- About
- Mission Statement
Education. Evidence. Regrowth.
- Education.
Prioritize knowledge. Make better choices.
- Evidence.
Sort good studies from the bad.
- Regrowth.
Get bigger hair gains.
Team MembersPhD's, resarchers, & consumer advocates.
- Rob English
Founder, researcher, & consumer advocate
- Research Team
Our team of PhD’s, researchers, & more
Editorial PolicyDiscover how we conduct our research.
ContactHave questions? Contact us.
Before-Afters- Transformation Photos
Our library of before-after photos.
- — Jenna, 31, U.S.A.
I have attached my before and afters of my progress since joining this group...
- — Tom, 30, U.K.
I’m convinced I’ve recovered to probably the hairline I had 3 years ago. Super stoked…
- — Rabih, 30’s, U.S.A.
My friends actually told me, “Your hairline improved. Your hair looks thicker...
- — RDB, 35, New York, U.S.A.
I also feel my hair has a different texture to it now…
- — Aayush, 20’s, Boston, MA
Firstly thank you for your work in this field. I am immensely grateful that...
- — Ben M., U.S.A
I just wanted to thank you for all your research, for introducing me to this method...
- — Raul, 50, Spain
To be honest I am having fun with all this and I still don’t know how much...
- — Lisa, 52, U.S.
I see a massive amount of regrowth that is all less than about 8 cm long...
Client Testimonials150+ member experiences.
 Scroll DownPopular Treatments
Scroll DownPopular Treatments- Treatments
Popular treatments. But do they work?
- Finasteride
- Oral
- Topical
- Dutasteride
- Oral
- Topical
- Mesotherapy
- Minoxidil
- Oral
- Topical
- Ketoconazole
- Shampoo
- Topical
- Low-Level Laser Therapy
- Therapy
- Microneedling
- Therapy
- Platelet-Rich Plasma Therapy (PRP)
- Therapy
- Scalp Massages
- Therapy
- More
IngredientsTop-selling ingredients, quantified.
- Saw Palmetto
- Redensyl
- Melatonin
- Caffeine
- Biotin
- Rosemary Oil
- Lilac Stem Cells
- Hydrolyzed Wheat Protein
- Sodium Lauryl Sulfate
- More
ProductsThe truth about hair loss "best sellers".
- Minoxidil Tablets
Xyon Health
- Finasteride
Strut Health
- Hair Growth Supplements
Happy Head
- REVITA Tablets for Hair Growth Support
DS Laboratories
- FoliGROWTH Ultimate Hair Neutraceutical
Advanced Trichology
- Enhance Hair Density Serum
Fully Vital
- Topical Finasteride and Minoxidil
Xyon Health
- HairOmega Foaming Hair Growth Serum
DrFormulas
- Bio-Cleansing Shampoo
Revivogen MD
- more
Key MetricsStandardized rubrics to evaluate all treatments.
- Evidence Quality
Is this treatment well studied?
- Regrowth Potential
How much regrowth can you expect?
- Long-Term Viability
Is this treatment safe & sustainable?
Free Research- Free Resources
Apps, tools, guides, freebies, & more.
- Free CalculatorTopical Finasteride Calculator
- Free Interactive GuideInteractive Guide: What Causes Hair Loss?
- Free ResourceFree Guide: Standardized Scalp Massages
- Free Course7-Day Hair Loss Email Course
- Free DatabaseIngredients Database
- Free Interactive GuideInteractive Guide: Hair Loss Disorders
- Free DatabaseTreatment Guides
- Free Lab TestsProduct Lab Tests: Purity & Potency
- Free Video & Write-upEvidence Quality Masterclass
- Free Interactive GuideDermatology Appointment Guide
- More
Articles100+ free articles.
-
Does Anavar Cause Hair Loss?
-
10 Best Shampoos for Hair Loss in 2026
-
XYON Review: Do Their Products Actually Regrow Hair?
-
Minoxidil Before and After Photos [2026] | Does It Work?
-
How to Get Finasteride: Is It Over the Counter?
-
Keeps Review: The Truth About Their Hair Loss Treatments?
-
7 Best Oils for Hair Growth
-
Hims Hair Growth Reviews: The Pros, Cons, and Real Results
PublicationsOur team’s peer-reviewed studies.
- Microneedling and Its Use in Hair Loss Disorders: A Systematic Review
- Use of Botulinum Toxin for Androgenic Alopecia: A Systematic Review
- Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia
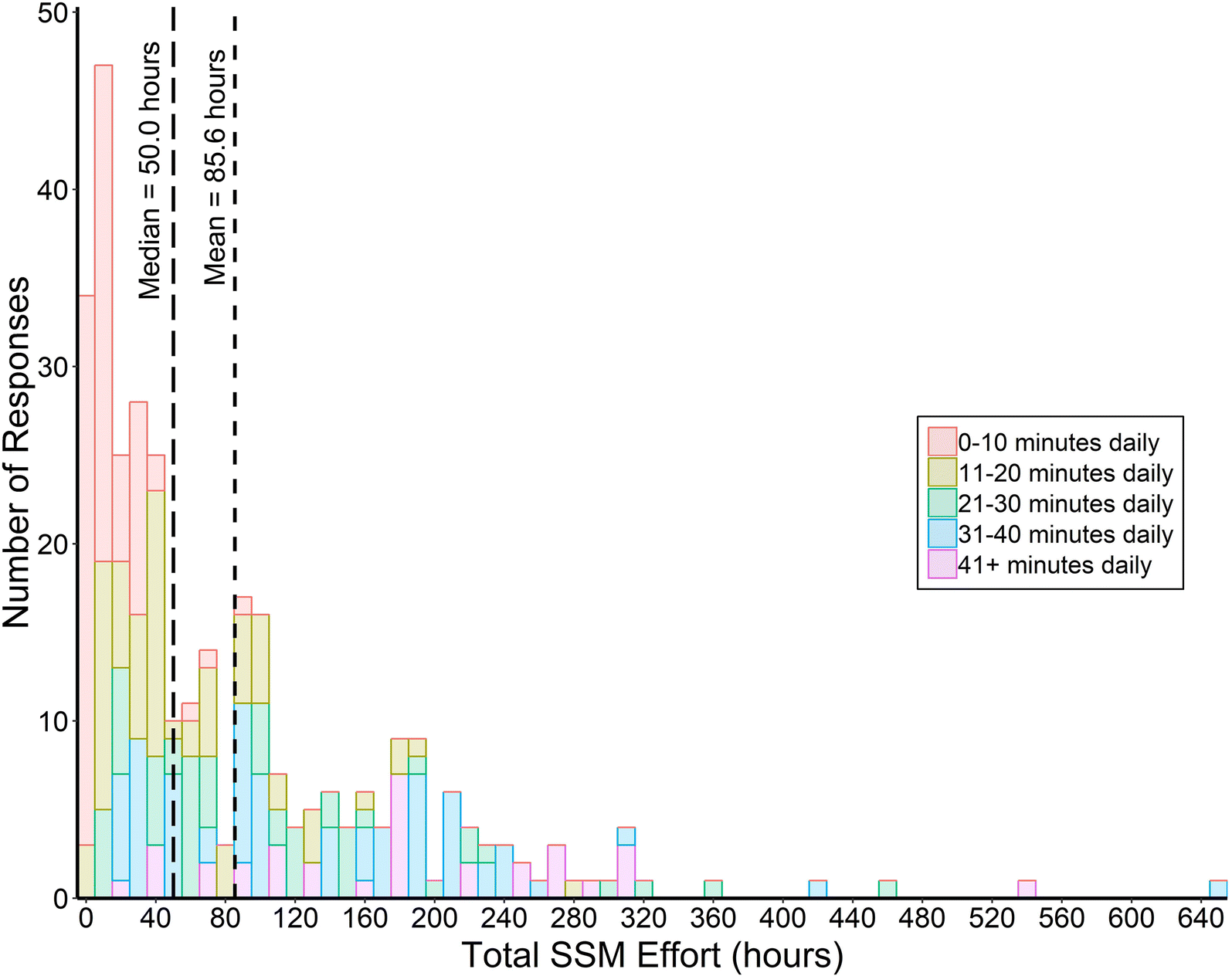
- Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results
- A Hypothetical Pathogenesis Model For Androgenic Alopecia:Clarifying The Dihydrotestosterone Paradox And Rate-Limiting Recovery Factors
Menu- AboutAbout
- Mission Statement
Education. Evidence. Regrowth.
- Team Members
PhD's, resarchers, & consumer advocates.
- Editorial Policy
Discover how we conduct our research.
- Contact
Have questions? Contact us.
- Before-Afters
Before-Afters- Transformation Photos
Our library of before-after photos.
- Client Testimonials
Read the experiences of members
Before-Afters/ Client Testimonials- Popular Treatments
-
Articles
Histamine and Hair Loss
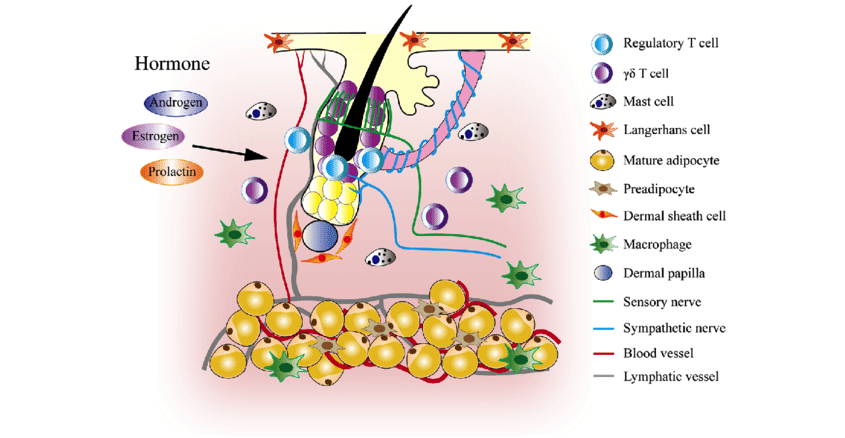
Our hair follicles are part of a niche of cells intimately involved in proper immune function. For example, right next to the dermal papilla, the type of cell that grows our hairs, there are a number of immune cells including:
- Macrophage, which helps remodel our extracellular matrix and clean up waste.
- Basophils, which help neutralize foreign particles.
- Neutrophils, which keep pesky microorganisms present on our scalps, in check.
- And in reference to today’s topic, Mast cells which secrete histamine to neutralize foreign invaders.

Chen, Chih-Lung & Huang, Wen-Yen & Wang, Eddy & Tai, Kang-Yu & Lin, Sung-Jan. (2020). Functional complexity of hair follicle stem cell niche and therapeutic targeting of niche dysfunction for hair regeneration. Journal of Biomedical Science. 27.
Mast cells can become counterproductive though when too much histamine is secreted. They induce immunoglobulin secretion by our B-cells (those same cells that act as antibodies to viruses), such as the release of IgE – the same immunoglobulin that can create anaphylactic shock.
Histamine is also a pro-inflammatory cytokine (a signaling molecule), that can generate a number of unwanted cell responses that tend to progress hair loss.
In this article, we take a look to see just how much are mast cells and histamine to blame for hair loss, and what can be done about this. We also take a look at the evidence for the use of antihistamines as a hair loss reversal tool.
Interested in Topical Cetirizine?
Support your hair with full-strength topical cetirizine, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.

What Is The Role Of Histamine In Hair Loss?
How Histamine Works
Histamine is counterintuitively not a hormone, instead, it’s actually a simple amino acid. We get histamine thanks to consuming its precursor amino acid histidine. And it is vitally important for maintaining normal physiology.
Histamine also binds to four receptors. Some of which are located on our skin, some in our gastrointestinal system, and some in our brain. Histamine in the brain is also important for acting as a neurotransmitter.
It’s the excess of histamine signaling that becomes problematic.
A perfect example of excessive histamine signaling being bad is in the case of seasonal allergies, or food allergies. Anyone who has had experience will know how quickly and fiery the body responds to these allergens. This is all due to the release of histamine and how it interacts with those receptors.
With excess histamine signaling, people become easily irritated and prone to inflammation. Body temperature also increases and the vascular system becomes more permeable, causing immune cells to leak into unwanted places.
This opening of our vascular system and leaking of immune cells in unwanted places is actually one way histamine connects to hair loss.
The Histamine-Hair Loss Connection
Because hair follicles and scalp act as a breeding ground for a variety of microorganisms, it is also very prone to exacerbated histamine signaling if the scalp biome balance is thrown off. Further, because histamine responds to changes in hormone levels, it’s very possible that the shift experienced with androgenic alopecia also increases histamine production.
Both androgenic alopecia and alopecia areata also show signs of dysregulated histamine signaling. Histamine in excess can induce pro-inflammatory cascades that cause premature apoptosis of cells, especially as it relates to the dermal papilla.
This rapid apoptosis can extend to cells (such as stem cells) sitting on our epidermis. Stem cells in the subcutaneous tissue and on the hair follicle’s outer root can bulge. Premature apoptosis of these cells makes it increasingly difficult to regrow hair since the stem cells which contribute to hair renewal are no longer present.
The Evidence For Histamine Contributing To Hair Loss
While the discussion on histamine specifically is rather sparse in relation to hair loss, there have been some advances in the past years on the role of histamine overall. For example …
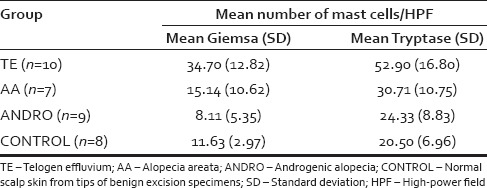
- When humans experience stress, the body tends to release histamine in much larger amounts. This excess of histamine is believed to affect our hair follicles and act as part of the pathophysiology of stress-induced telogen effluvium. In the following study, patients with telogen effluvium had significantly higher numbers of mast cells and the enzyme tryptase.[1]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5514792/.
Tryptase is an enzyme involved in the degradation of proteins, specifically by removing lysine, histidine, and arginine. Higher tryptase is also a hallmark of mast cell activation.

Grace SA, Sutton AM, Abraham N, Armbrecht ES, Vidal CI. Presence of Mast Cells and Mast Cell Degranulation in Scalp Biopsies of Telogen Effluvium. Int J Trichology. 2017;9(1):25-29
- Alopecia areata is one of the more commonly accepted forms of hair loss due to the immune system going awry. In alopecia areata, there is a large change in immune function due to the loss of immune privilege. Immune privilege is a mechanism the body uses to keep immune cells out of certain sensitive tissues.
When the hair follicles experience a collapse of immune privilege, they also experience a dramatic increase in a variety of immunological factors. Specifically, a rise in lymphocytes like CD8+ T-cells, and IgE. Both of which are either triggers/ secrete (T-cells) histamine or can be triggered by histamine release from mast cells.
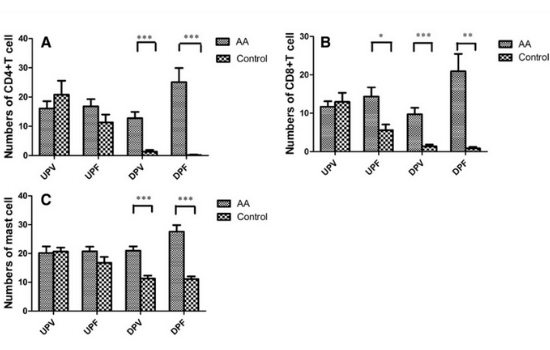
Specifically, the deep perivascular and perifollicular regions of those with alopecia areata, when compared to controls, had higher CD4+ T cell count, and CD8+ T cell count. They also had more mast cells.

Zhang X, Zhao Y, Ye Y, Li S, Qi S, Yang Y, Cao H, Yang J, Zhang X. Lesional infiltration of mast cells, Langerhans cells, T cells and local cytokine profiles in alopecia areata. Arch Dermatol Res. 2015 May;307(4):319-31. doi: 10.1007/s00403-015-1539-1. Epub 2015 Feb 1. PMID: 25638328.
These findings reached multiple orders of magnitude in terms of significance. Interestingly, this was not really something of concern when it came to the upper dermal region. Indicating that unless we look further down the dermis, we are unlikely to see any noticeable changes in immune profiles.
- Androgenic alopecia is often discussed as only ever being due to the increase in androgen signaling. Specifically, the production of DHT from testosterone via the 5AR enzyme and its binding to the androgen receptor. However, what isn’t often discussed is what happens afterward?
It’s not as if the androgen and the androgen receptor are initiating hair loss. Instead, the androgen receptor with DHT translocates into our cell’s nucleus and then tells the cell to change genetic expression. Some of those genes (but not all), happen to be genes for the production of extracellular matrix.
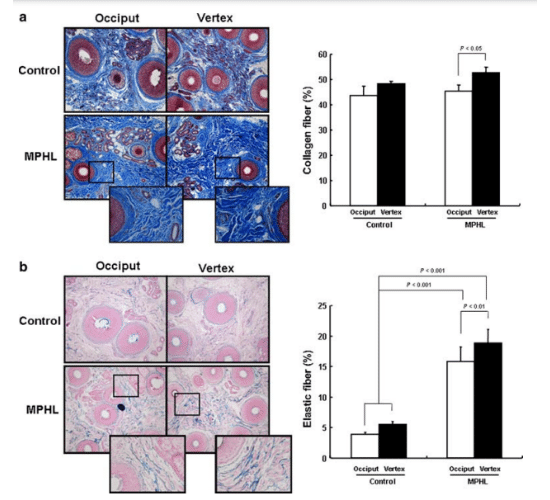
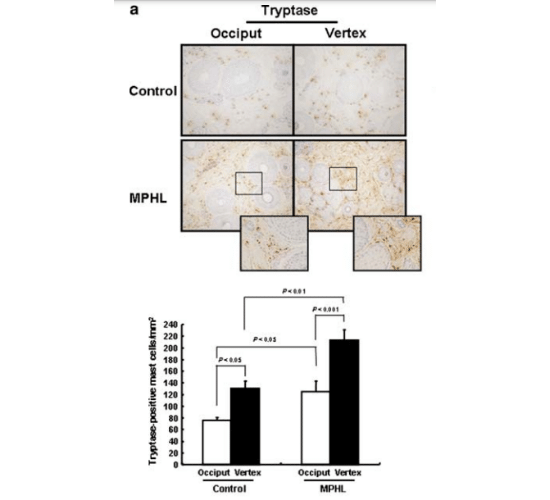
This can lead to the overproduction of elastin, leading to a feeling of hard tissue often referred to as fibrosis of the scalp. In another case-control study, the increase in collagen fibers, elastin, and the lower diameter of hair follicles, was apparently clear in those with androgenic alopecia.[2]https://pubmed.ncbi.nlm.nih.gov/18286292/

Won CH, Kwon OS, Kim YK, Kang YJ, Kim BJ, Choi CW, Eun HC, Cho KH. Dermal fibrosis in male pattern hair loss: a suggestive implication of mast cells. Arch Dermatol Res. 2008 Mar;300(3):147-52. doi: 10.1007/s00403-007-0826-x. Epub 2008 Feb 20. PMID: 18286292.
Figure (a) and the graph to the right of it are indicating the increase of collagen bundles in the occiput and vertex of either controls or those with AGA. While the occiput didn’t differ much, the vertex was clearly different.
Figure (b) is indicating the increase in elastin seen in those with androgenic alopecia as compared to control.
And when it came to mast cells, those with androgenic alopecia also had a higher level of the enzyme tryptase (again indicative of mast cell activation). Interestingly, tryptase is also a well known factor involved in the activation of TGF-ß and collagen remodeling, potentially pointing to a role of mast cells in the fibrosis of those with AGA.
Won CH, Kwon OS, Kim YK, Kang YJ, Kim BJ, Choi CW, Eun HC, Cho KH. Dermal fibrosis in male pattern hair loss: a suggestive implication of mast cells. Arch Dermatol Res. 2008 Mar;300(3):147-52. doi: 10.1007/s00403-007-0826-x. Epub 2008 Feb 20. PMID: 18286292.
It’s important to keep in mind that these findings were for a total of 10 patients and 5 controls. A greater sample size range is required to definitively tell if this is either a correlation or a fluke.
Interestingly, the increase in TGF-ß signaling appears to be contradictory when it comes to alopecia areata. In androgenic alopecia it’s implicated as a fibrosis-inducing agent, while in alopecia areata, the loss of TGF-ß is a precursor step to loss of immune privilege.
This change in activity of TGF-ß is known to be induced by a shift in mast cells from an immune-inhibitory role to a pro-inflammatory role.[3]https://pubmed.ncbi.nlm.nih.gov/24832234/
One research group had actually investigated this separately with a mice model and determined with incredible accuracy that one of the reasons for the differential response of mast cells as either good or bad, is partly due to the scalp microbiome and dermal fibroblasts.[4]https://pubmed.ncbi.nlm.nih.gov/30928651/
The mice study showed that the scalp microbiome activates toll-like receptors (a type of immune recognition receptor) and amplifies progenitor cells from the keratinocyte to become mast cells. Further, a change in how the mast cells behaved was seen. One of immune inhibition into one of pro-inflammation and immune cell recruitment.
It’s possible that for alopecia areata, a change in how the scalp microbiome interacts with immune cells is the prelude to the disease. While with androgenic alopecia, a change in how mast cells behave is a prelude to premature apoptosis of the dermal papilla cells.
Do Antihistamines Work Against Hair Loss?
The next step in assessing the role of mast cells in hair loss is to consider if anyone has looked at the use of antihistamines for hair loss. After all, while mechanistic and observational data connecting histamines to hair loss are important, interventional studies are really the only way to ascertain cause and effect.
Luckily, there are some research papers that addressed this question.
The first study investigated the antihistamine drug cetirizine (if you’ve ever tried claritin or zyrtec, this is the same active ingredient), because of its known inhibitory actions on histamine-1 receptors and PGD2 (a proinflammatory prostaglandin shown to worsen androgenic alopecia).[5]https://onlinelibrary.wiley.com/doi/abs/10.1111/jocd.13940
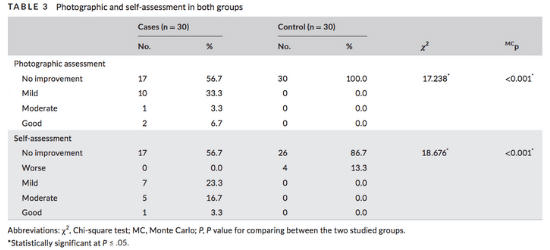
What the authors did was give 30 participants a 1% solution of topical cetirizine at 1mL doses. The second group which served as a control group was given a placebo solution. After six months these were the results:

Zaky, M. S., Abo Khodeir, H., Ahmed, H., & Elsaie, M. L. (2021). Therapeutic implications of topical cetirizine 1% in treatment of male androgenetic alopecia: A case‐controlled study. Journal of Cosmetic Dermatology, 20(4), 1154–1159.
Essentially, the control group showed no improvement with 4/30 of them seeing worsening responses. While the treatment group saw sparse improvements in photographic assessments and self assessments. Nothing too crazy, but still better than the control group.
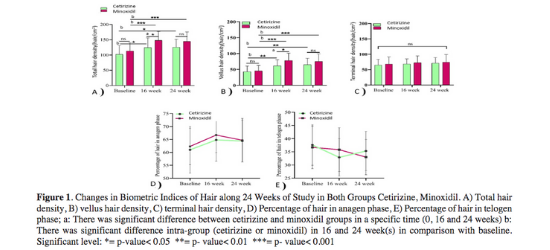
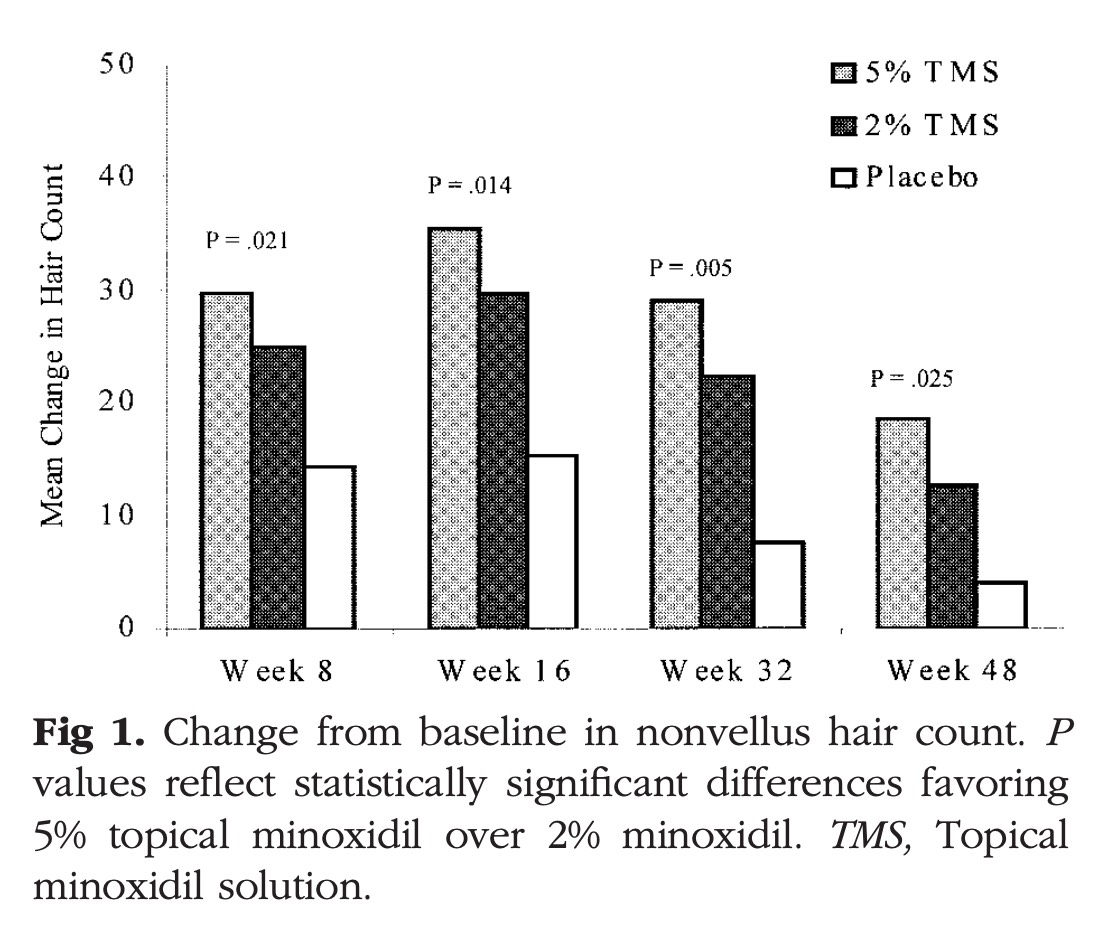
In a second study, researchers compared 1% cetirizine vs. 5% minoxidil. In this randomized controlled trial, both groups saw great results in terms of hair density, hair diameter and other hair loss parameters. Minoxidil however, outperformed topical cetirizine.[6]https://journals.library.ualberta.ca/jpps/index.php/JPPS/article/view/31456/21623
This is expected since minoxidil works by promoting the anagen phase of hair follicles. Cetirizine simply works by blocking the uptake of histamine in the histamine-1 receptor. This is fascinating to note though as by simply blocking the cellular actions of histamine, cetirizine has comparability to minoxidil.
Hossein Mostafa, D., Samadi, A., Niknam, S., Nasrollahi, S. A., Guishard, A., & Firooz, A. (2021). Efficacy of Cetirizine 1% Versus Minoxidil 5% Topical Solution in the Treatment of Male Alopecia: A Randomized, Single-blind Controlled Study. Journal of Pharmacy & Pharmaceutical Sciences, 24, 191–199.
Their outcomes showed some of the following features:
- Although baseline levels of hair density were higher in the minoxidil group, the cetirizine group had close efficacy. Keeping up with the results of the minoxidil group.
- Minoxidil had better results in terms of vellus hair density, despite starting with a higher baseline. And minoxidil had equal efficacy as cetirizine did in regards to terminal hair density.
- Cetirizine group had a greater reduction in telogen hair follicles 16-weeks in compared to minoxidil. But this effect rebounded slightly during the 24-week mark. Why this is the case is hard to determine.
Nonetheless, a combined therapy may be even more potent at addressing hair loss…
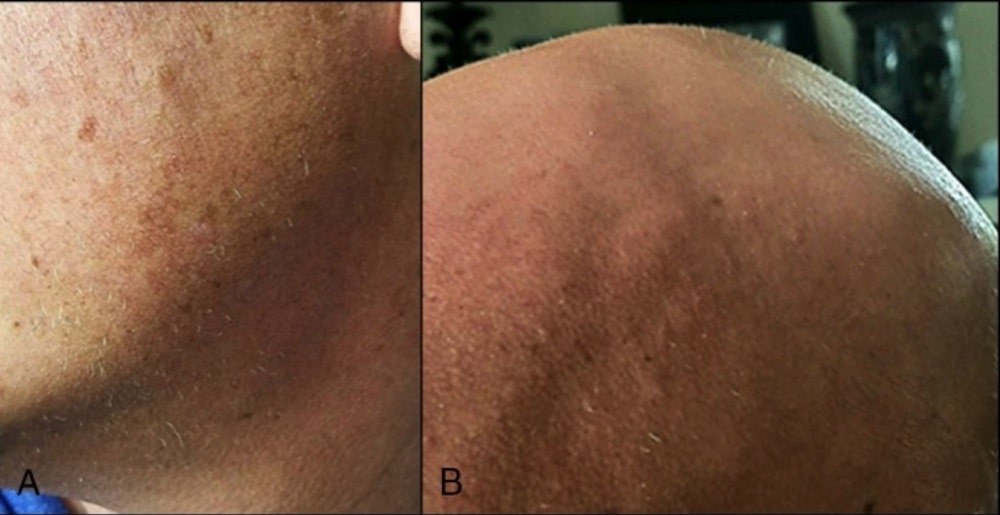
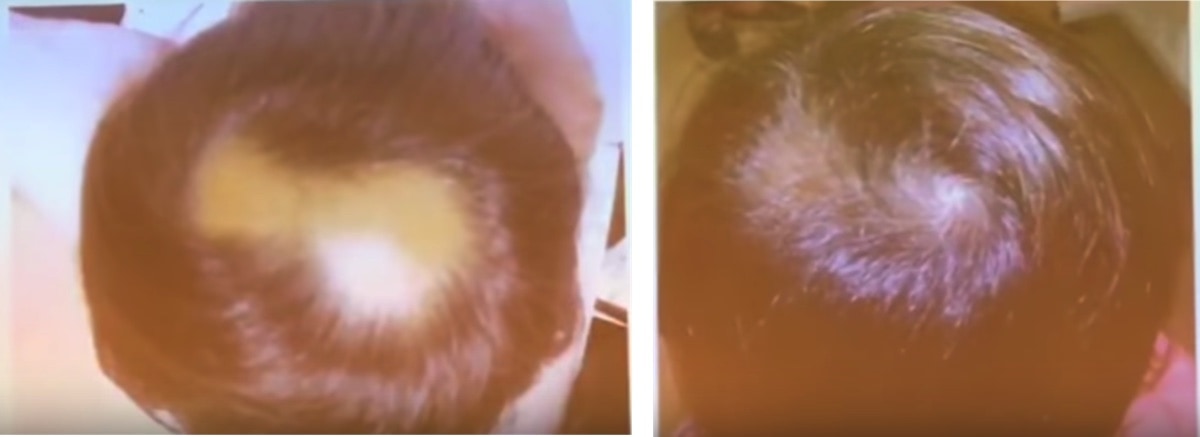
In the final study on cetirizine, patients were once again administering 1mL of a 1% solution of cetirizine topically. After six months, a dramatic improvement in hair regrowth was seen for the participants when compared to the control group.[7]https://pubmed.ncbi.nlm.nih.gov/28604133/

