.cn/news_details/3.html (Accessed: 09 September 2024) ↑14 Amazon, (no date). KX-826 DHT Blocker Hair Thickening,3 Days Oil Control 1-2 Weeks Hair Loss Reduction 4-6 Weeks New Hair Visible, Hair Regrowth Spray for Men and Women -1 Month Supply 60ml. Available at: https://www.amazon.com/Blocker-Thickening-Control-Reduction-Regrowth/dp/B0D97LT6MY (Accessed: 09 September 2024) ↑15 U.S. Food & Drug Administration, (2024). Cosmetics & U.S. Law. Available at: https://www.fda.gov/cosmetics/cosmetics-laws-regulations/cosmetics-us-law (Accessed: 09 September 2024) ↑16 U.S. Food & Drug Administration, (2022). Cosmetic Products. Available at: https://www.fda.gov/cosmetics/cosmetic-products-ingredients/cosmetic-products (Accessed: 09 September 2024) ↑17 Kintor Pharma. (2025). Long-Term Safety Phase III Clinical Trial Of KX-826 For The Treatment Of AGA Reached Primary Endpoint. Available at: https://en.kintor.com.cn/news_details/9.html (Accessed: March 2025) ↑18 Kintor Pharma. (2024). Starting Again! Pioneer Pharmaceuticals KX-826 Tincture Registrational Clinical Trial Investigators Meeting Successfully Held. Kintor Pharma. Available at: https://en.kintor.com.cn/news_details/4.html (Accessed: September 2024) In a recent milestone, a drug called ritlecitinib (brand name Litfulo™) has been approved for treating alopecia areata (AA) in adolescents and adults. Ritlecitinib is a type of drug classified as a kinase inhibitor.[1]Pfizer, (2023), FDA Approves Pfizer’s LITFULO™ (Ritlecitinib) for Adults and Adolescents with Severe Alopecia Areata. Pfizer. Available at: … Continue reading In this article, we are going to explore how ritlecitinib works, its safety and efficacy, and its implications for treating hair loss.
Key Takeaways
- Drug. The small molecule ritlecitinib is an inhibitor of Janus-associated kinase 3 (JAK3) recently approved for treating alopecia areata (AA).
- Clinical Data. Clinical trials have demonstrated that ritlecitinib can effectively promote hair regrowth in patients with AA.
- In a phase 2a study conducted on 142 patients (98 women and 44 men), ritlecitinib treatments resulted in improved hair growth in a substantial number of patients – 25% of patients showed 90% or more regrowth by the end of the study and 50% of patients showing 30% or more regrowth by the end of this study.[2]King, B., Guttman-Yassky, E., Peeva, E., Banerjee, A., Sinclair, R., Pavel, A.B., Zhu, L., Cox, L.A., Craiglow, B., Chen, L., Banfield, C., Page, K., Zhang, W., Vincent, M.S. (2021). A phase 2a … Continue reading
- A phase 2b/3 study conducted on 718 patients (446 women and 272 men), further supported the efficacy of ritlecitinib, with patients who received the 30 mg or 50 mg doses responding to a greater extent than controls.[3]King, B., Zhang, X., Harcha, W.G., Szepietowski, J.C., Shapiro, J., Lynde, C., Mesinkovska, N.A., Zwillich, S.H., Napatalung, L., Wasjsbrot, D., Fayyad, R., Freyman, A., Mitra, D., Purohit, V., … Continue reading
- In a sub-study conducted within these clinical trials, ritlecitinib also reduced the expression of several biomarkers associated with alopecia areata, which correlated with the improvement in disease severity as assessed by SALT scores.[4]Guttman-Yasky, E., Pavel, A.B., Diaz, A., Zhang, N., Duca, E.D., Estrada, Y., King, B., Banarjee, A., Banfield, C., Cox, L.A., Dowty, M.E., Page, K., Vincent, M.S., Zhang, W., Zhu, L., Peeva, E. … Continue reading
- Safety. Ritlecitinib is FDA-approved for prescription use, so it should be safe if your doctor recommends it. However, some mild side effects are associated with its use, including upper respiratory tract infections, nasopharyngitis, and headaches. Serious side effects were rare in the clinical trials described above. However, there were instances of breast cancer and shingles during the clinical trials (2 out of 718 patients each).
- Evidence Quality: Ritlecitinib scored 76/100 for evidence quality by our metrics.
- Best Practices. Ritlectinib is specifically indicated for severe alopecia areata and is not suitable for other types of hair loss. According to the patient information leaflet, ritlecitinib should be given at dosages of 50 mg once daily. [5]LITFULO, (2023). Highlights of prescribing information. LITFULO. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/215830s000lbl.pdf (Accessed: 18 September 2023)
What is Ritlecitinib?
Ritlecitinib is a small-molecule inhibitor of the enzyme janus-associated kinase (JAK) that was approved in the US in June 2023. [6]Ramirez-Marin & Tosti (2022), Evaluating the Therapeutic Potential of Ritlecitinib for the Treatment of Alopecia Areata. Drug Design, Development and Therapy. 16. 363-374. Available at: … Continue reading Over a year ago, another JAK inhibitor, baricitinib, was approved last year for severe AA. Now, there’s a second FDA-approved drug for this hair loss disorder, and of a similar class for its mechanisms of action.
The recommended dose of ritlecitinib is 50 mg orally once a day with or without food.[7]{Pfizer, (no date), LITFULO Medical Information. Pfizer. Available at: https://www.pfizermedicalinformation.com/en-us/litfulo/boxed-warning (Accessed: 14 September 2023)

Figure 1: Chemical structure of ritlecitinib.[8]Selleckchem (no date), Ritlecitinib. Selleckchem. Available at: https://www.selleckchem.com/products/pf-06651600.html (Accessed: 15 September 2023)
How Does Ritlecitinib Work?
Ritlecitinib comes under a class of drugs called Janus kinase (JAK) inhibitors. This is because it selectively inhibits a specific enzyme in the JAK family called JAK3. JAK3 is part of a cell signaling pathway called the JAK/STAT pathway, which transmits signals from outside the cell to the nucleus to regulate the expression of genes. This pathway is involved in the control of processes such as the maintenance of stem cells, the formation of new blood cells, and the inflammatory response.[9]Thomas, S.J., Snowden, J.A., Zeidler, M.P., and Danson, S.J. (2015), The role of JAK/STAT signaling in the pathogenesis, prognosis and treatment of solid tumors. British Journal of Cancer. 113. … Continue reading
The JAK/STAT pathway is activated by a range of growth factors and other signaling molecules, including a group of substances called cytokines. Cytokines are proteins that can modulate the immune system in different ways, depending onthe context.[10]Broussard, G., Damania, B. (2020), KSHV: Immune Modulation and Immunotherapy. Frontiers in Immunology. 10. 1-8. Available at: https://doi.org/10.3389/fimmu.2019.03084
In our article on baricitinib, we talk about the JAK/STAT pathway and how cytokine receptors can be described as transmembrane receptors – the receptors cross the cell membrane and have sections that can be found inside and outside the cell. The binding of the cytokine to the receptor on the outside of the cell causes a protein called JAK to bind to the inside portion of the receptor, leading it to undergo a process called trans-phosphorylation, in which a phosphate group is transferred from the receptor to the JAK protein(Figure 2).[11]Harrison, J.A. (2012), The JAK/STAT Pathway. Cold Spring Harbor Perspectives in Biology. 4(3). 1-3. Available at: https://doi.org/10.1101/cshperspect.a011205

Figure 2: Diagram showing the process of activation of STAT by JAK phosphorylation.[12]Luo, W., Li, Y.W., Jiang, L.J., Chen, Q., Wang, T., Ye, D.W. (2020). Targeting JAK-STAT signaling to Control Cytokine Release Syndrome in COVID-19. Trends in Pharmacological Sciences. 8. 531-543. … Continue reading
These JAK proteins, in turn, activate other pathways by phosphorylating proteins like the STATs (signal transducer and activator of protein transcription). When activated by JAK phosphorylation, STAT proteins undergo a change in shape, which allows them to move to the nucleus (called translocation), where they can then activate or deactivate specific genes involved in several cellular processes.[13]Awasthi, N., Liongue, C., Ward, A.C. (2021), STAT proteins: a kaleidoscope of canonical and non-canonical functions in immunity and cancer. Journal of Hematology & Oncology. 14(198). 1-17. … Continue reading
The response to JAK/STAT pathway activation can be different across different types of cells and tissue, depending on the specific type of proteins that make up the pathway and what other signaling pathways are operating in that cell. This provides a contextual element to JAK/STAT signaling.[14]Harrison, D.A., The JAK/STAT Pathway. Cold Spring Harbor Perspectives in Biology. 4(3). A011205. Available at: https://doi.org/10.1101/cshperspect.a011205
How does JAK/STAT signaling relate to AA?
The short answer: activation of the JAK/STAT pathway leads to hair loss caused by immune system activation.
How does AA develop? Let’s recap. Our hair follicles have something called ‘immune privilege’ – they are less subject to the immune response than most of the other areas of the body. This is thought to be in place to protect the stem-cell-containing area of the hair follicle, known as the bulge, which is required for new hair follicle growth in the hair cycle.[15]Azzawi, S., Penzi, L.R., Senna, M.M. (2018), Immune Privilege Collapse and Alopecia Development: Is Stress a Factor. Skin Appendage Disorders. 4(4).236-244. Available at: … Continue reading In AA, something triggers a breakdown of the immune privilege of the hair follicle. The exact cause of this breakdown is not fully understood, but it may involve genetic factors, environmental triggers, or a combination of both.
When the immune privilege is compromised, a group of immune cells called T cells begin to attack the hair follicle. As mentioned earlier, the JAK/STAT pathway plays a critical role in transmitting signals within cells. When the immune system attacks hair follicles, the JAK/STAT pathway is activated, sending signals instructing cells to participate in the attack. As a result, the cells around the hair follicles respond to these signals by causing inflammation and damaging the hair follicle. This disrupts the normal hair growth cycle and leads to hair loss in the affected areas (Figure 3).[16]Kumar, N., Kuang, L., Villa, R., Kumar, P., Mishra, J. (2021), Mucosal Epithelial Jak Kinases in Health and Diseases. Mediators of Inflammation. 1-17. https://doi.org/10.1155/2021/6618924

Figure 3: The collapse of immune privilege in the anagen hair follicle during AA.[17]Lensin, M., Jabbari, A. (2022), An Overview of JAK/STAT Pathways and JAK Inhibition in Alopecia Areata. Frontiers in Immunology. 13. 1-17. Available at: https://doi.org/10.3389/fimmu.2022.955035
Why target JAK3 specifically?
JAK3 is particularly important in the development and function of T cells.[18]Sohn, S.J., Forbush, K.A., Nguyen, N., Witthuhn, B., Nosaka, T., Ihie, J.N., Perimutter, R.M. (1998). Requirement for JAK3 in mature T cells: Its role in regulation of T cell homeostasis. The Journal … Continue reading By targeting JAK3, ritlecitinib may help inhibit T cell activity without affecting other immune cells as strongly. This targeted approach may help to reduce the autoimmune response while preserving some aspects of the immune system’s ability to fight infections.[19]Dai, Z., Sezin, T., Chang, Y., Lee, E.Y., Wang, E.H.C., Christiano, A.M. (2022), Induction of T cell exhaustion by JAK1/3 inhibition in the treatment of alopecia areata. Frontiers in Immunology. 13. … Continue reading
Furthermore, Targeting JAK3 may provide a more precise therapeutic approach for AA. Since JAK3 is primarily involved in immune responses mediated by certain subsets of T cells, it could potentially lead to fewer off-target effects on other immune system functions. Of course, this precision is desirable to avoid compromising the immune system’s ability to protect against infections. Inhibiting JAK1/2 may have broader effects on the immune system, potentially leading to more significant side effects. For example, JAK1/2 inhibitors might interfere with the body’s response to infections or impact other physiological processes.[20]Sardana, K., Bathula, S., Khurana, A. (2023), Which is the Ideal JAK Inhibitor for Alopecia Areata – Baricitinib, Tofacitinib, Ritlecitinib, or Ifidancitinib – Revisiting the … Continue reading By specifically targeting JAK3, the goal is to minimize unwanted side effects while still addressing the autoimmune component of the AA disease mechanism.
Is Ritlecitinib Effective at Treating Alopecia Areata?
Several clinical trials have either already been carried out using ritlecitinib or are ongoing. These trials have been conducted in adults, adolescents, and children, either with AA or cicatricial alopecia (which is similar to AA in terms of disease mechanism, although there are important differences). In total, we could find 2 completed clinical trials with a total number of patients included being 789. We will also cover one of the studies that were conducted at the same time as these trials with the same patients.
The first study was a phase 2a randomized, placebo-controlled study to evaluate the efficacy and safety of ritlecitinib and a similar drug, brepocitinib, in AA.[21]King, B., Guttman-Yassky, E., Peeva, E., Banerjee, A., Sinclair, R., Pavel, A.B., Zhu, L., Cox, L.A., Craiglow, B., Chen, L., Banfield, C., Page, K., Zhang, W., Vincent, M.S. (2021). A phase 2a … Continue reading 142 participants took part (98 female and 44 male) with an average age of 36. Participants were treated with 200 mg of ritlecitinib or 60 mg of baricitinib once daily for four weeks. Then, they were treated with a maintenance dose of 50 mg (ritlecitinib) or 30 mg (baricitinib) for the next 20 weeks. The results were promising for patients with AA who started the study with over 50% of scalp hair loss. Both medications resulted in significant hair regrowth, with 25% (ritlecitinib group) and 34% (baricitinib group) of patients achieving near-complete hair regrowth as measured by Severity of Alopecia Tool (SALT90) scores compared to the placebo group (Figure 4).
The SALT tool is validated for measuring the extent of hair loss in AA with 0% meaning no hair loss, and 100% meaning complete hair loss (with several grades in between).[22]Wyrwich, K.W., Kitchen, H., Knight, S., Aldhouse, N.V.J., Macey, J., Nunes, F.P., Dutronc, Y., Mesinkovska, N., Ko, J.M., King, B.A. (2020). The Alopecia Areata Investigator Global Assessment Scale: … Continue reading The SALT90 score, however, measures the percentage of people who achieved at least 90% of hair regrowth.