Rossi, A., Campo, D., Fortuna, M. C., Garelli, V., Pranteda, G., De Vita, G., … Carlesimo, M. (2017). A preliminary study on topical cetirizine in the therapeutic management of androgenetic alopecia. Journal of Dermatological Treatment, 29(2), 149–151.
The top row indicates the beginning of the study for the participants. While the bottom row indicates the end of the study. A clinical difference can be seen in all of the patients’ hairlines. In all cases, there were no known side effects too.
What’s Our Take On The Data?
There is a clear rationale for the induction of mast cells in the pathology of possibly all forms of hair loss, including a connection to immune defects like telogen effluvium. Mast cells play a critical role in feedback from the scalp microbiome to our scalp cell niche.
When mast cells go awry, they release histamine, tryptase, and a number of other factors that cause extracellular matrix remodeling, recruitment of immune cells, and a vicious cycle progressively worsening with time.
Addressing the excess histamine production by interfering with the histamine-1 receptor with cetirizine, abrogates most of the negatively associated responses and actually does seem to allow regeneration of hair follicles.
Based On The Evidence
The use of topical cetirizine can be a very appropriate tool to implement with androgenic alopecia and alopecia areata. The rise of mast cells and the enzyme tryptase in patients with telogen effluvium as compared to controls also provides a very compelling argument as to how stress correlates with hair shedding disorders.
It is with the totality of the current evidence, prior knowledge on the mechanisms of mast cells and their roles in our bodies, as well as the efficacy of antihistamines in improving hair loss, that we believe the weight of the evidence largely supports a causal role of mast cells in the development of various forms of hair loss.
What Then Should Be Done?
Since topical cetirizine consistently shows a net benefit in all the current clinical trials, the most logical addition should be topical cetirizine for any hair loss disorder. It may be that in conjunction with minoxidil, large improvements can be acquired.
Further, with topical anti-inflammatories, cetirizine can dramatically reduce the apoptosis rate of precious stem cells surrounding our hair follicles. There are alternatives to cetirizine that operate in similar mechanisms, reducing histamine release and subsequent binding to histamine-1 receptors.
Some of the useful ingredients that can reduce histamine production and the effects of histamine include:
- Vitamin B6.
- Copper.
- Vitamin C.
- Iron.
- Vitamin D.
- Ginger.
- Garlic.
- MSM.
And many more. A majority of the micronutrients and vitamins are also key cofactors for proper function of the enzymes involved in histamine degradation – such as Diamine oxidase and Histamine-N-Methyl Transferase enzymes.
Product Recommendations
Although we can’t generally acquire topical cetirizine, one can be made by dissolving 1 g in 100mL of water. Forming 1% w/v cetirizine, just as outlined in the studies. The only difference would be that the study used a form of alcohol instead of water.
A simple formulation you can make at home includes:
- Take 1 g of Cetirizine, crush it in a mortar, and pestle very finely.
- Dissolve it in 100mL of water.
- Add 1-5mL of ethyl alcohol (70-90%).
- Add 1-5mL of Coco glucoside to help with absorption, or more depending on the consistency you would like.
- Thoroughly mix the ingredients and store it in a dark brown bottle with a 1mL serving pump.
*Note: If you plan on using oral antihistamines, remember that they distribute widely throughout the body, not just the skin. The compounds prevent histamine from binding to the brain which is one of the reasons for the drowsy feeling many experience with Zyrtec or Claritin.
References[+]
References ↑1 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5514792/ ↑2 https://pubmed.ncbi.nlm.nih.gov/18286292/ ↑3 https://pubmed.ncbi.nlm.nih.gov/24832234/ ↑4 https://pubmed.ncbi.nlm.nih.gov/30928651/ ↑5 https://onlinelibrary.wiley.com/doi/abs/10.1111/jocd.13940 ↑6 https://journals.library.ualberta.ca/jpps/index.php/JPPS/article/view/31456/21623 ↑7 https://pubmed.ncbi.nlm.nih.gov/28604133/ To some extent, every hairline is unique. But there are identifiable hairline patterns, primarily based on age, gender and genetics. As men age, their hairline will typically recede a bit, known as ‘maturing.’ While this can understandably make men nervous, it’s not always a sign of male pattern balding. In this post, we’ll review the following:
- What defines a mature hairline
- What defines a receding hairline
- The difference between a mature and receding hairline
- How to treat a receding hairline
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
What is a Mature Hairline?

The hairline is the boundary between hair follicles and the forehead. Everyone’s hairline is unique, although there are some patterns that occur throughout our lives.
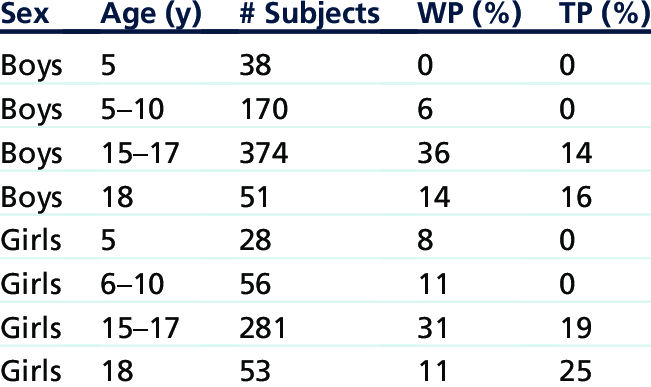
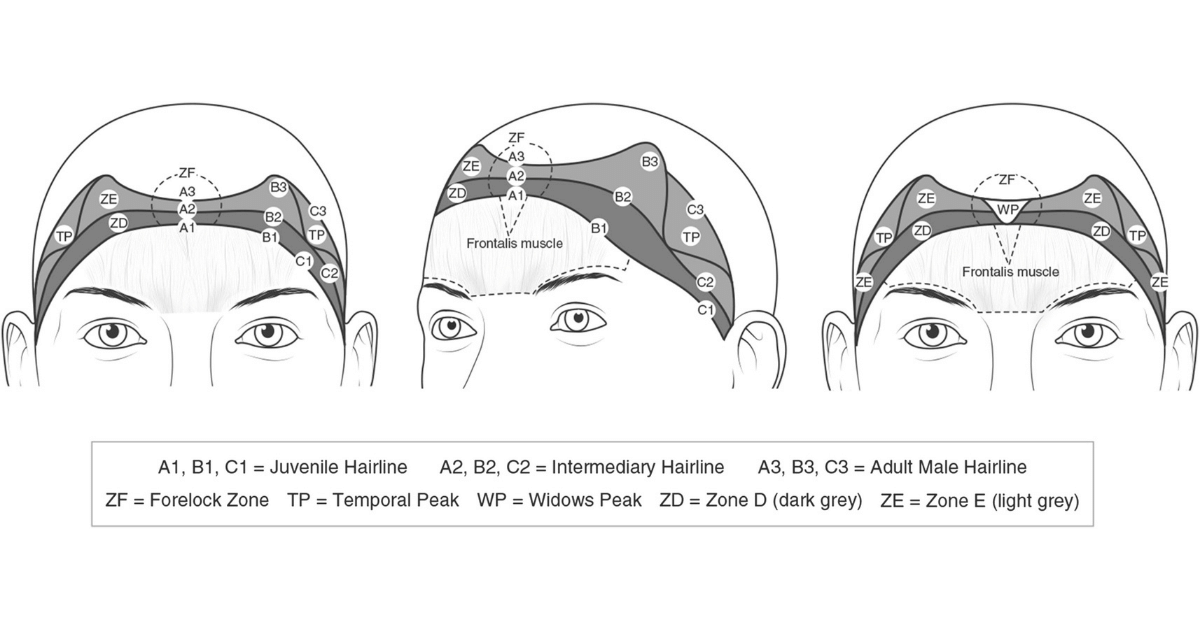
According to observational studies, prepubescent men and women both experience concave shaped hairlines. This generally concave hairline is similar across all races and ethnicities. Around the age of 10, a small percentage of children develop a widow’s peak, but this is not an effect of recession at the temples.[1]https://www.researchgate.net/publication/256479799_Phenotype_of_Normal_Hairline_Maturation

Full citation: Rassman, William & Pak, Jae & Kim, Jino. (2013). Phenotype of Normal Hairline Maturation. Facial plastic surgery clinics of North America. 21. 317-24. 10.1016/j.fsc.2013.04.001.
As young teens, when hair is fullest, there’s typically a stark boundary between the hair on the head and the forehead. In men especially, this changes with age. It’s believed that hormonal changes trigger the expression of certain genes, causing men’s hairlines to mature between mid-adolescence and middle-age. This maturation means the hairline shifts a few centimeters further back on the forehead.
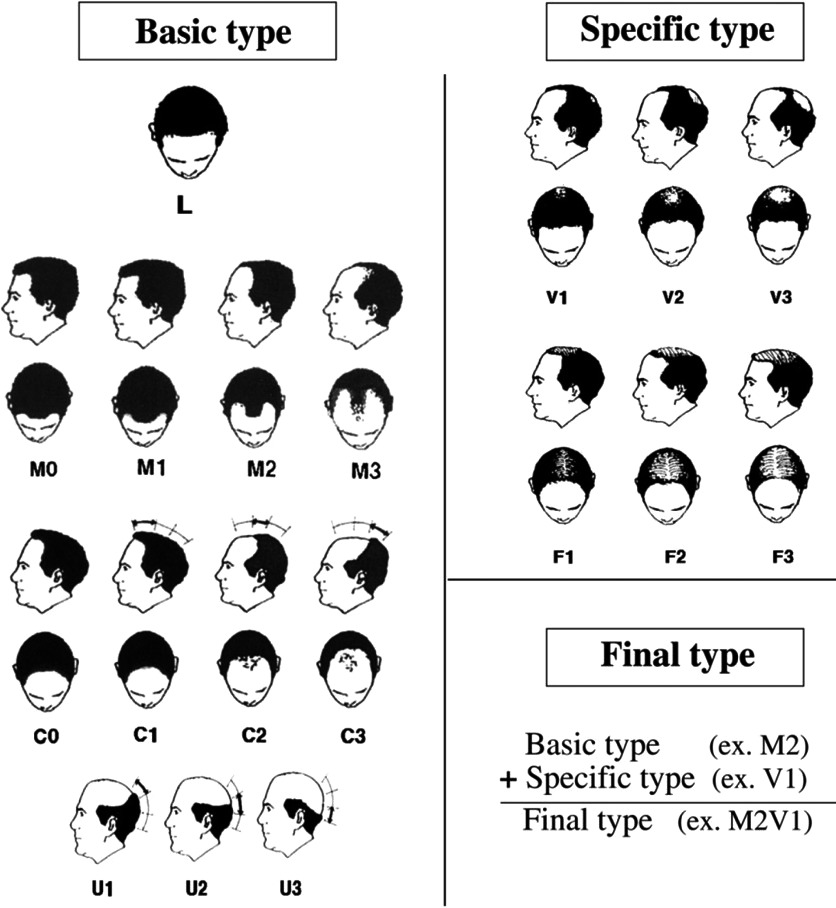
This shift may take place uniformly, following the rounded shape of the juvenile hairline, or may be more noticeable at the temples, resulting in a hairline that looks more like a letter M. There appears to be a relationship between the muscles of the forehead, the frontalis muscle, and the height of the hairline. Most adults with high mature hairlines have presented with high foreheads their entire lives. The varying degrees of normal hairline maturation can be seen in the image below.

Full citation: Rassman, William & Pak, Jae & Kim, Jino. (2013). Phenotype of Normal Hairline Maturation. Facial plastic surgery clinics of North America. 21. 317-24. 10.1016/j.fsc.2013.04.001.
As hairlines mature with age, some men hardly notice this change, as it occurs slowly over a period of 10 years or more. In others, this change happens more rapidly, causing concern.
Regardless of when or how quickly it happens, what characterizes a mature hairline is that the recession is limited to just a few centimeters, and then it stops. The hairline does not continue to recede, and remains well-defined, with little to no hair thinning.
A maturing hairline is a natural part of aging, and not indicative of androgenic alopecia (AGA), otherwise known as male pattern baldness.
At What Age Does Mature Hairline Stop?
If and when a juvenile hairline begins to recede, the most commonly asked question is – when does it typically stop?
Just as there’s no telling if and when the hairline will mature, there’s no predicting when a mature hairline will stop. A slightly different, but better question is – how do you differentiate between a maturing hairline, which will eventually stop receding, and receding hairline, which is a sign of male pattern baldness?
To answer this, we begin with an understanding of receding hairlines.
Take the guesswork out of growing hair.
Bypass years of trial and error. Get a personalized Regrowth Roadmap tailored to your hair loss type and treatment preferences. And leverage our support to implement it effectively.
Join Now
What is a Receding Hairline?
A receding hairline is among the earliest signs of androgenic alopecia. AGA often follows a predictable pattern. This pattern begins with a receding hairline, which is especially noticeable at the temples. Simultaneously or sequentially, hair then disappears from the crown of the head. Eventually, complete baldness occurs as the hairline recedes far enough back, and/or baldness from the crown of the head meets the hairline.
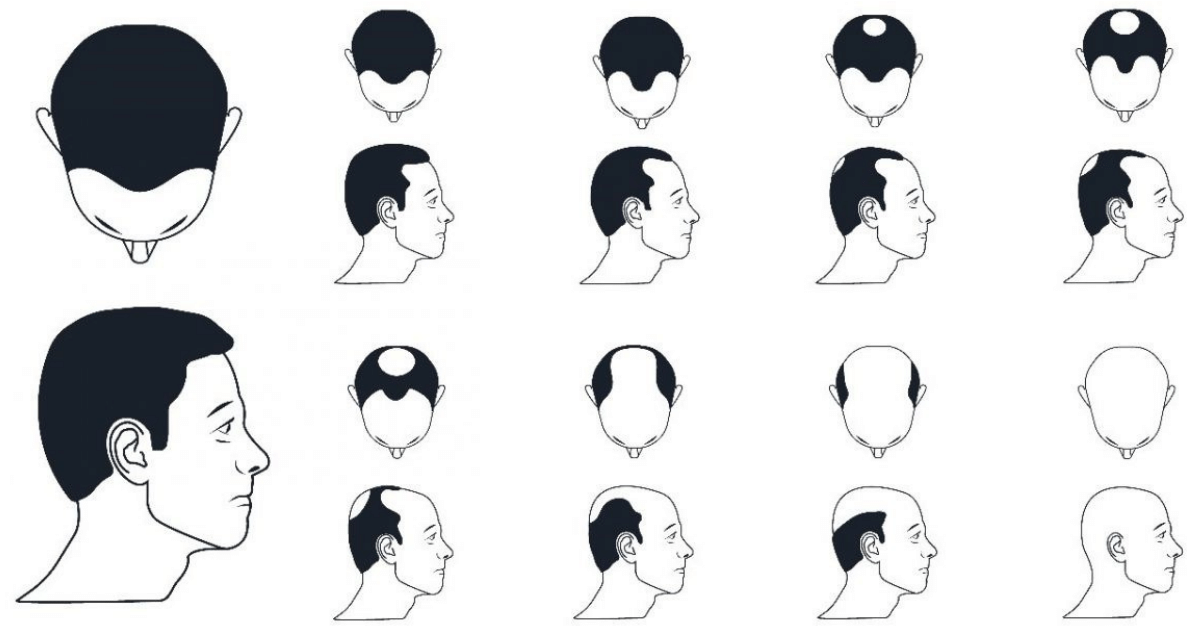
The Norwood-Hamilton scale is used by dermatologists to assess progression of AGA. By stage 2, minor recession of the hairline exists, although it’s barely differentiated from a maturing hairline. By stage 3, the hairline has receded much further at the temples, characteristic of androgenic alopecia.
What Causes a Receding Hairline?
Hair shedding is a common part of the normal hair growth cycle. Most people lose somewhere between 50-100 hairs each day, which typically goes unnoticed. When hair loss is localized to the front of the scalp and regrowth does not occur, the hairline recedes.
Age, genetics, gender, hormones, or how you care for and style your hair can all contribute to a receding hairline.
Age: While AGA can occur in children, it’s very rare. Most of the hairline changes that occur with age are not reflective of AGA, until after the age of 17. As we age, the chances of developing a receding hairline increase. Androgenic alopecia is more common in those who are middle-aged or older.
Genetics: Research suggests that there is no single gene involved in AGA. Rather, pattern hair loss is likely a polygenic disorder, meaning there are many gene variances that are involved in the predisposition of its development. Exactly which genes are responsible is still unknown, although a family history of androgenic alopecia is still its single greatest predictor.
Gender: Men are more likely than women to have a receding hairline. Although women do experience AGA, it more often presents as overall hair thinning and baldness that begins at the top of the scalp, and not a receding hairline.
Hormones: While the hormone dihydrotestosterone (DHT), is responsible for growth of hair on the body, this testosterone derivative also contributes to hair follicle miniaturization, and ultimately, hair loss. Although it’s unknown why AGA forms the pattern it does, the answer might have to do with androgen receptor density and 5α-reductase activity at the hairline.
Lifestyle: The onset of a receding hairline may be accelerated from certain forms of stress, medications, scalp environment, and/or hair styling — such as pulling hair too tight. Hair loss may arise from hormonal conditions unrelated to DHT, such as hypothyroidism or hyperthyroidism. Gut dysbiosis, heavy metal toxicity, and vitamin deficiency can all contribute to hair loss.
Unlike maturing hairlines, receding hairlines are not part of the normal aging process, but a sign of androgenic alopecia, another form of hair loss, or both.
Mature vs Receding Hairlines
A mature hairline doesn’t always become a receding hairline. So what indicates the difference between the two, and how can we tell the difference between early AGA and a simple shift in the hairline?
Timing of Hair Loss: Hairlines tend to mature in late adolescence or early adulthood. Generally, receding hairlines start later in life.
Pace of Hair Loss: A receding hairline tends to progress at a faster pace. While a maturing hairline may go unnoticed – a receding hairline is more likely to attract attention.
Shape of Hair Loss: A receding hairline tends to move more towards an M-shape, with hair loss at the temples far more pronounced. A mature hairline, on the other hand, will move back more evenly.
Extent of Hair Loss: As the hairline matures, it may move back 1-2 centimeters. With a receding hairline, this shift can be 1 inch or more.
Thinning of Hair: As a hairline matures, hair maintains its original thickness. Receding hairlines, on the other hand, are accompanied by hair thinning.
Diagnosing a Receding Hairline
A receding hairline is characteristic of androgenic alopecia, but it’s possible to have more than one type of hair loss, especially if the hairline is receding and hair is thinning or balding in other areas.
In the shower, when washing your hair, take all the hairs you shed onto your hands and stick them to the wall using the steam from the shower.
- Are the hairs of varying diameters? This is indicative of hair follicle miniaturization, a defining characteristic of AGA.
- Are the hairs all equal in thickness? This suggests no hair follicle miniaturization, and an AGA diagnosis is less likely. You could have a hair shedding disorder.
A doctor or dermatologist can help identify exactly which type of hair loss is present. This is important, for treatment protocols will vary depending on the cause of hair loss.
How to Prevent Further Receding
There isn’t one single solution for hair loss, which makes diagnosing the cause and type of hair loss important. But in general, a comprehensive solution will address the following:
- Regrowth Regimens: Depending on personal preferences, this could include medications or other science-based hair regrowth regimens.
- General Health: This includes specific dietary and lifestyle interventions based on age, gender, and type of hair thinning to address any conditions linked to the hair loss. While poor general health may accelerate hair loss, for most people, it’s very much a secondary factor in terms of influence over a receding hairline.
Of course, no treatment is always an option. Many choose to change hair styles in an effort to hide a receding hairline, or are comfortable living with it as is. If choosing treatment, factors to consider include how much time and money to invest on hair regrowth, tolerance for side-effects, and personal preference.
A few possible interventions are listed below (and not in order of importance or clinical efficacy).
Massaging: Massaging the scalp for 15 minutes, twice daily has the ability to activate the body’s innate healing responses, and reduce scalp tension. Our own study showed that 75% of people who massaged consistently for 8 months reported a stop or partial reversal in their hair thinning.[2]https://link.springer.com/article/10.1007/s13555-019-0281-6

English, R.S., Barazesh, J.M. Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results. Dermatol Ther (Heidelb) 9, 167–178 (2019).
Shampoos: Ketoconazole shampoo is not actually FDA-approved for pattern hair loss, but is a popular treatment for the condition nonetheless. It’s not yet very well studied, but may work well in combination with other therapies.
Natural Topicals: Jojoba, castor, rosemary, peppermint, and saw palmetto extract are just a few of the natural essential oils that have been marketed for hair regrowth. There are a few small studies showing that natural topicals may improve certain hair loss disorders.
Microneedling: Microneedling the scalp to treat hair loss is typically done biweekly. Microneedling evokes very low levels of inflammation which evoke a healing response from the body. Studies show microneedling can be successful when done alone, or when performed alongside other therapies. [3]https://www.tandfonline.com/doi/abs/10.1080/14764172.2017.1376094?journalCode=ijcl20

Semsarzadeh N, Khetarpal S. Platelet-Rich Plasma and Stem Cells for Hair Growth: A Review of the Literature. Aesthet Surg J. 2020 Mar 23;40(4):NP177-NP188.
Low-Level Laser Therapy: Low-level laser therapy (LLLT) is perhaps the most popular non-drug hair loss treatment and has FDA-clearance as a hair loss treatment for both men and women. The expensive and time consuming treatment does improve hair count for those with AGA.
Medications: Minoxidil and Finasteride are the only 2 FDA-approved medications for hair loss. Each treats AGA either orally or topically. While these medications have been proven effective to treat hair loss, they’re not for everyone. Both lead to side effects in some people, and generally require life-long use.
Botox: Botox is a neuromodulator which relaxes muscles and may also reduce certain inflammatory signaling proteins. Over the last decade, a few studies have been published measuring the hair-promoting effects of Botox on men with AGA.
Platelet-Rich-Plasma Therapy: Platelet-rich plasma therapy (PRP) is offered by thousands of dermatologists as a natural intervention for all types of hair loss. It is effective for androgenic alopecia and alopecia areata, but also expensive and ongoing injections are required to maintain results.
Stem Cell Therapy: Stem cell therapy is an expensive; relatively new therapy that is still under investigation. It’s also not a one-and-done treatment and requires multiple appointments. Early findings seem to suggest that 90% of subjects respond to stem cell therapy. And for AGA subjects, increases in hair count seem to hover around 20-30%.[4]https://pubmed.ncbi.nlm.nih.gov/31111157/
Effective treatment protocols often include some combination of the above. For example, studies suggest microneedling + minoxidil + finasteride, offers a response rate of 80-90% – with hair count increases ranging from 25-40% within 6-24 months.
Summary
As a man’s hairline matures, it will recede slightly from its juvenile position. This can be alarming, but it’s not always an early sign of male pattern baldness.
A receding hairline differs from a maturing hairline in that it may recede at a much faster pace, recede further back, and will recede more at the temples than in the center, resulting in an M-shaped hairline.
A receding hairline is characteristic of androgenic alopecia, but could be related to other types of hair loss too, especially if hair is thinning or balding in other areas.
Diagnosing a receding (vs maturing) hairline allows treatment to begin before baldness further progresses. Treatment options which have been proven effective include massaging, microneedling and medications. Efficacy improves when these methods are combined.
References[+]
References ↑1 https://www.researchgate.net/publication/256479799_Phenotype_of_Normal_Hairline_Maturation ↑2 https://link.springer.com/article/10.1007/s13555-019-0281-6 ↑3 https://www.tandfonline.com/doi/abs/10.1080/14764172.2017.1376094?journalCode=ijcl20 ↑4 https://pubmed.ncbi.nlm.nih.gov/31111157/ For men with pattern hair loss who want to combat pattern hair loss, the conflicting advice online can be overwhelming, particularly when it comes to finding the best DHT blockers.
After performing a quick Google search on the topic of DHT blockers, one might navigate to this Healthline article. The piece mentions dietary solutions like coconut oil, onions, turmeric, pumpkin seeds, and edamame.
Numerous extracts are mentioned as well, including green tea, saw palmetto, reishi mushroom, EGCG, propacil, and zinc.
There are also mentions of pharmaceuticals: finasteride, spironolactone, fluridil, ketoconazole, and dutasteride.
What’s effective? What’s dangerous? Could some DHT blockers actually make hair loss worse?
It’s time to navigate to the facts, not fiction, about DHT blockers. And determine which ones work and which ones don’t. This article outlines 6 DHT blockers, ranked from worst to best.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
But first, what is DHT?
DHT is short for dihydrotestosterone, which is a hormone made from testosterone. It’s also the main hormone implicated in pattern hair loss, one of the world’s most common hair loss disorders.
This article is not going to dive into the nuances of the DHT-pattern hair loss connection. That’s for a later article.
For now, readers should note that studies have determined:
- DHT is elevated in balding scalps [1]https://www.jdsjournal.com/article/S0923-1811(03)00249-4/fulltext
- Men who can’t produce DHT never go bald [2]https://www.amjmed.com/article/0002-9343(77)90313-8/pdf
- Human hair follicle dermal papillae cell clusters undergo cell death and miniaturization when exposed to DHT [3]https://www.karger.com/Article/Abstract/95251
- By reducing DHT levels in the scalp, many men can stop the progression of hair follicle miniaturization, and even regrow hair.[4]https://www.jaad.org/article/S0190-9622(98)70007-6/fulltext
Needless to say, if men want to fight pattern hair loss, they should consider lowering DHT. But herein lies the problem: DHT isn’t just a hormone linked to hair loss; it’s also a hormone that is critical for male development.
Moreover, in adulthood, DHT seems to be protective against high estrogen levels. As such, men who lower their DHT levels will sometimes report side effects, including weak erections, brain fog, and even gynecomastia – the growth of male breast tissue.
That’s why, when picking a DHT blocker, one must weigh power against safety. In other words, for any DHT reducer, hair density tends to increase in tandem with a heightened risk of side effects.
So, for this article, the six DHT reducers mentioned below are ordered from the lowest clinical efficacy and highest safety profile to the highest clinical efficacy and lowest safety profile.
1 – Saw Palmetto

Saw palmetto, a palm plant grown in the Southeastern U.S. is one of the most popular herbal DHT reducers, and not without reason. In one clinical study lasting two years, saw palmetto was shown to stop pattern hair loss in 90% of men taking the supplement.[5]https://journals.sagepub.com/doi/pdf/10.1177/039463201202500435 Other studies have shown a bit of regrowth when combining saw palmetto as a supplement and a topical.[6]https://www.karger.com/Article/FullText/509905
Based on Perfect Hair Health member results, saw palmetto, by itself, isn’t really that effective as a standalone treatment. But it’s better than nothing, and overall, studies show that the supplement is relatively safe – even over five-year time horizons.
For example, a meta-analysis examined 14 randomized, placebo-controlled studies that had reported adverse events, and found that saw palmetto’s risk of side effects was small, comparable to placebo groups. When events did occur, they were mainly upset stomachs or headaches experienced after taking the supplement on an empty stomach.[7]https://link.springer.com/article/10.2165%2F00002018-200932080-00003 Better yet, another study saw no concerning changes to bloodwork… with the majority of side effects reported in the placebo group – or in other words, people who weren’t even taking saw palmetto.[8]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2518869/ Lastly, out of thousands of participants taking saw palmetto, only a small handful have ever reported reductions in libido. This suggests that the risk of sexual side effects is much less than 1%.
Taken together, this puts saw palmetto first on our list of DHT reducers for men. It has relatively low efficacy, but a high safety profile – and it still does something. In other words, it appears very safe and might help to slow down or stop pattern hair loss. But don’t expect any miracles.
Keep the following tips in mind when taking saw palmetto:
- Take 320mg daily. According to the evidence, effective dosages for hair loss seem to range from 200mg – 320mg daily, depending on the extraction method.
- Split dosages. The volatile acids inside saw palmetto have short half-lives. So, it’s probably best to split up that 320mg daily dosage to half in the morning, half at night.
- Combine with ingredients to enhance absorption and efficacy. Specifically, beta-sitosterol, lecithin, inositol, phosphatidylcholine, and perhaps even niacin and biotin.
These recommendations just scratch the surface, especially in terms of which saw palmetto brands to avoid. But that’s for a later article.
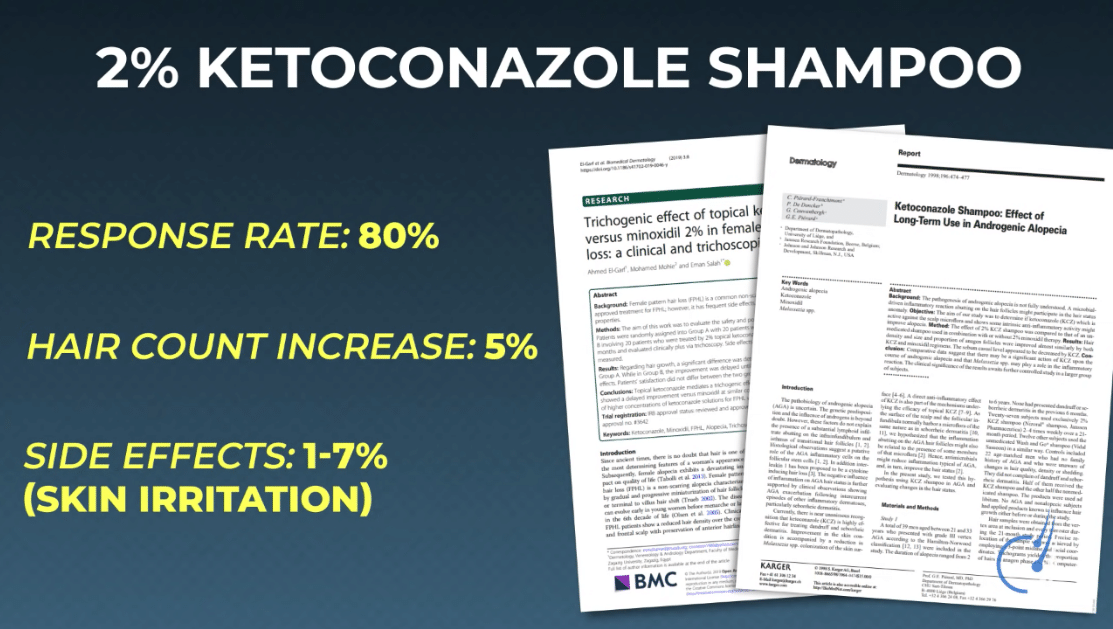
2 – Ketoconazole Shampoo
Ketoconazole is an anti-fungal medication. It’s used to treat skin conditions like dandruff, seborrheic dermatitis, and even jock itch. When formulated as a shampoo, there’s some evidence that it can improve hair counts, increase hair diameters, and potentially even lower scalp DHT levels in men – all without impacting hormone levels elsewhere in the body.
In fact, studies show that 2% ketoconazole, when used properly, boasts an 80% response rate with an average hair density increase of around 5%. Again, that’s no miracle, but with just 1-7% of people reporting side effects ranging from scalp itchiness to scalp dryness, ketoconazole can be considered a low cost, low effort, and moderately effective hair loss intervention.

Two quick notes for those who want to try ketoconazole:
- Get the 2% formulation. The 1% variety is available in supermarkets and drug stores, yet this dilution isn’t clinically effective at fighting hair loss. The 2% version is recommended. The product can be purchased without a prescription at NizoralShop.com.
- Use as directed. In most cases, that’s 2-4 times weekly, with a scalp contact time of 5-10 minutes. Failure to do this might result in wasted money and negligible results.
3 – Herbal DHT Reducers

Saw palmetto isn’t the only natural DHT reducer out there. There are studies showing that in cell cultures, other substances and herbal extracts can inhibit 5-alpha reductase, the enzyme that converts free testosterone into DHT, and in doing so, potentially lower DHT in humans.
Herbal DHT reducers include:
- Astaxanthin
- Azelaic acid
- Reishi mushroom extract
- Lycopene
- Green tea extract
- Beta-sitosterol
- Alpha-linolenic acid
- Zinc
- Curcumin
- Pumpkin seed oil
And the list goes on.
If we combine these all together, can we reduce more DHT than saw palmetto alone and see increased hair growth?
The logic is understandable. However, in biology, taking more of something doesn’t always equate to greater improvements – especially when taking things that all target the same pathway for DHT reduction: 5 alpha-reductase.
For instance, in one study, taking 3x the daily dose of saw palmetto for one year did not lead to 3x better improvements to an enlarged prostate; It led to the same improvements as a standard 320 mg dose.[9]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3326341/
Similarly, another study showed that mega-dosing saw palmetto and astaxanthin did not reduce blood levels of DHT any better than a small amount of saw palmetto and astaxanthin.[10]https://jissn.biomedcentral.com/articles/10.1186/s12970-014-0043-x And with this information in mind, when looking at clinical data on supplements like Nutrafol – which combines many natural potential DHT reducers into one pill – the hair regrowth isn’t really any more impressive than what we expect from a typical dose of saw palmetto alone.
Which begs the question: why mention the combination herbal extracts above both saw palmetto and ketoconazole?
There’s not a good answer.
All three of these options are similar in efficacy. But for these herbal combinations, where they differ probably isn’t efficacy; it’s safety.
There are very few long-term studies evaluating the safety profiles of herbal extracts for blocking DHT, particularly at the mega-dosages featured in best-selling DHT blockers on Amazon.
Adding in all these extra natural DHT-reducing herbs might have some effect, but one must be very selective in going about it. And those diminutive hair gains might not be worth the massively higher costs or the safety risks versus just taking saw palmetto alone.
Now on to pharmaceutical territory.
4 – Topical Finasteride

For men, finasteride is considered the gold standard treatment for pattern hair loss. Studies show that it can stop pattern hair loss in 80-90% of men, increase hair counts by 10%, and thicken miniaturizing hair – which all in, often equates to 20-30% improvements in hair density.[11]https://www.sciencedirect.com/science/article/pii/S0022202X15529357 The drug does this by inhibiting an enzyme called type II 5 alpha-reductase, thereby lowering DHT levels by 60-70%.
The problem is that oral finasteride reduces DHT everywhere, and not just on the scalp. In other words, it’s a systemic DHT reducer. And it’s this systemic lowering of DHT that some people use as a surrogate to predict a risk of side effects.
So people often ask: what if we could just localize finasteride’s effects to only the scalp? Well, that’s what topical finasteride attempts to do. It formulates oral finasteride as a topical – the medication can be applied directly to the scalp and, hopefully, reduce its risks of going systemic.
So, does this actually work?
Yes, to a degree.
Studies suggest that topical finasteride, at a 1% formulation, is “non-inferior” (or equivalent) to 1mg oral finasteride tablets in terms of hair regrowth.[12]https://pubmed.ncbi.nlm.nih.gov/19172031/ But concentrations as low as 0.005% have been shown to improve hair growth in men with pattern hair loss.[13]https://www.tandfonline.com/doi/abs/10.3109/09546639709160517 So, what about the systemic absorption part? Well, this is where things get complicated…

GF Mazzarella, GF Loconsole, GA Cammisa, GM Mastrolonardo & Ga Vena (1997) Topical finasteride in the treatment of androgenic alopecia. Preliminary evaluations after a 16-month therapy course, Journal of Dermatological Treatment, 8:3, 189-192
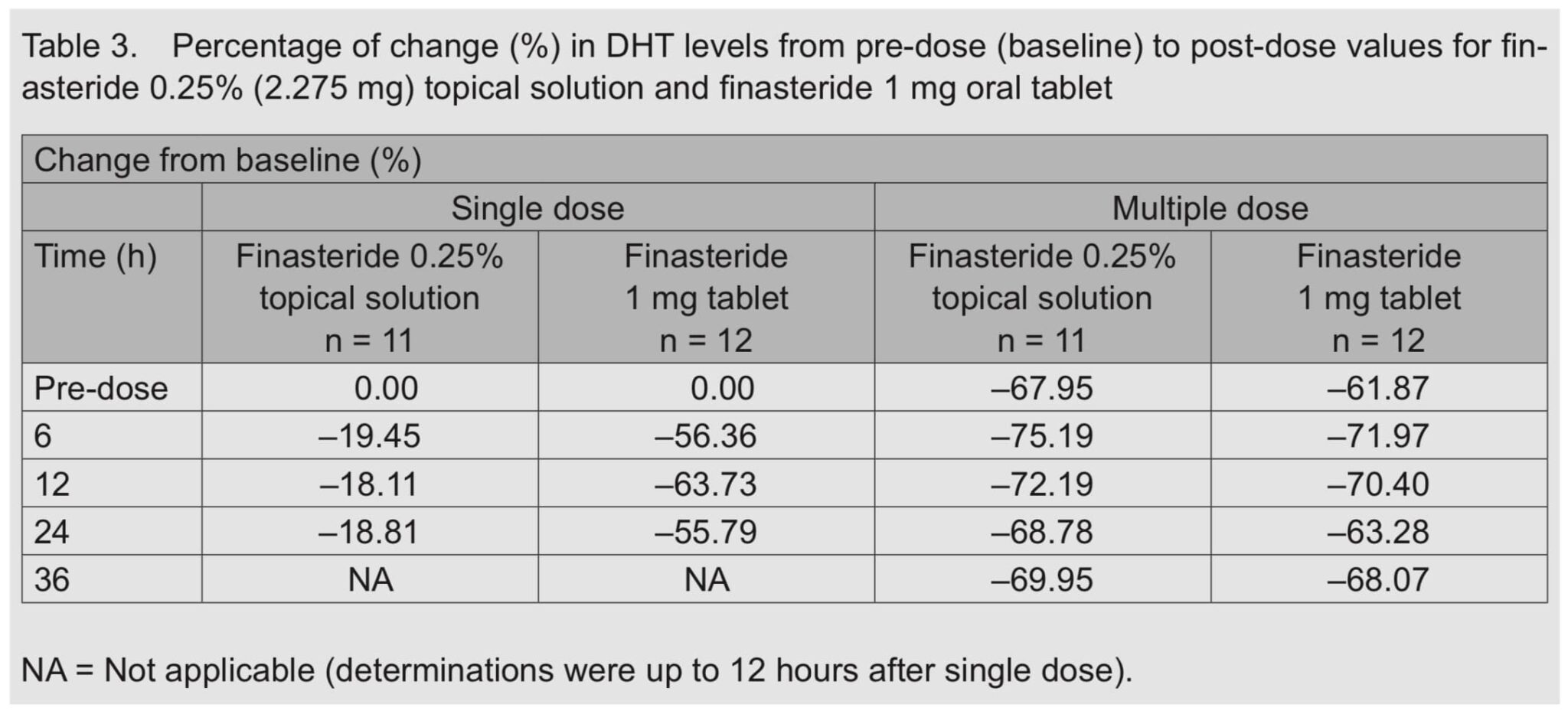
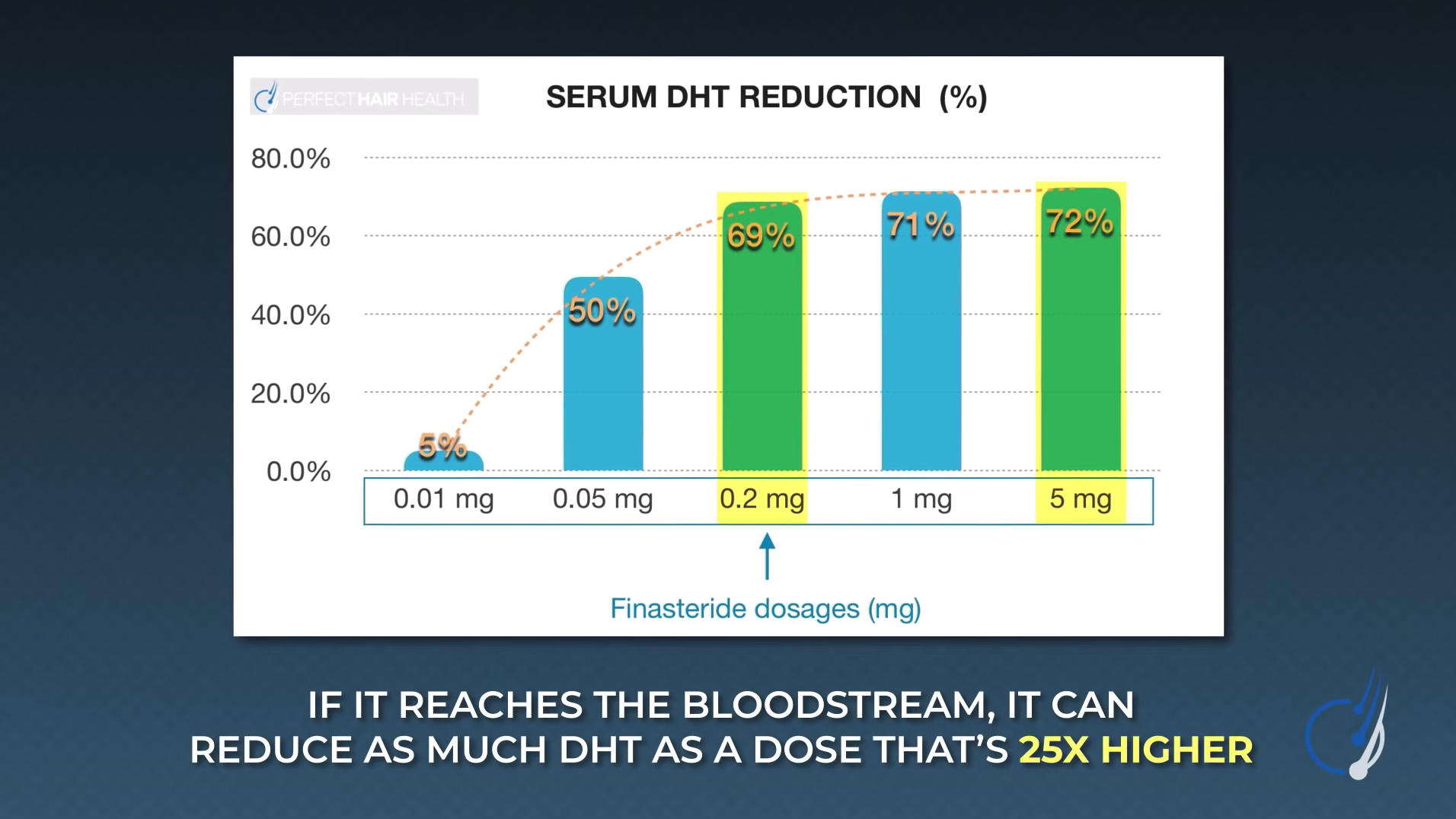
There are studies showing that topical finasteride at a 0.25% dilution can reduce scalp DHT by 24-75%, depending on the amount applied. And while larger applications reduce more scalp DHT, they also appear to have systemic effects on DHT. [14]https://pubmed.ncbi.nlm.nih.gov/25074865/

This is because finasteride has a dose-dependent logarithmic effect on DHT reduction. In other words, if just a tiny amount of the drug reaches the bloodstream, it can reduce just as much DHT as a dose that is 25 times higher.
That’s important, because depending on the percent of topical finasteride, the body may be exposed to more of the drug than if taking 1mg of finasteride orally. For example, applying 1mL per day of a 0.25% topical finasteride solution translates to the application of roughly 2.5mg of finasteride to the scalp.
That’s 2.5-fold more finasteride exposure than a daily 1mg oral dose. And again, just 0.2mg of that dose needs to enter the bloodstream to produce the same DHT-reducing effects everywhere as the oral medication.
For these reasons, many clinicians estimate that topical finasteride is roughly as effective as oral finasteride, but that it only reduces the risk of side effects by 30-50% compared to oral finasteride. There might be ways to lower this risk even further by changing the delivery vehicle of topical finasteride; however, it’s best to address that in a separate article.
5 – Oral Finasteride

Compared to topical finasteride, oral finasteride confers unique advantages: it’s easier to use, it affects all hair follicles rather than just the follicles where the topical is applied, and it’s supported by better clinical data. Across hundreds of studies and tens of thousands of participants, finasteride has demonstrated consistently impressive hair growth outcomes and a decent safety profile.
Better yet, the drug seems much more effective than its herbal alternatives. In one head-to-head study, it demonstrated significantly better hair growth outcomes over two years with finasteride versus saw palmetto. [15]https://pubmed.ncbi.nlm.nih.gov/23298508/ It’s this data that firmly cements finasteride as one of the more powerful DHT reducers on our list.
6 – Oral Dutasteride

Those looking for an even greater DHT-reducing effect may want to consider oral dutasteride. This medication is an inhibitor of type I and type II 5-alpha reductase and it’s prescribed off-label for those looking to treat pattern hair loss at the highest level.
Depending on the dose, dutasteride can reduce DHT levels by up to 95%. This makes it significantly more powerful than finasteride, with short-term studies showing that 0.5 to 2.5 mg of dutasteride regrows hair 2-5 times faster than finasteride, and even leads to more robust increases in hair counts.

Lee WS, Ro BI, Hong SP et al. A new classification of pattern hair loss that is universal for men and women: basic and specific (BASP) classification. J Am Acad Dermatol 2007; 57: 37–46.
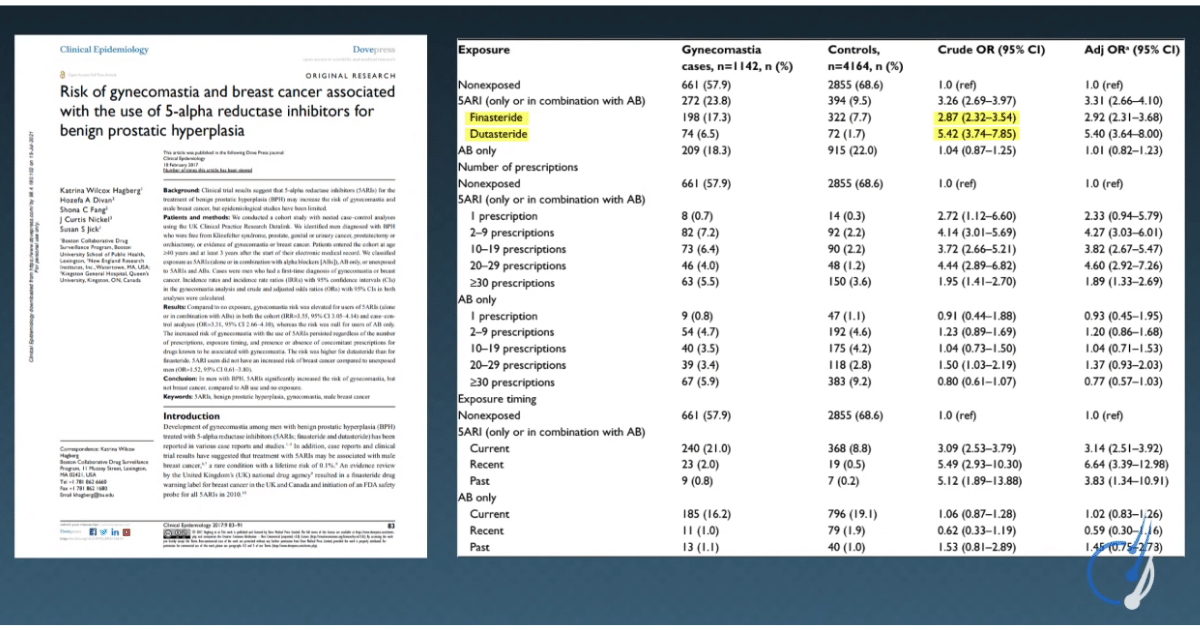
Interestingly, this meta-analysis showed that when used as a hair loss treatment, dutasteride’s risk of side effects was actually comparable to finasteride, despite lowering more DHT.[16]https://www.dovepress.com/getfile.php?fileID=48173 However, the risk of certain side effects – like gynecomastia – increases with dutasteride versus finasteride.
Zhou, Z., Song, S., Gao, Z., Wu, J., Ma, J., & Cui, Y. (2019). The efficacy and safety of dutasteride compared with finasteride in treating men with androgenetic alopecia: a systematic review and meta-analysis. Clinical interventions in aging, 14, 399–406. https://doi.org/10.2147/CIA.S192435
So, while it’s likely more effective, it also may come with a slightly higher risk of side effects.
Before concluding, there are a few more things worth mentioning.
First, the only scientifically honest way to compare effectiveness and side effect profiles across DHT reducers is to test them within the same study. This is because patient populations, hair counting methodologies, and side effect questionnaires all vary across hair loss studies. That makes crude comparisons across two random studies really hard to do.
Since a single study comparing all of these DHT reducers does not yet exist, we can’t claim that this analysis is perfect.
Second, it’s important to keep in mind that in the absolutes, every DHT mentioned here is relatively safe. Finasteride and dutasteride are taken by millions of men every day – most of whom report no issues.
Hair loss sufferers shouldn’t let these relative comparisons scare them away from trying these pharmaceuticals. If someone cannot tolerate a drug, they can always hop off and try something else.
Third, a few DHT reducers were left out: topical dutasteride, RU58841, procapil, and others. This was intentional: these treatments rely too much on experimental data and unpublished clinical trials to accurately gauge efficacy and safety profiles.
These topics will be covered, at length, in future articles.
References[+]
References ↑1 https://www.jdsjournal.com/article/S0923-1811(03)00249-4/fulltext ↑2 https://www.amjmed.com/article/0002-9343(77)90313-8/pdf ↑3 https://www.karger.com/Article/Abstract/95251 ↑4 https://www.jaad.org/article/S0190-9622(98)70007-6/fulltext ↑5 https://journals.sagepub.com/doi/pdf/10.1177/039463201202500435 ↑6 https://www.karger.com/Article/FullText/509905 ↑7 https://link.springer.com/article/10.2165%2F00002018-200932080-00003 ↑8 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2518869/ ↑9 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3326341/ ↑10 https://jissn.biomedcentral.com/articles/10.1186/s12970-014-0043-x ↑11 https://www.sciencedirect.com/science/article/pii/S0022202X15529357 ↑12 https://pubmed.ncbi.nlm.nih.gov/19172031/ ↑13 https://www.tandfonline.com/doi/abs/10.3109/09546639709160517 ↑14 https://pubmed.ncbi.nlm.nih.gov/25074865/ ↑15 https://pubmed.ncbi.nlm.nih.gov/23298508/ ↑16 https://www.dovepress.com/getfile.php?fileID=48173 Viviscal® is one of the most popular hair loss supplements in the world. What sets it apart from its competition? Clinical research. Viviscal has conducted 12+ human studies on its supplement line, all showing that its proprietary blend of marine extracts can improve hair growth in men and women, and with a variety of types of hair loss.
So, does this make Viviscal the go-to supplement for anyone interested in tackling hair loss naturally?
Maybe, maybe not. If there’s anything we’ve learned from other product reviews, it’s that clinical studies on a supplement rarely tell the full story.
More often than not, these studies can be designed to manufacture biased results; those results can create a false sense of hope; that hope can be transmitted to millions through advertising; that advertising won’t usually convey that the results from those clinical studies aren’t applicable to most of the people watching that ad.
That’s why it’s important to look beyond the marketing of a supplement to really see what that data says.
Before purchasing hair loss products, it’s important to examine the company’s products, marketing, and studies to find out whether this supplement is worth the investment.
Here’s the Perfect Hair Health approach to product reviews:
- Buy the product. Send the supplement to a third-party laboratory to test for impurities, heavy metals, and pathogenic microbes.
- Examine the ingredients. Compare the company’s rationale for these ingredients versus what the totality of research says.
- Read all published clinical studies. Evaluate their methodologies and results, identify areas of bias, and determine if these results align with the claims made in marketing.
The findings are surprising. The hope is that people fighting hair loss can make better decisions as to whether Viviscal is right for them.
Key takeaways
- Product: Supplement
- Effort: Low (once- or twice-daily supplement)
- Expectations: Clinical trials suggest improvement in as little as 3 months, however, Viviscal™ recommends at least 6 months of supplementation to see results.
- Response rate*: According to the clinical trials:
- Male pattern hair loss: 85%
- Women with temporary hair loss from stress, poor diet, or menstruation: 75-100%
- Autoimmune hair loss: 30-90%
- Regrowth rate*: According to the clinical trials:
- Male pattern hair loss: 0% (i.e., stabilization)
- Women with temporary hair loss from stress, poor diet, or menstruation: 10% to 32%
- Autoimmune hair loss: 5% to 85%. (Autoimmune hair loss is known to spontaneously fully reverse, so it’s hard to delineate how much of this is due to Viviscal versus the mysteries of biology.)
- Cost: $39.99/month
- Problems: Results contingent upon lifelong use; some biased methodologies in clinical research; hundreds of negative reviews online – with most seemingly complaining the product wasn’t effective after 3 months of use (despite one study showing a minimum 32% average increase in hair count after 3 months); for a product sold to millions of people, it’s nearly impossible to find clearcut before-and-after photos submitted by their customers.
All-Natural Hair Supplement
The top natural ingredients for hair growth, all in one supplement.
Take the next step in your hair growth journey with a world-class natural supplement. Ingredients, doses, & concentrations built by science.

*These response and regrowth rates likely do not reflect reality. Response rates and regrowth rates were calculated using Viviscal’s clinical studies. However, many of these studies came with biased methodologies. Normally, adjustments can be made for these biases in estimates. But the difference between clinical research versus customer reviews was so vast in this case, it’s hard finding a middle ground. The fact that so few before-after photos exist in Viviscal’s customer testimonials – after 25+ years of business – should be a telling sign to consumers.
Ordering experience
- Checkout: 7/10: One-page checkout made the process relatively easy, but coupon popups and the absence of an autofill or PayPal option made form filling a bit more cumbersome than other checkout pages.
- Fulfillment: 9/10: An email receipt was generated instantly upon receipt of the order, and later to announce that the product had shipped.
- Arrival: 8/10: Arrived within 5 days and without issues.
Highlights
Compared to other hair loss supplements, Viviscal has its perks.
- The company has conducted 12 clinical trials testing Viviscal™ in men and women with many types of hair loss. All of them show positive results.
- Viviscal’s supplements don’t contain a lot of extraneous ingredients. This is a positive; many hair loss supplements are chock-full of dozens of vitamins and minerals – many of which are harmful if over-consumed.
- The supplement contains ingredients that may address some underlying causes of hair loss.
- The supplement passed our product purities testing for heavy metals, pollutants, and pathogenic microbes. In other words, what you see on the label is what you get.
Having said that, when looking more closely at Viviscal’s clinical trials, marketing efforts, and product ingredients, a lot of issues emerged. Here are just a few.
- For a company that has conducted 12 clinical studies and been in business for 25+ years, there are almost no before-after photos from customers demonstrating clear, discernible improvements.
- Most of Viviscal’s studies are either unpublished or poorly designed.
- At least 33% of their studies were never published in a scholarly journal.
- Of the studies that were published, there are glaring typos and selection biases that make the results less impressive than perceived at first glance. For example, many of Viviscal’s studies use participants who are losing their hair temporarily as a result of stress, bad diets, or menstruation-related nutrient deficiencies. These participants are most likely to see hair regrowth from a nutritional supplement and would’ve also likely seen just as impressive hair growth with better stress management and nutritional planning. Moreover, in the developed world, this hair loss from these causes is relatively less common – and it’s also avoidable with simple dietary and lifestyle adjustments. Therefore, it’s disingenuous (and perhaps deceptive) to market the results of these participants to the general population of hair loss sufferers.
- Viviscal’s genesis story cannot be verified. Viviscal says that their product was developed after a Scandinavian professor observed that the Inuit peoples’ healthy, long-lasting hair was the result of their diets rich in marine foods. This professor allegedly was able to isolate the compounds responsible for the Inuit’s healthy hair, from which Viviscal was born.
However, none of this is recorded in any of the clinical studies published by Viviscal. Moreover, Viviscal has not responded to our emails requesting the name of the professor. Rather, research actually points to Viviscal being developed from an earlier product targeting to improve aging skin in women.
A full analysis of Viviscal’s company (and supplements) can be found below.
What is Viviscal®?
Viviscal™ is a hair loss supplement endorsed by hundreds of doctors in the U.S. It’s supported by 12 clinical trials and 25 years of research. It goes without saying that Viviscal is the most heavily researched hair loss supplement out there.
Viviscal® Man

What makes Viviscal unique?
There’s one “ingredient” that makes Viviscal unique from all other hair loss supplements: its proprietary blend of shark cartilage and oyster extract powder, known as their AminoMar™ Marine Complex.
According to the company’s FAQ’s:
“The groundbreaking, clinically proven marine complex available exclusively in Viviscal supplements. Derived from key marine protein molecules combined with a blend of Horsetail (Stem) Extract and naturally occurring Silica, it provides essential nutrients needed to promote existing hair growth from within.”
In fact, this proprietary blend (AminoMar™) has been the focus of every clinical study on Viviscal. Its clinical effectiveness is what makes Viviscal so enticing to consumers looking for a natural solution to thinning hair.
Product Offerings
Viviscal™ offers two product lines based on gender.
For women, they offer a Viviscal™ supplement as well as a shampoo, conditioner, and topical. For men, they offer a Viviscal™ supplement (with slightly different ingredients) and a shampoo.
This review focuses exclusively on Viviscal’s supplements. After all, the supplements are the products that have been clinically studied.
Viviscal Hair Growth Supplement – Ingredients
Both Viviscal™ for Women and Viviscal™ for Men contain:
- Vitamin C
- Calcium
- Zinc
- Horsetail extract
- AminoMar™ (Viviscal™’s properietary blend of shark cartilage and oyster extract power).
However, Viviscal™ for Women also contains niacin, iron, biotin, and millet seed whereas Viviscal™ for Men contains flaxseed. Here’s the full list of ingredients.
Viviscal Woman vs. Viviscal Man: product ingredients
Viviscal™ for Women Viviscal™ for Men Vitamin C Vitamin C Calcium Calcium Zinc Zinc AminoMar™ AminoMar™ Niacin Flaxseed Iron Biotin Millet seed There are also slight differences in the number of ingredients in each of the male and female supplements. Here are the labels.
Viviscal™ for Women

Viviscal™ for Men
How might these ingredients improve hair loss?
Viviscal’s clinical studies focus on their AminoMar™ proprietary blend. But their auxiliary ingredients – like flaxseed, biotin, and iron – may also help with hair growth for certain people, and in different ways.
Below is a list of Viviscal’s key ingredients and the company’s rationale for their inclusion. The team found some of Viviscal’s claims to be nondescript. These claims were compared against what the actual research says.
AminoMar™
What Viviscal® says
“The groundbreaking, clinically proven marine complex available exclusively in Viviscal supplements. Derived from key marine protein molecules combined with a blend of Horsetail (Stem) Extract and naturally occurring Silica, it provides essential nutrients needed to promote existing hair growth from within.”
What the research says
What’s Viviscal’s original rationale for how AminoMar™ might work?
After all, their website just says that this marine extract, “promote[s] existing hair growth from within.” That’s a bit vague.
Viviscal’s first study (1993) referenced three earlier studies that tested a similar marine extract.[1]https://pubmed.ncbi.nlm.nih.gov/1286738/ These studies focused on skin health, not hair health. But interestingly, they found that women using this marine extract also reported improvements to their brittle hair, at least in a survey that asked them about brittle hair.
But when we read these three studies, none of them explained or speculated about the ways in which the marine extract worked, either. To quote from the earliest study we could find:
“Although the mode of action of Imedeen® [the marine extract] is unclear, the results of the present study indicate that there are certain agents in the extract which seem to have a repairing effect on degenerated elastic and collagen tissue in the dermis.”[2]https://www.ncbi.nlm.nih.gov/pubmed/1864451
Again, this is very vague, and very unusual – especially for a scientific journal. But it seems that more recent research papers (i.e., those after 2010) have tried to offer better explanations.
For instance, this 2019 review attributes Viviscal’s hair-promoting effects to the fatty acids, polysaccharides, and cartilage proteins inside the marine proprietary blend.[3]https://www.karger.com/Article/FullText/492035
Specifically, the reviewers discuss a polysaccharide (i.e., sugar) called glycosaminoglycan. These sugars are found near the “powerhouse” of a hair follicle: the dermal papilla. This is near the hair follicle base, and it’s where a hair connects to its blood supply.
A hair follicle: note where the blood supply connects to its dermal papilla