Figure 4: Effect of Brepocitinib, Ritlectinib, or a placebo on SALT scores in patients with alopecia areata over 24 weeks. SALT30 = % of patients who showed a SALT score over 30%. SALT90 = % of patients who showed a SALT score over 90%.[23]King, B., Guttman-Yassky, E., Peeva, E., Banerjee, A., Sinclair, R., Pavel, A.B., Zhu, L., Cox, L.A., Craiglow, B., Chen, L., Banfield, C., Page, K., Zhang, W., Vincent, M.S. (2021). A phase 2a … Continue reading
Adverse events were reported in all three treatment groups, with common events including upper respiratory tract infection, nasopharyngitis, headache, acne, and nausea. Serious adverse events were only noted in the brepocitinib group, which could indicate that it may induce more hair regrowth than ritlecitinib but may not be as safe to use.
So, to summarize, although brepocitinib performed better, ritlecitinib also improved hair regrowth scores in patients with AA and appeared to be better tolerated than brepocitinib.
This particular clinical trial also contained a further sub-study to further evaluate the efficacy and safety of ritlecitinib and brepocitinib.[24]Guttman-Yasky, E., Pavel, A.B., Diaz, A., Zhang, N., Duca, E.D., Estrada, Y., King, B., Banarjee, A., Banfield, C., Cox, L.A., Dowty, M.E., Page, K., Vincent, M.S., Zhang, W., Zhu, L., Peeva, E. … Continue reading The study involved taking scalp biopsy samples from patients with AA at baseline and analyzing changes in specific biomarkers between baseline and weeks 12 and 24 of treatment.
Ritlecitinib significantly shifted gene expression in the scalp towards an improved, non-lesional profile. This improvement exceeded 100% of baseline at week 24, indicating a strong positive response to the treatment. Furthermore, the treatment led to a downregulation of inflammatory markers associated with T cells, T cell activation, and other immune response markers. These changes also correlated with an improvement in the SALT score (Figure 5).

Figure 5: Overall percentage improvement in the lesional scalp for each treatment group at weeks 12 and 24. P=<0.001 at weeks 12 and 24 comparisons with placebo and comparisons between treatment groups.[25]Guttman-Yasky, E., Pavel, A.B., Diaz, A., Zhang, N., Duca, E.D., Estrada, Y., King, B., Banarjee, A., Banfield, C., Cox, L.A., Dowty, M.E., Page, K., Vincent, M.S., Zhang, W., Zhu, L., Peeva, E. … Continue reading
However, the most recent study (just prior to ritlecitinib becoming FDA approved) was a 48-week phase 2b/3 randomized, double-blind, placebo-controlled clinical trial.[26]King, B., Zhang, X., Harcha, W.G>, Szepietowski, J.C., Shapiro, J., Lynde, C., Mesinkovska, N.A., Zwillich, S.H., Napatalung, L., Wajsbrot, D., Fayyad, R., Freyman, A., Mitra, D., Purohit, V., … Continue reading The trial was conducted across118 sites in 18 countries, with 718 patients (446 women, 272 men) aged 12 years and older with alopecia areata and at least 50% scalp hair loss – as measured by SALT severity scores.
The patients were assigned to either an oral ritlecitinib or placebo treatment, given once daily for 24 weeks. Several doses of ritlecitinib were tested, along with a variable 4-week loading dose and were followed by a 24-week extension period, during which the ritlecitinib group continued their treatment, and the placebo-treated group switched to ritlecitinib (Figure 6).

Figure 6: The clinical trial study design.[27]King, B., Zhang, X., Harcha, W.G., Szepietowski, J.C., Shapiro, J., Lynde, C., Mesinkovska, N.A., Zwillich, S.H., Napatalung, L., Wasjsbrot, D., Fayyad, R., Freyman, A., Mitra, D., Purohit, V., … Continue reading
The researchers found that patients on the 30 mg or 50 mg doses of ritlecitinib exhibited the highest regrowth scores, and including a loading dose resulted in further improvement. Response rates based on a SALT score of 20% or less at week 24 were significantly higher in ritlecitinib groups compared to the placebo (Figure 7A):
- 29.1% difference for 200 mg + 50 mg
- 20.8% difference for 200 mg + 30 mg
- 21.9% difference for 50 mg
- 12.8% difference for 30 mg
The response rates, based on a SALT score of 10 or less at week 24, were also significantly higher in ritlecitinib groups compared to the placebo (Figure 7B). Furthermore, the proportion of patients with a Patient Global Impression of Change (PGI-C) response of moderately or greatly improved was greater with ritlecitinib treatment compared to placebo at week 24 (Figure 7C). The PGI-C reflects a patient’s belief about the efficacy of a treatment.[28]Ferguson, L., Scheman, J. (2009). Patient global impression of change scores within the chronic pain rehabilitation program. The Journal of Pain. 10(4). S73. Available at: … Continue reading Regrowth of eyelashes and eyebrows was also observed with ritlecitinib treatment (Figures 7D/7E), with responses continuing up to week 48 in all ritlecitinib groups.

Figure 7: Efficacy of ritlecitinib treatment with or without loading doses and compared to placebo groups. (A): Response based on a SALT score of 20 or less. (B) Response based on a SALT score of 10 or less. (C): PGI-C response. (D): Eyebrow response. (E): Eyelash response. (F): Representative photo of a patient at baseline and week 24 with significant growth observed.[29]King, B., Zhang, X., Harcha, W.G., Szepietowski, J.C., Shapiro, J., Lynde, C., Mesinkovska, N.A., Zwillich, S.H., Napatalung, L., Wasjsbrot, D., Fayyad, R., Freyman, A., Mitra, D., Purohit, V., … Continue reading
So, to summarize, ritlecitinib was effective in promoting hair regrowth and was generally well tolerated (more on that below) in patients with alopecia areata. There is a longer-term efficacy study currently ongoing called ALLEGRO-LT, which aims to evaluate the safety and efficacy of ritlecitinib over a period of 60 months (5 years).[30]Clinical Trials (2023) Long-term PF-06651600 for the Treatment of Alopecia Areata (ALLEGRO-LT). NIH. Available at: … Continue reading This trial is due to finish in 2026 and will hopefully provide the long-term efficacy and safety data that is needed.
Is Ritlecitinib Safe?
The overall safety profile was observed throughout the study, and it was determined that ritlecitinib was generally well-tolerated across all doses and showed a favorable safety profile. The most common adverse effects (occurring in at least 10% of patients in any treatment group) included:
- Upper respiratory tract infection – 8.01% of all patients who took ritlecitinib.
- Nasopharyngitis – 13.01% of all patients who took ritlecitinib.
- Headache – 10.96% of all patients who took ritlecitinib
A total of 16 more serious adverse events were reported in 14 patients. These included:
- Infections (Five serious infections were reported. Notably, one patient experienced empyema (fluid between the lungs) and sepsis, while two cases of shingles occurred.
- Malignancies: Two cases of breast cancer were reported, one of which was deemed related to the treatment by an investigator.
- Other serious events were appendicitis, diverticulitis, and pulmonary embolism.
Treatment with ritlecitinib also led to changes in hematological parameters, including:
- Decrease in hemoglobin levels.
- Transient decrease in platelet count.
- Early decrease in absolute lymphocyte levels, particularly in groups with the 200 mg loading dose.
- Early decreases in natural killer cell counts, most apparent in groups with a 200 mg loading dose.
So 14/718 patients experienced a more serious adverse effect – so roughly 2% of patients, or 1 in 50. While you may consider these ‘good odds’, it is important to consider these potential adverse effects when making a treatment decision and always consult a physician.
Is Ritlecitinib for Me?
Ritlecitinib is an exciting new treatment; however, it is important to remember that it is for the treatment of severe alopecia areata only and will not work for other hair loss types like androgenetic alopecia, as the mechanisms of hair loss are very different. You may want to try this treatment if:
- You have severe alopecia areata.
- You have tried other treatments with no success.
- You have spoken to your physician, and they have suggested it based on your alopecia severity.
References[+]
References ↑1 Pfizer, (2023), FDA Approves Pfizer’s LITFULO™ (Ritlecitinib) for Adults and Adolescents with Severe Alopecia Areata. Pfizer. Available at: https://www.pfizer.com/news/press-release/press-release-detail/fda-approves-pfizers-litfulotm-ritlecitinib-adults-and (Accessed: 14 September 2023) ↑2, ↑23 King, B., Guttman-Yassky, E., Peeva, E., Banerjee, A., Sinclair, R., Pavel, A.B., Zhu, L., Cox, L.A., Craiglow, B., Chen, L., Banfield, C., Page, K., Zhang, W., Vincent, M.S. (2021). A phase 2a randomized, placebo-controlled study to evaluate the efficacy and safety of the oral janus kinase inhibitors ritlecitinib and brepocitinib in alopecia areata: 24-week results. Journal of the American Academy of Dermatology. 85(2). 379-387. Available at: https://doi.10.1016/j.jaad.2021.03.050 ↑3 King, B., Zhang, X., Harcha, W.G., Szepietowski, J.C., Shapiro, J., Lynde, C., Mesinkovska, N.A., Zwillich, S.H., Napatalung, L., Wasjsbrot, D., Fayyad, R., Freyman, A., Mitra, D., Purohit, V., Sinclair, R., Wolk, R. (2023). Efficacy and Safety of Ritlecitinib in adults and adolescents with alopecia areata: a randomized, double-blind, multicentre, phase 2b-3 trial. The Lancet. 401. 1518-1529. Available at: https://doi.org/10.1016/S0140-6736(23)00222-2 ↑4, ↑24, ↑25 Guttman-Yasky, E., Pavel, A.B., Diaz, A., Zhang, N., Duca, E.D., Estrada, Y., King, B., Banarjee, A., Banfield, C., Cox, L.A., Dowty, M.E., Page, K., Vincent, M.S., Zhang, W., Zhu, L., Peeva, E. (2022), Ritlecitinib and brepocitinib demonstrate significant improvement in scalp alopecia areata biomarkers. Atopic Dermatitis and Inflammatory Skin Disease. 149(4). P1318-1328. Available at: https://doi.org/10.1016/j.jaci.2021.10.036 ↑5 LITFULO, (2023). Highlights of prescribing information. LITFULO. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/215830s000lbl.pdf (Accessed: 18 September 2023) ↑6 Ramirez-Marin & Tosti (2022), Evaluating the Therapeutic Potential of Ritlecitinib for the Treatment of Alopecia Areata. Drug Design, Development and Therapy. 16. 363-374. Available at: https://doi.org/10.2147/DDDT.S334727 ↑7 {Pfizer, (no date), LITFULO Medical Information. Pfizer. Available at: https://www.pfizermedicalinformation.com/en-us/litfulo/boxed-warning (Accessed: 14 September 2023) ↑8 Selleckchem (no date), Ritlecitinib. Selleckchem. Available at: https://www.selleckchem.com/products/pf-06651600.html (Accessed: 15 September 2023) ↑9 Thomas, S.J., Snowden, J.A., Zeidler, M.P., and Danson, S.J. (2015), The role of JAK/STAT signaling in the pathogenesis, prognosis and treatment of solid tumors. British Journal of Cancer. 113. 365-371. Available at: https://doi.org/10.1038/bjc.2015.233 ↑10 Broussard, G., Damania, B. (2020), KSHV: Immune Modulation and Immunotherapy. Frontiers in Immunology. 10. 1-8. Available at: https://doi.org/10.3389/fimmu.2019.03084 ↑11 Harrison, J.A. (2012), The JAK/STAT Pathway. Cold Spring Harbor Perspectives in Biology. 4(3). 1-3. Available at: https://doi.org/10.1101/cshperspect.a011205 ↑12 Luo, W., Li, Y.W., Jiang, L.J., Chen, Q., Wang, T., Ye, D.W. (2020). Targeting JAK-STAT signaling to Control Cytokine Release Syndrome in COVID-19. Trends in Pharmacological Sciences. 8. 531-543. Available at: https://doi.org/10.1016/kj.tips.2020.06.007 ↑13 Awasthi, N., Liongue, C., Ward, A.C. (2021), STAT proteins: a kaleidoscope of canonical and non-canonical functions in immunity and cancer. Journal of Hematology & Oncology. 14(198). 1-17. https://doi.org/10.1186/s13045-021-01214-y ↑14 Harrison, D.A., The JAK/STAT Pathway. Cold Spring Harbor Perspectives in Biology. 4(3). A011205. Available at: https://doi.org/10.1101/cshperspect.a011205 ↑15 Azzawi, S., Penzi, L.R., Senna, M.M. (2018), Immune Privilege Collapse and Alopecia Development: Is Stress a Factor. Skin Appendage Disorders. 4(4).236-244. Available at: https://doi.org/10.1159/0000485080 ↑16 Kumar, N., Kuang, L., Villa, R., Kumar, P., Mishra, J. (2021), Mucosal Epithelial Jak Kinases in Health and Diseases. Mediators of Inflammation. 1-17. https://doi.org/10.1155/2021/6618924 ↑17 Lensin, M., Jabbari, A. (2022), An Overview of JAK/STAT Pathways and JAK Inhibition in Alopecia Areata. Frontiers in Immunology. 13. 1-17. Available at: https://doi.org/10.3389/fimmu.2022.955035 ↑18 Sohn, S.J., Forbush, K.A., Nguyen, N., Witthuhn, B., Nosaka, T., Ihie, J.N., Perimutter, R.M. (1998). Requirement for JAK3 in mature T cells: Its role in regulation of T cell homeostasis. The Journal of Immunology. 160(5). 2130-2138. Available at: https://doi.org/10.4049/jimmunol.160.5.2130 ↑19 Dai, Z., Sezin, T., Chang, Y., Lee, E.Y., Wang, E.H.C., Christiano, A.M. (2022), Induction of T cell exhaustion by JAK1/3 inhibition in the treatment of alopecia areata. Frontiers in Immunology. 13. 1-14. Available at: https://doi.org/10.3389/fimmu.2022.955038 ↑20 Sardana, K., Bathula, S., Khurana, A. (2023), Which is the Ideal JAK Inhibitor for Alopecia Areata – Baricitinib, Tofacitinib, Ritlecitinib, or Ifidancitinib – Revisiting the Immunomechanisms of the JAK Pathway. Indian Dermatology Online Journal. 14. 465-474. Available at: https://doi.org/10.4103/idoj.idoj_452_22 ↑21 King, B., Guttman-Yassky, E., Peeva, E., Banerjee, A., Sinclair, R., Pavel, A.B., Zhu, L., Cox, L.A., Craiglow, B., Chen, L., Banfield, C., Page, K., Zhang, W., Vincent, M.S. (2021). A phase 2a randomized, placebo-controlled study to evaluate the efficacy and safety of the oral janus kinase inhibitors ritlecitinib and brepocitinib in alopecia areata: 24-week results. Journal of the American Academy of Dermatology. 85(2). 379-387. Available at: https://doi.org/10.1016/j.jaad.2021.03.050 ↑22 Wyrwich, K.W., Kitchen, H., Knight, S., Aldhouse, N.V.J., Macey, J., Nunes, F.P., Dutronc, Y., Mesinkovska, N., Ko, J.M., King, B.A. (2020). The Alopecia Areata Investigator Global Assessment Scale: A Measure for Evaluating Clinically Meaningful Success in Clinical Trials. 183(4). 702-709. Available at: https://doi.org/10.1111/bjd.18883 ↑26 King, B., Zhang, X., Harcha, W.G>, Szepietowski, J.C., Shapiro, J., Lynde, C., Mesinkovska, N.A., Zwillich, S.H., Napatalung, L., Wajsbrot, D., Fayyad, R., Freyman, A., Mitra, D., Purohit, V., Sinclair, R., Wolk, R. (2023). Efficacy and safety of ritlecitinib in adults and adolescents with alopecia areata: a randomized, double-blind, multicentre, phase 2b-3 trial. The Lancet. 401(10387). 1518-1529. Available at: https://doi.org/10.1016/S0140-6736(23)002222-2 ↑27, ↑29 King, B., Zhang, X., Harcha, W.G., Szepietowski, J.C., Shapiro, J., Lynde, C., Mesinkovska, N.A., Zwillich, S.H., Napatalung, L., Wasjsbrot, D., Fayyad, R., Freyman, A., Mitra, D., Purohit, V., Sinclair, R., Wolk, R. (2023). Efficacy and Safety of Ritlecitinib in Adults and Adolescents with Alopecia Areata: a Randomized, Double-Blind, Multicentre, Phase 2b-3 Trial. The Lancet. 401. 1518-1529. Available at: https://doi.org/10.1016/S0140-6736(23)00222-2 ↑28 Ferguson, L., Scheman, J. (2009). Patient global impression of change scores within the chronic pain rehabilitation program. The Journal of Pain. 10(4). S73. Available at: https://doi.org/10.1016/j.pain.2009.01.258 ↑30 Clinical Trials (2023) Long-term PF-06651600 for the Treatment of Alopecia Areata (ALLEGRO-LT). NIH. Available at: https://clinicaltrials.gov/study/NCT04006457?term=ALLEGRO-LT&checkSpell=false&rank=1 (Accessed: 18 September 2023) Ketoconazole is a versatile antifungal drug with widespread applications. It is commonly employed to address dandruff issues. It is also utilized off-label as a remedy for hair loss in both men and women, specifically targeting conditions like androgenic alopecia and telogen effluvium that result from an overgrowth of microorganisms on the scalp.
In this guide, we’ll delve into why you might be shedding after using ketoconazole, the difference between normal and abnormal shedding, solutions, and recommendations for those experiencing hair shedding.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is Ketoconazole?
Ketoconazole is an antifungal medication that is typically used to treat a variety of fungal infections in the body; however, it is also used in the treatment of hair loss conditions like androgenic alopecia (AGA) and telogen effluvium (TE) in the form of topicals and shampoos. Some ketoconazole-based products formulated for hair loss are available over-the-counter (OTC), such as 1% ketoconazole shampoos. In some instances, healthcare professionals may recommend or prescribe stronger ketoconazole treatments.
How Does Ketoconazole Work?
Ketoconazole works as an antifungal agent by disrupting the cell membranes of fungi, inhibiting their growth and replication. The antifungal properties of ketoconazole can help to alleviate these scalp conditions by reducing fungal activity and inflammation. The potential benefit for hair loss conditions such as AGA and TE is that a healthier, less inflamed scalp can create a more favorable environment for hair growth.
Further research suggests that ketoconazole shampoo can reduce dihydrotestosterone (DHT) levels by inhibiting 5 alpha-reductase. Combined usage with finasteride may lead to a more complete treatment.[1]Perez, B.S.H. (2004). Ketoconazole as an adjunct to finasteride in the treatment of androgenetic alopecia in men. Medical Hypotheses. 62(1). 112-115. Available at: … Continue reading
What are the Possible Causes of Hair Shedding After Ketoconazole Use?
Hair shedding after ketoconazole treatment can be disconcerting, but it’s important to understand the potential reasons behind this phenomenon.
Initial Ketoconazole Use
If you have been using ketoconazole for 1-3 months and are experiencing shedding, it may be because the scalp is still adjusting (and responding) to new treatments. Therefore, it’s possible that some of your shedding is due to a positive treatment response.
Ketoconazole Side Effect
According to Nizoral, in rare cases, ketoconazole may cause “inflamed hair follicles, hair loss, or changes in hair texture”.[2]Nizoral, (no date). Nizoral Anti-Dandruff Shampoo Ketoconazole. Nizoral. Available at: https://www.medicines.org.uk/emc/files/pil.6456.pdf (Accessed: 25 October 2023) You can find out if the hair shedding experienced is due to ketoconazole if you are also experiencing scalp dryness, hair dryness, and itchiness. Furthermore, if scalp redness is also experienced, you may be experiencing an allergic reaction to the product.
Seasonal Shedding
Toward the middle and end of the summer, humans undergo a temporary uptick in shedding due to hair cycle seasonality. While this shedding is primarily unavoidable, it also shouldn’t interfere with the success of any long-term hair loss treatments. So, your current bout of shedding might relate more to seasonality than anything else.
Other Hair Loss Products
Sometimes, the shedding might not be from ketoconazole but rather from other recently added treatments. Treatments like minoxidil shorten the non-growing (telogen) phase, which induces the shedding of club telogen hairs, leading to an increase in hair shedding.[3]Shadi, Z. (2023). Compliance to Topical Minoxidil and Reasons for Discontinuation among Patients with Androgenetic Alopecia. Dermatology and Therapy (Heidelb). 13(5). 1157-1169. Available at: … Continue reading
Ketoconazole Overuse
Overusing ketoconazole can lead to irritation, scalp dryness, and hair loss. Therefore, when using a product such as this, you should use it only as often as recommended by the brand or your doctor.
The Difference between Normal Hair Shedding and Abnormal Hair Loss
Normal hair shedding and abnormal hair loss are distinct processes that can affect the health and appearance of your hair. Understanding their differences is crucial for maintaining good hair care and addressing potential issues.
Normal Shedding
We all shed scalp hair; it’s a normal part of the hair follicle cycle, with the average number of hairs shed daily ranging from 50-100 hairs.[4]American Academy of Dermatology, (no date). Do you have hair loss or hair shedding? American Academy of Dermatology. Available at: … Continue reading These hairs typically fall out with no discomfort or noticeable changes in hair density and do not result in visible thinning or bald spots.
Abnormal Shedding
In contrast, abnormal hair loss, alopecia, involves excessive or sudden hair loss beyond normal shedding. It can be caused by various factors, such as genetics, medical conditions, stress, hormonal changes, medication, or an improper diet.[5]Alessandrini, A., Bruni, F., Piraccini, B.M., Starace, M. (2021). Common causes of hair loss – clinical manifestations, trichoscopy, and therapy. JEADV. 35. 629-640. Available at: … Continue reading Abnormal hair loss often leads to noticeable thinning, receding hairlines, or bald patches. Recognizing and addressing the underlying cause of abnormal hair loss is essential for effective treatment and management.
Solutions and Recommendations for Those Experiencing Hair Shedding Due to Ketoconazole
If the ketoconazole shampoo is causing hair shedding with or without scalp irritation, you do not necessarily have to stop usage. The following solutions may help to reduce symptoms:
- Switch from 2% to 1% ketoconazole. This should reduce the “power” of ketoconazole and, thereby, its effect on the hair.
- Reduce ketoconazole’s usage frequency and/or scalp contact time. While ketoconazole shampoo is typically used 2-3 times weekly and left on the scalp for up to 15 minutes, these usage parameters can irritate many people’s scalps. The simplest way to troubleshoot this is to reduce your use. Opt for 1-2 times weekly ketoconazole shampooing and/or only leave in the shampoo for 2-5 minutes.
- Add in a conditioner. After shampooing with ketoconazole, add in a conditioner. This should help moisturize the scalp and hair, reducing any hair texture changes caused by scalp/hair dryness.
If you decide to make any of the above changes, it’s important to give it time to see if the shedding stops or reduces. Assessing the effects of any change in hair care products or routines typically takes several weeks.
If this does not resolve the hair shedding, consider stopping the shampoo and/or seeking help from our community.
References[+]
References ↑1 Perez, B.S.H. (2004). Ketoconazole as an adjunct to finasteride in the treatment of androgenetic alopecia in men. Medical Hypotheses. 62(1). 112-115. Available at: https://doi.org/10.1016/s0306-9877(03)00264-0 ↑2 Nizoral, (no date). Nizoral Anti-Dandruff Shampoo Ketoconazole. Nizoral. Available at: https://www.medicines.org.uk/emc/files/pil.6456.pdf (Accessed: 25 October 2023) ↑3 Shadi, Z. (2023). Compliance to Topical Minoxidil and Reasons for Discontinuation among Patients with Androgenetic Alopecia. Dermatology and Therapy (Heidelb). 13(5). 1157-1169. Available at: https://doi.org/10.1007/s13555-023-00919-x ↑4 American Academy of Dermatology, (no date). Do you have hair loss or hair shedding? American Academy of Dermatology. Available at: https://www.aad.org/public/diseases/hair-loss/insider/shedding#:~:text=It ‘s%20normal%20to%20shed%20between,this%20condition%20is%20telogen%20effluvium. (Accessed: 25 October 2023) ↑5 Alessandrini, A., Bruni, F., Piraccini, B.M., Starace, M. (2021). Common causes of hair loss – clinical manifestations, trichoscopy, and therapy. JEADV. 35. 629-640. Available at: https://doi.org/10.1111/jdv.17079 When selecting hair loss treatments, it’s critical to understand how fast your hair loss is progressing, and why the speed your hair loss should influence your treatment choices – particularly for those with rapidly-progressing androgenic alopecia.
In this article, we’ll uncover:
- The average speed of hair loss progression (per year)
- How to estimate your own speed of hair loss (at home)
- Why people with faster hair loss face bigger stakes for treatment failures
- How to minimize these failures by understanding evidence quality
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
If we have androgenic alopecia, how quickly will we lose hair?
Clinical studies suggest that men with androgenic alopecia will lose 5% hair volume per year. At this rate, it typically takes 15-25 years for a man to go fully bald.[1]Rushton DH, Ramsay ID, Norris MJ, Gilkes JJ. Natural progression of male pattern baldness in young men. Clin Exp Dermatol. 1991 May;16(3):188-92. doi: 10.1111/j.1365-2230.1991.tb00343.x. PMID: … Continue reading[2]Sinclair R. Male pattern androgenetic alopecia. BMJ. 1998 Sep 26;317(7162):865-9. doi: 10.1136/bmj.317.7162.865. PMID: 9748188; PMCID: PMC1113949.
However, it’s important to remember that 5% is just the average rate of hair loss.
In other words, 5% is just the mid-point on a bellcurve. Some people will lose hair at a much slower rate than 5% yearly; others will lose hair much faster.
Why should we care about how fast (or slow) we’re losing hair?
Because men & women with faster hair loss face a bigger opportunity cost for failed treatments. For these individuals, the cost of failure is much, much higher. Consider the following hypothetical:
Person A is losing hair slowly. They try a nutraceutical product, which is supported by low-quality evidence. It doesn’t work. After 12 months, they quit. They now have 1% less hair compared to a year ago. Their hair basically looks the same.
Person B is losing hair rapidly. They try the same nutraceutical product. It doesn’t work. After 12 months, they quit. They now have 25% less hair compared to a year ago. Their hair loss has significantly advanced.
Clinical studies overwhelmingly suggest it’s easier to stop hair loss than it is to regrow significant amounts of lost hair.[3]Sinclair R, Torkamani N, Jones L. Androgenetic alopecia: new insights into the pathogenesis and mechanism of hair loss. F1000Res. 2015 Aug 19;4(F1000 Faculty Rev):585. doi: … Continue reading
Therefore, when choosing treatments, time is of the essence. This is especially true for people with rapid-onset hair loss. So if we want to make fully-informed treatment choices, we should know how quickly our hair loss is advancing.
How can we estimate how fast we’re losing hair?
Ask yourself the following question:
In the last 6 months, have you experienced a visual loss in hair density? In other words, during this time, do you feel your hair loss has gotten cosmetically worse?
If no, you’re probably losing hair more slowly. If yes, you’re probably losing hair faster than 5% yearly.
After all, researchers have calibrated mens’ hair density changes with self-perception data, and they concluded: (3)
“…a deterioration in hair density > 15% was required before subjective awareness became evident.”Long-story short: if you’re weighing your treatment options, do a quick assessment of how fast you’re losing hair.
The slower your hair loss, the more wiggle room you have to experiment. Why? Because the cost of failure might only equate to a 5% loss in hair density.
The faster your hair loss, the more imperative it is to seek treatments with the highest levels of clinical support. Why? Because these treatments tend to maximize your chances of success, and your magnitude of hair regrowth.
We rank some of these treatment options in this video. Moreover, we dive into what constitutes a good study in this article. It’s a deep-dive into how hair loss companies cheat their clinical trials.
Evidence quality example: saw palmetto vs. finasteride
Compare two potential hair loss interventions: saw palmetto and finasteride. One is natural; the other is a drug. Both substances have clinical support for hair growth, particularly for androgenic alopecia. Both substances also work similarly: they help lower the hormone dihydrotestosterone (DHT) in balding regions.
Similar substances. Similar mechanisms. Both clinically supported. But are these truly equal interventions for hair growth? A deeper dive into the evidence on both interventions paints a more nuanced (and dramatically different) picture than what is suggested at face-value.
Saw Palmetto for Hair Loss: 2022 Meta-Analysis
Over nine studies totaling 381 people have shown that saw palmetto might help improve androgenic alopecia.[4]Evron E, Juhasz M, Babadjouni A, Mesinkovska NA. Natural Hair Supplement: Friend or Foe? Saw Palmetto, a Systematic Review in Alopecia. Skin Appendage Disord. 2020 Nov;6(6):329-337. doi: … Continue reading At face value, this sounds great. But looking closer, many of these studies are what we would call lower quality: most of them lacked a placebo group, some were funded by companies selling saw palmetto, and all had small sample sizes.
This means that, for each study, there’s a higher risk of false-positive results: results due to statistical noise that would’ve washed out with a larger sample size.
This phenomenon happens all the time: early studies on an intervention showing promise, followed by larger, more robust studies showing no effect for that same intervention.
In fact, this happened once before for this same supplement – saw palmetto – but for the indication of prostate enlargement.
In the 1990s, several small studies suggested that saw palmetto extract might help reduce symptoms of an enlarged prostate.[5]Descotes, J., Rambeaud, J., Deschaseaux, P. et al. Placebo-Controlled Evaluation of the Efficacy and Tolerability of Permixon® in Benign Prostatic Hyperplasia after Exclusion of Placebo … Continue reading These studies inspired better-controlled clinical trials with hundreds of participants over extended periods, in which saw palmetto showed little-to-no effect.[6]Suzuki M, Ito Y, Fujino T, Abe M, Umegaki K, Onoue S, Noguchi H, Yamada S. Pharmacological effects of saw palmetto extract in the lower urinary tract. Acta Pharmacol Sin. 2009 Mar;30(3):227-81. doi: … Continue reading
Again, study quality, results replication, and sample sizes all inform evidence quality. The lower the evidence quality, the more variance researchers will find between “study results” and “real-world results”. The higher the evidence quality, the less variance between “study” and “real-world” results. In the case of saw palmetto’s effects on prostate enlargement, low-quality data suggested benefit… until higher-quality data came long that brought into question that benefit.
Saw Palmetto Versus Finasteride: Clinical Evidence
When comparing the hair regrowth data on saw palmetto to that of finasteride, the totality of evidence and quality of evidence differ significantly. For instance, finasteride has been studied for 30+ years, in over 30,000 patients, across hundreds of research groups, with dozens of randomized clinical trials – nearly all of which showed significant hair density and hair count increases.
In fact, if you just looked at the treatment arm of one of the randomized, blinded, placebo-controlled studies on oral finasteride, you’d see that the number of participants in a portion of this single study outnumber all participants across all hair growth studies evaluating saw palmetto by a factor of four.[7]Kaufman KD, Olsen EA, Whiting D, Savin R, DeVillez R, Bergfeld W, Price VH, Van Neste D, Roberts JL, Hordinsky M, Shapiro J, Binkowitz B, Gormley GJ. Finasteride in the treatment of men with … Continue reading[8]Evron E, Juhasz M, Babadjouni A, Mesinkovska NA. Natural Hair Supplement: Friend or Foe? Saw Palmetto, a Systematic Review in Alopecia. Skin Appendage Disord. 2020 Nov;6(6):329-337. doi: … Continue reading