When a hair follicle is growing, glycosaminoglycan levels surrounding the dermal papilla increase.[4]https://www.ncbi.nlm.nih.gov/pubmed/1610689 And when a hair sheds, glycosaminoglycan levels in these regions decrease. Thus, one hypothesis is that AminoMar™ increases glycosaminoglycan levels surrounding our hair follicles, and in doing so, helps a hair grow longer and shed less frequently.
There might be some truth to this, too. In clinical studies on AminoMar™, the extract helps elongate our hair growth cycle – shifting more hairs into their growth stages, and fewer hairs into their shedding stages (more on this later).
Flaxseed (Viviscal® for Men)
What Viviscal® says
According to Viviscal, flaxseed extract is included in their male supplement because it contains vitamin E and omega 3 fatty acids, two substances that they say promote hair health.
“Vitamin E helps to nourish your roots and scalp and is found in Flaxseed. Flaxseed is one of the best foods to eat to combat hair loss, or to give your hair an extra boost of nutrients. Omega-3 fatty acid is in this amazing little, yet powerful, nutrient, helping to prevent your hair from drying out and losing its shine.”
What the research says
There is evidence that vitamin E supplementation might improve hair growth. And vitamin E is found inside flaxseed extract. According to NutritionData, one tablespoon of flaxseed oil (i.e., 14 grams) contains 2.4 milligrams of vitamin E, or 12% of our recommended daily intake.[5]https://nutritiondata.self.com/facts/nut-and-seed-products/3163/2
Unfortunately, Viviscal supplements include just 0.05 grams of flaxseed extract. Adjusting for the size difference, this implies that Viviscal has only a fraction of 1% of our recommended vitamin E intake. Given that the studies on vitamin E for hair growth used supplements containing 667% our recommended daily intake, the amount in Viviscal is negligible, and likely has zero effect on our hair.[6]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3819075/
As far as omega 3 fatty acids are concerned, this 2015 study showed that omega 3 supplementation (alongside antioxidants like vitamin E) increased hair counts by ~ 5% in women with general thinning. But again, the amount of omega 3 + vitamin E in that study is dozens of times higher than the amount found in Viviscal, so results really cannot be compared.[7]https://onlinelibrary.wiley.com/doi/abs/10.1111/jocd.12127
The bottom line: in some cases, vitamin E and omega 3 from flaxseed extract might improve hair loss, but probably not in the negligible amounts found in a Viviscal supplement.
Biotin (Viviscal® for Women)
What Viviscal® says
“Also known as Vitamin H, it is a water-soluble Vitamin B complex (Vitamin B7) that helps the body to metabolize carbohydrates, fats and amino acids, which are the building blocks of protein and thus essential in the formation of the hair structure.”
What the research says
Low-grade biotin deficiencies aren’t uncommon in the U.S. In fact, during pregnancy, about 50% of women will develop what’s known as a marginal biotin deficiency. This is when biotin levels drop slightly below what’s considered normal.
Having said that, marginal biotin deficiencies aren’t linked to hair loss. Rather, biotin-related hair loss is only seen in what’s known as a “profound deficiency”. These occur as a result of genetic mutations, chronic alcoholism, chronic antibiotic abuse, and/or a diet that is completely devoid of biotin for years.
So, just how common are partial or profound biotin deficiencies in the developed world?
Incredibly rare. According to worldwide neonatal screening surveys:
“…The incidence of profound biotin deficiency is one in 112271, and the incidence of partial deficiency is one in 129282.”[8]https://www.ncbi.nlm.nih.gov/books/NBK547751/
In other words, severe biotin deficiencies occurs in less than .001% of people. And again, only severe biotin deficiencies are causally linked to hair loss.
This begs the question: how useful is it to supplement with biotin for hair?
According to some research groups, not very useful at all. In fact, one investigation team has recommended to “reject the practice of supplementing with high doses of biotin for treating hair loss” unless there is a lab-confirmed deficiency, and that the deficiency is severe enough to be of concern.[9]https://perfecthairhealth.com/nutrient-deficiency-hair-loss/#biotin
Thus, biotin supplementation (even at the 400% recommended daily intake found in Viviscal®) probably won’t be that helpful, at least for the overwhelming majority of people taking the supplement.
Vitamin C and Iron (iron in Viviscal® for Women only)
What Viviscal® says
“[Vitamin C:] A powerful antioxidant that helps to absorb more Iron into the blood, which in turn promotes hair growth. Vitamin C in Viviscal supplements is sourced from the acerola cherry.”
“[Iron:] An essential mineral that has several important roles in the body, Iron helps to make red blood cells, which carry oxygen around to cells in the body, including hair follicles. Thinning hair can be one of the visible symptoms of anemia (Iron deficiency).”
What the research says
Viviscal’s rationale for including both vitamin C and iron center around an effort to enhance iron levels in their customers.
Vitamin C helps to increase iron absorption. This vitamin is included in both Viviscal® Man and Viviscal® Woman. However, supplemental iron is only found inside the female formulation of Viviscal. And this is because, unlike men, women are at a much higher risk of developing low iron (i.e., anemia) as a result of iron loss from menstruation.
There’s some evidence to support these positions. For instance, studies have linked mild-to-severe iron deficiencies in women to a variety of hair loss disorders – ranging from female pattern hair loss to telogen effluvium.[10]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3678013/ [11]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6385517/ And while there’s still debate over how effective (and how high) iron levels need to raise in order to improve hair loss, it goes without saying that a lot of women have experienced great improvements to hair growth by restoring their iron to adequate levels.
Unfortunately, supplemental iron also harbors some risks. This is because iron is oxidative – meaning that in excess, its presence can create oxidative stress, also known as inflammation.
In fact, evidence indicates that vitamin C and iron salts (like the ferrous fumarate used in Viviscal™ for Women) may have a dangerous and synergistic interaction. Specifically, research suggests that vitamin C can “propel” the oxidative action of iron, meaning that vitamin C may enhance the inflammation that excess iron causes.[12]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC340385/ This suggests that in cases of longterm, excessive iron + vitamin C supplementation, we’re more likely to experience problems like ulcerations, inflammation, exacerbation of chronic disease, and, potentially even cancer.
Customer testimonials
It’s one thing to look at a supplement’s ingredients, then build a case for whether the research shows these ingredients will or won’t help with hair loss. It’s another thing to measure whether all of these ingredients – when taken together – actually improve hair growth in men and women with thinning hair.
To do this, one can analyze two pieces of evidence:
- Customer testimonials. Viviscal has been in business for 25+ years. They claim to average one product sale every single minute of the day. That equates to millions of customers, and (hopefully) thousands of before-after photos.
- Clinical research. Viviscal is the most heavily studied hair loss supplement in the world. If Viviscal’s clinical research proves as promising as claimed in their marketing, then customer testimonials should be validated in the data: increases to hair counts, hair diameters, etc.
This section focuses on that first lever: customer testimonials and before-after photos.
12 clinical studies and 25+ years of business. But where are the before-and-after photos?
When it comes to hair loss, before-and-after photosets are probably the most powerful tool used to validate the effectiveness of any approach. Yes, clinical trials are great (and often required). As will be discussed later, clinical research is only valid when a study is properly designed. Thus, if a product truly works, one can expect to see a combination of both clinical evidence + customer testimonials.
On review websites, customer reviews of Viviscal are mostly negative. However, these reviews were left out of this product review. Why? Because reviews can be written by anyone – including competitors or Viviscal employees. And given the inability for review websites to verify and rank the validity of any review, the focus remained on hard evidence: that of which is presented by Viviscal on their own website.
So, as one of the best-selling hair loss supplements on the planet, how does Viviscal do in the customer success department?
Puzzlingly, Viviscal has almost no customer before-and-after photos (at least on their website).
And of the ones that are featured, it’s as if they’re designed to be intentionally misleading. These can be segmented segment this by the photos featured on Viviscal’s (1) main website, (2) female site, and (3) male site.
The photos featured on Viviscal® appear to have had their backgrounds trimmed and/or recolored. This masks any lighting differences across photos; it makes fair photo comparisons impossible.
The success featured on Viviscal® Woman aren’t actually focused on hair; rather, they’re simply photos of women wearing different hairstyles before and after starting the supplement.
And the few customer photos featured on Viviscal® Man either face the same problems above or were taken from impossible-to-compare angles and lightings.
Why is this concerning?
Well, in their marketing, Viviscal claims that one packet of Viviscal is sold every single minute. This should equate to 10+ million customers over a 25-year period. And if the product were truly as effective as advertised, one would expect Viviscal to present significantly more before after-photos, and of significantly better quality.
For instance, let’s assume that Viviscal only has one million consistent customers (a fraction of what is suggested in their marketing). Now assume that just 0.1% of those customers (or one in 1,000) decide to take before-after photos, then share those photos with Viviscal. That leaves Viviscal with 1,000 before-after photos from which to share on their website.
For some reason, Viviscal seems to only have ~20 photosets total across men and women. And instead of high-quality photo comparisons, we’re left with misleading photosets.
What about before-after photos from Viviscal’s clinical studies?
It’s true that Viviscal’s clinical studies have higher-quality photosets, and that in some cases, these photosets demonstrate clear, discernible hair regrowth. But it’s also important to contextualize these photosets – because not all photos are from people with common hair loss types.
For men with androgenic alopecia (AGA) – the most common form of hair loss in adult men – the highest-quality before-after photoset available from a Viviscal study only showed stabilization after 180 days of use. In fact, this is the one advertised on their website.
For women, the highest-quality before-after photosets come from their website (here) and clinical studies [13]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3509882/
But these women only had temporary forms of hair loss due to stress, poor diet, and nutrient deficiencies due to menstruation. In other words, these before-after photos don’t represent what the average Viviscal customer should expect, because hair loss from these causes are lesser common, and likely do not represent the average customer of Viviscal.
Now for Viviscal’s clinical studies …
Clinical studies
When it comes to clinical studies on a hair loss supplement line, Viviscal® is the industry leader.
According to their marketing materials, Viviscal has conducted 12 clinical trials – more human studies on their product than any other hair loss supplement out there.
And even better, these clinical trials aren’t limited to just one population, or one type of hair loss. Of the 12 clinical trials, seven were conducted on women, two were done men with androgenic alopecia (AGA), and two were completed on men and women with autoimmune hair loss disorders like alopecia areata, alopecia totalis, and alopecia universalis.
In other words, they’ve not only got the most clinical studies, but they’ve also studied their supplement on the majority of types of hair loss out there. And amazingly, all of the studies have appeared to reap great results.
Viviscal’s clinical studies: summarized
Viviscal™’s Clinical Trials, Their Subjects, and the Results Study #1 (2014) Females with Self-Perceived Hair Thinning “• 32% increase in terminal hairs after 3 months • 39% decrease in hair shedding
• After 3 months there was significant self-perceived improvements in overall hair volume, scalp coverage and hair strength.”
Study #2 (2014) Females with Self-Perceived Hair Thinning • 57% increase in terminal hairs after 3 months • 80% increase in terminal hairs
• 12% increase in hair diameter after 6 months
• After 3 and 6 months there was a significant self-perceived improvement in overall hair volume, scalp coverage, hair and nail strength.
Study #3 (2014) Females with Subclinical Hair Thinning “• a 7.4% increase in hair diameter after 6 months • an 18% reduction in hair shedding after 3 months.”
Study #4 (2014) Females with Self-Perceived Hair Thinning • 94% in hair volume • 92% hair thickness
• 91% in nail growth rate and
• 92% in nail strength
After 6 months.
Study #5 (2012) Females with Self-Perceived Hair Thinning • 111% increase in terminal hairs after 3 months versus no change amongst the placebo subjects. • 125% increase in terminal hairs after 6 months versus no change amongst the placebo subjects.
• After 3 and 6 months there were significant self-perceived improvements in overall hair volume, thickness, and scalp coverage.
Study #6 (2011) African American Females with Self-Perceived Hair Thinning “Rapid changes in hair growth and appearance in as little as 2 months.” Study #7 (2010) Females with Self-Perceived Hair Thinning “After a 10 week period, there was an average 46% reduction in hair loss reported. 75% saw an increased thickness in the body of their hair and 75% saw an increase in overall hair volume.” Study #8 (1997) Men with AGA • 75.3% of patients observed a significant decrease in hair loss • 14.6% of patients showed partial regrowth
Study #9 (1996) Males and Females with Alopecia Areata, Alopecia Totalis, or Alopecia Universalis • 92% of areata group showed regrowth of permanent hair. After four months of treatment: • 83.3% of totalis group showed regrowth of permanent hair and
• 31.8% of universalis group showed regrowth of permanent hair after five months.
• Complete cure was observed in 14% of areata, 25% of totalis and 5% of universalis.
Study #10 (1994) Men with AGA “Hair loss stopped for 100% of subjects after two months treatment. 43% showed total regrowth, 23% showed three quarter regrowth, 13% showed half regrowth & 13% showed 30-50% regrowth.” Study #11 (1992) Men with AGA “100% of treated subjects reported that hair loss had stopped after 2 months of treatment. Mean increase in non-vellus hair of 38% was recorded in patients after 6 months treatment. 95% of subjects showed both clinical and histological cure.” Study #12 (1992) Males and Females with Alopecia Areata, Alopecia Totalis, or Alopecia Universalis “85% of subjects with Alopecia Areata were completely cured & 10% showed significant improvement. 25% of subjects with Alopecia Totalis were completely cured & 20% showed significant improvement.” At a glance, this body of clinical research seems to position Viviscal as the go-to supplement for anyone with thinning hair. But as the Perfect Health team learned from its investigation into Nutrafol, clinical trial results can be misleading.
For instance, studies can pick participants who most likely have nutrient deficiency-related hair loss, and are thereby most likely to see hair regrowth from taking any nutritional supplement (not just the brand being investigated. Studies can also use biased hair counting methodologies to make it appear as though a supplement regrows a ton of hair, even when the results don’t translate to visual improvements to hair density.
So, do Viviscal’s studies have any of these biases?
In many cases, yes.
Whether or not these biases invalidate the body of research of Viviscal remains to be seen. It would be unproductive to go through each Viviscal study and dissect every little problem. Doing this would turn this already-long product review into a full-fledged novel.
In focusing more on the larger issues across these studies, hair loss sufferers can decide for themselves whether these concerns are worrying enough to influence purchasing decisions.
Problem #1: at least 33% of Viviscal’s clinical trials were never published
It’s one thing to conduct a clinical trial, analyze the data, write the results into a manuscript, submit that manuscript to a journal, get it reviewed by experts, receive feedback, make revisions, resubmit, and then finally have your study accepted for publication in a scholarly journal.
It’s another thing to conduct a clinical trial, analyze the data, write the results into a manuscript, and then bypass peer review and, instead, just publish the results as part of your marketing materials.
According to Perfect Hair Health research, 33% of Viviscal’s clinical trials fall under that secondary category. Of the 12 studies listed on Viviscal’s website, our investigation showed that four studies (#4, #6, #7, and #12) never made it into a scholarly journal. In fact, 3 of those 4 studies were never even submitted for publication.
Why not publish the results of a clinical trial in a scholarly journal, especially if the results are positive?
This is actually more commonplace than most people realize. In fact, conducting a clinical trial and not publishing the results in a scholarly journal happens all the time – especially for companies studying (and selling) natural health products.
Just take the companies selling low-level laser therapy devices. Companies in that hair loss sector have a history of registering clinical trials containing biased hair counting methods (e.g.., grouping vellus + terminal hair counts). These companies never intend to submit their results to a scholarly journal. Rather, they conduct these studies so that when their great (manufactured) results come in, they can legally claim their devices can “increase hair thickness by over 200%”.
In these cases, the goal isn’t to prove that the clinical research is legitimate; the goal is to avoid getting sued over false claims.
As such, it’s not a priority for these companies to submit their clinical data for peer review. If they did, reviewers would likely find the flaws in the study design, and then reject the study for publication.
Therefore, the most common reason why a company won’t publish clinical results in a journal – at least when those results are favorable – is that they know that the study is biased, and that the paper won’t survive peer review. So, instead, these companies will just write up their results to look like a paper, and then use it as part of their marketing.
(Note: this is different from burying unfavorable clinical trial results – or in other words, never publicizing the findings. This is what Nutrafol is suspected of doing for one of the clinical trials that they completed, but never published.)
For Viviscal, favorable unpublished clinical trial results make up 33% of the studies advertised on their website.
Now, this isn’t the end of the world… because that still leaves 8+ studies that have gone through peer review, and have been published in journals.
So, how do these published trials stack up?
Well, these published studies also have issues. This leads to another problem.
Problem #2: of Viviscal’s published studies, most of them were published in low-ranking journals
Low-ranking journals, and why they should be avoided
If the four studies Viviscal never published were ignored in favor of the eight studies that survived peer review, there would still be a great deal of noise that makes Viviscal’s emphasis on their clinical research problematic.
For starters, these eight clinical studies weren’t published in high-ranking dermatology journals. Rather, they were published in lower-ranking journals in dermatology and medicine. These are journals that rank below the top quartile, according to SciMago Journal Rankings.
Now, one might wonder, “Who cares about a journal’s ranking? Peer review means peer review!” But unfortunately, this isn’t true. This is because not all peer review is created equal.
Quality reviewers – those of reputable institutions and research centers – generally reject review requests from unknown or lesser-respected journals. Why? Because the papers submitted there are often of lower quality. This forces lower-quality journals to send mass emails of review requests –until they either find someone to accept the review or they decide to make a decision on the paper without any external review at all.
In the case of low-ranking journals, too often are their reviewers people with zero expertise regarding the manuscript in which they’re reviewing.
For example, Perfect Hair Health has published two papers about androgenic alopecia. A list of the last three review requests from low-ranking journals? Manuscripts about:
- Dapsone-loaded micro sponge gel for acne management
- Business management practices
- R&D teams: how innovation and performance varies between large American and Chinese firms
All three review requests were declined because the company only publishes research on hair.
So, just think of how far down a list someone has to get before they contact Perfect Hair Health: someone with zero experience, let alone expertise, in any of these fields.
What’s worse: a quick Google search just revealed that two of these three papers passed peer review, made it into a journal, and are now indexed in scholarly databases. That suggests they were reviewed by someone! If not me, then who? Someone with an equally absent level of expertise? Or nobody at all – given some journals’ incentives to collect authors’ payments in exchange for publications?
Now, back to Viviscal.
The company did, in fact, publish their clinical studies in lower-ranking journals. Knowing this, is there evidence that these studies weren’t properly reviewed?
Yes. In fact, one can identify – just by reading these papers – errors so big, they should’ve been flagged by literally anyone reading the paper.
Example 1: grammatical errors… in the first sentence of a paper
See the first of Viviscal’s 2015 study, published in International Journal of Trichology:
“Since skin and hair quality are potent vitality signals, and hair growth deficiency can cause significant psychological morbidity.”
That’s not even a complete sentence.
Example 2: hair count increases of 1,381%
In Viviscal’s first-ever study, investigators show the results of Viviscal supplementation on hair counts of men with androgenic alopecia (AGA) after six months. Their final hair count increase? A jump from 1,238 to 17,101 hairs per measured region… an increase of 1,381%.

Obviously, this is just a typo. The investigators clearly meant to write 1,710 and not 17,1010 (as indicated by the hair count differences listed in the final row). But a serious reviewer should’ve caught this.
This is the difference between publishing in reputable journals, and publishing just so you can tell people that your product has a peer-reviewed clinical study. The former actually matters; the latter is just for marketing.
Problem #3: Many of Viviscal’s studies have selection bias. Many were done on people with a type of hair loss that doesn’t represent the majority of Viviscal consumers.
It doesn’t just matter how people write up a clinical study; it also matters how that study was conducted. And in this regard, many of Viviscal’s published studies have serious problems. This is especially true in the way that they’ve selected participants for their study.
For reference, there are dozens of types of hair loss, and each type has a different set of causes. The most common types of hair loss are (1) androgenic alopecia (AGA) – also known as male and female pattern hair loss, and (2) telogen effluvium.
Current census is that AGA is caused by a combination of hormones and genetics. It’s chronic, progressive, and without treatment, it worsens. Conversely, telogen effluvium is a form of temporary hair loss. It’s got a wide set of causes – stress, medication use, hypothyroidism, etc. – and once the underlying cause of telogen effluvium is resolved, usually the hair will return in 3-6 months.
For women, one common cause of telogen effluvium is a nutrient deficiency. And one of the most common nutrient deficiencies in women of “childrearing age” is iron – because women lose iron each month during menstruation.
Therefore, this is a percentage of women losing their hair from telogen effluvium – a temporary form of hair loss. And a percentage of those women have telogen effluvium due to low iron stores. If these women correct their low iron stores, they’ll often regrow their hair.
So, let’s look at some of the best Viviscal studies: the ones published in journals that are lower-ranking, but still high enough to likely find reputable reviewers.
These studies were conducted in the U.S. That means they had to register the trials on clinicaltrials.gov. And whenever a trial registers on this site, they have to outline the selection criteria for participants. In other words, they have to tell you how the investigators selected people to include (or exclude) as part of their study.
So, when it comes to participant selection, what do all three of Viviscal’s US-based clinical trials have in common?
All of the studies selected women with temporary forms of hair thinning – mainly the result of poor diets, stress, or menstrual cycles – of which would’ve resolved without a nutritional supplement if the person had just taken measures to get more of those nutrients into their diets.
To quote directly from the trial setups:
“Inclusion Criteria: Females with self-perceived thinning hair associated with poor diet, stress, hormone influences or abnormal menstrual cycle.”
All of these clinical trials showed statistically significant hair count increases to Viviscal after 3-6 months of use. Not surprisingly, at least two of these trials were conducted by the Ablon Group – the research institution that used nearly the same selection criteria for Nutrafol’s clinical study – which sufferers from the same problems will be illustrated.
Why is this such a problem?
For two reasons.
Firstly, this selection criteria is incredibly narrow. Women with telogen effluvium from a nutrient deficiency represent only a fraction of people with hair loss. While there’s no data on the incidence of nutrient deficiency-driven telogen effluvium, it probably responsible for less than 10% of hair loss cases in the U.S.
This means that if Viviscal advertises its “clinical results” to all U.S. hair loss sufferers – the results from their clinical trial won’t apply to 90% of them. But consumers don’t know this. They read the words “clinically proven”, and expect that this product applies to them and will reap positive results.
That’s the first problem.
The second problem is that if the women in this study had just reduced their stress levels, improved their diets, and/or made an effort to get more iron, they likely would’ve seen the same degree of hair regrowth… and without the aid of a supplement that costs $39.99 every month.
After all, studies on women with nutrient deficiency-related telogen effluvium have shown equivalent increases in hair counts – without Viviscal’s proprietary ingredients – and all with a basic nutritional supplement.[14]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6136400/
Are there any studies that fairly assess Viviscal?
Yes.
There is one clinical study on Viviscal that appears to meet this criteria. It was done on men with androgenic alopecia (AGA) – the most common cause of hair thinning for adult males.
It was a 1997 study conducted on 200 men with AGA, all of whom were instructed to take Viviscal® for Men twice daily for six months. The study wasn’t published in a high-ranking journal, but it also didn’t have the same selection criteria biases identified in Viviscal’s more recent studies.
Moreover, the study had clearly defined methodologies. The researchers used objective measurements for results – like hair count changes using a trichogram, or hairline changes by calculating the distance between the hairline and the eyebrows before and after treatment. In addition, the researchers also had participants complete a self-assessment survey to standardize their opinions of the supplement.
Over the six-month period, 32 men dropped out of the study. But of the 178 men who completed the trial, here were their results:
- Across all Viviscal users, hair counts increased by 4% (statistically insignificant)
- 75% of men reported a decrease in hair loss (i.e., the rate of hair loss slowed)
- 15% of men showed partial hair density improvements
These results aren’t that impressive. But, in our opinion, they’re the fairest results ever published on Viviscal. Why? Because they set realistic expectations of the supplement.
Males with AGA who are taking Viviscal should set their expectations that the supplement simply slows down the progression of hair loss; the supplement will not fix the problem. And for those who (1) are happy with that expectation, (2) understand the effects only last with continued use, and (3) don’t mind paying $39.99 per month indefinitely – then this supplement might be a good choice.
Viviscal’s clinical research: the bottom line
- Viviscal boasts over 12 clinical studies on their product line – more studies than any other hair loss supplement.
- However, of these 12 studies, four of them were never published in a scholarly journal.
- Of the studies that were published, these clinical trials were published in low-ranking journals that tend to have really easy peer-review procedures,
- Resultantly, these studies were published with problems that would’ve been flagged – and likely would’ve led to a rejection – in reputable journals: for example, typos in the opening sentences and selection biases for participants.
- This is most evident with three of Viviscal’s published studies: the ones that tested the supplement on women with temporary hair thinning as a result of stress, a poor diet, or menstruation-related iron loss. These types of hair loss sufferers are most likely to benefit from a basic nutritional supplement – particularly ones containing iron, zinc, and antioxidants.
- Moreover, hair loss due to a nutrient deficiency is relatively uncommon compared to all hair loss causes. This type of hair loss accounts for just a small fraction of hair loss cases in the U.S. – likely less than 10%. Therefore, it’s unethical to advertise these results as “clinically effective” to all people with hair loss, when the results only apply to a small portion of a people hearing the claim.
- There is one study on Viviscal that seems fairly conducted: a trial on 200 men with androgenic alopecia (AGA). This is the most common form of hair loss in adult men. The trial found that Viviscal did not statistically improve hair counts, but that the supplement did help decrease the rate of hair loss for these men.
As such, our takeaways on Viviscal’s clinical research are the following:
- The product is great for females with hair loss due to a poor diet and/or nutrient loss from menstruation.
- The product is great for males with AGA who want to take a natural approach to improving their hair and only want to slow down the rate of hair loss – and are comfortable spending $39.99 per month to do so.
Otherwise, we think that Viviscal by itself is not an effective solution for most people with hair loss, and that this money could be better invested elsewhere.
Product purity: heavy metals, microbes, and contaminants
While Viviscal’s clinical studies and testimonials aren’t as impressive as they look at first glance, there is good news. The company makes a high-quality supplement… at least in terms of product purity.
The Perfect Hair Health team bought Viviscal® For Men and sent it to a third-party lab testing facility to test for contaminants often found in consumer supplement products: heavy metals, pathogenic microbes, and impurities related to materials processing.
There were no red flags. By all means, this supplement appears to be made well. What you see on the ingredients list is what you get.
Viviscal® Man purity: heavy metals, microbes, and pesticide residues

This is a positive, as some products that the Perfect Hair Health team has reviewed (i.e., Hairguard Anti-Hair Loss Essentials Supplement) have demonstrated an absence of the ingredients they list on their product labels.
BONUS: How did Viviscal start?
This isn’t related to our analysis of the supplement, but it’s a part of our investigation worth sharing.
Viviscal says that the company all began with the discovery (and development) of AminoMar™ Marine Complex – a proprietary blend of shark cartilage and oyster extract power. According to their website:
“AminoMar is a proprietary marine complex available exclusively in Viviscal hair growth* supplements. In the 1980s, a professor from Scandinavia discovered that the Inuits’ great hair and skin was the result of their fish- and protein-rich diet. He isolated the key protein molecules in their diet and it was from these origins that AminoMar was created. Since then, Viviscal has been tried and tested by clinicians around the world.”
The story sounds almost too good to be true. An unnamed Scandinavian researcher… An observation made amongst the Inuits…. The identification of diet as responsible for the Inuit’s great hair… The isolation of key protein molecules from that diet… The packaging of these molecules into a clinically supported supplement.
Is there any validity to this story? The Perfect Hair Health team attempted to identify this mysterious Scandinavian researcher, his early research on the Inuits, and how this research eventually culminated into the product Viviscal.
These efforts just led to more confusion.
Viviscal’s beginnings: fact or fiction?
Research began by combing through Viviscal’s earliest published studies from the 1990s. It was assumed that in these early papers, Viviscal would discuss their novel proprietary blend: how they came across it, how the blend’s suspected effects might improve hair growth, and why the company has decided to study the blend in a clinical setting.
Unfortunately, the team couldn’t find any references mentioning the story that Viviscal explains in their marketing.
The closest thing identified was a 2019 literature review on alternative hair loss treatments, “Complementary and Alternative Treatments for Alopecia: A Comprehensive Review.” According to that review:
“Marine proteins, including extracellular matrix components from sharks and mollusks, have been produced for over 15 years to enhance hair growth. A Scandinavian researcher first described the exceptionally healthy skin and hair of the Inuit peoples to be a result of their fish- and protein-rich diet [36, 37]”.[15]https://www.karger.com/Article/FullText/492035
But when checking the review’s references (i.e., studies “[36, 37]”), it was found that those studies didn’t actually support the claims made in that quote.
For instance, that first reference is to Viviscal’s first-ever study.[16]https://www.ncbi.nlm.nih.gov/pubmed/1286738 That study had already been read and there was no mention of Inuits or a Scandinavian researcher. The second reference (i.e., “37”) couldn’t be found either. Why? Because according to Viviscal, that reference is to a clinical trial that was never even published.
So, the digging continued. The only thing to do next: read all of the studies mentioned in Viviscal’s first study from 1992. In other words, read the papers within a paper.
Still no references to a Scandinavian researcher or the Inuit… or anything about how this marine extract was developed or its purported mechanisms of action.
A how-to guide on passing peer review

The closest thing the team could find were studies on a product called Imedeen® – a marine extract supplement that was shown to improve skin health in females. These studies were done from 1991-1992 – one year before Viviscal’s first study – but these studies also don’t mention what prompted anyone to start studying these marine extracts.
What is Viviscal’s true genesis story?
This remains unknown. Perfect Hair Health reached to Viviscal® in a good faith effort to obtain the name of this Scandinavian professor, so that the team could verify the story they tell in their marketing. No reply has been recieved.
Interestingly, a 2001 clinical study on HairGain® – the earlier brand name of Viviscal® – was found.[17]https://www.researchgate.net/publication/12056799 This study showed that the supplement led to impressive hair regrowth in men with androgenic alopecia. The study was done by a man named Erling Thom – a Scandinavian researcher who was later accused of falsifying data in the studies he conducted on alternative health products.
The team couldn’t find any evidence tying Erlin Thom to Viviscal’s earlier clinical research. But there also wasn’t any evidence that he wasn’t involved. After all, Viviscal’s elusive genesis story seems to have no paper trail – which is odd for a product involved in so much clinical research.
It appears as though Viviscal was created from Imedeen® – an earlier product that contained a similar marine extract, but was positioned for improving aging skin rather than hair loss. Survey portions of Imedeen® studies in the early 1990’s showed that women also reported improvements to their brittle hair. So, our guess is that marketers of Imedeen® saw an opportunity to retarget the product, and either sold off or repositioned the marine extract into a hair supplement and later started testing it on hair loss sufferers.
But as far as this Scandinavian professor, his observations on the Inuits, and the actual identification of why these marine extracts might prove helpful to skin or hair… this part of the story seems to remain lost in time (and clinical research).
Viviscal®: who are the best candidates?
Viviscal® might be right for …
- Females with hair loss due to a poor diet and/or nutrient loss from menstruation.
- Males with AGA who want to take a natural approach to improving their hair and only want to slow down the rate at which they’re losing hair – and are comfortable spending $39.99 per month to do so.
Viviscal® might not be a good fit for …
- Male with AGA with expectations any higher than the above.
- Females with hair loss related to thyroid dysfunction, PCOS, childbirth, stress, vitamin D deficiency… or virtually anything else outside of the nutrient deficiencies that Viviscal® Woman helps to address (i.e., fatty acids, iron, and zinc).
The bottom line
Viviscal is the most clinically studied hair loss supplement on the planet. But that doesn’t mean it’s the best hair loss supplement available. This is obvious at the outset with Viviscal’s relatively low number of customer before-after photos featured on their website – which, for a company with millions of customers over 25+ years, is a little unusual.
Moreover, Viviscal’s clinical research isn’t as impressive as conveyed in its marketing. For starters, at least 33% of their clinical studies were never published in a scholarly journal. Of the ones that were published, all of them were published in low-ranking dermatology journals – with many of those studies containing glaring typos and selection biases that would’ve led to their rejection from reputable journals.
In addition, the Viviscal studies producing the clearest before-after photos were done on women with temporary hair loss due to stress, a poor diet, and/or nutrient deficiencies as a result of menstruation. This specific type of hair loss is the one that is best positioned to respond to a nutritional supplement, and it’s also a type of hair loss that is (1) relatively uncommon among hair loss sufferers in the developed world, and (2) one that can be improved without a $39.99 supplement – and just through lifestyle and dietary changes.
Lastly, Viviscal®’s genesis story of a Scandinavian professor – his observations on Inuits, their hair-healthy diets, and the isolation of marine compounds responsible for the Inuit’s great hair – is either exaggerated or fabricated. After review, it can be assumed that this product was developed from an earlier skincare product (with a similar marine extract) after survey research found that women thought that product also improved their brittle hair.
On the positives – Viviscal® Man did pass Perfect Hair Health’s third-party laboratory testing for heavy metals, pollutants, and pathogenic microorganisms. In other words, what you see on the label is what you get. But unfortunately, this isn’t enough to earn a recommendation – especially given its price point and the discrepancies in Viviscal’s real-world results versus their clinical research.
Questions? Comments? Please reach out in the dedicated forum thread below
References[+]
References ↑1 https://pubmed.ncbi.nlm.nih.gov/1286738/ ↑2 https://www.ncbi.nlm.nih.gov/pubmed/1864451 ↑3, ↑15 https://www.karger.com/Article/FullText/492035 ↑4 https://www.ncbi.nlm.nih.gov/pubmed/1610689 ↑5 https://nutritiondata.self.com/facts/nut-and-seed-products/3163/2 ↑6 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3819075/ ↑7 https://onlinelibrary.wiley.com/doi/abs/10.1111/jocd.12127 ↑8 https://www.ncbi.nlm.nih.gov/books/NBK547751/ ↑9 https://perfecthairhealth.com/nutrient-deficiency-hair-loss/#biotin ↑10 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3678013/ ↑11 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6385517/ ↑12 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC340385/ ↑13 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3509882/ ↑14 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6136400/ ↑16 https://www.ncbi.nlm.nih.gov/pubmed/1286738 ↑17 https://www.researchgate.net/publication/12056799 Anyone searching “How to reverse hair loss online” has undoubtedly come across the Big Three protocol: minoxidil (Rogaine®), finasteride (Propecia®), and ketoconazole shampoo (Nizoral®).
What many might not know: despite ketoconazole’s popularity, it’s not actually FDA-approved for pattern hair loss, nor is it as well-researched as minoxidil or finasteride.
In fact, there are just a few human studies on Nizoral for hair loss and even fewer on people with just androgenic alopecia, the most common form of hair thinning in men.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
Is Ketoconazole Worthy of Big Three Status?
Here we’ll uncover the evidence on ketoconazole for hair regrowth. We’ll cut straight-to-the-facts about ketoconazole, its effects on hair loss, and whether or not this shampoo is a good fit. Along the way, we”ll also uncover…
- Which formulation is better: 1% or 2% ketoconazole
- Why not everyone is a good candidate for ketoconazole
- How to (potentially) increase ketoconazole’s efficacy (see our before-after photos)
- Who needs to worry about ketoconazole’s potential side effects
Nizoral for Hair Loss: Overview
- Effort: Low (used as shampoo just 2-3 times per week)
- Expectations: According to studies so far, hair loss improvement is observed after 3-6 months
- Response rate: 80%+
- Regrowth rate: ~5% alone; 25-40% if combined with microneedling and/or finasteride and/or minoxidil
- Cost: Low ($10-$20 per bottle of 100ml, which should last two months)
- Problems: Not as well-studied as finasteride or minoxidil; 2% formulations work better but generally require a prescription (though this can be circumvented online); less studied on women (though it’s likely just as effective)
Key Takeaways
Ketoconazole is a low-cost, low-effort shampoo with practically no side effects. It’s clinically shown to help improve hair loss from both androgenic alopecia (AGA) and telogen effluvium (TE).
While 1% ketoconazole is available over the counter, 2% ketoconazole usually requires a doctor’s prescription. Studies show that 2% ketoconazole is more effective, particularly in helping to normalize excessive hair shedding from rapid-onset AGA and/or TE. [1]https://pubmed.ncbi.nlm.nih.gov/9669136/
Can Nizoral help with hair growth?
If a 2% prescription-strength formulation is used, yes.
By itself, ketoconazole is unlikely to stimulate hair regrowth on par with finasteride or combination therapies. So, ketoconazole is just one part of a multi-pronged hair loss regimen. This shampoo may have synergistic effects with stimulation-based therapies like microneedling, massaging, and/or platelet-rich plasma therapy. It also seems to pair well with most FDA-approved / FDA-cleared treatments like finasteride, minoxidil, and low-level laser therapy.
While oral ketoconazole comes with significant risks of side effects, 2% ketoconazole shampoo seems to carry little (if any) risks of side effects – mainly because of its low time of exposure and systemic absorption versus its oral formulations.
The best candidates for 2% ketoconazole shampoo are hair loss sufferers who are comfortable using the shampoo 2-3 times per week and who are dealing with dandruff and/or excessive hair shedding from AGA or TE.
More information on the science behind ketoconazole – its mechanisms of action, supporting evidence, expectations for hair regrowth, and contraindications – can be found below.
What Is Ketoconazole?

Ketoconazole: molecular structure
Ketoconazole is more commonly mentioned by the brand name Nizoral®, and most people know about it as a shampoo.
Simply put, ketoconazole is an anti-fungal medication. It’s a drug commonly used to help improve fungal-related conditions – like dandruff, fungal infections, certain hormone-linked diseases, and even hair loss from fungal and non-fungal causes.
If it’s a fungal medication, why is it used for hair loss?
Because ketoconazole’s mechanisms of action – as an anti-fungal, anti-inflammatory, anti-androgenic, and pro-anagen agent – all overlap with the causes of telogen effluvium and androgenic alopecia.
Here’s how.
Ketoconazole’s anti-fungal properties help fight off yeast, fungi, and bacterial infections that can cause excessive hair shedding.
As an anti-fungal medication, ketoconazole may also have anti-inflammatory effects, especially in hair follicle sites.[2]https://www.ncbi.nlm.nih.gov/pubmed/9669136
Many yeast, fungi, and bacteria feed off our dead skin as well as the oils our skin produces (i.e., sebum) which helps to lubricate our hair. Resultantly, these species can often be found residing in parts of our hair follicle – specifically, the infundibulum (i.e., the upper third of each hair shaft) and sebaceous glands.
However, sometimes too many yeast, fungi, and/or bacteria may colonize our sebaceous glands – leading to over-colonization. This is particularly true with the fungus-like yeast species Malassezia spp., which is found in 65% of healthy scalps.[3]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4367942/
Many of these species produce toxic byproducts (i.e. porphyrins) as part of their digestion of sebum. In cases of over-colonization, the accumulation of toxins elicits an inflammatory response in the sebaceous gland. Ironically, the body often responds by sending more sebum to the sebaceous glands – which would help to otherwise resolve the inflammation, but not in these instances. Rather, the excess sebum simply feeds these pathogenic microorganisms, and the process continues.
This is known as a sebum-feedback loop. At moderate levels, it leads to excessive dandruff. At higher levels, it triggers excessive hair shedding – often characterized as microorganism-driven telogen effluvium (TE).
Enter ketoconazole – a potent anti-fungal medication that can help kill off these pathogens and, in doing so, stop this feedback loop.
Ketoconazole damages the cell membranes of fungi and yeast.[4]https://pubchem.ncbi.nlm.nih.gov/compound/Ketoconazole Specifically, it stops a fungus from producing ergosterol – a crucial part of the cell membrane that helps keep cellular content from leaking out as well as unwelcome substances from invading.
The end result?
Ketoconazole helps kill off pathogenic yeast/fungi, which then reduces scalp inflammation and helps resolve any excessive hair shedding (TE).
This is also why ketoconazole is such an effective treatment for scalp conditions caused by fungi – like dandruff and seborrheic dermatitis. Those conditions are also often caused by Malassezia spp. – the fungus-like yeast that is (fortunately) hypersensitive to ketoconazole.
Ketoconazole might help reduce inflammation in 30-50% of men with androgenic alopecia
Research shows that 30-50% of hair loss sufferers with androgenic alopecia (AGA) also have P. acnes and/or Malassezia spp. infections in the scalp. Just like with TE, the presence of these microbes may exacerbate inflammation, induce early hair shedding, and thereby accelerate the progression of AGA.
In these cases, anti-fungal and/or antibacterial shampoos tend to be useful – because they help to reduce the infections that are accelerating hair shedding in AGA.
Ketoconazole might have anti-androgenic effects in scalp tissues
Ketoconazole isn’t just an anti-fungal; it also has anti-androgenic properties when taken orally. And, while researchers have debated whether these findings extend to topically applied ketoconazole, at least one peer-reviewed paper makes a strong argument in its favor.
Specifically, this hypothetical model argues that topically applied ketoconazole has anti-androgenic properties.[5]https://www.ncbi.nlm.nih.gov/pubmed/14729013 In particular, it may help reduce dihydrotestosterone (DHT) – the main hormone implicated in AGA – and in two ways:
- Inhibits 5-alpha reductase. This is an enzyme that converts free testosterone into DHT.
- Blocks androgen receptors. Androgen receptors are where DHT attaches to a cell to influence tissue function (i.e., hair follicle miniaturization). If androgen receptors are blocked, DHT cannot bind to these cells, and thus does not affect that tissue’s functionality.
Together, if ketoconazole has enough of a DHT-reducing effect in balding scalp tissues, it should help to improve AGA – similar to the ways in which treatments like finasteride work.
Ketoconazole may prolong the anagen phase of the hair growth cycle
At any given moment, roughly 85% of scalp hairs are in their growth (anagen) phase, while remaining hairs are either in a resting (catagen) or shedding (telogen) phase.
One defining characteristic of telogen effluvium (TE) is a large increase in the number of shedding versus growth phase hairs (i.e., increased telogen:anagen ratio). In TE, it’s not uncommon to see telogen:anagen ratios of 40-50% and beyond.
This is also observed in androgenic alopecia (AGA) – though to a lesser degree, as AGA is characterized more so by hair follicle miniaturization, less so by hair shedding.
Interestingly, one research team demonstrated that, for reasons unknown, ketoconazole appears to prolong the anagen (growth) phase of hair follicles affected by TE and/or AGA.[6]https://www.ncbi.nlm.nih.gov/pubmed/18498517
This effect should help delay the progression of both conditions, and maybe even partially reverse them.
Summary of Mechanisms
Ketoconazole might improve telogen effluvium by:
- Killing off pathogens in the scalp, thus normalizing excessive hair shedding triggered by microorganism-mediated inflammation
- Prolonging the anagen phase of the hair cycle
Ketoconazole might improve androgenic alopecia by:
- Killing off pathogens in the scalp, thus normalizing excessive hair shedding triggered by microorganism-mediated inflammation
- Reducing scalp DHT levels by inhibiting 5-alpha reductase and blocking androgen receptors
- Prolonging the anagen phase of the hair cycle
Altogether, these mechanisms suggest that ketoconazole may improve both TE and AGA. So, what’s the evidence in human studies?
Clinical studies: is ketoconazole effective for hair loss?
As is always the case with hair loss research, context is key. And when looking into the effectiveness of ketoconazole, we need to evaluate all clinical studies with several things in mind:
- Was the ketoconazole tested on androgenic alopecia or other hair loss disorders?
- Was the formulation strength 1% or 2%?
- What, exactly, was measured?
To date, there are only four clinical studies on ketoconazole and hair loss (that we could find). As such, we’ll present them in detail. If you’d like, you can skip to the summaries of each study.
Ketoconazole Shampoo: Effect of Long-Term Use in Androgenic Alopecia
Full text: Piérard-Franchimont et al., 1998 [7]https://www.ncbi.nlm.nih.gov/pubmed/9669136
Study one: 2% ketoconazole versus a normal shampoo
- Who: 39 male only-AGA-subjects
- What: 2% ketoconazole shampoo versus a normal shampoo. During the study duration, 27 men used ketoconazole while 12 men used normal shampoo. There were also 22 non-AGA-controls – half of them testing ketoconazole; half of them trying normal shampoo.
- How long: 2-4 times per week for 21 months
- Measurement: AGA pilary index (PI). This was defined as the percentage of hairs in anagen (A) x average diameter (D, μm) of the hair shafts 1.5 cm from the hair bulb.
- Results:
- PI of non-AGA-controls remained unchanged, no matter the type of shampoo used (ketoconazole versus normal shampoo).
- PI of only-AGA-subjects with unmedicated shampoo showed a slow linear decrease over time, while the ketoconazole group “yielded a progressive PI increase that became evident after a 6-month survey and apparently reached a plateau value after about 15 months”.
- Takeaways:
- In men without androgenic alopecia, ketoconazole doesn’t improve anagen hair counts or hair shaft diameter
- In men with androgenic alopecia, ketoconazole improves both anagen hair counts and overall hair shaft diameter
Study two: 2% ketoconazole versus 2% minoxidil
- Who: 8 male only-AGA-subjects; 4 using ketoconazole, and 4 using minoxidil
- What: 2% ketoconazole shampoo (vs. 2% minoxidil lotion)
- How long: ad libitum (i.e., as often as desired) for 6 months
- Measurements: hair density; hair shaft diameter and the corresponding sebaceous gland
- Results:
- “A 7% increase in the median hair shaft diameter was yielded by both the [ketoconazole] shampoo and minoxidil + unmedicated shampoo combination.”
- “A 19.4% decrease in the mean sebaceous gland area was observed in the [ketoconazole] group. In contrast, the same variable increased by 5.3% in the minoxidil + unmedicated shampoo group.”
- Ketoconazole improved density of hair by 18% compared to minoxidil by 11%.
- Takeaways:
- Ketoconazole increases hair shaft diameter by 7%, similar to minoxidil
- Ketoconazole decreases sebaceous gland size by nearly 20% – possibly due to its anti-fungal effects. In other words, ketoconazole kills off pathogens that over-colonize, and thereby over-enlarge, the sebaceous glands. This was unique to ketoconazole (minoxidil did not have this effect).
- Ketoconazole improves hair density nearly twice as well as minoxidil
Key points:
These studies are all on men with AGA only, all of whom tested 2% ketoconazole as a shampoo.
The results all show significant improvements to hair density, as well as prolonged anagen phases and hair diameter. Moreover, one study also found that ketoconazole decreased sebaceous gland size – most likely a result of its ability to kill off pathogens overcrowding those sebaceous glands. For these reasons, it’s not unreasonable to assume that ketoconazole might also decrease sebum output.
Nudging hair shedding by antidandruff shampoos. A comparison of 1% ketoconazole, 1% piroctone olamine, and 1% zinc pyrithione formulations

Full text: Piérard-Franchimont et al., 2002 [8]https://onlinelibrary.wiley.com/doi/abs/10.1046/j.1467-2494.2002.00145.x
- Who: 150 men presenting with telogen effluvium related to androgenic alopecia associated with dandruff, separated into three groups with different shampoos: 50 men on 1% ketoconazole, 50 on 1% piroctone olamine, and 50 on 1% zinc pyrithione
- What: 1% ketoconazole shampoo versus two other anti-dandruff shampoos
- How long: 2-3 times a week, for 6 months
- Measurements: hair shedding, hair density, anagen hair percentage, mean proximal hair shaft diameter, sebum excretion rates
- Results:
- Pruritus and dandruff cleared rapidly in all three shampoo groups
- Hair density remained unchanged in all three shampoo groups
- Hair shedding decreased by 17.3% in the ketoconazole group, 16.5% in the piroctone olamine group, and 10.1% in the zinc pyrithione group
- Anagen hair ratio increased by 4.9% in the ketoconazole group, 7.9% in the piroctone olamine group, and 6.8% in the zinc pyrithione group
- Sebum excretion rate decreased by 4.8% in the ketoconazole group, 2.9% in the piroctone olamine group, and 5.5% in the zinc pyrithione group
Key points:
The men featured in this study have telogen effluvium and androgenic alopecia. And, encouragingly, it seems like 1% ketoconazole shampoo 2-3 times per week lessened hair shedding by ~20%, increased hair shaft thickness by ~5%, and decreased sebum output by ~5%.
The bottom-line: comparing across studies, 1% ketoconazole isn’t as impressive as 2%, but the results are still there. For men (and women) suffering from both TE and AGA, 1% or 2% ketoconazole might be a great intervention (among other treatments).
Comparative Efficacy of Various Treatment Regimens for Androgenetic Alopecia in Men
Full text: Khandpur et al., 2002 [9]https://www.ncbi.nlm.nih.gov/pubmed/12227482
- Who: 100 male only-AGA-subjects randomized into four groups:
- 30 finasteride
- 36 finasteride + minoxidil
- 24 minoxidil
- 10 finasteride + ketoconazole
- What: 2% ketoconazole shampoo + finasteride 1mg oral/day (vs. finasteride vs. finasteride + 2% minoxidil vs. 2% minoxidil)
- How long: 3 times a week for 1 year
- Measurements: patients’ self-assessment and physicians’ assessment. Photographs were taken.
- Results: finasteride + minoxidil and finasteride + ketoconazole reap the best improvement scores for both self- and physician-assessments. However, finasteride + minoxidil slightly outperformed finasteride + ketoconazole.
Key points:
2% ketoconazole works well as a combination therapy with finasteride.Pilot Study of 15 Patients Receiving a New Treatment Regimen for Androgenic Alopecia: The Effects of Atopy on AGA
Full text: A.W. Rafi et al., 2011 [10]https://www.ncbi.nlm.nih.gov/pubmed/22363845
- Who: 15 AGA subjects with either atopic dermatitis or seborrheic dermatitis
- What: 2% ketoconazole shampoo. 8 subjects used NuH Hair + finasteride + minoxidil + ketoconazole, 5 using only NuH Hair, 1 using NuH Hair + finasteride + ketoconazole, 1 using NuH Hair + ketoconazole (a subject with seborrheic dermatitis)
- How long: ketoconazole usage 2-3 times a week for 9 months
Measurements: Average time for hair regrowth, photo and investigator assessments - Results:
- Average time for hair regrowth
- 30 days with NuH Hair + finasteride + minoxidil + ketoconazole
- 30 days with NuH Hair + finasteride + ketoconazole
- 60 days with NuH Hair + ketoconazole
- 90 days with NuH Hair alone
- Average time for hair regrowth
Key points:
Ketoconazole works well as a combination therapy with finasteride and minoxidil, and it can also improve AGA even in men with atopic and/or seborrheic dermatitis.Key points summary of clinical trials
- By itself and as a combination therapy, 2% ketoconazole improves AGA and TE by:
- Increasing anagen (growth) hairs
- Increasing hair shaft diameter
- Increasing hair density
- Hair improvements from 2% ketoconazole seem to sustain, not wane (at least over 21 months of use)
- 2% ketoconazole increases hair density; 1% ketoconazole doesn’t
Very broadly speaking, ketoconazole alone might be a little bit less effective than minoxidil alone, but it also seems to be a better bet in some respects: more people respond to Nizoral for hair loss, its effects don’t wane over 21 months, and it targets AGA from multiple angles.
Applying Ketoconazole
If you want to get the most out of ketoconazole, here are some tips to maximize your chances of hair regrowth and use ketoconazole in the most effective way:
Opt for 2% prescription, not 1% over-the-counter
There is evidence that prescription-strength 2% ketoconazole is (much) more effective than 1 % ketoconazole.
In this study, 2% ketoconazole shampoo increased hair density by 18% while in this study, 1% ketoconazole shampoo didn’t change hair density at all. Both times, ketoconazole was applied around 3 times a week for 6 months. [11]https://www.ncbi.nlm.nih.gov/pubmed/9669136 [12]https://onlinelibrary.wiley.com/doi/abs/10.1046/j.1467-2494.2002.00145.x
Also, in this study, 1% ketoconazole and 2% ketoconazole were compared with their effect on seborrheic dermatitis, and the results were so that “[ketoconazole] 2% had superior efficacy compared to [ketozonaole] 1% in the treatment of severe dandruff and scalp seborrheic dermatitis.”[13]https://www.karger.com/Article/PDF/51628
So get the 2% ketoconazole, not the 1%.
How can I get the 2% Nizoral shampoo without a prescription?
One of our members found 2% ketoconazole online, and from a company called Nizoral Shop.
So how does this company was circumventing prescriptions and shipping to the U.S. (and elsewhere)?
As it turns out, their Nizoral products depart from overseas warehouses where prescriptions are not required.
So, for anyone looking for 2%, Nizoral Shop might be a great option. The company later offered our members a 20% discount on the first 100 orders from our community.
To access case studies, expert interviews, forums, comprehensive guides, and other special offers, join our membership. You will also get a personalized Regrowth Roadmap tailored to your needs and treatment preferences.
We aren’t affiliated with any physical product brands, and we haven’t tried this shampoo brand. The company did say that for anyone making orders during the COVID-19 period: “It is highly recommended to select UPS/DHL priority express shipping option, as the other shipping methods are suspended until further notice due to the current pandemic.”
Get the Nizoral shampoo, not the topical
This is just a practical tip. In some countries, there is a topical version of ketoconazole available to consumers. Arguably, as a topical, ketoconazole would likely have more significant effects versus a shampoo – mainly because of the differences in the length of time on the scalp.
At the same time, topical ketoconazole may be more likely to cause side effects due to higher systemic absorption. What’s more, the topical non-shampoo version of ketoconazole has never been used in human studies on hair loss.
So, we recommend sticking to what’s studied; not what’s theoretically potentially more effective. Go with Nizoral shampoo.
Apply 2-4 times per week
Collectively, these studies show that applying 2% ketoconazole 2-3 times per week seems to show the most promise at resolving hair loss disorders and not just dandruff. So, plan on using this shampoo around every other day.
Do I have to use it forever?
Not necessarily. If ketoconazole’s most beneficial mechanism of action is that it kills off the over-colonization of pathogenic organisms that are creating additional scalp inflammation, then chances are that after these pathogenic organisms are gone, you may be able to significantly reduce usage frequencies after months 3-4.
That means transitioning to once-weekly usage (or less).
Combine ketoconazole with other hair loss therapies and treatments
Generally speaking, in ketoconazole studies on humans with AGA, the best results have been achieved by those that used ketoconazole in combination with other treatments.
This makes sense, as ketoconazole’s mechanisms of action are different from minoxidil, which are different from microneedling, which are different from finasteride. The more mechanisms you target, the better your results (in most cases).
In fact, we have an example from our community of a member doing just this: combining ketoconazole with microneedling, massaging, and minoxidil to break through a period of stagnation in hair recovery.
Here are his results: 20+ months of scalp massage alongside microneedling, minoxidil, and ketoconazole

Hair growth from scalp massage alongside microneedling, minoxidil, and ketoconazole
Nizoral for Hair Loss: The Side Effects
This study showed that high doses of oral ketoconazole can impair testosterone production in men, but this review article from drugs.com states that these effects haven’t been reported – even with topical ketoconazole – and seem unlikely anyway because through topical application, way too little substance is absorbed.[14]https://www.ncbi.nlm.nih.gov/pubmed/3659003[15]https://www.drugs.com/monograph/ketoconazole-topical.html
So, based on this information, you don’t need to worry about the shampoo’s effect on testosterone.
Rare side effects are summarized here. These are not prevalent, particularly if ketoconazole is formulated as a shampoo.[16]https://www.drugs.com/sfx/ketoconazole-topical-side-effects.html
All in all, ketoconazole shampoo seems to be relatively free of side effects, and a relatively safe option for those with excessive hair shedding from androgenic alopecia, telogen effluvium, or both.
For those with sensitive skin who wish to try a more natural Nizoral formulation, Sent from Earth Caffeine & Saw Palmetto Shampoo may suffice. However, this shampoo contains just 1% ketoconazole. We are not affiliated with this company; we just wanted to provide an example of what else is out there.
Who are the best candidates for Nizoral?
In regard to hair loss sufferers, ketoconazole is proven to help:
Those with androgenic alopecia
Having checked the studies above, it is pretty indisputable that ketoconazole improves AGA in humans – and not only in those who suffer additionally from seborrheic dermatitis or telogen effluvium, but clearly also in those who have only AGA. [17]https://www.ncbi.nlm.nih.gov/pubmed/9669136
Those with a hair shedding disorder (like telogen effluvium)
When TE is derived from a pathogenic microorganism, seborrheic dermatitis, or both (which can be the case), ketoconazole might help – as its anti-fungal effects can intervene in the earliest stages of seborrheic dermatitis development.[18]https://donovanmedical.com/hair-blog/2017/5/23/is-it-possible-for-seb-derm-to-cause-hair-loss
Interestingly, ketoconazole seems to improve TE regardless of its causes. We know this from the above study with 150 TE men, which showed that ketoconazole improved TE outcomes – despite the high likelihood of myriad TE causes present within that study.[19]https://onlinelibrary.wiley.com/doi/abs/10.1046/j.1467-2494.2002.00145.x
These studies are mostly on men. What about women?
To our knowledge, there are no published studies on Nizoral for hair loss in females with pattern alopecia (yet). However, one study on females found that 2% ketoconazole as a topical (not shampoo) demonstrated similar efficacy compared to 2% minoxidil over six months of use.[20]https://biomeddermatol.biomedcentral.com/articles/10.1186/s41702-019-0046-y
Given the results of this study (and ketoconazole’s suspected mechanisms of action), there is reason to believe ketoconazole shampoo is probably effective for women, as well.[21]https://www.derm.theclinics.com/article/S0733-8635(12)00093-9/abstract
You’re an ideal candidate for ketoconazole if you…
- Suffer from AGA and/or a hair shedding disorder, particularly alongside seborrheic dermatitis or symptoms of microorganism overgrowths (like excessive dandruff and/or sebum activity)
- Want the benefit of a chemical treatment without a high risk of severe side effects
- Are using minoxidil/finasteride and want to increase their efficacy
- Are performing stimulation-based therapies (i.e., massaging, microneedling, and/or platelet-rich plasma) and want to speed up the regrowth process.
Who is not a good candidate for ketoconazole?
Ketoconazole is less researched on women, although that doesn’t make it less effective. But there are contraindications for oral ketoconazole in pregnant women – and, as a precaution, the standard recommendation is for all women who intend on getting pregnant to avoid even the topical formulations.[22]https://www.drugs.com/pregnancy/ketoconazole.html
Regarding mothers who breastfeed, ketoconazole use is generally considered acceptable, but caution is recommended.[23]https://www.drugs.com/breastfeeding/ketoconazole.html
Above all, both men and women are strongly advised against the use of oral ketoconazole for the treatment of AGA/pattern hair loss. While topical/shampoo formulations have a strong safety profile, oral ketoconazole doesn’t. Consequently, it comes with a higher risk of side effects and is even banned from sale in certain countries.
Summary
Ketoconazole isn’t as well-researched as minoxidil or finasteride. However, studies show that it might be an effective add-on treatment for hair loss (specifically, androgenic alopecia).
There’s evidence that ketoconazole is almost as effective as minoxidil (Rogaine®) at increasing hair density… and that it might be particularly helpful for those with pattern hair loss with rapid hair shedding (i.e., telogen effluvium). So, if you fit within these categories, you might want to consider trying it.
Having said that, ketoconazole formulation matters. While 1% over-the-counter ketoconazole might help reduce dandruff and improve hair loss, 2% prescription ketoconazole is likely superior in its ability to improve hair loss outcomes. So, if you’re going to commit to Nizoral for hair loss, commit fully. Visit your doctor and get a prescription. Or, order online from the Nizoral Shop. Then, start shampooing.
References[+]
References ↑1 https://pubmed.ncbi.nlm.nih.gov/9669136/ ↑2, ↑7, ↑11, ↑17 https://www.ncbi.nlm.nih.gov/pubmed/9669136 ↑3 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4367942/ ↑4 https://pubchem.ncbi.nlm.nih.gov/compound/Ketoconazole ↑5 https://www.ncbi.nlm.nih.gov/pubmed/14729013 ↑6 https://www.ncbi.nlm.nih.gov/pubmed/18498517 ↑8, ↑12, ↑19 https://onlinelibrary.wiley.com/doi/abs/10.1046/j.1467-2494.2002.00145.x ↑9 https://www.ncbi.nlm.nih.gov/pubmed/12227482 ↑10 https://www.ncbi.nlm.nih.gov/pubmed/22363845 ↑13 https://www.karger.com/Article/PDF/51628 ↑14 https://www.ncbi.nlm.nih.gov/pubmed/3659003 ↑15 https://www.drugs.com/monograph/ketoconazole-topical.html ↑16 https://www.drugs.com/sfx/ketoconazole-topical-side-effects.html ↑18 https://donovanmedical.com/hair-blog/2017/5/23/is-it-possible-for-seb-derm-to-cause-hair-loss ↑20 https://biomeddermatol.biomedcentral.com/articles/10.1186/s41702-019-0046-y ↑21 https://www.derm.theclinics.com/article/S0733-8635(12)00093-9/abstract ↑22 https://www.drugs.com/pregnancy/ketoconazole.html ↑23 https://www.drugs.com/breastfeeding/ketoconazole.html Studies show that within 3-6 months of stopping minoxidil, any hair growth resulting from the drug is lost. After quitting minoxidil, hair counts can even temporarily fall below where they would’ve been had we never sought treatment at all, before eventually rebounding back to baseline.
Why does this happen? Is there a way to lessen the “withdrawal shed” from minoxidil? For those who’ve seen hair gains with minoxidil but prefer not to use it forever, there may be some methods to mitigate shedding after quitting minoxidil. This article explains the evidence, and provides an action plan.
- About Minoxidil
- Why People Stop Taking Minoxidil
- What Happens When Quitting Minoxidil
- Is Minoxidil Plus Microneedling the Answer?
- How to (Possibly) Prevent Shedding After Stopping Minoxidil
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
About Minoxidil
Minoxidil is an over-the-counter drug approved by the FDA to treat androgenic alopecia. It’s commonly known by the brand name Rogaine. Along with finasteride, minoxidil is one of only two drugs approved to treat androgenic alopecia in both men and women.
Nobody actually knows how minoxidil works. Minoxidil was initially developed in the 1980s as an oral drug to treat high blood pressure. But when patients started reporting “unwanted” hair regrowth after three or more months of use, its manufacturers decided to reformulate it into a topical and begin testing it on men with androgenic alopecia.[1]https://www.jaad.org/article/S0190-9622(08)00809-8/abstract
Today, we still aren’t sure how it works. But since side effects are minimal, it was nonetheless approved by the FDA for use. There are two primary hypotheses on the mechanisms behind minoxidil.
Hypothesis 1: Minoxidil is a Vasodilator
One defining characteristic of androgenic alopecia is reduced blood flow to balding regions. While there’s debate over whether reduced blood flow is a consequence or cause of hair loss, it’s undisputed that without proper blood supply to a hair follicle, hair cannot grow.
As a vasodilator, minoxidil widens blood vessels, potentially increasing blood flow to the scalp. In addition, Minoxidil opens potassium ion channels, which some researchers think works alongside vasodilation to improve hair growth.[2]https://pubmed.ncbi.nlm.nih.gov/9395721/
Hypothesis 2: Minoxidil Alters the Hair Growth Cycle
It’s possible that minoxidil kicks miniaturizing hair follicles back into the anagen (growth) phase of the hair cycle. Hairs thus become thicker, giving the appearance of overall improved hair density. This could be the result of minoxidil decreasing prostaglandin D2 levels while boosting other prostaglandins, like prostaglandin E2, to downregulate pro-inflammatory growth factors that are linked to hair shedding.[3]https://www.jidonline.org/article/S0022-202X(15)42806-4/pdf
In addition, Minoxidil may prolong the growth phase of the hair cycle by maintaining beta-catenin activity in dermal papilla cells.[4]https://pubmed.ncbi.nlm.nih.gov/21524889/
How Long Does Minoxidil Take to Work?
Minoxidil’s event horizon is approximately 3-6 months. Over half of the people who try it respond to minoxidil within this time frame. But early results tend to wane over time.
One study found that at six months, men using 5% minoxidil twice-daily saw a near-60% change in hair ‘weight’ in balding regions.[5]https://www.sciencedirect.com/science/article/pii/S019096229970006X In other words, their hair had thickened or regrown to weigh 60% more than it did at the start of the study.
That’s huge.
Unfortunately, the same study showed that at 96 weeks, those hair weights decreased to merely 25% higher than baseline. This also happens to be a consistent finding across most studies on minoxidil. Just see this 48-week chart on the effects of 2% and 5% minoxidil on hair counts.[6]https://pubmed.ncbi.nlm.nih.gov/12196747/ Results tend to peak at week 16, then decline thereafter.