When it comes to evidence quality and totality, combining all participants across all saw palmetto studies cannot even add up to a single treatment arm of one placebo-controlled finasteride study.[9]Kaufman KD, Olsen EA, Whiting D, Savin R, DeVillez R, Bergfeld W, Price VH, Van Neste D, Roberts JL, Hordinsky M, Shapiro J, Binkowitz B, Gormley GJ. Finasteride in the treatment of men with … Continue reading[10]Evron E, Juhasz M, Babadjouni A, Mesinkovska NA. Natural Hair Supplement: Friend or Foe? Saw Palmetto, a Systematic Review in Alopecia. Skin Appendage Disord. 2020 Nov;6(6):329-337. doi: … Continue reading
With this visual, we can really see the relative differences in evidence quality across saw palmetto and finasteride. And this is just one of the dozens of finasteride studies available.
Hierarchy of Evidence & Totality of Evidence
These comparisons illustrate two concepts: the hierarchy of evidence – which evaluates how well studies are designed – and the totality of evidence – which evaluates how much research has been done on any one intervention. The higher the hierarchy of evidence and totality of the evidence, the more likely it is that those study results reflect the real-world experience of people trying it.
We capture these concepts inside our Treatment Metrics: a standardized tool we use to help hair loss sufferers evaluate the science supporting (or not supporting) any hair loss intervention at-a-glance.
Again, for a deep-dive into these concepts, see this article.
This is important because people can use the hierarchy and totality of evidence to rank how hair loss interventions might compare to one another. At the top of the list, there are pharmaceutical options. Toward the bottom of the list, there are natural interventions – which absolutely work for some people. But again, the hierarchy and totality of evidence supporting them are more limited, which means that in real life, there will be higher variability in clinical results versus real-world results.

An example hierarchy of evidence for FDA-approved and experimental hair loss interventions.
Here’s how not understanding this can become a problem.
If you’re fighting hair loss, and you’re hit with an advertisement for a product that claims, “clinically proven to regrow hair”, it’s possible this claim is true. But if that claim is also based on a single, small-scale study funded by the company selling you that product, then it’s also true that the evidence supporting that product is not very robust and subject to bias, and that it has a lower likelihood of getting you the hair gains you desire.
In other words, that product probably ranks lower on the hierarchy of evidence and totality of the evidence. So if someone tries it, there are higher odds that the results from that single clinical study won’t reflect their real-world experience.
How Does This All Relate to Hair Loss Speeds?
If you have faster-onsetting hair loss, your opportunity costs for failed treatments are high. In a single year of failed experimentation, you might not lose 5% hair volume; you might lose 20% of your hair or more. There’s a good chance this will be cosmetically significant, which means that people with quickly-progressing hair loss don’t have the same time-freedom as people with slowly-progressing hair loss to play around with interventions that are poorly supported.
So, when considering treatments, one must remember how fast they’re losing hair.
The slower it’s progressing, the better a candidate you are for more experimental, lesser-supported interventions. The faster your hair loss, the more you should consider FDA-approved treatments that rank strongly on the hierarchy and totality of evidence.
Long story short: when fighting hair loss, time is of the essence. The speed of hair loss should always inform candidacy for novel therapies. The slower the hair loss, the better position someone is in to experiment. The faster the hair loss, the more aggressively hair loss should be treated.
References[+]
References ↑1 Rushton DH, Ramsay ID, Norris MJ, Gilkes JJ. Natural progression of male pattern baldness in young men. Clin Exp Dermatol. 1991 May;16(3):188-92. doi: 10.1111/j.1365-2230.1991.tb00343.x. PMID: 1934570. ↑2 Sinclair R. Male pattern androgenetic alopecia. BMJ. 1998 Sep 26;317(7162):865-9. doi: 10.1136/bmj.317.7162.865. PMID: 9748188; PMCID: PMC1113949. ↑3 Sinclair R, Torkamani N, Jones L. Androgenetic alopecia: new insights into the pathogenesis and mechanism of hair loss. F1000Res. 2015 Aug 19;4(F1000 Faculty Rev):585. doi: 10.12688/f1000research.6401.1. PMID: 26339482; PMCID: PMC4544386. ↑4, ↑8, ↑10 Evron E, Juhasz M, Babadjouni A, Mesinkovska NA. Natural Hair Supplement: Friend or Foe? Saw Palmetto, a Systematic Review in Alopecia. Skin Appendage Disord. 2020 Nov;6(6):329-337. doi: 10.1159/000509905. Epub 2020 Aug 23. PMID: 33313047; PMCID: PMC7706486. ↑5 Descotes, J., Rambeaud, J., Deschaseaux, P. et al. Placebo-Controlled Evaluation of the Efficacy and Tolerability of Permixon® in Benign Prostatic Hyperplasia after Exclusion of Placebo Responders. Clinical Drug Investigation 9, 291–297 (1995). https://doi.org/10.2165/00044011-199509050-00007 ↑6 Suzuki M, Ito Y, Fujino T, Abe M, Umegaki K, Onoue S, Noguchi H, Yamada S. Pharmacological effects of saw palmetto extract in the lower urinary tract. Acta Pharmacol Sin. 2009 Mar;30(3):227-81. doi: 10.1038/aps.2009.1. PMID: 19262550; PMCID: PMC4002402. ↑7, ↑9 Kaufman KD, Olsen EA, Whiting D, Savin R, DeVillez R, Bergfeld W, Price VH, Van Neste D, Roberts JL, Hordinsky M, Shapiro J, Binkowitz B, Gormley GJ. Finasteride in the treatment of men with androgenetic alopecia. Finasteride Male Pattern Hair Loss Study Group. J Am Acad Dermatol. 1998 Oct;39(4 Pt 1):578-89. doi: 10.1016/s0190-9622(98)70007-6. PMID: 9777765. Reparex Against Grey Hair is a product that claims to “restore hair color naturally from the inside out, unlike hair dyes”.[1]Reparex, (no date), Reparex Against Grey Hair. Available at: https://reparexshop.com/usa/reparex-against-grey-hair (Accessed: 30 January 2023 Reparex is owned by a company called BOOS Labs – established in 1991 – which makes many different cosmetic products.
Reparex Against Grey Hair doesn’t have any clinical efficacy and safety data associated with it and there are some inconsistencies in the information provided on their website (more on that below). However, let’s take a look at what mechanistic data might be available for this product (if any) and determine if it is a product that is worth your time and money.
Key Takeaways
- Branding. Reparex markets Against Gray Hair products as topically applied alternatives to commercially available hair dyes. Their branding is marketed towards both men and women.
- What makes it unique? Reparex attempts to differentiate itself from other hair colorant products by claiming that its product uses a unique mechanism. They state that “Reparex removes Oxygen from oxidized colorless melanin using the enzyme g-reductase which binds with silver nitrate. This results in the restoration of melanin’s natural color”.[2]Reparex, (no date), How does it work? Available at: https://reparexshop.com/usa/reparex-against-grey-hair (Accessed: 30 January 2023
- Clinical Support. Currently, no clinical data is available to show us the efficacy and safety of this product.
- Concerns.
- The major concern for this product is that there is no mechanistic, efficacy, or safety data (and the explanation they do provide doesn’t make a lot of sense). Basically, this means that we don’t know if this product actually works or whether it’s safe to use for any length of time.
- The websites and documents associated with this product include conflicting and sometimes incorrect information. This makes it confusing to navigate or really understand how the product works.
- The before-and-after photos shown on the website appear to show the same photo for both the before and after shots. Also, in some photos, it is impossible to actually tell if the after photo is of the same person as the before photo (examples below).
- Recommendations to Reparex. In order to improve their service and reassure potential customers, we would recommend that Reparex do the following:
- Take a close look at the information they are providing to customers on their websites and correct inconsistencies and mistakes where possible.
- Conduct long-term, pre-registered, placebo-controlled trials to determine the efficacy and safety of Reparex as a product that can reverse hair graying.
- Be transparent with their before-and-after photos and encourage people to take multiple photos of different angles of the face so that it is possible to identify them as the same person.
- Provide mechanistic data so we can understand exactly how Reparex works (in other words, what is the biological mechanism that their product supposedly affects?).
- Our Current Thoughts. Due to the points mentioned above, we cannot recommend Reparex as a product for reversing gray hair. The onus is on Reparex to provide clear information and clinical data to convince us that this product works.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is Reparex?
Reparex is a brand owned by a company called BOOS Labs that was established in 1991. They create multiple products including the Against Grey Hair product range. Reparex state that Against Grey Hair “Restores your own hair color, bringing back that natural look”.[3]Reparex, (no date), Reparex Against Grey Hair. Available at: https://reparexshop.com/usa/reparex-against-grey-hair/ (Accessed: 29 January 2023

Figure 1: Example of the Reparex Against Grey Hair products. Adapted from:[4]Reparex, (no date), Reparex Against Grey Hair. Available at: https://reparexshop.com/usa/reparex-against-grey-hair/ (Accessed: 29 January 2023
Reparex says that their product “is an outcome of life-long research made by a well-known biochemist and doctor Oto Sova, M.D, PhD. He developed and created a unique enzymatic formula which fits all people and is 100% safe for the human body”.[5]Boos Labs, (no date). How it works. Available at: https://forgreyhair.com/how-it-works (Accessed: 30 January 2023
Oto Sova has, according to the website “studied in several scientific centers in Europe and was a student of several Nobel Prize winners”.[6]For Grey Hair, (no date), For Grey Hair. Available at: https://forgreyhair.au/blog.html (Accessed: 29 January 2023
Who is their target consumer?
Reparex has products aimed at treating gray hair for both men and women. The case studies on their website include 11 men and 6 women.
What products do Reparex offer?
The Reparex range, including prices and volumes, is tabulated below.
Product Size Price Reparex Against Grey Hair for Men 150ml $54.95 Reparex Against Grey Hair for Women 150ml $54.95 Reparex Against Gray Hair for Beard and Mustache 150ml $54.95 Table 1: Prices of Reparex products. Adapted from:[7]Reparex, (no date), Reparex Shop. Available at: https://reparexshop.com/usa/reparex-against-grey-hair/ (Accessed: 27 January 2023
Reparex also offers anti-dandruff lotions, shampoos, and skin ointments aimed at psoriasis sufferers.[8]Reparex, (no date), Reparex Shop. Available at: https://reparexshop.com/usa/reparex-against-grey-hair/ (Accessed: 27 January 2023 These however are not part of the Against Grey Hair Range.
How do they claim these offerings are unique?
Reparex claims that their product is not a hair dye as, according to their definition, “hair dye colors your hair from the outside, but Reparex changes the hair color from the inside. It restores the original hair color, just as your hair was before it became gray”.[9]Reparex, (no date), FAQ. Available at: https://reparexshop.com/usa/faq/ (Accessed: 27 January 2023
Quite what they mean by ‘’…changes hair color from the inside.’’ isn’t clear, and the data to support their claim to this mechanism (not to mention evidence that the product actually changes hair color) is lacking. This makes it difficult to determine whether this product is actually unique.
What is their pricing?
As can be seen above, you’re looking at spending $54.95 a bottle for the specific product you want in the Against Grey Hair series, which should last you around a month.[10]Reparex, (no date), Reparex Shop. Available at: https://reparexshop.com/usa/reparex-against-grey-hair/ (Accessed: 27 January 2023
As there don’t appear to be other products that claim to do what Reparex does, there is not much to compare the price to. But, compared to standard hair dyes, which can be very cheap at around $10, this is perhaps on the pricier side.
Product Science: Deep Dive
Firstly, let’s give a brief overview of how melanin is formed and cover some reasons why hair might turn gray.
Melanin is a type of material in your hair that gives it its color. There are two types of melanin (eumelanin and pheomelanin) and these are both created by special types of cells called melanocytes. Melanocytes are present in both the skin and hair whose primary job is to create melanin. Eumelanin is a darker pigment and is responsible for darker hair color, and pheomelanin is responsible for lighter hair color. An individual person’s hair color will be based upon a specific amount of each type of melanin and their genetics.[11]Slominski, A., Wortsman, J., Plonka, P.M., Schallreuter, K.U., Paus, R., Tobin D. (2005). Hair Follicle Pigmentation. Journal of Investigative Dermatology. 124(1), 13-21. Available at: … Continue reading
In the hair follicle, melanocytes undergo a cycle of growth (proliferation) and rest, in tandem with the hair follicle’s own growth (anagen) and non-growing (telogen) cycles. Specialized stem cells called melanocyte stem cells are located in the bulge of the hair follicle, are activated at the start of the hair follicle growing phase, and supply melanocytes to the core part (the matrix) of the hair follicle. Melanocytes then undergo multiple divisions so that there is a continuous store of melanocytes (and therefore melanin) in the bulb of the hair follicle.[12]Nishimura, E.K. (2011). Melanocyte stem cells: a melanocyte reservoir in hair follicles for hair and skin pigmentation. Pigment Cell & Melanoma Research. 24(3), 401-410. Available at: … Continue reading
Melanin is then packaged into a small ‘packet’ called a vesicle (or a melanosome) which is then transferred into the cells that make the actual substance of the hair follicle (matrix keratinocytes).[13]Schlessinger, D.I., Anoruo, M.D., Schlessinger, J. (2022). Biochemistry, Melanin, In: StatPearls, Treasure Island (FL). StatPearls publishing. Available at: … Continue reading Matrix keratinocytes are cells found in the matrix of the hair follicle, where they are highly proliferative (actively undergo cell division) to form the hair shaft you eventually see as your hair.
The synthesis of melanin involves specific biochemical reactions (called redox reactions) which are made possible by a couple of enzymes called tyrosinase and tyrosinase-related protein (TRP). These enzymes are involved at each step of the production of reactive oxygen species (ROS), such as hydrogen peroxide (H2O2) or O2- as can be seen in Figure 2. Redox reactions are chemical reactions in which a compound can either lose an electron (oxidized) or gain an electron (reduced).[14]Denat, A., Kadekaro, A.L., Marrot, L., Leachman, S, Abdel-Malek, Z.A. (2014). Melanocytes as Instigators and Victims of Oxidative Stress. Journal of Investigative Dermatology. 134(6). 1512-1518 … Continue reading
ROS are chemical compounds that contain oxygen and are therefore highly reactive, so they readily interact with the environment around them. These can cause an environment called oxidative stress which, among other things, can cause damage to melanocytes and other cells in the hair follicle.[15]NIH, (no date), Reactive oxygen species. Available at: https://cancer.gov/publications/dictionaries/cancer-terms/def/reactie-oxygen-species (Accessed: 30 January 2023

Figure 2. The synthesis of eumelanin and pheomelanin. Adapted from:[16]Denat, A., Kadekaro, A.L., Marrot, L., Leachman, S, Abdel-Malek, Z.A. (2014). Melanocytes as Instigators and Victims of Oxidative Stress. Journal of Investigative Dermatology. 134(6). 1512-1518 … Continue reading
However, the hair follicle has a natural defense against ROS -an enzyme called catalase. Catalase breaks down hydrogen peroxide over a series of chemical reactions (also redox reactions), resulting in the production of water and oxygen, and providing protection against oxidative stress.[17]Goyal, M.M., Basak, A. (2010). Human Catalase: Looking for Complete Identity. Protein & Cell. 1(10). 888-897. Available at: https://doi.org/10.1007/is13238-010-0113-z
While there are in-built mechanisms in place for reducing oxidative stress, these can be dysregulated by old age, radiation, inflammation, and psychological/emotional stress. It has been found that there is an increase in oxidative stress and death (apoptosis) of melanin-producing cells (melanocytes) in individuals with gray hairs, as well as a reduction of key protectors against oxidative stress, such as Bcl-2 (and catalase which we will go into further below) and growth factors involved in melanocyte growth such as c-Kit. This reduction in melanocytes subsequently leads to less melanin in hair shafts, giving hair a gray appearance (Figure 3).[18]Arck, P.C., Overall, R., Spatz, K., Liezman, C., Handjiski, B., Klapp, B.F., Birch-Madin, M.A., Peters, E.M.J. (2006). Towards a “free radical theory of graying”: melanocyte apoptosis in the … Continue reading

Figure 3. Hypothesized mechanisms of oxidative stress in the human hair follicle. Adapted from:[19]Arck, P.C., Overall, R., Spatz, K., Liezman, C., Handjiski, B., Klapp, B.F., Birch-Madin, M.A., Peters, E.M.J. (2006). Towards a “free radical theory of graying”: melanocyte apoptosis in the … Continue reading
A further study compared isolated growing hair follicles, dermal papilla cells (DPCs), and other specialized hair follicle cells from gray- and brown-haired donors.[20]Wood, J.M., Decker, H., Hartmann, H., Chavan, B., Rokos, H., Spencer, J.D., Hasse, S., Thornton, S.J., Shalbaf. M., Paus, R., Schallreuter, K.U. (2009). Senile hair graying: H2O2-mediated oxidative … Continue reading The researchers showed that catalase and other enzymes responsible for maintaining a healthy redox balance within the hair follicle are reduced in graying hair, leading to a negative cycle of imbalance and subsequent oxidative stress. In addition to this, hydrogen peroxide was also found to be present in the graying hair follicle whereas it was not present in the brown hair follicle. Furthermore, the researchers found that tyrosinase activity, the enzyme essential for facilitating the synthesis of melanin, was reduced after melanocytes were incubated with increasing doses of hydrogen peroxide (Figure 4).

Figure 4: Tyrosinase activity (as measured by the formation of dopachrome which tyrosinase facilitates) after increasing hydrogen peroxide treatments. Adapted from:[21]Wood, J.M., Decker, H., Hartmann, H., Chavan, B., Rokos, H., Spencer, J.D., Hasse, S., Thornton, S.J., Shalbaf. M., Paus, R., Schallreuter, K.U. (2009). Senile hair graying: H2O2-mediated oxidative … Continue reading
So, it is generally thought that oxidative stress can build up through different stressors in addition to the reactive oxygen species naturally produced through the synthesis of melanin. When oxidative stress builds up, it can reduce the activity of melanocytes and even induce them to die. In these circumstances as there is no longer enough melanin produced to provide keratinocytes with the natural pigment and hairs become gray.
But what does all this have to do with Reparex?
Reparex states that “as we get older hair turns gray due to a natural build-up of hydrogen peroxide in the hair follicles, which causes oxidative stress which oxidizes melanin and consecutively causes graying”. Then they claim that “Reparex removes Oxygen from oxidized colorless melanin using the enzyme g-reductase which binds with silver nitrate. This results in restoration of melanin’s natural color”.[22]Reparex, (no date), How does it work? Available at: https://reparexshop.com/usa/reparex-against-grey-hair (Accessed: 29 January 2023
While the statement above is an attempt to explain the mechanism of action of the Against Grey Hair products, it does not seem to fit with the current theories that state that we lose melanin rather than have colorless melanin within our hair. Additionally, the information on their website is quite confusing and inconsistent, so the only thing we can do is try to break the product down and see how it might work.
The two main ingredients in Reparex’s Against Grey Hair products are silver acetate and glucuronate reductase. Reparex claims that “glucuronate reductase…was able to remove the oxygen from hair melanine [sic] and gives it to silver nitrate”.[23]Boos Labs, (no date), Product Information File. Available at: https://www.forgreyhair.co.uk/wp-content/uploads/sites/12/2022/09/PIF-FGH.pdf (Accessed: 27 January 2023
So, let’s see what these ingredients might do…
Silver acetate…or is it silver nitrate?
Reparex uses the terms silver acetate and silver nitrate interchangeably throughout its website. While they are superficially similar chemical names, they are certainly not the same chemical. In their reasoning for including these chemicals, Reparex state that when they just used the glucuronate reductase by itself it “…took away the oxygen and the hair darkened, but after a while, the hair turned gray again, because the enzymes had no place to transfer the taken oxygen and so they put it back in the hair…therefore it was necessary to engage some ‘oxygen scavenger’ and thus the addition of a minimum amount of silver acetate. As a result, For Grey Hair has become fully functional and usable”.[24]Boos Labs, (no date), The single best treatment for gray hair invented by Oto Sova. Available at: https://forgreyhair.com.au/httpswwwforgreyhaircombest-treatment-for-grey-hair.c128.html (Accessed: 30 … Continue reading
However, with regard to silver acetate, we weren’t able to find any evidence to suggest that it can bind to oxygen or react with oxygen. Furthermore, there does not appear to be any precedence for using silver acetate in hair products.
Silver nitrate, however, can react with oxygen. Furthermore, it has been used as a hair colorant. used daily, it slowly darkens or lightens the hair. So, perhaps there is some rationale for including silver nitrate [25]Guerra-Tapia, A., Gonzalez-Guerra, E. (2014). Hair Cosmetics: Dyes. Actas Dermo-Sifiliográficas (English Edition). 105(9), 833-839. https://doi.org/10.1016j.adengl.2014.02.003
Glucuronate Reductase
Glucuronate reductase is an enzyme that belongs to a family of oxidoreductases. Oxidoreductases are enzymes that facilitate redox reactions.[26]Legesse, H.B., Assefa, B.E. (2021). Biological Application and Disease of Oxidoreductase Enzymes. Oxidoreductase. Available at: https://doi.org/10.5772/intechopen.93328 With regard to Reparex, we can hypothesize that it might work by facilitating a redox reaction in which hydrogen peroxide present in graying hair gets broken down, therefore clearing it from the hair. Perhaps this would reduce oxidative stress and prevent damage to melanocytes. Even if this was the case, would this mechanism still work to replenish already lost melanocytes? Perhaps not.
In any case, as there is no actual mechanistic data, all we can do is speculate and hypothesize, but is there any clinical information about whether this product actually works?
Does Reparex work as a hair treatment?
Unfortunately, there is no clinical data associated with this product that can tell us whether it actually works. There are some case study before-and-after photos presented on the Reparex website; however, some of these appear to actually be just the same photo twice, and it’s impossible to tell if some of the before-and-after photos are the same person, even if there are some notable changes.
Additionally, Reparex offers “2 Free Reparex products of your choice for and before and after photos from our customers”.[27]Reparex, (no date), Reparex Against Grey Hair. Available at: https://reparexshop.com/usa/reparex-against-grey-hair (Accessed: 30 January 2023 The problem with only having before-and-after photos and an incentive to provide them, is that it’s more likely that only people who have positive responses to the treatment will post their results. Furthermore, it’s possible that there are a number of people who saw no improvement, that Reparex may have chosen not to show. This can be avoided with pre-registered clinical trials with disclosed patient numbers, as they will need to show details for all the participants regardless of whether they show a response to the treatment or not.

Figure 5: Before and after photos that appear to be the same photo. Adapted from:[28]Reparex, (no date), Our Satisfied Customers. Available at: https://reparexshop.com/usa/reparex-against-grey-hair/ (Accessed: 29 January 2023