Olsen, E. A., Dunlap, F. E., Funicella, T., Koperski, J. A., Swinehart, J. M., Tschen, E. H., & Trancik, R. J. (2002). A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men. Journal of the American Academy of Dermatology, 47(3), 377–385.
This is echoed on 5-year studies on minoxidil, which show a steady decline in non-vellus hair counts in target areas after year one: [7]https://pubmed.ncbi.nlm.nih.gov/2180995/

Olsen, E. A., Weiner, M. S., Amara, I. A., & DeLong, E. R. (1990). Five-year follow-up of men with androgenetic alopecia treated with topical minoxidil. Journal of the American Academy of Dermatology, 22(4), 643–646.
Somewhat relatedly, other studies have demonstrated greatly increased hair counts that failed to translate to visual improvements in hair density.[8]https://www.jaad.org/article/S0190-9622(08)00809-8/abstract
Long-story short: over time, minoxidil’s efficacy begins to wane. And while minoxidil can temporarily increase hair counts, these increases don’t always lead to cosmetic levels of hair regrowth.
Why is this?
Minoxidil helps kickstart hairs back into the anagen (growth) phase of the hair cycle. However, it doesn’t address DHT-driven hair follicle miniaturization. So, while hair counts increase, hair diameters continue to decline, leading to a loss of hair volume and thereby hair thinning over time.
Most people who try minoxidil quit within a year as their results stabilize or slowly decline.
Let’s take a closer look at why, and what happens when they do.
Why Stop Taking Minoxidil?
People who stop taking minoxidil tend to fall into two main camps. Either minoxidil is just not working for them at all, or it is working, but for various reasons, they’d prefer to pass on a twice-daily application for the rest of their lives.
Minoxidil Non-Responders
Some people simply don’t respond to minoxidil. This could be a sign their hair loss stems from a condition other than androgenic alopecia. But as we’ll see, minoxidil just doesn’t always work well on its own.
Is it Androgenic Alopecia?
Non-response to minoxidil could signify that hair loss is not due to androgenic alopecia but something else. There’s some evidence that oral minoxidil might improve hair shedding disorders like chronic telogen effluvium, but it’s technically not FDA-approved for that condition.[9]https://link.springer.com/article/10.1007%2Fs40257-018-0409-y
Is it Strong Enough?
When choosing between 2% and 5%, choose the more potent formula. Studies show that in men, 5% minoxidil is better than the 2% formula, and the same is likely true for women. Prescriptions are available for concentrations of 10% or 15%, and studies show minoxidil non-responders often see better hair growth after switching to these strengths.[10]https://pubmed.ncbi.nlm.nih.gov/28078868/
Is it in Use as a Monotherapy?
The reality is that minoxidil just isn’t very effective by itself. To understand why it helps to learn about an enzyme called Sulfotransferase.
In order to become active, minoxidil must come into contact with Sulfotransferase. About 40% of balding men just don’t have enough Sulfotransferase to elicit a response to Minoxidil – which happens to closely correspond with the percent of non-responders of minoxidil.
What might help increase Sulfotransferase levels? We’ll get to that later.
The Downsides of Minoxidil
Even minoxidil responders may not want to use it forever. It can be costly and inconvenient, and it does have some minor side effects.
Cost
Monthly minoxidil use costs between $15-$40. Hair loss sufferers will need to try it for 6 months and spend close to $200 just to see if they’re a responder. Stick with it for years, and they could end up spending thousands. Some users find that as their results taper off, it no longer warrants the ongoing expense.
Note: the price of minoxidil can be dramatically reduced by purchasing in bulk and through big brands – like the minoxidil offered from Kirkland. But these formulations tend to come with propylene glycol and other carrier ingredients that can irritate the scalp.
Side Effects
The biggest side effect of minoxidil seems to be skin irritation. Between 2% to 6% of users report this.[11]https://www.researchgate.net/publication/221695328_Minoxidil_Use_in_Dermatology_Side_Effects_and_Recent_Patents However, allergy testing suggests that up to 80% of skin-irritation related side effects from minoxidil may not be caused by the minoxidil itself, but rather, a carrier ingredient called propylene glycol.[12]http://www.thaiscience.info/Journals/Article/JMAT/10986429.pdf
There are brands that offer minoxidil without propylene glycol, so be sure to check the labels if you have any concerns of allergies.
Additional side effects include toxicity to cats, under-eye bags, and potential heart palpitations. But these are all relatively rare.
Inconvenience
As hair growth treatments go, minoxidil is relatively easy and convenient. Still, not everyone wants to commit to twice-daily use for the rest of their lives, regardless of its effectiveness. And as we mentioned earlier, minoxidil alone is not an effective long-term treatment. To keep results from waning, using minoxidil in combination with other therapies is recommended, which only adds time and expense.
So if someone decides to stop taking minoxidil, what are the expectations?
What Happens When Stopping Minoxidil
In 1999, researchers conducted a study on the effects of abruptly ceasing minoxidil after long-term treatment.[13]https://www.jaad.org/article/S0190-9622(99)70006-X/fulltext Not only did the group who stopped minoxidil shed hair, but for a month or two, they actually crossed below the threshold of where they would have been if they’d never used minoxidil to begin with.
Let’s take a closer look at what happened.
The Study on Stopping Minoxidil
Researchers spent more than two years following four separate cohorts. One group was treated with 2% minoxidil, another group with 5%, one group was given a placebo, and the fourth group did nothing.
Both the 2% and 5% groups saw improvements in hair counts by the three-month mark. As we’ve said, these improvements leveled off a bit from that point forward but were still higher than hair counts in the placebo and control groups.
After almost two years of treatment, at the 96-week mark, the investigators took the people in the 2% and 5% minoxidil groups and discontinued treatment. We can see the exact moment this occurred by looking at the data on hair weights, which soon started decreasing.

Price, V. H., Menefee, E., & Strauss, P. C. (1999). Changes in hair weight and hair count in men with androgenetic alopecia, after application of 5% and 2% topical minoxidil, placebo, or no treatment. Journal of the American Academy of Dermatology, 41(5), 717–721.
Three months later, by week 108, their hair loss had dipped well below the placebo group and below where they were at the start of the study. Another three months after that, by week 120, both the 2% and 5% groups had rebounded to rejoin toss sufferers will end up right where they started.
As mentioned, any excess shedding should not be permanent, as hair will readjust to new homeostasis without the drug.
So the question becomes, is there a method to weaning from minoxidil that can prevent or reduce shedding?
Is Minoxidil Plus Microneedling the Answer?
In the above study, minoxidil was used as a monotherapy. And we know from the research that combining minoxidil with additional therapies, such as microneedling, can improve outcomes for non-responders and may prevent results from waning after the initial 3-6 months of usage.
So could microneedling also prevent (or delay) shedding if one decides to stop taking minoxidil? Let’s investigate what happens when we use these two therapies in tandem.
About Microneedling
Microneedling is a micro-wounding procedure that involves pricking the skin with tiny needles using either a roller or a pen-shaped tool. Studies have shown microneedling elicits growth factors, signaling proteins, and the enzymatic activity of Sulfotransferase, which we referred to earlier.
In some studies, Microneedling plus Minoxidil seems to elicit a fourfold greater effect on hair count increases than Minoxidil alone.[14]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3746236/
In fact, when combining minoxidil with microneedling, new data show that all new hair gains might hold for much longer – even after quitting all treatments.
The Data on Combined Therapies
Let’s take a closer look at a 2020 study to see why microneedling could be the key to maintaining hair growth, even after quitting minoxidil.[15]https://pubmed.ncbi.nlm.nih.gov/29028377/
In the study, researchers split men into 3 groups. One treated their hair loss with minoxidil only, another group with microneedling only, and one group combined the two therapies. As other studies have shown, the combined therapies were significantly more effective in terms of hair growth.
But what the researchers did next was interesting. They stopped all treatments for each of the 3 groups, then brought them in 6 months later to ask, ‘how much hair growth did you retain, even in the absence of treatment?’ Here were their results:
- Minoxidil Only – 90% lost all new hair growth (just 10% retained new growth)
- Microneedling Only – 70% retained some new hair, 20% retained all new hair, 10% lost all new hair
- Combined Therapies – 70% retained some new hair, 20% retained all new hair, 10% lost all new hair
So the group that combined minoxidil with microneedling not only experienced at least twice the hair growth of the other two groups, but 70% of them held on to at least some of this new growth, even after stopping all treatments. And yet, before we conclude that microneedling plus minoxidil is a fail-safe method for maintaining hair growth after treatment ends, there are some possibilities to consider.
- It’s possible if researchers asked the same question 12 months versus 6 months later, all groups would report an equal amount of hair loss. We’ve seen with other therapies, Finasteride for example, that gains disappear over a longer timeline.
- While the number 70% sounds big, the sample size in this study was relatively small. Each group contained just 20 men. So, while it’s great that 14 men maintained at least some of their results for 6 months after treatment ended, it’s possible this percentage could change within a larger sample.
So, while the study above is promising, we don’t really have enough data to definitively say whether or not hair shedding after quitting minoxidil can be prevented.
We’ve yet to see any literature that would help predict who will or will not shed badly from minoxidil. However logically, it may be that those who respond better to minoxidil (or the more hair minoxidil helps one keep during use) simply have more hair to lose during withdrawal.
Anecdotally, about 50% of the male Perfect Hair Health members who have slowly weaned from minoxidil while maintaining microneedling therapy noticed no cosmetic differences in their hair counts afterward.
Basically, they’re able to maintain similar visuals even without the drugs. The other 50% do see a decline visually, but it’s nowhere near baseline or very rarely all the way back to baseline.
If hair loss sufferers do get to a point where they’re happy with their hair and want to wean away from drugs, doing so with the right tapering protocol while continuing the use of microneedling could be a solution.
The Best Way to Quit Minoxidil
When is the best time to call it quits? Never, if you’d like to take as much risk off the table as you can.
Otherwise, the following tips may help minimize any shedding related to minoxidil withdrawals.
- Start microneedling before quitting. Minoxidil and microneedling are synergistic treatments. Try them together for at least 3-6 months before dropping the drug.
- Don’t quit cold turkey. Follow a tapering protocol to minimize abrupt changes to the scalp environment. (We have a detailed weaning protocol in our membership.)
- Continue with alternative treatments. An effective weaning protocol takes up to 6 months. Continue with microneedling during this time.
- Replace minoxidil with natural therapies. Individuals may wish to experiment with other topicals instead, such as 2-5% rosemary oil.
For the most part, minoxidil requires lifelong use to hold onto any hair maintained or regrown. As such, shedding often occurs for 3-6 months following a stop in minoxidil application. But, we can significantly mitigate this shed by combining minoxidil with additional therapies and following a tapering protocol.
Summary
Minoxidil can be an effective treatment for androgenic alopecia, although research says when used alone, results taper off over time. Combining minoxidil with wounding therapies such as microneedling can make it more effective.
When stopping minoxidil, hair loss can be expected. Research shows losses will be greatest within the first 3-6 months of quitting but will eventually rebound to where hair counts would have been had minoxidil never been applied.
This doesn’t mean hair loss sufferers are stuck taking minoxidil for the rest of their lives. The same microneedling therapies that make minoxidil more effective may help sustain results after quitting the drug. This is especially true for those who commit to a strict tapering protocol versus quitting minoxidil cold turkey.
So should people use minoxidil?
For many, it’s worth a try. Some people will see visual improvements, some of which can be maintained with a proper weaning program. In the worst case, people will most likely end up where they would’ve been without treatment, but not worse off.
References[+]
References ↑1 https://www.jaad.org/article/S0190-9622(08)00809-8/abstract ↑2 https://pubmed.ncbi.nlm.nih.gov/9395721/ ↑3 https://www.jidonline.org/article/S0022-202X(15)42806-4/pdf ↑4 https://pubmed.ncbi.nlm.nih.gov/21524889/ ↑5 https://www.sciencedirect.com/science/article/pii/S019096229970006X ↑6 https://pubmed.ncbi.nlm.nih.gov/12196747/ ↑7 https://pubmed.ncbi.nlm.nih.gov/2180995/ ↑8 https://www.jaad.org/article/S0190-9622(08)00809-8/abstract ↑9 https://link.springer.com/article/10.1007%2Fs40257-018-0409-y ↑10 https://pubmed.ncbi.nlm.nih.gov/28078868/ ↑11 https://www.researchgate.net/publication/221695328_Minoxidil_Use_in_Dermatology_Side_Effects_and_Recent_Patents ↑12 http://www.thaiscience.info/Journals/Article/JMAT/10986429.pdf ↑13 https://www.jaad.org/article/S0190-9622(99)70006-X/fulltext ↑14 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3746236/ ↑15 https://pubmed.ncbi.nlm.nih.gov/29028377/ Minoxidil is just one of two FDA-approved hair loss drugs. But FDA-approval doesn’t necessarily equate to guaranteed results with Minoxidil. In fact, many hair loss sufferers use minoxidil (i.e., Rogaine®) for six months and still don’t see significant benefits.
Why is that? In other words, why do 50% of people seem to respond favorably to minoxidil, while the remaining 50% see little-to-no benefit?
Research suggests this split in regrowth might be tied to an enzyme in the hair follicle called sulfotransferase.
Without coming into contact with sulfotransferase, Minoxidil won’t have an effect, and about 40% of men just don’t have enough sulfotransferase to elicit a response to Minoxidil.
Minoxidil is a pro-drug, meaning it has to be activated before it can exert its effects. Sulfotransferase plays an irreplaceable role in this because it turns minoxidil (its pro-drug form) into minoxidil sulfate (its active form).
We call this a rate-limiting step in the response rate to topical minoxidil, meaning the individual activity of the sulfotransferase enzymes on your scalp will predict your response rate to minoxidil.
This enzyme is also found in the liver. When oral minoxidil is ingested, it passes through these sulfotransferase enzymes, where it’s then distributed to the hair follicles throughout the body.
Interested in Topical Minoxidil?
High-strength topical minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.
When Can Responders Expect to See Visible Regrowth from Minoxidil?

Olsen, E. A., Dunlap, F. E., Funicella, T., Koperski, J. A., Swinehart, J. M., Tschen, E. H., & Trancik, R. J. (2002). A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men. Journal of the American Academy of Dermatology, 47(3), 377 385.
First, let’s talk about the event horizon for Minoxidil. With Minoxidil, results can be expected a little faster than Finasteride, so typically shedding is experienced between two and four months, but then re-growth is usually cosmetically perceptible around the one month to six-month mark. This makes sense, as Minoxidil acts more like a stimulant, or growth agonist.
Minoxidil turns more hairs on; it doesn’t necessarily target miniaturization. So Minoxidil doesn’t have as dramatic of an impact on reversing hair miniaturization and thereby improving hair thickness, but it can help to create a denser, fuller head of hair.
For those looking to reverse hair thinning, here are three ways to enhance the effectiveness of minoxidil treatment.
1. Acute Wound Generation via Microneedling
One of the easiest ways to enhance the efficacy of minoxidil is through acute wound generation, which is best administered through microneedling and massage.
Microneedling plus Minoxidil seems to elicit a four-fold greater effect of hair count increases than just Minoxidil alone.
Microneedling elicits growth factors, signaling proteins and enzymatic activity of sulfotransferase. Microneedling may also increase topical absorption and potentially even attenuate scarring – all of which pair well with minoxidil use.
Researchers started testing minoxidil + microneedling as a combination treatment back in 2013 – with incredible results.

One study showed over 12 weeks, minoxidil+ microneedling increased minoxidil efficacy four-fold and led to a 40% increase in hair count – with real, visual hair changes.[1]http://www.ijtrichology.com/article.asp?issn=0974-7753;year=2013;volume=5;issue=1;spage=6;epage=11;aulast=Dhurat
More recently, this study showed that over 6 months, minoxidil + microneedling had a 100% response rate and led to a 25% increase in hair count.[2]https://www.tandfonline.com/doi/abs/10.1080/14764172.2017.1376094?journalCode=ijcl20
It’s suspected that these improvements are due to microneedling’s ability to:
1 – Enhance skin enzymes required to activate minoxidil (i.e., sulfotransferase),
2 – Improve the absorbability of topicals like minoxidil – since the wounding allows for easier access to hair follicles and their blood supply, and
3 – Potentially attenuate or partially reverse fibrosis.
As with microneedling, Perfect Hair Health’s standardized scalp massages may help responders increase hair counts.
2. Switch to higher concentrations
Studies show that minoxidil non-responders see better hair growth after switching to 10% or 15% minoxidil. One such study was conducted on women with female pattern hair loss who were non-responders to 5% Minoxidil. They were trialed with 15% Minoxidil topically, and 70-80% of them saw a significant response. Participants saw an average of about 13% increase in hair counts.[3]https://clinicaltrials.gov/ct2/show/NCT02486848
So moving from 5% as a non-responder to 15% can really improve results.
Anecdotally, 15% Minoxidil is relatively safe. There’s not a ton of data on it, but when looking at the half-lives of Minoxidil, its transfusion into the system, and how much circulates from topical application, it doesn’t seem like there’s a massive uptake in the systemic volume of Minoxidil from going from 5% to 15%, at least from a biological perspective.
3. Add in topical retinol / retinoic acid
Another way to improve sulfotransferase activity? Using Tretinoin or Retinoic Acid. These are Vitamin A derivatives that help to activate sulfotransferase activity, stimulate a little bit of inflammation and cell turnover and in doing so, make minoxidil way more effective.
Topical minoxidil is delivered as a “pro-drug” – meaning that it is not technically active when it touches the scalp skin. Rather, minoxidil has to come into contact with an enzyme called sulfotransferase.
Unfortunately, many men and women don’t have enough sulfotransferase activity in the skin to elicit a major hair change with minoxidil alone. Fortunately, adding in topical retinol / retinoic acid can increase the activation of sulfotransferase, and thereby minoxidil – potentiating even bigger hair gains.
Just a few short years ago, hair loss sufferers had to ask their doctor to write a prescription for Vitamin A derivatives. There are brands online that sell combination formulas – like Happy Head, Adegen®, and MinoxidilMax. No doctor visit is required.
These companies sell products, but are these companies actually legitimate? Do their products actually contain the advertised ingredients? How do these formulas stand up to our rigorous lab tests? Join the Perfect Hair Health Membership Program to find out.

Summary
About 60% of people seem to be hyper-responders to Minoxidil. They see great hair count increases, and usually, they’ll see this in the first six months of treatment. Then those hair count increases will steadily decline over time. For the other 40% of people who try Minoxidil, there’s zero effect.
For high-responders, there is utility in taking a more multifactorial approach to Minoxidil treatment, where microneedling, high-concentration Minoxidil, and retinoic acid are combined to accelerate hair growth.
References[+]
Stool transplants – also known as fecal microbiota transplants (FMT) – are a controversial therapy reserved for life-threatening bacterial infections and autoimmune disorders. Fascinatingly, people who’ve undergone stool transplants have later reported unintended benefits: weight loss, less acne, personality improvements, and even hair regrowth.
At face value, a connection between stool transplants and hair loss sounds like science fiction. How could altering the bacteria inside of our guts affect hair growth on top of our scalps?
At the same time, new research suggests that the hair loss-fecal microbiota connection is very real, and may even become a future therapeutic target for people looking to regrow hair.
In this article, we’ll dive into the science surrounding stool transplants: what this therapy is, what it does to our gut microbiome, and the evidence linking fecal microbiota transplants to hair regrowth in alopecia areata, telogen effluvium, and maybe even androgenic alopecia.
We’ll even showcase a few before-after photos featured in studies and forums from people who received stool transplants to treat unrelated health conditions, and ended up (accidentally) experiencing hair regrowth.
If you have any questions, feel free to reach us in the comments below.
Table of contents
All-Natural Hair Supplement + Topical
The top natural ingredients for hair growth, all in one serum & supplement.
Take the next step in your hair growth journey with a world-class natural serum & supplement. Ingredients, doses, & concentrations built by science.

What is a fecal microbiota transplant (i.e., stool transplant)?
Our guts are like a storage facility for large colonies of microbes. Because of the role the gut microbiome encompasses, many diseases and conditions that relate to a dysfunctional gut microbiome, have now been treated utilizing a fecal microbiota transplant.
An artist’s rendering of gut organisms and debris

A fecal microbiota transplant (FMT) is basically what it sounds like: the transfer of stool from one individual’s colon into another person. The aim? To improve gut bacteria density and diversity. In other words: increase the total number of “good” bacteria in the gut, as well as the number of “good” species.
Stool transplants – or FMTs – are nothing new. This practice has been around since the 4th century. More recently, it gained notoriety when the FDA approved FMTs for recurrent Clostridium difficile infections – a deadly bacterial infection that often grows resistant to antibiotics [1].
In this context, FMT’s are incredibly successful. For a benchmark, antibiotic treatments for C. difficile tend to boast a 20-30% remission rate. FMTs boast around a 90% remission rate [2]. In the veterinary world, FMT’s are used for similar purposes [3].
While the use of a FMT seems most pertinent to gastrointestinal diseases, there is a much broader spectrum for the therapy in relation to other conditions, such as multiple sclerosis, Alzheimer’s disease, epilepsy, obesity, and metabolic syndrome (to name only a few) [4, 5].
Can fecal microbiota transplants alter our gut microbiome?
FMTs are perhaps one of the most powerful ways to alter our gut microbiome: the collection of bacteria inside our intestines that help regulate anything from autoimmune reactions to hormonal levels to nutrient metabolism.
C. difficile & stool transplants: alterations to gut flora
In one study, researchers decided to investigate 55 stool samples from donors and recipients who used FMTs as a treatment for C. difficile infections. They found major differences in the pre- versus post-procedure samples of the recipients [6].
Before the procedure, healthy donors’ stools contained a significant portion of the phylum of bacteria – known as Firmicutes and Bacteroides – constituting roughly 85% of bacteria identified.
We can first think of a phylum as the link between different species of bacteria. For example, while an oak tree differs from a palm tree, ultimately, they’re still all trees. As such, no one group can be labeled as good or bad as often the species within those groups can exhibit both helpful and disruptive properties. This is evident with helminth infections – where the same helminth can cause inflammation in the first-world but protect from malaria in the developed world. To put it simply: the effects of a bacteria often rely on its environment, the health of an individual, the ratio of that bacteria to others, and about a billion other factors [7,8].
However, in the case of resistant Clostridium infections, Firmicutes and Bacteroides tend to be absent. This suggests that these phylum may play a role in preventing gut dysbiosis and thereby C. difficile overgrowths.
With respect to the study, here’s what researchers found:
- Prior to the stool transplants, recipients’ stools had lower amounts of Firmicutes and Bacteroides and markedly high Fusobacteria and Proteobacteria.
- Donor stool contained exceptionally higher Firmicutes and Bacteroides, as well as lower Fusobacteria and Proteobacteria.
- After treatments, recipients’ stool showed the higher Firmicutes and Bacteroides as well as lower Fusobacteria and Proteobacteria (thereby more closely resembling that of the donor’s gut).
- After transplantation, the more closely a recipient’s gut matched that of its donor, the more likely that recipient was to experience a remission from C. difficile.
In other words, FMTs significantly altered gut flora – and to the benefit of sick patients.
Interestingly, the health of our gut microbiome is linked to many hair loss disorders – particularly alopecia areata and telogen effluvium. Moreover, research now links gut bacteria to the regulation of DHT – the hormone implicated in pattern hair loss.
We’ll dive into this evidence below: what it is, what it means, and why it might rewrite a lot of what we think we know about hair loss.
Stool transplants for hair loss: the evidence
When it comes to FMTs as a treatment for hair loss, evidence is very limited. This is because reports of fecal transplants and hair regrowth have mainly happened by accident – specifically, after a patient with C. difficile + hair loss receives a stool transplant and later inadvertently sees improvements to both conditions.
Nonetheless, there is compelling evidence of a gut microbiome-hair loss connection. To best outline this evidence, we’ll dive into the research on FMT’s and hair loss as organized by :
- Alopecia Areata
- Telogen Effluvium
- Androgenic Alopecia
Let’s begin.
Alopecia areata and fecal microbiota transplants
Alopecia areata (AA) is an autoimmune form of hair loss; it often presents as patchy-related hair loss in the scalp. Researchers currently believe AA is the result of a collapse in “immune privilege” of the hair follicles – whereby the immune system begins to read hair follicles as foreign invaders, and then starts to attack them.
Alopecia areata: patchy hair loss

When it comes to stool transplants, alopecia areata is the best-studied form of hair loss. This isn’t saying much – because there’s not a ton of data on stool transplants and hair regrowth in general. Again, the studies here have been unintended and inadvertent: people with alopecia areata seem to have higher rates of gut dysbiosis, and thereby they seem to suffer disproportionately from infections like C. difficile. Therefore, they’re probably more likely to eventually become eligible for extreme treatments like a stool transplant – which is why we have case reports of FMTs and AA-related regrowth in the first place.
So, what limited evidence do we have on stool transplants for hair regrowth from alopecia areata?
Case reports of FMTs and hair regrowth from alopecia areata
Study #1: two uncontrolled retrospective case reports
In a study where two patients received an FMT for treating Clostridium difficile, researchers reported that both people saw an unintended benefit of hair regrowth following the procedure [14]. In these cases, both patients were classified as having alopecia universalis – an advanced form of alopecia areata where the hair loss has progresses beyond the scalp and to the body.
In the first case, the 38-year old man began to grow peach fuzz not only on his head, but also his face and arms. The regrowth became cosmetically noticeable 8 weeks after the stool transplant – after having suffered from progressive alopecia universalis for decades without any improvements.
In the second case, a 20-year old man – diagnosed with alopecia universalis 2 years prior to his FMT – saw major improvements to scalp hair regrowth over a 1.5-year period after receiving a stool transplant. Prior to the FMT, this subject had tried to treat his alopecia using corticosteroid injections, topical steroids, squaric acid, and laser treatments— all to no avail. While this man also received steroid injections within his scalp after the FMT, he began to grow hair throughout the rest of his body as well, even where had not received a steroid injection [21].

Study #2: a case report of FMT + hair regrowth in an elderly patient with diffuse alopecia areata
In a second study investigating FMT’s effects on an elderly man (86-year old) with diffuse alopecia areata, researchers found some unexpected benefits [15]. Originally, FMT was used to treat his intestinal disorders (with success). However, alongside the treatment of his other digestive ailments, his hair thickness began to return. What’s more, his previously gray hair had regrown as its original color.

These are just three case reports. That’s not really “overwhelming” evidence…
You’re right! We always have to evaluate any intervention in respect to its quality and quantity of evidence. In regard to FMT and alopecia areata, the quality and quantity of evidence is low: three uncontrolled, retrospective case reports.
Having said that, we also have to recognize that the total number of alopecia areata patients who (1) develop C. difficile, and (2) have it progress to the severity where they become eligible for an FMT – is also low. On that note, the evidence here has excited other research teams enough to launch a clinical trial on FMT and alopecia areata – the results of which will (hopefully) be available in the coming year.
So, needless to say, the preliminary evidence (and mechanistic data) supporting a connection between is FMT and AA-related regrowth is exciting enough to continue exploring.
How might FMT’s improve alopecia areata?
Alopecia areata is mainly categorized by an autoimmune attack on the hair follicles. This is predominantly mediated by a group of immune cell known as T-cells. Specifically, a type of T-cell known as TH17 [16].
Not surprisingly, TH17 is a major contributor to intestinal conditions that manifest as inflammation. Since the gut is our largest site of immune cell concentration, then by altering the gut microbiome to a more favorable anti-inflammatory profile, we may be able to alter T-cell activity throughout the rest of our body.
In fact, studies have shown that modulating the microbiome to favor this anti-inflammatory profile can nearly shutdown TH17 cell activity [17]. By this very same mechanism, it is possible that a more widespread shutdown of TH17 could alleviate a TH17-mediated attack on hair follicles – even at the top of the scalp.
Furthermore, there is an established link between inflammatory bowel disease and alopecia areata [18]. The implication: an unhealthy microbiome may drive both inflammatory bowel disease and alopecia areata. After all, patients with alopecia areata and inflammatory bowel conditions who undergo FMT seem to inadvertently regrow hair – and at a consistency worth noting by investigators.
Summary so far: Alopecia areata (AA) is an autoimmune form of hair loss; it’s likely driven by the over-activation of T-cells, and specifically, TH17 cells. Interestingly, patients with AA who’ve undergone stool transplants (FMTs) to treat C. difficile infections have inadvertently regrown hair. The gut microbiome is the body’s largest site of immune cell concentration – and thereby TH17 activation. So, it’s plausible that FMTs might dampen TH17 immune activation – all by restoring gut microflora balance to a more commensal state.
Telogen effluvium and stool transplants
Telogen effluvium (TE) is a temporary form of hair loss that is characterized by a dysregulation of the hair cycle.
This can occur in many ways: for instance, too many hairs can “shed” prematurely, or there can be a delay between when a hair sheds out and when a new hair grows in (to start a new hair cycle). This often presents as diffuse thinning, or sometimes even region-specific shedding (oftentimes the hairline for women).
A hair loss patient with suspected telogen effluvium (TE)

What causes telogen effluvium (TE)?
Telogen effluvium (TE) is sort of like a catch-all diagnosis for a wide array of hair loss triggers. But the main drivers of TE are often considered (1) stress (emotional or physical), (2) nutrient imbalances, and (3) chronic conditions (i.e., hypothyroidism, heavy metal toxicities, etc.).
Currently, there are no studies investigating a link between FMTs and TE. However, there is mechanistic evidence that FMTs may help address some (of the many) underlying factors leading to TE.
For example, nutrient deficiencies – namely, iron, zinc, and/or vitamin D – have been associated with telogen effluvium [20]. Given that evidence implicates the state of the microbiome in nutrient absorption, it’s possible that disruptions to the microbiome may result in poor nutrient absorption and, consequently, telogen effluvium-related hair shedding [21].
Research has also found elevated cadmium levels in some people with TE – a trace element that may trigger hair shedding if consumed in excness [22]. Most interesting, though, is that excessive cadmium has also been shown to alter the gut microbiome of mice in a way that directly mirrors individuals plagued by antibiotic-resistant Clostridium difficile infections… the exact condition FMT is designed to treat [23].
Altogether, direct (i.e., by bacterial infection) or indirect (i.e., by excess cadmium) changes to the microbiome, both of which seem to be associated with telogen effluivum, may benefit from FMT.
Summary so far: Telogen effluvium (TE) is a temporary form of hair loss caused by a disruption to the hair cycle – oftentimes resulting from stress, nutrient imbalances, or a chronic condition. While no evidence directly implicates stool transplants as a therapeutic procedure for TE, there is mechanistic data showing that our gut microbiome has the capacity to improve chronic conditions as well as the synthesis of vitamins commonly found as deficient in TE patients. Therefore, it’s possible that stool transplants might help TE by addressing its underlying causes. But again, we’re extrapolating here!
Androgenic alopecia and fecal transplants
Androgenic alopecia (AGA) is one of the world’s most common hair loss disorders – affecting at least 50% of women and 80% of men throughout a lifetime. Its often characterized by progressive hair follicle miniaturization, whereby affected hair follicles get thinner and thinner over a series of hair cycles. It presents most commonly across the top of the scalp as temple recession + a bald spot in men, and diffuse thinning in most women.
Androgenic alopecia in a male: temple recession
What causes androgenic alopecia (AGA)?
While all of the causes aren’t fully elucidated, most researchers agree that AGA is caused by a combination of male hormones and genetics, and possibly the scalp’s environment (i.e., inflammatory microorganisms, the contraction of muscles surrounding the scalp perimeter, inflammation-mediated tension, etc.).
Specifically, the hormone dihydrotestosterone (DHT) seems to overexpress in balding scalp regions. In vitro studies demonstrate that DHT may trigger premature shedding, inflammatory signaling proteins, and cell death in dermal papillae cells (the “powerhouse” of the hair follicle) – all of which can lead to progressive hair follicle miniaturization. Moreover, studies have shown that men without DHT do not go bald, and that reducing DHT can help prevent (and partially reverse) the balding process.

Is there evidence that stool transplants can improve pattern hair loss (AGA)?
Clinical evidence? No. Mechanistic evidence? Yes. Anecdotes of AGA improvements after stool transplants? Yes – even with photos. We’ll uncover all of this below.
First, to our knowledge, no case reports or clinical trials investigating the benefits of FMT have occurred. Nonetheless, the absence of evidence doesn’t imply evidence against a therapy (remember: FMTs are a very limited intervention). On that note, there are anecdotes online of people with AGA regrowing their hair (accidentally) following a fecal transplant.
One anecdote comes from a male forum user who suffered simultaneously from both irritable bowel syndrome (IBS) and AGA. In the past, he’d tried to treat his AGA with finasteride. Unfortunately, he did not see any improvements, so he stopped using the drug.
In search for a way to improve his IBS, he later stumbled upon the evidence supporting fecal microbiota transplants to treat C. difficile, Crohn’s disease, and gut dysbiosis. His symptoms were severe enough that he ended up tracking down a willing practitioner and giving the therapy a try – potentially outside of legal means.
A week after the therapy, he reported that his hair shedding dramatically decreased. A year later, he reported significant hair thickening (and potential regrowth)… regrowth that occurred outside of any drug interventions or hair growth therapies.
AGA-related hair regrowth one-year after a stool transplant

This anecdote is promising. But again, it’s just the experience of one person. Beyond this report, are there any other examples?
When it comes to fecal microbiota transplants – we couldn’t find any other anecdotes of hair regrowth from AGA. But interestingly, we were able to find reports of hair regrowth (with photos) from people adhering to incredibly restrictive diets that completely revamp gut microflora constitutions.
One such diet is the carnivore diet – whereby someone nearly completely restricts carbohydrate and fiber intake and begins to subsist entirely off of meat. It sounds like a crazy diet (and it just might be). However, it’s also the only diet where I’ve actually seen people regrow hair lost due to androgenic alopecia. For instance:
- A 1928 case report detailed two men under clinical observation for an entire year while eating only meat. One observation from the investigation team? One of the men saw a complete stop in the progression of his pattern hair loss.
- Some members of our community (who have failed to see success with drugs like finasteride) have later opted to adopt the carnivore diet as an experiment for health. A few of these members have reported hair regrowth.
For an example – take Brian (a member of our community). He’d tried finasteride for two years, saw zero improvements, and then eventually quit the drug. Later, he and his wife decided to try the carnivore diet. Simultaneously, he also started to incorporate our scalp massages to see if that would improve his hair loss (since finasteride didn’t work).
One year later, he’d noticed significant hair regrowth at hairline, as well as overall hair thickening. Here were his results.
AGA-related hair regrowth one-year after the carnivore diet + massaging

Interestingly, preliminary evidence suggests that the carnivore diet may increase gut microorganism biodiversity – one of the objectives of FMT. It may also reduce the totality of bacteria inside the gut – since these microorganisms feed off carbohydrate and fiber (two things that are nearly eliminated on a diet consisting of all meat).
Moreover, the carnivore diet eliminates a lot of inflammatory food groups (i.e., FODMAPs) that might contribute to systemic inflammation for sensitive individuals. This may help reduce the number of pathogenic bacteria residing in the gut, as well [27].
This leads to some interesting discussion points about a possible connection between AGA, stool transplants, the carnivore diet, and subsequent changes to the microbiome that could improve hair loss outcomes. We’ll explore these below.
Mechanisms: how might stool transplants improve pattern hair loss?
There’s evidence that our microbiome may help regulate our endocrine system (i.e., the balance of our sex hormones). More specifically, our microbiome may play a direct role in the metabolism of androgens – the sex hormone implicated in AGA.
To start, here’s a quick overview on how hormone metabolism works:
- Once circulating hormones have “completed” a task, they reach the liver. The liver is where free hormones (i.e., the active, unbound hormones) in our blood are processed to later become excreted.
- The liver conjugates these free hormones. Simply put, the livers converts the structure of these hormones from lipophilic (i.e., fat-loving) to hydrophilic (i.e., water-loving). This does two things: it makes the hormone less potent, and it increases that hormone’s chances of entering the digestive tract (i.e., small and large intestine) where they can get excreted.
- Once these conjugated forms of hormones enter the digestive tract, the body excretes these conjugates or metabolites in the stool and urine.
Put simply, our liver conjugates active hormones, those hormones enter our digestive tract, then our digestive tract flushes those hormones out of the body.
But here is where things get interesting: some of our gut bacteria produce an enzyme called beta-glucuronidase. This enzyme has the ability to reverse the process of hormone excretion. Specifically, when conjugated forms of hormones come into contact with beta-glucuronidase, those hormones become unconjugated. In other words, they reconvert back into an active (i.e., unbound) form – where they can potentially reenter our circulatory system.
So, if gut bacteria have the ability to act as gatekeepers for hormone excretion and reabsorption, what does this have to do with AGA?
Fascinatingly, research in healthy men has demonstrated that free dihydrotestosterone (DHT) – the hormone implicated in AGA – exists at levels in the colon at levels 70-fold higher than free DHT found in the blood [24].
This suggests (at least) two things:
- Serum levels of DHT represent just a tiny fraction of total DHT within our body.
- If this free DHT can exit the digestive tract and reenter the circulatory system, this means that gut bacteria might act as a gatekeeper for androgen excretion / reabsorption… and that our microflora might be directly implicated in androgenic-linked conditions: heart disease, prostate enlargement, and maybe even pattern hair loss.
It’s already been shown that gut bacteria have a directly influence on steroid levels. In fact, in the case of periodontal disease and gingivitis, certain cultured bacterial species can actually increase levels of testosterone and DHT [25]. Moreover, researchers have linked this increase to the development of inflammation in periodontitis itself.
Free DHT (as opposed to conjugated DHT) is the type of DHT that likely elicits the majority of DHT-mediated effects on the body. This includes supporting the processes that lead to AGA. You can learn more about this here.
Can unconjugated DHT (in the gut) reenter the circulatory system?
No studies have demonstrated this. But to our knowledge, no studies have actually asked this question (to our knowledge). Not to sound like a broken record, but the absence of evidence cannot imply evidence against something.
It’s worth noting that gut bacteria can produce (and recirculate) estrogens. So, it’s not out of the realm of possibilities that DHT can also be recirculated. In fact, it’s more likely than not.
Moreover, studies on patients with post-finasteride syndrome (long-lasted sexual dysfunction and/or cognitive disorders after cessation of finasteride) show marked gut microbiota alterations [26]. Researchers believe that these microbiota alterations may possibly contribute to the symptoms of finasteride syndrome.
Of course, there are still no clear connections between post-finasteride syndrome and these microbiome alterations. However, if free DHT levels in the colon contribute to overall DHT levels and finasteride results in prolonged changes to the population of these bacteria, it’s possible that reduced colon DHT may contribute to blood DHT, and, thereby the symptoms of post-finasteride syndrome.
Similarly, the opposite could also prove true: if colonic DHT influences blood DHT levels (in an upwards or downwards direction), then anything that increases the total number of our gut bacteria might also increase DHT levels.
Whether this affects scalp DHT (and thereby AGA) – we just don’t know. But we do find these anecdotes of stool transplants and/or carnivore diets regrowing hair absolutely fascinating. After all, both interventions likely lead to improvements in gut biodiversity and changes to the total number of commensal / pathogenic microflora. Therefore, they likely alter DHT activity in the gut. But whether these effects extend to our scalp hair – we can’t yet say (aside from admiring those before-after photos and “hoping” that, after all these years, it’s just that easy to reverse AGA).
Summary so far: Androgenic alopecia (AGA) is driven by a combination of genes and androgens. Interestingly, some patients who’ve undergone stool transplants have later reported hair thickening from AGA without any other treatments. The main hormone implicated in AGA is dihydrotestosterone (DHT). Recent research has found that gut bacteria can actually produce DHT, and even convert it from an inactive to active form. Moreover, researchers recently discovered that free DHT is found in stool samples at levels 70-fold greater than in the blood supply. It has been demonstrated that gut microorganisms influence estrogen production, and the amount of estrogen circulating in our blood. Therefore, it’s not unreasonable to assume that gut flora may also act as gatekeepers for DHT activation between the gut and the circulatory system. If true, this may directly implicate gut bacteria in the pathogenesis of AGA.
Fecal microbiota transplants: undergoing the procedure
What’s it like to do a fecal microbiota transplant?
While FMT may sound like a cure-all for all autoimmune ailments, it’s worth mentioning that research here is still in its infancy, and there’s always the very real possibility that a transplant won’t work or might worsen your symptoms due to unforeseen interactions between donor and recipient microflora.
In the US and Europe, strict guidelines are set to screen a potential donor for any negative attributes that could trigger unwanted side effects for the recipient. There is a questionnaire that is given, stool sample analysis is performed approximately four weeks prior, and blood samples taken [1], followed by an additional interview at the time of the donation. Preferably, you would want a stool sample from someone close to you, with whom you may have shared a common environment. This reduces the chances of any unwanted immune reactions that may occur.
Any failure in the proper preparation of the FMT can present with complications such as bacteremia (i.e., bacteria in the bloodstream) or hospitalizations. Other mishaps such as perforations can occur, but tend to be attributed to the tools and technicians rather than infectious agents [10].
Usually, preparations of the fecal material are done up to six hours before the procedure. The sample is frozen, then thawed out, and, finally mixed with a solution to deliver in a syringe.
It’s also been shown that the size of the sample matters dramatically. Usually, sample sizes are around 50g, which is no more than a few teaspoons. With difficult to treat clostridium infections, larger sample sizes have demonstrated better efficacy and reduced chances chances of failure with the treatment [11]. Many times, FMT requires multiple treatment sessions as well for optimal results.
An important (and interesting) aspect of the procedure is the fact that antibiotics are not to be given to the recipient within 48-hours [12]. While this may seem like an obvious aspect of FMT, this also points to the possibility that it actually is the bacteria present within the stool itself that produces results… not another confounding variable such as immune molecules, proteins, or other components.
Even more supportive of that notion: studies have shown when the procedure is given to the lower digestive tract, (which is also where a majority of the gut microbiome resides), results are drastically better than when administered in the upper digestive tract [1].
Is there a way around the “yuck factor” of FMT?
The idea of taking someone else’s fecal material and implanting it inside of your colon isn’t exactly appealing. And while a lot of the hesitancy is likely psychological, it’s reasonable to ask if there’s a way to do an FMT without doing an enema.
Yes. Researchers have shown that oral capsules produced results on par with the procedure itself – at least in the treatment of resistant Clostridium infections [13]. Obviously, oral supplementation may come across as even less appealing to some. Tto others, the possibility of supplementation certainly reduces the “barrier to entry”.
Summary: stool transplants for hair loss
By regulating the gut microbiome and reducing gut inflammation, a fecal microbiota transplant may improve hair loss outcomes for alopecia areata, telogen effluvium, and perhaps even androgenic alopecia.
Evidence on stool transplants and hair regrowth is incredibly limited. Our knowledge base comes from:
- Four case reports demonstrating significant hair regrowth across patients with autoimmune forms of hair loss
- Anecdotes from people who’ve undergone stool transplants for gut dysbiosis and later reported inadvertent hair regrowth
- Mechanistic data revealing possible connections between stool transplants, the gut microbiome, DHT production, and immunological changes – as well as their overlap with common hair loss disorders.
Nonetheless, I personally find this arena of research fascinating, and I hope it rapidly expands.
In the meantime, please note that we’re not recommending stool transplants as a first-line of defense for any hair loss disorder. If you’re interested in getting one, you’ll need to connect with a qualified physician – we’re not in a position to help you here.
You can reach us in the comments any time!
References
- Wang, J.-W., Kuo, C.-H., Kuo, F.-C., Wang, Y.-K., Hsu, W.-H., Yu, F.-J., … Wu, D.-C. (2018). Fecal microbiota transplantation: Review and update. Journal of the Formosan Medical Association. doi:10.1016/j.jfma.2018.08.011
- van Nood E, Vrieze A, Nieuwdorp M, Fuentes S, Zoetendal EG,de Vos WM, et al. Duodenal infusion of donor feces for recur-rent Clostridium difficile.N Engl J Med2013;368:407e15.
- Pereira GQ, Gomes LA, Santos IS, Alfieri AF, Weese JS, Costa MC. Fecal microbiota transplantation in puppies with canine parvovirus infection. J Vet Intern Med. 2018 Mar;32(2):707-711. doi: 10.1111/jvim.15072. Epub 2018 Feb 20. PMID: 29460302; PMCID: PMC5867004.
- [Vendrik, K., Ooijevaar, R. E., de Jong, P., Laman, J. D., van Oosten, B. W., van Hilten, J. J., Ducarmon, Q. R., Keller, J. J., Kuijper, E. J., & Contarino, M. F. (2020). Fecal Microbiota Transplantation in Neurological Disorders. Frontiers in cellular and infection microbiology, 10, 98. https://doi.org/10.3389/fcimb.2020.00098
- Vrieze A, Van Nood E, Holleman F, Salojärvi J, Kootte RS, Bartelsman JF, Dallinga-Thie GM, Ackermans MT, Serlie MJ, Oozeer R, Derrien M, Druesne A, Van Hylckama Vlieg JE, Bloks VW, Groen AK, Heilig HG, Zoetendal EG, Stroes ES, de Vos WM, Hoekstra JB, Nieuwdorp M. Transfer of intestinal microbiota from lean donors increases insulin sensitivity in individuals with metabolic syndrome. Gastroenterology. 2012 Oct;143(4):913-6.e7. doi: 10.1053/j.gastro.2012.06.031. Epub 2012 Jun 20. Erratum in: Gastroenterology. 2013 Jan;144(1):250. PMID: 22728514.
- Yoon H, Shim HI, Seol M, Shin CM, Park YS, Kim N, Lee DH. Factors Related to Outcomes of Fecal Microbiota Transplantation in Patients with Clostridioides difficile Infection. Gut Liver. 2021 Jan 15;15(1):61-69. doi: 10.5009/gnl20135. PMID: 32839363.
- Leimbach A, Hacker J, Dobrindt U. E. coli as an all-rounder: the thin line between commensalism and pathogenicity. Curr Top Microbiol Immunol. 2013;358:3-32. doi: 10.1007/82_2012_303. PMID: 23340801.
- Renga G, Bellet MM, Stincardini C, Pariano M, Oikonomou V, Villella VR, Brancorsini S, Clerici C, Romani L, Costantini C. To Be or Not to Be a Pathogen: Candida albicans and Celiac Disease. Front Immunol. 2019 Dec 5;10:2844. doi: 10.3389/fimmu.2019.02844. PMID: 31867008; PMCID: PMC6906151.
- Flannigan, K. L., Rajbar, T., Moffat, A., McKenzie, L. S., Dicke, F., Rioux, K., Workentine, M. L., Louie, T. J., Hirota, S. A., & Greenway, S. C. (2017). Changes in Composition of the Gut Bacterial Microbiome after Fecal Microbiota Transplantation for Recurrent Clostridium difficile Infection in a Pediatric Heart Transplant Patient. Frontiers in cardiovascular medicine, 4, 17. https://doi.org/10.3389/fcvm.2017.00017
- [Dailey, F. E., Turse, E. P., Daglilar, E., & Tahan, V. (2019). The dirty aspects of fecal microbiota transplantation: a review of its adverse effects and complications. Current Opinion in Pharmacology, 49, 29–33. doi:10.1016/j.coph.2019.04.008
- Cammarota, G., Ianiro, G., Tilg, H., Rajilić-Stojanović, M., Kump, P., Satokari, R., Sokol, H., Arkkila, P., Pintus, C., Hart, A., Segal, J., Aloi, M., Masucci, L., Molinaro, A., Scaldaferri, F., Gasbarrini, G., Lopez-Sanroman, A., Link, A., de Groot, P., de Vos, W. M., … European FMT Working Group (2017). European consensus conference on faecal microbiota transplantation in clinical practice. Gut, 66(4), 569–580. https://doi.org/10.1136/gutjnl-2016-313017
- William M. Tauxe, MST, Tanvi Dhere, MD, Angela Ward, MSN, FNP, Lori D. Racsa, DO, Jay B. Varkey, MD, Colleen S. Kraft, MD, MSc, Fecal Microbiota Transplant Protocol for Clostridium Difficile Infection, Laboratory Medicine, Volume 46, Issue 1, Winter 2015, Pages e19–e23, https://doi.org/10.1309/LMCI95M0TWPDZKOD
- Kao D, Roach B, Silva M, Beck P, Rioux K, Kaplan GG, et al.Effect of oral capsule- vs colonoscopy-delivered fecal micro-biota transplantation on recurrent Clostridium difficile infec-tion: a randomized clinical trial.JAMA2017;318:1985e93.
- Rebello, D., Wang, E., Yen, E., Lio, P. A., & Kelly, C. R. (2017). Hair Growth in Two Alopecia Patients after Fecal Microbiota Transplant. ACG case reports journal, 4, e107. https://doi.org/10.14309/crj.2017.107
- [Xie, W. R., Yang, X. Y., Xia, H. H., Wu, L. H., & He, X. X. (2019). Hair regrowth following fecal microbiota transplantation in an elderly patient with alopecia areata: A case report and review of the literature. World journal of clinical cases, 7(19), 3074–3081. https://doi.org/10.12998/wjcc.v7.i19.3074
- Loh SH, Moon HN, Lew BL, Sim WY. Role of T helper 17 cells and T regulatory cells in alopecia areata: comparison of lesion and serum cytokine between controls and patients. J Eur Acad Dermatol Venereol. 2018 Jun;32(6):1028-1033. doi: 10.1111/jdv.14775. Epub 2018 Jan 17. PMID: 29283462.
- [Pandiyan, Pushpa & Bhaskaran, Natarajan & Zou, Mangge & Schneider, Elizabeth & Jayaraman, Sangeetha & Huehn, Jochen. (2019). Microbiome Dependent Regulation of Tregs and Th17 Cells in Mucosa. Frontiers in Immunology. 10. 426. 10.3389/fimmu.2019.00426.
- Maghfour J, Olson J, Conic R, R, Z, Mesinkovska N, A: The Association between Alopecia and Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Dermatology 2021. doi: 10.1159/000512747
- Ojuawo A, Keith L. The serum concentrations of zinc, copper and selenium in children with inflammatory bowel disease. Cent Afr J Med. 2002 Sep-Oct;48(9-10):116-9. PMID: 14562534.
- Asghar, F., Shamim, N., Farooque, U., Sheikh, H., & Aqeel, R. (2020). Telogen Effluvium: A Review of the Literature. Cureus, 12(5), e8320. https://doi.org/10.7759/cureus.8320
- Krajmalnik-Brown, R., Ilhan, Z. E., Kang, D. W., & DiBaise, J. K. (2012). Effects of gut microbes on nutrient absorption and energy regulation. Nutrition in clinical practice : official publication of the American Society for Parenteral and Enteral Nutrition, 27(2), 201–214. https://doi.org/10.1177/0884533611436116
- [Abdel Aziz AM, Sh Hamed S, Gaballah MA. Possible Relationship between Chronic Telogen Effluvium and Changes in Lead, Cadmium, Zinc, and Iron Total Blood Levels in Females: A Case-Control Study. Int J Trichology. 2015 Jul-Sep;7(3):100-6. doi: 10.4103/0974-7753.167465. PMID: 26622152; PMCID: PMC4639951.
- He X, Qi Z, Hou H, Qian L, Gao J, Zhang XX. Structural and functional alterations of gut microbiome in mice induced by chronic cadmium exposure. Chemosphere. 2020 May;246:125747. doi: 10.1016/j.chemosphere.2019.125747. Epub 2019 Dec 24. PMID: 31891852.
- Colldén, H., Landin, A., Wallenius, V., Elebring, E., Fändriks, L., Nilsson, M. E., Ryberg, H., Poutanen, M., Sjögren, K., Vandenput, L., & Ohlsson, C. (2019). The gut microbiota is a major regulator of androgen metabolism in intestinal contents. American journal of physiology. Endocrinology and metabolism, 317(6), E1182–E1192. https://doi.org/10.1152/ajpendo.00338.2019
- Soory M. Bacterial steroidogenesis by periodontal pathogens and the effect of bacterial enzymes on steroid conversions by human gingival fibroblasts in culture. J Periodontal Res. 1995 Mar;30(2):124-31. doi: 10.1111/j.1600-0765.1995.tb01261.x. PMID: 7776153.
- Borgo, F., Macandog, A. D., Diviccaro, S., Falvo, E., Giatti, S., Cavaletti, G., & Melcangi, R. C. (2020). Alterations of gut microbiota composition in post-finasteride patients: a pilot study. Journal of endocrinological investigation, 10.1007/s40618-020-01424-0. Advance online publication. https://doi.org/10.1007/s40618-020-01424-0
- Pedersen N, Ankersen DV, Felding M, Wachmann H, Végh Z, Molzen L, Burisch J, Andersen JR, Munkholm P. Low-FODMAP diet reduces irritable bowel symptoms in patients with inflammatory bowel disease. World J Gastroenterol. 2017 May 14;23(18):3356-3366. doi: 10.3748/wjg.v23.i18.3356. PMID: 28566897; PMCID: PMC5434443.
The calcium-hair loss connection
The connection between calcium and hair loss isn’t straightforward. On the one hand, no studies have directly examined the relationship between calcium and hair loss. On the other hand, calcium imbalances are common in chronic conditions linked to hair shedding. So, what’s the verdict on the calcium-hair loss connection?
Can low calcium levels cause hair loss? What about high calcium levels? And if yes, by which mechanisms?
This article uncovers the answers. By the end, you’ll uncover:
- The calcium-hair loss connection: where this mineral does (and doesn’t) influence hair loss
- Calcium loading: why supplementing isn’t always the answer
- The two chronic conditions linked to hair loss and a calcium imbalance… and what to do about them.
If you have any questions, please feel free to reach out in the comments.
All-Natural Hair Supplement
The top natural ingredients for hair growth, all in one supplement.
Take the next step in your hair growth journey with a world-class natural supplement. Ingredients, doses, & concentrations built by science.
What is calcium?
Calcium is one of the most abundant trace minerals in the body. It’s most well-known for its role as a building block of teeth and bone. But, calcium does much more than that. It’s a cellular signaling molecule – driving processes from inflammation to skin cell production and the firing of our neurons (1-3).
Calcium: an essential mineral

Interestingly, calcium also influences our endocrine system: the glands, tissues, and organs that regulate hormone production. And our endocrine systems can influence nearly every aspect of biology, including the development of common hair loss disorders like androgenic alopecia (AGA) and telogen effluvium.
This is why so many people wonder if calcium plays a role in hair loss. The thinking is as follows: calcium levels influence our hormone production, and hormones influence hair loss. So maybe calcium imbalances can cause hair loss.
But is this actually true? Let’s dive into the evidence.
Can a calcium deficiency cause hair loss?
Necessary disclaimer: at the extremes, anything can cause hair loss. For example, a water deficiency can cause hair loss. If we don’t drink water, we die. If we’re dead, we can’t grow hair.
The same is true for most vitamins, minerals, and nutrients – including calcium. If we don’t ingest any calcium, we can’t grow bone. If we can’t grow bone, we die. If we’re dead, we can’t grow hair.
I hope you see where I’m going with this – which is that we’re asking the wrong question. Rather than ask, “Can a calcium deficiency cause hair loss?”, we need to ask is, “Can a calcium deficiency within realistic means cause hair loss?”
And to answer that question, we have to dive into the literature. So, what do the studies say about calcium’s role in hair loss?
There are no studies measuring calcium’s role in human hair loss.
We know that calcium is essential for the function of many tissues. We know that calcium plays a significant role in cellular signaling, a process necessary for maintaining hair growth. And we know that, in animal studies, vitamin D-deficient dogs fed a low-calcium diet develop hair loss (4).
Unfortunately, no studies have directly examined the relationship between calcium and hair loss in humans. That means we don’t yet have data to directly answer this question.
What also makes this complicated: calcium is a tightly regulated mineral. We need calcium to mediate thousands of biochemical processes. In cases of dietary deficiencies, our bodies pull calcium from bone to maintain optimal levels. In cases of dietary surpluses, our bodies expel excess calcium to avoid over-accumulation.
For these reasons, it’s unlikely that – under normal settings – our bodies would let calcium levels to drop low enough to cause problems like bone mineral depletion or hair cycling dysfunction.
But what about abnormal settings?
For example, what about in cases of disease states where our bodies’ nutrient demands are much higher… or nutrient absorption is much lower (i.e., SIBO)… or certain supplements, medications, or surgeries have caused a dysregulation of nutrients in the body?
Under these scenarios, are calcium levels implicated in hair loss? Interestingly, the answer is yes.
Both low and high calcium levels are linked to hair loss – at least indirectly. Here’s how.
The indirect links between calcium imbalances & hair loss
Calcium deficiencies: polycystic ovarian syndrome (PCOS)
Polycystic Ovarian Syndrome (PCOS) is a chronic condition that affects 15-20% of women of reproductive age (5). Its biological biomarkers: high testosterone and insulin insensitivity. Its tell-tale signs: the formation of small cysts on the ovaries, missed or infrequent periods (cycles of 35+ days), weight gain, sluggishness, and even the development of female pattern hair loss – a consequence of the prolonged hormonal imbalances (specifically, the elevated testosterone).
Interestingly, PCOS is also associated with slight (but significant) deficiencies in vitamin B-12, C, D, and calcium (6). This begs the question: are these nutrient deficiencies a cause or a consequence of PCOS?
At least so far, literature reviews suggests that PCOS-related nutrient deficiencies are consequences of PCOS, not causes (7). Specifically, these nutrient deficiencies are partly the result of prolonged insulin resistance, which can increase nutrient demand.
That means that calcium deficiencies do not cause PCOS, and are thereby only indirectly associated with the female pattern hair loss that often accompanies the condition.
Calcium surpluses: hyperparathyroidism
Interestingly, there’s at least one more way that calcium imbalances are indirectly linked to hair loss. In this case, it’s a calcium surplus… and the condition is called hyperparathyroidism.
To explain this, we’ll start by uncovering the parathyroid glands, how this relates to hair shedding, and where calcium comes into play.
The parathyroid-hair loss connection
The parathyroid glands are part of our endocrine system. They consist of four glands that sit right behind the thyroid.
When our blood calcium levels go down, the parathyroid is responsible for getting them back in the normal range. It does this by secreting a hormone called parathyroid hormone (8).
The way this happens is out-of-scope for this article, but in short, parathyroid hormone signals for our bodies to leech calcium from our bone. In leeching bone calcium, blood levels of calcium increase, and the calcium then gets redistributed to other tissues in need.
Parathyroid’s action on bone to maintain calcium homeostasis