Figure 6: Before and after photos where you cannot tell if the results are for the same person. Adapted from [29]Reparex, (no date), Our Satisfied Customers. Available at: https://reparexshop.com/usa/reparex-against-grey-hair/ (Accessed: 29 January 2023
So, there is no clinical data and no mechanism of action data, meaning that if we did want to use it, we have to trust Reparex and its unconvincing before-and-after photos. But can we actually trust them?
Other than the confusing information on the website about their own product, Reparex also has some somewhat shaky information in their FAQs which leads us to question their overall knowledge about hair. An example is:
“Q: Does REPAREX reduce hair loss?
A: According to latest scientific research, hair loss is caused by a lack of elements such as nickel and iron. We cannot say which one of these is particularly missing for each individual therefore REPAREX cannot help your hair to grow again but we can assure you that it will not cause hair loss to start nor make it worse if you are already suffering from hair loss. Our product has no effect on hair loss.”[30]Reparex, (no date), FAQs. Available at: https://reparexshop.com/usa/faq/ (Accessed: 29 January 2023
While vitamin and mineral deficiency can certainly contribute towards hair loss, in reality, it’s not the only way that hair loss can develop.[31]Almohanna, H.M., Ahmed, A.A., Tsatalis, J.P. (2019). The Role of Vitamins and Minerals in Hair Loss: A Review. Dermatology and Therapy. 9, 51-70. Available at: … Continue reading For example, androgenetic alopecia (AGA) can be caused by an overproduction or oversensitivity to androgens (such as dihydrotestosterone); telogen effluvium can be caused by multiple triggering events, including pregnancy; alopecia areata can be caused as a function of autoimmune dysregulation (to name a few).[32]Alessandrini, A., Bruni, F., Piraccini, B.M., Starace, M. (2020). Common causes of hair loss – clinical manifestations, trichoscopy and therapy. Journal of the European Academy of Dermatology and … Continue reading
Is Reparex Against Grey Hair safe?
Reparex states that “REPAREX has been carefully tested according to the latest EC regulations for cosmetic products; this includes testing for heavy metal content, skin irritation, and any general harm. It has also been evaluated by independent Cosmetic Product Safety Assessors. Furthermore, REPAREX has also been registered at the Central Registration of Cosmetic Products in Brussels and according to its status as harmless it was released to the EU market as harmless and 100% legal.”[33]Reparex, (no date) FAQ. Available at: https://reparexshop.com/usa/faq/ (Accessed: 29 January 2023
However, to our knowledge, there has been no published efficacy or safety data for this product, so we cannot say with certainty that this product is safe to use long-term. It’s also worth noting there are dozens of examples whereby short-term (i.e., 1-2 year) data suggested that a natural substance might be safe, only for long-term (i.e., 5-10+ year) data to show the exact opposite. One example: the effects of vitamin E and selenium supplements on prostate cancer. Short-term data suggested benefit, while long-term data showed these supplements doubled the rates of prostate cancer in men with already-adequate vitamin E and selenium levels.
Should I use Reparex?
You may consider trying out this product if:
- You are unhappy with your gray hair
- You do not want to use other hair dyes
- You are happy using products that have no efficacy or safety data
- You are ok buying a product from a company that has confusing and incorrect information on their website
You may be better placed however to just use a standard hair dye, which you can buy for a fraction of the price.
Recommendations to the company
We would recommend that Reparex look at the information that they are showing on their websites and make sure that it is consistent with (1) the actual ingredients in the product and (2) current scientific data. Furthermore, we recommend that Reparex conduct some mechanistic and long-term pre-registered clinical trials to determine the efficacy and safety of Reparex as a product that can reverse hair graying. Additionally, Reparex should address the issues with their before-and-after photos and make sure that they are not the same photos, and that people can be clearly identified as the same person.
Final thoughts
If you are comfortable trying products with zero published clinical or mechanistic data, and you do not want to use hair dyes, then Reparex might be something you could consider experimenting with. Otherwise, we do not recommend using this product in its current state.
References[+]
References ↑1, ↑27 Reparex, (no date), Reparex Against Grey Hair. Available at: https://reparexshop.com/usa/reparex-against-grey-hair (Accessed: 30 January 2023 ↑2 Reparex, (no date), How does it work? Available at: https://reparexshop.com/usa/reparex-against-grey-hair (Accessed: 30 January 2023 ↑3, ↑4 Reparex, (no date), Reparex Against Grey Hair. Available at: https://reparexshop.com/usa/reparex-against-grey-hair/ (Accessed: 29 January 2023 ↑5 Boos Labs, (no date). How it works. Available at: https://forgreyhair.com/how-it-works (Accessed: 30 January 2023 ↑6 For Grey Hair, (no date), For Grey Hair. Available at: https://forgreyhair.au/blog.html (Accessed: 29 January 2023 ↑7, ↑8, ↑10 Reparex, (no date), Reparex Shop. Available at: https://reparexshop.com/usa/reparex-against-grey-hair/ (Accessed: 27 January 2023 ↑9 Reparex, (no date), FAQ. Available at: https://reparexshop.com/usa/faq/ (Accessed: 27 January 2023 ↑11 Slominski, A., Wortsman, J., Plonka, P.M., Schallreuter, K.U., Paus, R., Tobin D. (2005). Hair Follicle Pigmentation. Journal of Investigative Dermatology. 124(1), 13-21. Available at: https://doi.org/10.1111/j.0022-202X.2004.23528.x ↑12 Nishimura, E.K. (2011). Melanocyte stem cells: a melanocyte reservoir in hair follicles for hair and skin pigmentation. Pigment Cell & Melanoma Research. 24(3), 401-410. Available at: https://doi.org/10.1111/j.1755-148X.2011.00855.x ↑13 Schlessinger, D.I., Anoruo, M.D., Schlessinger, J. (2022). Biochemistry, Melanin, In: StatPearls, Treasure Island (FL). StatPearls publishing. Available at: https://www.ncbi.nlm.nih.gov/books/NBK459156/ (Accessed: 30 January 2023 ↑14, ↑16 Denat, A., Kadekaro, A.L., Marrot, L., Leachman, S, Abdel-Malek, Z.A. (2014). Melanocytes as Instigators and Victims of Oxidative Stress. Journal of Investigative Dermatology. 134(6). 1512-1518 Available at: https://doi.org/10.1038/jid.2014.65 ↑15 NIH, (no date), Reactive oxygen species. Available at: https://cancer.gov/publications/dictionaries/cancer-terms/def/reactie-oxygen-species (Accessed: 30 January 2023 ↑17 Goyal, M.M., Basak, A. (2010). Human Catalase: Looking for Complete Identity. Protein & Cell. 1(10). 888-897. Available at: https://doi.org/10.1007/is13238-010-0113-z ↑18 Arck, P.C., Overall, R., Spatz, K., Liezman, C., Handjiski, B., Klapp, B.F., Birch-Madin, M.A., Peters, E.M.J. (2006). Towards a “free radical theory of graying”: melanocyte apoptosis in the aging human hair follicle is an indicator of oxidative stress induced tissue damage. The FASEB Journal. 20(9), 1567-1569. Available at: https://doi.org/10.1096/fj.05-04039fje ↑19 Arck, P.C., Overall, R., Spatz, K., Liezman, C., Handjiski, B., Klapp, B.F., Birch-Madin, M.A., Peters, E.M.J. (2006). Towards a “free radical theory of graying”: melanocyte apoptosis in the aging human hair follicle is an indicator of oxidative stress induced tissue damage. The FASEB Journal. 20(9), 1567-1569. Available at: https://doi.org/10.1096/fj.05-04039fje ↑20 Wood, J.M., Decker, H., Hartmann, H., Chavan, B., Rokos, H., Spencer, J.D., Hasse, S., Thornton, S.J., Shalbaf. M., Paus, R., Schallreuter, K.U. (2009). Senile hair graying: H2O2-mediated oxidative stress affects human hair color by blunting methionine and sulfoxide repair. The FASEB Journal. 23(7), 2015-2336. Available at: https://doi.org/10.1096/fj.08-125435 ↑21 Wood, J.M., Decker, H., Hartmann, H., Chavan, B., Rokos, H., Spencer, J.D., Hasse, S., Thornton, S.J., Shalbaf. M., Paus, R., Schallreuter, K.U. (2009). Senile hair graying: H2O2-mediated oxidative stress affects human hair color by blunting methionine and sulfoxide repair. The FASEB Journal. 23(7), 2015-2336. Available at: https://doi.org/10.1096/fj.08-125435 ↑22 Reparex, (no date), How does it work? Available at: https://reparexshop.com/usa/reparex-against-grey-hair (Accessed: 29 January 2023 ↑23 Boos Labs, (no date), Product Information File. Available at: https://www.forgreyhair.co.uk/wp-content/uploads/sites/12/2022/09/PIF-FGH.pdf (Accessed: 27 January 2023 ↑24 Boos Labs, (no date), The single best treatment for gray hair invented by Oto Sova. Available at: https://forgreyhair.com.au/httpswwwforgreyhaircombest-treatment-for-grey-hair.c128.html (Accessed: 30 January 2023 ↑25 Guerra-Tapia, A., Gonzalez-Guerra, E. (2014). Hair Cosmetics: Dyes. Actas Dermo-Sifiliográficas (English Edition). 105(9), 833-839. https://doi.org/10.1016j.adengl.2014.02.003 ↑26 Legesse, H.B., Assefa, B.E. (2021). Biological Application and Disease of Oxidoreductase Enzymes. Oxidoreductase. Available at: https://doi.org/10.5772/intechopen.93328 ↑28, ↑29 Reparex, (no date), Our Satisfied Customers. Available at: https://reparexshop.com/usa/reparex-against-grey-hair/ (Accessed: 29 January 2023 ↑30 Reparex, (no date), FAQs. Available at: https://reparexshop.com/usa/faq/ (Accessed: 29 January 2023 ↑31 Almohanna, H.M., Ahmed, A.A., Tsatalis, J.P. (2019). The Role of Vitamins and Minerals in Hair Loss: A Review. Dermatology and Therapy. 9, 51-70. Available at: https://doi.org/10.1007/s13555-018-0278-6 ↑32 Alessandrini, A., Bruni, F., Piraccini, B.M., Starace, M. (2020). Common causes of hair loss – clinical manifestations, trichoscopy and therapy. Journal of the European Academy of Dermatology and Venereology. 35, 629-640. Available at: https://doi.org/10.1111/jdv.17079 ↑33 Reparex, (no date) FAQ. Available at: https://reparexshop.com/usa/faq/ (Accessed: 29 January 2023 What is Ketoconazole?
Ketoconazole is an antifungal medication frequently used to treat various fungal infections around the body, including the scalp. It has also proven effective in managing hair loss problems, such as androgenic alopecia (AGA) and telogen effluvium (TE), typically through topical forms like shampoos.
One of the advantages of using ketoconazole for hair loss is that it has a low risk of causing side effects in most people. Some products with ketoconazole, like 1% ketoconazole shampoos, are also available over the counter without a prescription. Healthcare professionals may recommend or prescribe stronger ketoconazole treatments for specific cases in certain situations – with 2% ketoconazole shampoos showing clinical effectiveness in treating androgenic alopecia.
With that said, a portion of people do experience side effects from ketoconazole. With no roadmap to resolve these side effects, these users will often discontinue the medication – thereby forfeiting the hair gains they could’ve experienced had they found a way to resolve those adverse events.
In this article, we’ll explore what these side effects are, and how most of these side effects can be mitigated, minimized, and even resolved with proper troubleshooting.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What are the Common Side Effects of Ketoconazole Shampoo?
While oral ketoconazole has notable risks associated with side effects, the use of 1-2% ketoconazole shampoo appears to have minimal, if any, side effects due to its limited exposure time and low absorption into the bloodstream compared to the oral form. Nevertheless, there are instances where individuals using ketoconazole shampoo may encounter adverse effects. These occurrences could include:[1]Drugs.com (2023). Nizoral Shampoo Side Effects. Available at: https://www.drugs.com/sfx/nizoral-shampoo-side-effects.html (Accessed: 26 October 2023)
- Skin irritation
- Itching
- Stinging or burning
- Blistering
- Dry skin
- Increased hair shedding
In very rare cases, some people also report hair discoloration.[2]Kuibicki, S.L., Damanpour, S., Mann, R. (2020). Ketoconazole shampoo-induced hair discoloration. International Journal of Women’s Dermatology. 6(2). 121-122. Available at: … Continue reading
What Should I Do to Combat These Side Effects?
If you’ve begun to experience side effects from using ketoconazole shampoo, it’s crucial to take proactive steps to mitigate these effects so you can still benefit from the treatment. Understanding how to manage these side effects can make a significant difference in your comfort and the effectiveness of the shampoo. It’s important to remember that while most side effects are mild and manageable, they are still noteworthy and require appropriate action to ensure they don’t escalate or adversely affect your hair and scalp health.
Scalp Dryness, Hair Dryness, Dandruff, and/or Itchiness
If you experience abnormal hair texture, scalp or hair dryness, dandruff, and/or itchiness, you should consider the following:
- Switch from 2% to 1% ketoconazole. This should reduce the “power” of ketoconazole and, thereby, its drying effect on the hair.
- Reduce ketoconazole’s usage frequency and/or scalp contact time. While ketoconazole shampoo is typically used 2-4 times weekly and left on the scalp for 5-15 minutes, these usage parameters can irritate many peoples’ scalps. The simplest way to troubleshoot this is to reduce your use. Opt for 1-2 times weekly ketoconazole shampooing and/or only leave in the shampoo for 2-5 minutes.
- Add in a conditioner. After shampooing with ketoconazole, add in a conditioner. This should help moisturize the scalp and hair, reducing hair texture changes caused by scalp/hair dryness.
Hair Shedding
Understanding the reasons behind hair shedding is important when using ketoconazole shampoo, as it helps in distinguishing between normal hair loss and the potential side effects of the treatments. Various factors can influence hair shedding, and it’s important to identify whether this shedding is (1) a positive shed in response to starting ketoconazole, (2) a reaction to the ketoconazole itself, and/or (3) if this hair shedding is actually coincidental to your introduction of ketoconazole, and is instead caused by other factors: seasonal hair cycling, the introduction or withdrawal of other hair loss treatments, and/or telogen effluvium sheds.
Medical and legal consensus – with any treatment-related side effect – is to stop that treatment and consult with your doctor immediately. Nonetheless, we’ll go through a few of these situations below, along with potential troubleshooting advice for resolution:
Scalp Issues
If your hair shedding is accompanied by scalp dryness, hair dryness, and/or itchiness, then this might be a reaction from the ketoconazole shampoo, and you can follow the above-mentioned measures to mitigate the side effects.
If your hair shedding is accompanied by scalp redness, then there is a slight possibility that you are having a very rare allergic reaction to the shampoo. In cases like this, we recommend stopping the ketoconazole and seeing a doctor or dermatologist who can further assess your tolerability. While allergic reactions to ketoconazole are rare, it is usually best to err on the side of caution – especially as ketoconazole tends to be a lower-leverage treatment option (meaning that it often does not produce vast amounts of hair regrowth).
Scalp Adjustment to Treatment
If any other side effects do not accompany your hair shedding and you have just started ketoconazole in the last 3 months, then it may just be that your scalp is still adjusting (and responding) to new treatments. Therefore, it might be that some of your shedding is due to a positive treatment response. We’ll have more articles about this soon.
Seasonal Shedding
Sometimes, increases to hair shedding have nothing to do with your hair loss treatments and, instead, are simply a function of seasonal hair shedding.
Humans undergo a temporary uptick in shedding due to hair cycle seasonality. In the northern hemisphere, these upticks typically occur in July and August, then settle into lower shedding rates in winter. While this shedding is mostly unavoidable, there’s also good news: it doesn’t really interfere with the success of your long-term hair loss treatments. So, if you’re within peak windows of time for seasonal hair shedding, you may want to consider that at least some of this shedding might not be due to ketoconazole, but instead, due to seasonality.
Recent Introduction/Withdrawal of Other Treatments
It may also be that the hair shedding might not be related to ketoconazole use. If you have withdrawn from or introduced other hair loss treatments within the last three months, these changes may also explain recent upticks to hair shedding.
Skin Burning, Peeling, or Redness
As mentioned above, scalp redness has a slight possibility of being a rare allergic reaction to the shampoo. We recommend stopping using the shampoo and seeing your doctor or dermatologist for advice.
Hair Discoloration
Hair discoloration is a rarer side effect of ketoconazole shampoo, but a few long-term treatment users have reported it. Under these circumstances, we recommend you stop using ketoconazole shampoo and instead switch to other shampoos with anti-dandruff and antifungal properties, but that work through different mechanisms and thus may not evoke the same effect. Consider shampoos with the following active ingredients: selenium sulfide and/or zinc pyrithione.
Shampoos with these ingredients are widely sold over the counter and are specifically formulated to reduce dandruff and skin flaking. There’s also some evidence that they may support hair growth in those with androgenic alopecia, female pattern hair loss, and/or telogen effluvium associated with microorganism overgrowths.[3]Trueb, R.M., Henry, J.P., Davis, M.G., Schwartz, J.R. (2018). Scalp Condition Impacts Hair Growth and Retention via Oxidative Stress. International Journal of Trichology. 10(6), 262-270. Available … Continue reading,[4]McGinley, K.J., Leyden, J.J. (1982). Antifungal activity of dermatological shampoos. Archives of Dermatological Research. 272(3-4). 339-342. Available at: https://doi.org/10.1007/BF00509065
Other Side Effects
If you experience any other side effects and want advice from the community, feel free to make a forum post describing your growth regimen, ketoconazole shampoo routine, and specific side effects. Our team and community will chime in with resources and strategies to help you resolve this. You can post your questions here.
References[+]
References ↑1 Drugs.com (2023). Nizoral Shampoo Side Effects. Available at: https://www.drugs.com/sfx/nizoral-shampoo-side-effects.html (Accessed: 26 October 2023) ↑2 Kuibicki, S.L., Damanpour, S., Mann, R. (2020). Ketoconazole shampoo-induced hair discoloration. International Journal of Women’s Dermatology. 6(2). 121-122. Available at: https://doi.org/10.1016/j.ijwd.2019.10.010 ↑3 Trueb, R.M., Henry, J.P., Davis, M.G., Schwartz, J.R. (2018). Scalp Condition Impacts Hair Growth and Retention via Oxidative Stress. International Journal of Trichology. 10(6), 262-270. Available at: https://doi.org/10.4103/ijt.ijt_57_18 ↑4 McGinley, K.J., Leyden, J.J. (1982). Antifungal activity of dermatological shampoos. Archives of Dermatological Research. 272(3-4). 339-342. Available at: https://doi.org/10.1007/BF00509065 Is hair loss treatment lifelong? It can be daunting to think that’s the case, as it seems quite a commitment. But while it’s true for most cases of androgenic alopecia, lifelong hair loss treatment may not be as scary as it seems. In this article, we will delve into the effects of stopping hair loss treatments and how a shift in perspective can improve how we feel about “lifelong” hair loss treatments.
Is Hair Loss Treatment Lifelong?
The short answer is yes: hair loss treatments must be continued, or results gained will be lost. This is at least true for most cases of androgenic alopecia (more on this below). The longer answer is that:
- This isn’t true for all hair loss cases. There are plenty of situations where hair loss treatments are only temporary, as the hair regrowth sustains even after quitting. It depends on the type(s) of hair loss.
- “Lifelong” treatments aren’t as scary as they seem. The fact that some treatments might require a lifelong commitment should never be a reason not to try that same treatment, at least today.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
Let’s first look at what we know about what happens when you quit a hair loss treatment.
What Happens if I Quit a Hair Loss Treatment?
Luckily, some studies explain what happens when you quit traditional hair loss treatments like minoxidil and finasteride. There is even a study looking at what happens if you stop microneedling.
What Happens if I Quit Minoxidil?
In 1999, a study explored the implications of discontinuing minoxidil after long-term use. The study yielded intriguing results, as the group that ceased minoxidil treatment observed a period of increased hair shedding and a temporary drop in hair counts, falling below their pre-treatment levels.
Four groups of 9 men with AGA were followed over two years, with each group receiving either 2% minoxidil, 5% minoxidil, a placebo, or no treatment. The 2% and 5% minoxidil groups displayed a notable increase in hair counts after three months, which reached a plateau but remained higher than those observed in the placebo and control groups.
Approximately two years into the study, at the 96-week mark, the individuals in the 2% and 5% minoxidil groups stopped their treatments. This discontinuation is evident in the data related to hair weights, which began to decline shortly afterward (see Figure 1). Three months later, around week 108, their hair loss had fallen well below the levels seen in the placebo group, even dipping below their initial hair counts. However, by week 120, three months later, the 2% and 5% minoxidil groups had rebounded and returned to a level comparable to their baseline hair counts before the study began.

Figure 1: Changes in hair weight and hair count in men with androgenetic alopecia after application of 5% and 2% topical minoxidil, placebo, or no treatment. The line at 96 weeks shows the time when minoxidil treatment was stopped.[1]Price, V.H., Menefee, E., Strauss, P.C., (1999). Changes in hair weight and hair count in men with androgenetic alopecia after application of 5% and 2% topical minoxidil, placebo, or no treatment. … Continue reading
It should be noted that any excess hair shedding experienced during this transition phase is usually not a permanent condition. With time, the hair adjusts to a new equilibrium without the presence of the drug, and excessive shedding should subside, returning to pre-treatment levels.
What Happens if I Quit Finasteride?
The informational insert for Propecia, a finasteride brand, indicates that hair loss typically resumes within 3 to 12 months after stopping the medication, and hair counts may revert to pre-treatment levels. This conclusion is grounded in the results from Phase II and III clinical trials, which were crucial for the FDA’s approval of finasteride for treating androgenic alopecia.
In these trials, a subset of participants received finasteride for an entire year. Subsequently, they were unknowingly switched to a group that received a placebo (a sugar pill) during the second year, corresponding to months 12-24 of the study. The researchers closely monitored and documented changes in hair counts for these participants from the start (month 0) throughout 24 months. They then compared these changes with those who continued using finasteride throughout the study and those who consistently received the placebo.[2]Kaufman, K.D., Olsen, E.A., Whiting, D., Savin, R., DeVillez, R., Bergfeld, W., Price, V.H., van Neste, D., Roberts, J.L., Hordinsky, M., Shapiro, J., Binkowitz, B., Gormley, G.J. (1998). Finasteride … Continue reading
What the Findings Say
The study revealed that ceasing finasteride and switching to placebo resulted in hair counts falling back to their initial levels, or even slightly below, within 12 months after stopping the medication (Figure 2).

Figure 2: Hair count mean change from baseline. Fin – Pbo = the group who initially took finasteride and then were unknowingly switched to placebo.[3]Kaufman, K.D., Olsen, E.A., Whiting, D., Savin, R., DeVillez, R., Bergfeld, W., Price, V.H., van Neste, D., Roberts, J.L., Hordinsky, M., Shapiro, J., Binkowitz, B., Gormley, G.J. (1998). Finasteride … Continue reading
However, there are also interesting studies that can provide information about taking a break from finasteride.
Biological Effects of Finasteride After Quitting
Because finasteride has a terminal half-life of 5-7 hours, and it takes about 4-5 days for the drug to fully dissociate from tissues, its biological effects on hormone profiles can persist for approximately 30 days after discontinuation.
In practical terms, this means finasteride can continue to have a therapeutic impact in reducing scalp levels of dihydrotestosterone (DHT) even several weeks after discontinuing the medication (see Figure 3).

Figure 3: Serum DHT concentration before and after quitting finasteride treatment.[4]Clark, R.V., Hermann, D.J., Cunningham, G.R., Wilson, T.H., Morrill, B.B., Hobbs, S. (2004). Marked Suppression of Dihydrotestosterone in Men with Benign Prostatic Hyperplasia by Dutasteride, a Dual … Continue reading
Exploring Alternative Finasteride Dosing Schedules
A study investigated whether a daily dose of 1 mg was necessary to maintain hair regrowth. Initially, a group of men was placed on a daily 1 mg finasteride regimen for a year. In the second year, the men were divided into two groups: one continued to take finasteride daily, while the other group adopted a 30-days-on, 30-days-off dosing schedule.[5]Kim, K.H., Park, S.M., Lee, Y.J., Sim, W.Y., Lew, B.L. (2020). Similar efficacy of maintenance treatment of finasteride 1 mg every other month compared with finasteride 1 mg daily in Korean men with … Continue reading
The second group used finasteride for only half the time (i.e., 6 months as opposed to 12 months), yet both groups experienced similar improvements in hair parameters during the second year.
The underlying hypothesis for this result was that finasteride’s pharmacokinetics might allow for dosing schedules that alternate monthly. This approach could potentially accommodate those who wish to reduce their drug exposure or take breaks from the medication without significantly compromising their hair gains.
What If I Need To Stop Taking Finasteride For Any Other Reason?
When pausing finasteride use for an extended period exceeding 30 days, there is a higher risk of hair loss resuming due to the dissipation of the drug’s effects on scalp DHT levels. Both clinical withdrawal studies and anecdotal reports from finasteride users support this phenomenon.
Hair loss may not immediately return for many individuals but might become noticeable around the second or third month after quitting. To maintain the benefits of the drug on hair health, it is advisable to keep the withdrawal period beyond 30 days as short as possible.
If you want to learn more about the pharmacokinetics of finasteride and how you can maximize your treatment usage, you can follow these links:
- Finasteride: How Long Does It Stay In The Bloodstream?
- Finasteride: How Long Does It Stay Active in Scalp Tissue?
- What Happens If I Stop Using Finasteride?
What Happens if I Quit Microneedling?
Currently, there is only one clinical study evaluating the effects of microneedling cessation. This study compared the effects of using minoxidil only, microneedling only, and using both minoxidil and microneedling together.[6]Bao, L., Zong, H., Fang, S., Zheng, L.i, Y. (2022). Randomized trial of electrodynamic microneedling combined with 5% minoxidil topical solution for treating androgenetic alopecia in Chinese males … Continue reading
The study involved 71 male participants with androgenetic alopecia (AGA), divided into three distinct treatment groups:
- 5% minoxidil applied twice daily for 24 weeks (23 participants).
- Microneedling sessions were conducted every 3 weeks, totaling 8 treatments (23 participants).
- A combination of both treatments over 24 weeks (25 participants).
The researchers assessed changes in hair density and diameter at three-week intervals and conducted a six-month follow-up after the final treatment.
What the Findings Say
All groups exhibited significant increases in non-vellus hair density three weeks post-treatment. Notably, the combination group showed the most substantial increase in non-vellus hair density (56.45±7.82 roots per cm²), outperforming the ~28 increase in the minoxidil group and ~32 in the microneedling group.
These findings align with earlier research, particularly a paper by Dhurat et al., highlighting microneedling’s role in enhancing minoxidil’s effectiveness.
Six-Month Follow-Up Insights
Six months after the completion of the treatments, the study revealed intriguing long-term effects:
- In the minoxidil-only group, 90% of participants lost all newly acquired hair within six months post-treatment cessation, a finding consistent with previous minoxidil research.
- Conversely, in both the microneedling-only and the combination groups, 70% of participants retained some new hair, and 20% maintained all new hair growth (referenced in Figure 4).
Figure 4 illustrates the comparative hair regrowth across the three groups during the initial 24 weeks of treatment and the subsequent 24 weeks post-treatment.

Figure 4: The effect of a) minoxidil-only, b) microneedling-only, and c) minoxidil and microneedling on hair regrowth during the initial 24 weeks of treatment, and a further 24 weeks after treatment.[7]Bao, L., Zong, H., Fang, S., Zheng, L.i, Y. (2022). Randomized trial of electrodynamic microneedling combined with 5% minoxidil topical solution for treating androgenetic alopecia in Chinese males … Continue reading
These results suggest that microneedling, alone and in combination with minoxidil, offers more durable effects on hair maintenance, even after treatment discontinuation. The sustained impact in the combination group also indicates that microneedling may enhance minoxidil’s long-term effectiveness.
In summary, while managing hair loss often requires lifelong treatment, there are instances where benefits can continue even after the cessation of certain therapies. Studies have shown that minoxidil and finasteride necessitate ongoing use to maintain hair growth, as discontinuation can reverse benefits. However, treatments such as microneedling, alone or in combination with minoxidil, have demonstrated more enduring effects, offering sustained hair maintenance even after stopping the treatment.
How Can We Change Our Mindset About “Lifelong” Hair Loss Treatments?
Changing our mindset about lifelong hair loss treatment involves embracing it as a part of routine self-care, much like daily exercise or a balanced diet. It’s about viewing these treatments not as burdensome but as an empowering step toward self-confidence and well-being. Recognizing that consistency is key to success, we can integrate these treatments into our daily routines.
Let’s take a look at some ways that we can improve our mindset about long-term treatment.
1. Let hair care become part of a daily self-care routine.
Taking care of our hair is important to our overall health and well-being. We all have a daily skincare routine to maintain our skin’s health and appearance, and we can apply the same principles to our hair care routine.
Hair loss treatments should be viewed as a constructive practice that can help preserve and enhance our natural features. Whether we choose to use topical solutions, medications, or nutritional supplements, these treatments can help us maintain the health and vitality of our hair.
By adopting this mindset, we can reframe hair loss treatment as a positive and nurturing practice that empowers us to take control of our hair’s health, just like how we care for our skin, caring for our hair can be a normal and rewarding part of our daily wellness routine.
Another perspective:
2. Starting treatment today does not mean committing to that treatment forever.
Research shows that when someone quits treatment, their hair loss will resume. Within several months, their hair will return to its state before treatment. As you can see above, minoxidil users typically experience a loss of gains within 3-6 months, with an initial excess shedding period and then a return to baseline. For finasteride users, that timeframe is often 6-12 months (or longer), and quitting microneedling can take over 6 months to lose hair gains.
Importantly, those same studies show people are never worse off after starting and then quitting hair loss treatments.
This is critical because it means there is little risk when trying a hair loss treatment and later withdrawing it. By doing so, hair loss is not accelerated; it simply returns to baseline after quitting. In effect, the time spent on the treatment has slowed the progress of future hair loss.
It’s significantly easier to arrest the progression of hair loss than to regrow hair. That means that when fighting hair loss, time is of the essence. We speak about this in our treatment mistakes video series, which is available for members, particularly in the videos about balding speeds.
As such, trying a treatment today does not require a lifelong commitment to that treatment. Just by giving that treatment a shot, the rate of hair loss potentially slows down. If a decision is made later to quit or taper away from that treatment, the data strongly suggest that your efforts should never make things worse in the long-run.
Do Any Hair Loss Treatments Work Permanently, Even After Quitting Them?
For some cases of telogen effluvium and alopecia areata, yes. There may be conditional situations where this might be true for scarring alopecias.
For cases of androgenic alopecia, the clinical data suggests hair loss treatments need to be lifelong. Some studies have indicated that adding microneedling to minoxidil might enhance the staying power of minoxidil’s hair gains by several months, even 6+ months after quitting both interventions.
We talk about these phenomena in this video. Remember that the data are preliminary, so don’t quit any treatments because of that study.
So, why not take action now and begin a regrowth protocol to put yourself in the best possible future position? Any progress made will, at the very least, slow down the progression of hair loss over time, providing benefits even without a lifelong commitment to treatment.
References[+]
References ↑1 Price, V.H., Menefee, E., Strauss, P.C., (1999). Changes in hair weight and hair count in men with androgenetic alopecia after application of 5% and 2% topical minoxidil, placebo, or no treatment. Journal of American Academy of Dermatology. 41(5.1). 717-721. Available at: https://doi.org/10.1016/s0190-9622(99)70006-x ↑2, ↑3 Kaufman, K.D., Olsen, E.A., Whiting, D., Savin, R., DeVillez, R., Bergfeld, W., Price, V.H., van Neste, D., Roberts, J.L., Hordinsky, M., Shapiro, J., Binkowitz, B., Gormley, G.J. (1998). Finasteride in the treatment of men with androgenetic alopecia. Journal of the American Academy of Dermatology. 39(4.1). 578-589. Available at: https://doi.org/10.1016/S0190-9622(98)70007-6 ↑4 Clark, R.V., Hermann, D.J., Cunningham, G.R., Wilson, T.H., Morrill, B.B., Hobbs, S. (2004). Marked Suppression of Dihydrotestosterone in Men with Benign Prostatic Hyperplasia by Dutasteride, a Dual 5alpha-Reductase Inhibitor. The Journal of Clinical Endocrinology & Metabolism. 89(5). 2179-2184. Available at: https://doi.org/10.1210/jc.2003-030330 ↑5 Kim, K.H., Park, S.M., Lee, Y.J., Sim, W.Y., Lew, B.L. (2020). Similar efficacy of maintenance treatment of finasteride 1 mg every other month compared with finasteride 1 mg daily in Korean men with androgenetic alopecia after taking finasteride 1 mg daily for 1 year. Journal of the American Academy of Dermatology. 83(6). Available at: https://doi.org/10.1016/j.jaad.2020.06.828 ↑6 Bao, L., Zong, H., Fang, S., Zheng, L.i, Y. (2022). Randomized trial of electrodynamic microneedling combined with 5% minoxidil topical solution for treating androgenetic alopecia in Chinese males and molecular mechanistic study of the involvement of the Wnt/β-catenin signaling pathway. Journal of Dermatological Treatment. 33(1). 483-493. Available at: https://doi.org/10.1080/09546634.2020.1770162 ↑7 Bao, L., Zong, H., Fang, S., Zheng, L.i, Y. (2022). Randomized trial of electrodynamic microneedling combined with 5% minoxidil topical solution for treating androgenetic alopecia in Chinese males and molecular mechanistic study of the involvement of the Wnt/B-catenin signaling pathway. Journal of Dermatological Treatment. 33(1). 483-493. Available at: https://doi.org/10.1080/09546634.2020.1770162 When it comes to microneedling vs. platelet-rich plasma, which is better? Dermatologists often recommend platelet-rich plasma therapy (PRP) as a treatment for hair loss. This autologous therapy evokes the body’s natural healing response, as does microneedling. We look at what the research studies say about the effectiveness of these two treatments. Time and cost factors are also important considerations for most people.
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is Microneedling?
Microneedling, a minimally invasive cosmetic procedure, has emerged as a promising treatment for various forms of hair loss, including androgenic alopecia (AGA). This technique involves using specialized devices, like rollers of pens, equipped with fine needles to create controlled micro-injuries on the scalp.

A derma roller for at-home microneedling.
These micro-injuries stimulate the body’s natural wound-healing processes, enhancing blood flow and promoting the release of growth factors essential for hair regeneration. This method not only improves hair density and thickness but also increases the efficacy of topical hair growth products by facilitating deeper penetration into the scalp.[1]Dhurat, R., Sukesh, M.S., Avhad, G., Dandale, A., Pal, A., Pund, P. (2013). A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study. International … Continue reading,[2]English, R.S., Ruiz, S., DoAmaral, P. (2021). Microneedling and Its Use in Hair Loss Disorders: A Systematic Review. Dermatology and Therapy. 12. 41-60. Available at: … Continue reading
What is Platelet-Rich Plasma Therapy?
Platelet-rich plasma (PRP) therapy is increasingly recognized as an effective treatment for hair loss, particularly AGA. This procedure involves drawing a patient’s blood, processing it to concentrate platelets and growth factors, and injecting this enriched plasma into the scalp.
PRP therapy stimulates hair follicles, promotes new hair growth, and enhances hair density and thickness. The growth factors and proteins in PRP promote tissue repair and regeneration, making it a promising non-surgical option for hair loss. Clinical studies have also demonstrated the efficacy of PRP in improving hair count and thickness in individuals with hair loss.[3]Gentile, P., Garcovich, S., Bielli, A., Scioli, M.G., Orlandi, A., Cervelli, V. (2015). The Effect of Platelet-Rich Plasma in Hair Regrowth: A Randomized Placebo-Controlled Trial. Stem Cells … Continue reading,[4]Cervantes, J., Perper, M., Wong, L.L., Eber, A. E., Fricke, A.C.V., Wikramanayake, T.C., Jiminez, J.J. (2018). Effectiveness of Platelet-Rich Plasma for Androgenetic Alopecia: A Review of the … Continue reading
Microneedling vs. PRP: Which Is Better?
When hair loss patients visit dermatologists for advice, it’s not uncommon for those physicians to recommend autologous therapies. These hair loss therapies, such as platelet-rich plasma (PRP) therapy, PRP + Acell, adipose-derived stem cells, exosomes, and others, are derived from our tissues. These treatments must be conducted in a clinical setting and administered by a healthcare professional. While there is scientific evidence behind these therapies, it is also a significant cash cow for dermatologists, so it is no surprise that they recommend this treatment.
What these dermatologists won’t tell patients is that there is an alternative to PRP that:
- Can be administered at home
- Leverages the exact same mechanisms of action as PRP
- Costs just a fraction of the price (usually 0.1% of the cost of a single PRP session)
- Might be just as effective as PRP
That alternative is microneedling.
What Does the Clinical Evidence Say?
Two randomized, blinded, controlled clinical trials indicate that microneedling produces the same hair parameter improvements as PRP. Let’s take a closer look at these studies and determine if PRP has any benefits over microneedling.
Study 1 – Split Scalp Study Comparing Microneedling Alone to Microneedling with PRP
This one-year-long study included 30 male patients with varying degrees of androgenic alopecia. Each participant received treatments on different halves of their scalp – one half received microneedling only, and the other half of the scalp received microneedling and PRP together. The treatments were conducted over four months, with a follow-up evaluation three months after the final session. The effectiveness was measured using dermoscopic microphotographs and patient satisfaction scores.[5]Aggarwal K, Gupta S, Jangra RS, Mahendra A, Yadav A, Sharma A. Dermoscopic Assessment of Microneedling Alone versus Microneedling with Platelet-Rich Plasma in Cases of Male Pattern Alopecia: A … Continue reading
The Results
- Hair Thickness and Density: Both treatments significantly improved hair thickness and density. The microneedling-only group nearly doubled the increase in hair thickness compared to the microneedling and PRP groups, though the difference between the groups was not statistically significant (Figure 1).
- Patient Satisfaction: Most patients reported moderate satisfaction with the treatment outcomes, noting reduced hair loss but not necessarily new hair growth.
- Long-Term Effects: A follow-up revealed that some patients experienced a recurrence of hair loss, indicating the need for ongoing or maintenance treatments.

Figure 1: Average hair density before and after treatment for microneedling and microneedling + PRP treated groups. While there were significant improvements in both groups compared to before treatment, there was no significant difference between the two groups.[6]Aggarwal K, Gupta S, Jangra RS, Mahendra A, Yadav A, Sharma A. Dermoscopic Assessment of Microneedling Alone versus Microneedling with Platelet-Rich Plasma in Cases of Male Pattern Alopecia: A … Continue reading
The Conclusion
Both microneedling and PRP can effectively treat androgenic alopecia and improve hair parameters and patient satisfaction. However, adding PRP to microneedling did not show any significant additional benefits over microneedling alone.
Study 2 – PRP Compared to Saline Injection
Another study was conducted with 26 women with female pattern hair loss. The women were randomly assigned to receive either 10 mL of PRP or a normal saline placebo. The study’s primary endpoints were hair count and hair mass index (HMI), measured at baseline and after 26 weeks. Additionally, a patient survey was conducted to gauge personal perceptions of treatment effectiveness.[7]Puig CJ, Reese R, Peters M. Double-Blind, Placebo-Controlled Pilot Study on the Use of Platelet-Rich Plasma in Women With Female Androgenetic Alopecia. Dermatol Surg. 2016 Nov;42(11):1243-1247. Doi: … Continue reading
The Results
- Hair Count and Mass: There was no statistically significant difference between the PRP and placebo groups regarding hair count and HMI after 26 weeks. This suggests that the needle insertion and the subsequent acute inflammation may be the reason for the improvement in hair growth, rather than the injection and the PRP (spoiler alert, you can get the same effect from just microneedling).
- Patient Survey: A small percentage (13.3%) of the treatment group reported substantial improvement in aspects like hair loss rate, hair thickness, and ease of hair management compared to the placebo group. However, these subjective improvements did not align with the objective measurements of hair count and HMI.
The Conclusion
This study, despite being well-designed, did not demonstrate a significant advantage of PRP over placebo in treating female androgenetic alopecia. The findings suggest that further research is needed to fully understand the role of PRP in hair loss treatment, including the possible contribution of the injection process beyond the growth factors in PRP.
So, it’s not looking great for PRP compared to microneedling. But are there any other redeeming qualities?
What About the Cost?
We know that PRP can improve hair loss outcomes, but it does not appear to be any more effective than microneedling. So does the cost make it more appealing?
No.
PRP is several times more expensive than microneedling. Let’s break it down a bit.
Microneedling Cost-Benefit
Let’s start with the costs:
- Initial investment: A microneedling device (roller or pen) can range from $10 – $200 for at-home devices.
- Replacement costs: Needles or cartridges, if applicable.
- Maintenance: Limited to cleaning and sterilizing the device.
Now, let’s see the benefits:
- Effectiveness: Proven to improve hair thickness and density in several studies.
- Convenience: This can be done at home.
- One-time cost: Mostly just the initial investment; very low ongoing costs.
Platelet-Rich Plasma Cost-Benefit
Costs:
- Per Session Cost: Each PRP session can range from $400 – $1300, depending on material quality and where you go.
- Annual cost: $1500 – $10,000 (assuming 3-4 sessions)
- Frequency: Initially, multiple sessions are needed, often 3-4 per year
- Maintenance: Every 6 – 12 months after the initial treatment to maintain hair regrowth.
Benefits:
- Effectiveness: Clinical studies show that it can stimulate hair growth and increase hair density (though microneedling can produce the same results).
- Professional Supervision: Performed by medical professionals, offering expertise and safety.
Based on the above information, it’s safe to say that you get more for your money with microneedling, given its effectiveness and significantly lower costs.
What About the Convenience / Ease of Use?
Several key differences become apparent when comparing the convenience and ease of use between microneedling and PRP.
Microneedling
Microneedling is notably convenient, especially with at-home devices. It allows individuals to perform the treatment at their own pace and in the comfort of their own homes, eliminating the need for frequent clinic visits. Furthermore, these devices are relatively straightforward to use. After an initial learning curve, users can quickly integrate the treatment into their routine. These sessions can also be relatively quick, often taking less than 10 minutes, and can be easily scheduled around personal routines and commitments.
If you want to learn more about integrating microneedling into your routine, look at our Ultimate Guide here.
Platelet-Rich Plasma
PRP therapy, on the other hand, is less convenient compared to microneedling due to the necessity of visiting a clinic or a healthcare provider for each session. This requires scheduling appointments, possibly taking time off work, and traveling to the clinic.
It is also not a self-administered treatment. It requires a skilled medical professional to draw the blood, process it to concentrate the platelets and inject it into the scalp. The process is more complex and clinical compared to miconeedling. Moreover, each PRP session, including preparation and treatment, takes longer than a typical microneedling session (treatment alone can take ~1 hour!), and the need to schedule and attend clinic appointments adds to the time commitment.
Overview Comparing Microneedling and PRP Therapy
Take a look at this overview table that we’ve created to get a quick comparison between the two treatments.
Criteria Microneedling PRP Therapy Effectiveness Similar improvements in hair count and thickness in comparative studies. Cost per Session Relatively low; cost primarily involves the purchasing of a microneedling device. This can range from less than $10 for a derma roller to ~$80+ for a derma pen.
If you want an aesthetician to do it for you, it can cost $50 – $150 per session.Higher. It involves the cost of blood draws, processing, and injections per session. The cost of just one injection can range anywhere from $400 – $1300, depending on the materials’ quality and where you go for treatment. Total Cost for Treatment There is a one-time cost for the device, which can be reused multiple times. Treatments (3-4 rounds) could cost $1500 – $10,000. Session Frequency It can vary; typically, once a week to once every few weeks. Every 4-6 weeks for the first 3-4 months, then maintenance treatments every 6- 12 months. Ease-of-Use/Convenience You can perform it at home but must learn the proper technique. A healthcare professional must perform it in a clinical setting. Recovery Time/Side Effects Minimal; may include temporary redness or irritation. Minimal; may include scalp tenderness, swelling, or mild pain at the injection sites. Longevity of Results Long-term consistent use is required for sustained results – however, some benefits may be retained even after the stoppage of treatment. Periodic maintenance sessions are needed for sustained results. In addition to saving time and money (which can amount to tens of thousands of dollars), it’s important to be cautious when following a dermatologist’s recommendation for PRP or any other autologous hair growth therapy. Instead, when weighing the options between microneedling and PRP, it may be wise to consider the benefits of microneedling.
References[+]
References ↑1 Dhurat, R., Sukesh, M.S., Avhad, G., Dandale, A., Pal, A., Pund, P. (2013). A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study. International Journal of Trichology. 5(1). 6-11. Available at: https://doi.org/10.4103/0974-7753.114700 ↑2 English, R.S., Ruiz, S., DoAmaral, P. (2021). Microneedling and Its Use in Hair Loss Disorders: A Systematic Review. Dermatology and Therapy. 12. 41-60. Available at: https://doi.org/10.1007/s13555-021-00653-2 ↑3 Gentile, P., Garcovich, S., Bielli, A., Scioli, M.G., Orlandi, A., Cervelli, V. (2015). The Effect of Platelet-Rich Plasma in Hair Regrowth: A Randomized Placebo-Controlled Trial. Stem Cells Translational Medicine. 4(11). 131-1323. Available at: https://doi.org/10.5966/sctm.2015-0107 ↑4 Cervantes, J., Perper, M., Wong, L.L., Eber, A. E., Fricke, A.C.V., Wikramanayake, T.C., Jiminez, J.J. (2018). Effectiveness of Platelet-Rich Plasma for Androgenetic Alopecia: A Review of the Literature. Skin Appendage Disorders. 4. 1-11. Available at: https://doi.org/10.1159/000477671 ↑5, ↑6 Aggarwal K, Gupta S, Jangra RS, Mahendra A, Yadav A, Sharma A. Dermoscopic Assessment of Microneedling Alone versus Microneedling with Platelet-Rich Plasma in Cases of Male Pattern Alopecia: A Split-Head Comparative Study. Int J Trichology. 2020 Jul-Aug;12(4):156-163. doi: 10.4103/ijt.ijt_64_20. Epub 2020 Sep 19. PMID: 33376284; PMCID: PMC7759059. ↑7 Puig CJ, Reese R, Peters M. Double-Blind, Placebo-Controlled Pilot Study on the Use of Platelet-Rich Plasma in Women With Female Androgenetic Alopecia. Dermatol Surg. 2016 Nov;42(11):1243-1247. Doi: 10.1097/DSS.0000000000000883 IngredientsPharmaceuticalsNatural RemediesCompany Reviews
By Perfect Hair Health TeamSep 10, 2025Dutasteride Before and After: 10 Success Stories
Oral dutasteride is one of the most powerful treatments for androgenic alopecia, offering deeper DHT suppression than finasteride. But what kind of results should you realistically expect? In this article, we break down how dutasteride works, what clinical studies actually show, how typical outcomes...
By Sarah King, PhDJul 31, 2025Where To Buy Topical Dutasteride?
Topical dutasteride is an exciting option in the hair loss arsenal, and sourcing it has become easier with the advent of modern telehealth. The U.S. market offers the greatest flexibility (with Ulo leading in customization and lab‑verified purity). In Canada, Xyon Health and Jupiter provide solid op...
By Sarah King, PhDJul 16, 2025Topical Minoxidil for Hair Growth: Efficacy, Safety, and How to Enhance Results
Topical minoxidil is the most established over-the-counter treatment for hair loss, with decades of use behind its FDA approval. But how does it actually work, and what determines whether it will work for you? In this article, we explore the science behind topical minoxidil, its strengths and limita...
By Sarah King, PhDJul 9, 2025Oral Minoxidil for Hair Growth: Is it Effective and Safe? Our Analysis
Oral minoxidil, once a blood pressure medication, is now gaining traction as a powerful off-label treatment for hair loss. But how does it compare to topical minoxidil, and is it safe? In this article, we explore the mechanisms behind oral minoxidil’s hair growth effects, its role in treating differ...
By Perfect Hair Health TeamJul 8, 2025Introducing Ulo: The Future of Hair Loss Telemedicine
Ulo is a new telehealth brand focused exclusively on hair growth. With its commitments to evidence, personalization, & consumer safety, the company aims to provide best-in-class products that have not only been independently lab tested, but also offer a level of customization unrivaled by other ...
By Sarah King, PhDJun 23, 2025OS-01 Hair Review: Does It Live Up to the Hype?
Curious about OneSkin’s OS-01 scalp serum that’s all over your feed? It claims to combat hair thinning by targeting cellular senescence, essentially attempting to “rejuvenate” your follicles. In this deep dive, we break down what senescence actually is, how it affects hair loss, and whether the scie...
By Sarah King, PhDJun 12, 2025Stretching The Truth: 3 Misrepresented Claims From Hair Loss Studies
Think that new hair growth product sounds too good to be true? It might be. In this article, we break down how research findings in hair loss treatments are often misinterpreted, or worse, misrepresented. From misleading percentages to press release spin, we highlight real examples involving TTFE, N...
By Ben Fletcher, PhDMay 19, 2025Does Minoxidil Cause Skin Aging?
Online discussions have raised alarms about a possible link between minoxidil and premature skin aging, especially among users reporting under-eye puffiness, dryness, and fine lines. Could a hair loss treatment really be affecting facial skin quality? This article takes a balanced look at the scienc...
By Sarah King, PhDMay 12, 2025Thermus Thermophilus Extract Does Not Increase Hair Density By 96.88%, Despite Dermatology Times’ Claims.
Can Thermus Thermophilus Extract (TTFE) really boost hair density by 96.88%? That’s what a recent Dermatology Times article claimed. But a closer look at the original study tells a very different story. In this article, we unpack the misleading interpretation of TTFE data, why it matters even when i...
By Sarah King, PhDMay 5, 2025Does Retinoic Acid (Tretinoin) Improve Hair Growth From Minoxidil?
Retinoic acid, a biologically active form of vitamin A, has long been known for its role in skin health, but could it also help with hair loss? In this article, we explore the science behind retinoic acid and its derivative tretinoin, their effects on hair follicle stem cells, and whether clinical s... - Mission Statement
 Scroll Down
Scroll Down More
More More
More