However, there are cases where this process can backfire.
Studies have shown that when parathyroid hormone is added to hair follicle cultures, it can cause them to prematurely enter the catagen phase of the hair cycle (9). Catagen is the transition step between the growth and shedding phases of the hair cycle. Therefore, anything that initiates catagen will eventually culminate into hair shedding.
If many hairs enter catagen at once, the hair shedding can be so drastic that it leads to a visible decrease in hair density. This can lead to a temporary form of hair thinning called telogen effluvium.
Hypothetically, this opens up the possibility that chronically elevated parathyroid hormone levels could trigger chronic, persistent hair shedding. Unsurprisingly, hair loss is a common complain amongst those with an overactive parathyroid (9).
So, what causes parathyroid hormone to remain elevated for significant periods of time? And what does any of this have to do with calcium intake?
The parathyroid-calcium connection
When parathyroid hormones go out of range, it is classified as a condition called hyperparathyroidism. There are two types of hyperparathyroidism: primary and secondary.
Primary hyperparathyroidism is almost always caused by a tumor on the parathyroid gland (10). Treatment for this type of hyperparathyroidism is usually confined to removing the affected gland – and through surgery.
Secondary hyperparathyroidism, on the other hand, are characterized as out-of-range parathyroid hormone levels caused by something unrelated to a direct dysfunction of the parathyroid gland itself. As such, its causes are more complex, individualized, and wide-ranging than primary hyperparathyroidism.
One common cause of secondary hyperparathyroidism is chronic kidney disease – which severely impacts the kidney’s ability to handle calcium and vitamin D.
The other common cause of secondary hyperparathyroidism is a vitamin D deficiency (11). Interestingly, vitamin D helps regulate calcium levels in the blood. When vitamin D levels are low, calcium levels in the blood drop. This engages the parathyroid gland to increase secretion of parathyroid hormone, all so that calcium levels can increase.
Low vitamin D >> low serum calcium >> increased parathyroid hormone >> increased calcium leeching from bone >> increased serum calcium
Therefore, hyperparathyroidism is another scenario where we can see imbalanced calcium levels and hair loss. In this case, it’s usually high calcium. But similar to PCOS, the calcium dysregulation is a consequence of the chronic condition, and not a cause of the hair thinning.
If I have secondary hyperparathyroidism, will eating less calcium lower my calcium scores?
Probably not. Here’s a quick overview of the relationship between calcium intake and elevated parathyroid hormones:
- No studies have currently established a link between calcium and secondary hyperparathyroidism.
- One study on almost 60,000 women found that increased calcium intake was independently associated with a decreased risk of developing primary hyperparathyroidism (12). This suggests that, in the long run, consuming adequate calcium may prevent primary hyperparathyroidism caused by tumors.
- Outside of this, some studies (13-15) have suggested that calcium and parathyroid hormones have an inverse relationship. In other words, decreased calcium intake may lead to increased parathyroid hormone levels while increased intake leads to lower parathyroid levels. However, this increase doesn’t lead to parathyroid hormones going out of range.
From this, we can glean three things: (1) adequate calcium intake may prevent primary hyperparathyroidism, but (2) poor calcium intake doesn’t appear to cause secondary hyperparathyroidism, and (3) decreased calcium intake may lead to increased parathyroid hormone (however, this doesn’t likely lead to hyperparathyroidism).
So, when we look at the big picture, it seems that poor calcium intake isn’t strongly associated with hyperparathyroidism as both a cause or a treatment. Rather, it elevates parathyroid levels, but not too far outside of the normal range.
Therefore, if you’re dealing with hair loss and you have high (or low) calcium scores, consider getting tested for vitamin D, PCOS, and hyperparathyroidism. In the interim, make sure to eat adequate amounts of calcium.
The good news is that for most modern diets, getting enough calcium shouldn’t be too hard.
How to optimize calcium intake
In general, I’ve always felt best to get nutrients from foods as opposed to supplements. In the case of calcium, this is especially important. Here’s why.
Calcium supplementation has been linked to an increased risk of cardiovascular events (16). In some cases, calcium supplements can also disrupt the pH of the stomach, which is critical for optimal digestion and nutrient assimilation (and, thus, hair growth) (17).
The good news is that calcium is readily available in the diet – even if you’re not currently consuming dairy. Here are just a few non-dairy foods replete with calcium:
Food sources of calcium (RDI: 1,000mg) Food source, serving size Mg, % DV Egg shells (3g) 1,200mg, 120% Firm tofu (100g) 683mg, 53% Black eyed peas (100g) 128mg, 10% Okra (100g) 77mg, 6% Trout (100g) 86mg, 7% Acorn squash (100g) 44mg, 3% For most adults consuming a balanced diet, you’re probably getting enough calcium. However, if you want to be sure about your calcium intake (and other nutrients), you can always track the micronutrient sufficiency of your diet using Cronometer or FitDay.
Summary
Calcium is an essential nutrient. But aside from extreme deficiencies, calcium imbalances don’t appear to cause hair loss.
There are no human studies examining the role of calcium levels and hair loss. However, calcium is indirectly related to hair follicle cycling. Moreover, studies have shown that vitamin D-deficient animals fed a low calcium diet develop alopecia. Therefore, it’s not unreasonable to wonder if calcium plays a role in hair loss.
To date, there are only two scenarios where calcium imbalances are linked to thinning hair:
- Low calcium and hair loss observed in polycystic ovarian syndrome patients
- High calcium and hair loss observed in hyperparathyroid patients
But in both situations, the calcium imbalances are consequences of the condition, rather than the cause of the hair loss.
Evidence shows that dietary calcium has little-to-no impact on blood calcium levels, at least within normal boundaries. Having said that, calcium supplementation may lead to an increased risk of heart disease – and potentially as a direct consequence to increased arterial calcification. For these reasons, it’s generally best to avoid calcium supplements altogether and stick to food sources (if possible).
The bottom line: calcium likely plays little to no role in the overwhelming majority of hair loss cases. If you’re dealing with hair loss and you have high (or low) calcium scores, consider getting tested for vitamin D, PCOS, and hyperparathyroidism. You might save yourself a lot of time, energy, and hair.
Questions? Comments? Please reach out in the comments section below.
References
- Klein G. L. (2018). The Role of Calcium in Inflammation-Associated Bone Resorption. Biomolecules, 8(3), 69. https://doi.org/10.3390/biom8030069
- Bikle, D. D., Xie, Z., & Tu, C. L. (2012). Calcium regulation of keratinocyte differentiation. Expert review of endocrinology & metabolism, 7(4), 461–472. https://doi.org/10.1586/eem.12.34
- Gleichmann, M., & Mattson, M. P. (2011). Neuronal calcium homeostasis and dysregulation. Antioxidants & redox signaling, 14(7), 1261–1273. https://doi.org/10.1089/ars.2010.3386
-
Mady LJ, Ajibade DV, Hsaio C, Teichert A, Fong C, Wang Y, Christakos S, Bikle DD. The Transient Role for Calcium and Vitamin D during the Developmental Hair Follicle Cycle. J Invest Dermatol. 2016 Jul;136(7):1337-1345. doi: 10.1016/j.jid.2016.02.813. Epub 2016 Mar 16. PMID: 26994969.
- Sirmans SM, Pate KA. Epidemiology, diagnosis, and management of polycystic ovary syndrome. Clin Epidemiol. 2013;6:1-13. Published 2013 Dec 18. doi:10.2147/CLEP.S37559
-
Szczuko M, Skowronek M, Zapałowska-Chwyć M, Starczewski A. Quantitative assessment of nutrition in patients with polycystic ovary syndrome (PCOS). Rocz Panstw Zakl Hig. 2016;67(4):419-426. PMID: 27925712.
- El Hayek S, Bitar L, Hamdar LH, Mirza FG, Daoud G. Poly Cystic Ovarian Syndrome: An Updated Overview. Front Physiol. 2016;7:124. Published 2016 Apr 5. doi:10.3389/fphys.2016.00124
-
Lofrese JJ, Basit H, Lappin SL. Physiology, Parathyroid. [Updated 2020 Jul 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-.
-
Skrok, A., Bednarczuk, T., Skwarek, A., Popow, M., Rudnicka, L., & Olszewska, M. (2015). The effect of parathyroid hormones on hair follicle physiology: implications for treatment of chemotherapy-induced alopecia. Skin pharmacology and physiology, 28(4), 213–225. https://doi.org/10.1159/000375319
-
Pokhrel B, Levine SN. Primary Hyperparathyroidism. [Updated 2020 Aug 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-.
-
Muppidi V, Meegada SR, Rehman A. Secondary Hyperparathyroidism. [Updated 2020 Jun 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-.
-
Paik, J. M., Curhan, G. C., & Taylor, E. N. (2012). Calcium intake and risk of primary hyperparathyroidism in women: prospective cohort study. BMJ (Clinical research ed.), 345, e6390. https://doi.org/10.1136/bmj.e6390
-
Jorde, R., Sundsfjord, J., Haug, E., & Bonaa, K. H. (2000). Relation between low calcium intake, parathyroid hormone, and blood pressure. Hypertension (Dallas, Tex. : 1979), 35(5), 1154–1159. https://doi.org/10.1161/01.hyp.35.5.1154
-
Patel, P., Mughal, M. Z., Patel, P., Yagnik, B., Kajale, N., Mandlik, R., Khadilkar, V., Chiplonkar, S. A., Phanse, S., Patwardhan, V., Patel, A., & Khadilkar, A. (2016). Dietary calcium intake influences the relationship between serum 25-hydroxyvitamin D3 (25OHD) concentration and parathyroid hormone (PTH) concentration. Archives of disease in childhood, 101(4), 316–319. https://doi.org/10.1136/archdischild-2015-308985
-
Aloia, J., Bojadzievski, T., Yusupov, E., Shahzad, G., Pollack, S., Mikhail, M., & Yeh, J. (2010). The relative influence of calcium intake and vitamin D status on serum parathyroid hormone and bone turnover biomarkers in a double-blind, placebo-controlled parallel group, longitudinal factorial design. The Journal of clinical endocrinology and metabolism, 95(7), 3216–3224. https://doi.org/10.1210/jc.2009-1294
-
Bolland, M. J., Grey, A., & Reid, I. R. (2013). Calcium supplements and cardiovascular risk: 5 years on. Therapeutic advances in drug safety, 4(5), 199–210. https://doi.org/10.1177/2042098613499790
-
Salisbury BH, Terrell JM. Antacids. [Updated 2020 Sep 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526049/
Does vitamin B12 improve hair growth? Supplement companies say yes, but scientific studies reveal a much murkier (and nuanced) relationship between vitamin B12, hair loss, and hair growth… one you’ll want to understand before you start supplementing.
In this article, we’ll dive into the arguments for and against a connection between vitamin B12 and hair growth. We’ll explore methylation, vitamin B12’s role in the hair cycle, and B12’s connection to different hair loss disorders. Then, we’ll reveal when vitamin B12 might (and might not) help our hair.
Finally, we’ll outline some potential best-practices for those who want to supplement with vitamin B12 for hair growth. After all, too little (and too much) of this vitamin may be counterproductive to both our hair and overall health.
All-Natural Hair Supplement
The top natural ingredients for hair growth, all in one supplement.
Take the next step in your hair growth journey with a world-class natural supplement. Ingredients, doses, & concentrations built by science.
What is vitamin B12?
Vitamin B12 is a singular vitamin apart of the greater B complex family. Like many B vitamins, vitamin B12 acts as an enzymatic cofactor for essential functions of the body (1). Specifically, vitamin B12 helps us metabolize food, produce red blood cells, and “methylate” DNA (more on this later). It also plays a protective role in cardiovascular health, as it helps to reduce excess amounts of a protein called homocysteine – which, at high levels, is inflammatory.
Vitamin B12 Supplement Mockup

Given its importance in so many bodily functions, it’s natural to wonder: does vitamin B12 also help fight hair loss? After all, it seems to be a staple ingredient in most hair health nutritional supplements. So, what does the evidence show?
The case for a vitamin B12-hair loss connection
From a scientific perspective, vitamin B12 might support hair growth in many ways.
- Vitamin B12 help support the production of DNA – which is necessary to maintain the rapid cell division that drives hair growth (2). Without cell division, not only can hair not grow… but human life cannot sustain itself, either. In this respect, technically anything that supports human survival – even water – supports hair growth.
- Vitamin B12 helps us produce hemoglobin – a molecule inside our red blood cells that carries oxygen and iron into our tissues (3). When someone has low hemoglobin, they often have an iron deficiency (i.e., anemia). Interestingly, anemia is highly correlated with hair loss – particularly in women ages 14-40 – and vitamin B12 supplementation can help improve hemoglobin product and thereby iron levels for those who are deficient.
But there’s also another reason that vitamin B12 might support hair growth – and it happens to do with one of the biggest buzzwords surrounding this vitamin: methylation.
In the simplest terms, methylation is a way in which our bodies can “turn on” or “turn off” certain genes. In other words, methylation helps change our gene expression – and thereby influences our ability to prevent cancer, reduce inflammation, and everything in between.
Here are just a few roles that methylation – and our methylation cycle – regulates inside our bodies:
- Production of methionine and cysteine. These are two sulfur-based amino acids that play integral roles in muscle building, inflammation regulation, and antioxidant production.
- Glutathione production. Sulfur amino acids are a major precursor for glutathione, the body’s master antioxidant.
- Homocysteine reduction. High levels of homocysteine in the blood are linked to a variety of inflammatory diseases.
- Production of SAMe. This protein is believed to support mental health, among many other things (4).
So, how does methylation relate to B12 and hair loss?
In one study on rabbits, researchers found methionine to be a promoter of hair growth. The mechanism behind this? An increase in the activity of the Wnt/β-catenin signaling pathway (5).
The Wnt/β-catenin pathway is important to this discussion for a few reasons:
- This pathway helps promote the creation of stem cells, which are required for hair growth and hair follicle function (6).
- In androgenic alopecia (AGA) – the most common form of hair loss in adult men – male hormones interfere with Wnt/β-catenin signaling. Specifically, this signaling pathway is dampened, also known as downregulated. As a result, hair follicle stem cell activity is impaired, which prevents proper hair cycling. This shortens the growth stage of a hair follicle, causing it to prematurely shed. Over time, this hinders hair growth and may even accelerate hair follicle miniaturization – a defining hallmark of male and female pattern hair loss (7).
Here’s where vitamin B12 might come into play:
Vitamin B-12 is a cofactor in the methylation cycle, meaning that it helps to activate methylation. Interestingly, vitamin B-12 deficiencies are believed to be a major driver of a dysfunctional methylation cycle – as evidenced by an association between homocysteine levels and vitamin B-12 deficiency (8). This suggests that the methylation cycle is “backed up”, preventing homocysteine from being converted to cysteine and methionine.
Thus, B-12 deficiency may impair methionine synthesis from the methylation cycle. Because we know that methionine contributes to Wnt/β-catenin signaling, it’s possible that a reduction in methionine may lead to reduced Wnt/β-catenin activity. And therefore, it’s possible that a vitamin B12 deficiency in scalp tissues might play a role for people dealing with androgenic alopecia.
Summary (so far): how vitamin B12 might help fight hair loss
There are a variety of ways that vitamin B12 might be connected to hair loss in humans:
- Vitamin B12 helps support DNA synthesis. Without DNA synthesis, we would die. We can’t grow much hair if we’re dead.
- Vitamin B12 helps normalize hemoglobin production (and thereby iron levels). For females with both hair loss and an iron deficiency, vitamin B12 might be a great way to improve iron status and encourage hair growth.
- Vitamin B12 helps support methylation. This might have ramifications for one of the world’s most common hair loss disorders – male pattern hair loss (AGA. In AGA-affected hair follicles, the Wnt / β-catenin signaling pathway is dampened, which leads to shorter-growing hair, premature hair shedding, and potentially even hair follicle miniaturization. If this happens to be the direct result of a deficit in localized methylation in scalp tissues, then vitamin B12 might help improve methylation and thereby improve Wnt / β-catenin signaling, which would allow for hairs to grow longer, shed less prematurely, and (hopefully) not miniaturize as quickly.
But it’s important to stress: these suspected mechanism are all hypothetical. Yes, vitamin B12 is connected to each mechanism. Yes, these mechanisms are linked to hair loss (and hair growth). But there’s a difference between association and causation. And this difference, unfortunately, is consistently forgotten by companies trying to sell you B12 supplements. Thus, to prove a strong association or causation, the real questions we should be asking are:
- Are vitamin B12 deficiencies (in skin tissues or throughout the body) observed more frequently in people who are balding?
- Does vitamin B12 – through supplementation or topical application – actually improve hair loss outcomes?
In answering these questions, we can actually discern whether or not it makes sense for most people to spend money on vitamin B12 supplements to try and regrow their hair.
And as you can guess, these questions happen to lead us to our next section: the case against a vitamin B12-hair loss connection.
The case against a vitamin B12-hair loss connection
While there is hypothetical evidence linking vitamin B12 to hair loss and hair growth, this argument begins falls apart when we zoom out and start looking at the broader evidence.
Specifically, we’re going to talk about the following:
- Misconceptions about methylation, B12, Wnt/β-catenin pathways, and hair loss
- Vitamin B12 levels of hair loss patients
- Observations in birth control-induced vitamin B12 deficiencies, and what this does (or doesn’t do) to hair
Methylation misconceptions
Earlier we discussed how, in balding hair follicles, a deficiency in the methylation cycle might interfere with Wnt/β-catenin signaling pathways, which might accelerate hair loss. We argued that because vitamin B12 supports methylation, this vitamin might also help reverse this methylation deficiency, and thereby help fight hair loss from androgenic alopecia.
But it’s important to note: vitamin B12 is just one (of many) vitamins and nutrients that support methylation. For instance, many other B-vitamins also support methylation, and these B-vitamins are found in abundance in foods like beef, eggs, and poultry.
This means that even if you do have a vitamin B12 deficiency, your body will likely be able to compensate for this – at least from a methylation perspective – via your dietary choices. Therefore, in balding hair follicles, even if Wnt / β-catenin downregulation were exclusively due to a methylation issue (it isn’t), your body would still have many “fallback” vitamins to address that methylation issue. So, in androgenic alopecia, changes to a hair follicle’s gene expression cannot be significantly attributed to a vitamin B12 deficiency.
Therefore, it also shouldn’t be surprising to find out that there aren’t any differences in vitamin B12 levels between those with and without hair loss.
Looking at B12 levels in the blood of hair loss patients
When we zoom out beyond the actual hair follicle and look at studies on people with common hair loss disorders like AGA, telogen effluvium (TE), or alopecia areata (AA) – the data are consistently clear: there is no difference in blood measurements of vitamin B12 between people with and without hair loss (9). In other words, people who are losing their hair and who have full heads of hair appear to have the same vitamin B12 levels.
Even more compelling, recent literature reviews have found no evidence to support the use of vitamin B12 for hair loss of any type (9). That means that not only are vitamin B12 levels the same across those with and without hair loss, but that for those with hair loss, vitamin B12 supplementation generally doesn’t improve hair loss outcomes.
What about women with hair loss due to an iron deficiency? Doesn’t vitamin B12 help improve iron stores, and have some therapeutic benefit here?
Yes and no.
Earlier, we argued a connection between hemoblogin, iron, vitamin B12, and hair loss. As a refresher, hemoglobin is a molecule found in red blood cells. Hemoglobin carries oxygen and iron, and in general, when someone has low hemogloblin levels, they also have low iron (10). Low iron levels are often found in women ages 14-40 with hair loss. Vitamin B12 is a key cofactor in hemoglobin formulation. Therefore, you might be able boost hemoglobin production with vitamin B12, and therefore potentially normalize low iron levels. If someone is dealing with hair loss as a direct result of low iron levels, then vitamin B12 supplementation might help to normalize these levels and maybe regrow some hair.
So, in a situation where someone’s hair loss is due to poor iron status, and their poor iron status is a direct result of low vitamin B12, then it absolutely makes sense to supplement with vitamin B12. In doing so, you’d improve hemoglobin production, oxygen and iron transport, and (very likely) hair loss outcomes. This is why a lot of popular hair loss supplements – like Nutrafol – contain B12.
At the same time, a vitamin B12 deficiency is only one possible contributor toward an iron deficiency. A more likely contributor? A deficiency in iron itself (11). So, while vitamin B12 is probably therapeutically useful in some circumstances of iron deficiency-related hair loss, it’s not the only reason – or even the biggest reason – for why the iron deficiency arises.
Therefore, B12 is likely useful for a much smaller percentage of women than advertisements for these hair health supplements might lead you to believe.
Observations in birth control-induced B12 deficiency
This argument is further strengthened by another observation researchers have made: women with vitamin B12 deficiencies caused by hormonal birth control don’t experience hair loss or adverse changes to hair growth (9). As such, even when a deficiency is present, it doesn’t seem to negatively impact hair growth. In fact, many women on hormonal contraceptives report the opposite effect – hair regrowth – which is why some contraceptives are also used off-label as a hair loss treatment.
The good news? Vitamin B12 might help reverse premature hair graying
In regard to hair health, there is one way that vitamin B12 might positively impact hair health outcomes. It might help to prevent, or even reverse, premature graying.
To be clear, the majority of research doesn’t indicate B12 deficiency is a cause of hair loss. But, there are several reports supporting an association between inadequate B12 levels and premature hair graying, which is grey hair that onsets before the ages of 20-30 (depending on the demographic) (12).
For instance, one small study demonstrated that individuals with premature hair graying had lower vitamin B12, folate, and biotin levels than control subjects without premature gray hair (13). Additionally, some studies report a higher incidence of premature graying in pernicious anemia, a blood condition sometimes caused by B12 deficiency (14).
There are also three case reports of patients reversing their premature gray hair with B12 supplementation (15-17). Needless to say, there seems to be evidence of both an association of low B12 and early greying, and a reversal of early greying following B12 supplementation.
The association between B12 deficiency and premature graying isn’t fully established, and there are absolutely other factors that can lead to premature hair graying. Moreover, B12 supplementation is really only relevant to reversing graying hair in the context of B12 deficiency.
That being said, a vitamin B12 deficiency may be worth investigating for anyone experiencing premature hair graying – regardless of whether you’re losing your hair.
The verdict: in most situation, vitamin B12 likely has no effect on hair loss (and hair regrowth), but vitamin B12 might reverse premature hair graying in the presence of B12 deficiency
Although hypothetical evidence suggests an absence of B12 activity could negatively impact hair growth, in vivo human studies indicate that either (1) there is no relationship between vitamin B12 deficiency and hair loss and/or (2) there is an overriding factor (like methionine provision outside of the methylation cycle) that prevents B12 deficiency from causing hair loss.
The exception to this is if someone has iron deficiency-related hair loss, and if their iron deficiency is exclusively the result of poor hemoglobin production due to a vitamin B12 deficiency. In this case, vitamin B12 supplementation can address the deficiency, improve hemoglobin production, and thereby drastically improve iron transport (and, ultimately, hair growth). But it goes without mentioning that this is a very specific scenario that is not faced by the majority of hair loss sufferers in the developed world.
In any case, it’s clear that supplementing with B12 is probably not the best solution for improving hair growth – at least as a standalone therapy.
That being said, it’s important to note that having adequate B12 is essential for optimal health. Even if it doesn’t cause hair loss, B12 deficiency can still lead to anxiety, fatigue, neuropathy, and cardiovascular issues, among other health issues. Moreover, B12 deficiency appears to be one potential cause of premature hair graying.
As such, even if it doesn’t improve hair loss, some may still find it necessary to supplement with vitamin B12. So, in these cases, what’s the best approach for supplementation?
Things to keep in mind when supplementing with vitamin B12
Vitamin B12 supplements are available in three forms: cyanocobalamin, methylcobalamin, and adenosylcobalamin. Methyl- and adenosylcobalamin are naturally-occurring forms of B12 whereas cyanocobalamin is synthetic.
Though synthetic is not always subpar to naturally-occurring forms of B12, in this case, supplementing with methyl- and adenosylcobalamin B12s is much more efficient. The reason for this is they are already in their active forms, ready to be used by the body. Cyanocobalamin, on the other hand, requires enzymatic processing before it can be utilized. On top of this, cells don’t seem to retain cyanocobalamin as well as some of the other forms (18).
Additionally, some researchers have raised concerns with long term cyanocobalamin supplementation, due to the cyanide present in the compound (18). Even though these concerns aren’t yet substantiated, an abundance of caution may be warranted here.
The bottom line? If your diet isn’t providing you with enough vitamin B12 and you choose to supplement, consider opting for a B-complex or multivitamin formulated with methyl- or adenosylcobalamin.
Summary
Vitamin B12 deficiency isn’t likely to be a cause for hair loss. As such, claims that supplementing with B12 will improve hair growth are largely unfounded. This is despite some pretty compelling theoretical evidence – like B12’s role in hemoglobin formation, nucleic acid synthesis, and the methylation cycle that produces growth-supporting methionine.
It just goes to show how important it is that we don’t rely on studies of isolated nutrients in cell cultures. Moreover, we shouldn’t have high hopes for products marketed on these premises when it comes to regrowing our hair.
That being said, vitamin B12 deficiency can still cause real problems and, in some cases, may be an underlying factor in premature hair graying. So, for those who are dealing with early-onset gray hair, it may be worth checking your B12 levels. And if you are deficient? Restoring your B12 levels may just reverse the condition.
So, if supplementing is warranted in your case, opt for a methyl- or adenosylcobalamin-containing supplement over one containing cyanocobalamin. They’re more bioavailable and may be safer in the long-term.
But, for the overwhelming majority? You’re likely to get all the vitamin B12 you need from food — more than enough to rule it out as a plausible factor in hair loss.
Have any questions about vitamin B12? Leave them below.
References
- Al Amin ASM, Gupta V. Vitamin B12 (Cobalamin) [Updated 2020 Jun 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559132/
- Almohanna HM, Ahmed AA, Tsatalis JP, Tosti A. The Role of Vitamins and Minerals in Hair Loss: A Review. Dermatol Ther (Heidelb). 2019;9(1):51-70. doi:10.1007/s13555-018-0278-6
- Ferreira GC. Heme biosynthesis: biochemistry, molecular biology, and relationship to disease. J Bioenerg Biomembr. 1995;27(2):147-150. doi:10.1007/BF02110029
- Sharma A, Gerbarg P, Bottiglieri T, et al. S-Adenosylmethionine (SAMe) for Neuropsychiatric Disorders: A Clinician-Oriented Review of Research. J Clin Psychiatry. 2017;78(6):e656-e667. doi:10.4088/JCP.16r11113
-
Zhu Y, Wu Z, Liu H, Liu G, Li F. Methionine promotes the development of hair follicles via the Wnt/β-catenin signalling pathway in Rex rabbits. J Anim Physiol Anim Nutr (Berl). 2020 Jan;104(1):379-384. doi: 10.1111/jpn.13238. Epub 2019 Nov 15. PMID: 31732998.
- Choi YS, Zhang Y, Xu M, et al. Distinct functions for Wnt/β-catenin in hair follicle stem cell proliferation and survival and interfollicular epidermal homeostasis. Cell Stem Cell. 2013;13(6):720-733. doi:10.1016/j.stem.2013.10.003
- Chen X, Liu B, Li Y, et al. Dihydrotestosterone Regulates Hair Growth Through the Wnt/β-Catenin Pathway in C57BL/6 Mice and In Vitro Organ Culture. Front Pharmacol. 2020;10:1528. Published 2020 Jan 23. doi:10.3389/fphar.2019.01528
- Gilfix BM. Vitamin B12 and homocysteine. CMAJ. 2005;173(11):1360. doi:10.1503/cmaj.1050170
- Almohanna HM, Ahmed AA, Tsatalis JP, Tosti A. The Role of Vitamins and Minerals in Hair Loss: A Review. Dermatol Ther (Heidelb). 2019;9(1):51-70. doi:10.1007/s13555-018-0278-6
- National Academy of Sciences (US) and National Research Council (US) Division of Medical Sciences. Conference on Hemoglobin: 2–3 May 1957. Washington (DC): National Academies Press (US); 1958. THE ROLE OF IRON IN HEMOGLOBIN SYNTHESIS. Available from: https://www.ncbi.nlm.nih.gov/books/NBK224286/
- Trost LB, Bergfeld WF, Calogeras E. The diagnosis and treatment of iron deficiency and its potential relationship to hair loss. J Am Acad Dermatol. 2006 May;54(5):824-44. doi: 10.1016/j.jaad.2005.11.1104. PMID: 16635664.
- Kumar AB, Shamim H, Nagaraju U. Premature Graying of Hair: Review with Updates. Int J Trichology. 2018;10(5):198-203. doi:10.4103/ijt.ijt_47_18
- Daulatabad D, Singal A, Grover C, Chhillar N. Prospective Analytical Controlled Study Evaluating Serum Biotin, Vitamin B12, and Folic Acid in Patients with Premature Canities. Int J Trichology. 2017;9(1):19-24. doi:10.4103/ijt.ijt_79_16
-
Dawber RP. Integumentary associations of pernicious anaemia. Br J Dermatol. 1970 Mar;82(3):221-3. doi: 10.1111/j.1365-2133.1970.tb12428.x. PMID: 5441758.
-
Noppakun N, Swasdikul D. Reversible hyperpigmentation of skin and nails with white hair due to vitamin B12 deficiency. Arch Dermatol. 1986 Aug;122(8):896-9. PMID: 3740873.
-
Carmel R. Hair and fingernail changes in acquired and congenital pernicious anemia. Arch Intern Med. 1985 Mar;145(3):484-5. PMID: 3977516.
-
Niiyama S, Mukai H. Reversible cutaneous hyperpigmentation and nails with white hair due to vitamin B12 deficiency. Eur J Dermatol. 2007 Nov-Dec;17(6):551-2. doi: 10.1684/ejd.2007.0285. Epub 2007 Oct 19. PMID: 17951150.
- Paul C, Brady DM. Comparative Bioavailability and Utilization of Particular Forms of B12 Supplements With Potential to Mitigate B12-related Genetic Polymorphisms. Integr Med (Encinitas). 2017;16(1):42-49.
Alopecia areata is an autoimmune form of hair loss that affects 2% of people worldwide. If you’re dealing with alopecia areata, the burden of hair loss often feels overwhelming – as the condition can progress rapidly, inexplicably, and without regard.
Fortunately, alopecia areata is treatable. In many cases, it’s also reversible. The first step toward making progress? Understanding alopecia areata, its myriad triggers, and how these factors relate to your unique hair loss situation.
In this article, we’ll uncover the characteristics of alopecia areata: its clinical presentations, histological features, and more. We’ll also dive into alopecia areata’s causes: what we know, what we don’t, and what this type of hair loss can tell us about our health.
Finally, we’ll outline treatments for alopecia areata (both conventional and natural): the research supporting them, the expectations for regrowth, and who might be the best candidates for each intervention.
What is alopecia areata?
Alopecia areata (AA) is a form of hair loss driven by autoimmunity. To put it simply, alopecia areata occurs when our bodies mistakenly recognize our hair follicles as foreign invaders, and then begin to attack our hair follicles. This leads to the dysfunction of hair follicle stem cells, and eventually, hair loss.
What does alopecia areata look like?
You might know alopecia areata (AA) from its “patchy” presentation, whereby slick-bald patches begin to form in a non-uniform fashion. But AA can also vary in appearance – and even mask the look of many other common hair loss disorders.
Types of alopecia areata
Alopecia areata focalis or “patchy” alopecia areata Hair loss in patches, can extend beyond just the scalp. The most common form of alopecia areata. It may or may not progress into alopecia totalis or alopecia universalis. 
Alopecia areata totalis Loss of all hair on the scalp including eyelashes and eyebrows. 
Alopecia areata universalis Hair loss of the scalp, eyelashes, eyebrows, and whole body, including all body hair. 
Ophiasis or alopecia areata marginata Hair loss around the circumference of the head in a band-like fashion. It is most commonly seen behind the ears and the nape of the neck, but can occur in the frontal hairline and extend throughout the scalp in severe cases, as well. 
Ophiasis inversus Hair loss that begins in the center of the scalp and progresses into the surrounding regions. 
Alopecia areata incognita Diffuse hair loss whereby no specific bald “patches”, normally characteristic of alopecia areata, can be distinguished. 
What’s the histology of alopecia areata?
Histology is a term used to describe a close-up view of a tissue’s structure. In the world of hair loss, histology refers to the microscopic view of a hair follicle (i.e., what a hair follicle looks like when biopsied).
When doctors are uncertain about someone’s hair loss diagnosis, they’ll often take a biopsy of their patient’s scalp so that they can get a look of the histological features of the affected hair follicles. Then, they’ll compare what they see against the histological hallmarks of certain hair loss disorders.
It might sound invasive, but these scalp biopsies are perhaps the most effective way for dermatologists to definitively diagnose someone’s hair loss. And when it comes to alopecia areata, this type of hair loss has a lot of interesting features:
- Inflammation. Specifically, the infiltration of lymphocytes near hair follicle stem cell bulges. Lymphocytes are immune cells; the bodies uses them as part of an inflammatory response. Where there are high lymphocytes, there are usually high amounts of inflammation. One study found that 84% of alopecia areata subjects presented with this kind of inflammation.
- Dysfunctional hair follicle stem cell bulges. Hair follicle stem cells contain the blueprints to make new hair follicles. When too many lymphocytes collect near these stem cells, they generate inflammation, and that inflammation interferes with the ability for these stem cells to function. This leads to stem cell dysfunction and an inability to form new hair.
- Hair follicle miniaturization. This is a decrease in hair strand diameter, which leads to thinner-looking hair. One study observed that 90% of alopecia areata subjects had hair follicle miniaturization. Conversely, this study only found miniaturization in 25% of subjects. This study found that the presence of miniaturization is likely dependent on the nature of the hair loss – for example, early stages of AA likely do not present with miniaturization. It is most commonly often found in recurrent and chronic forms of AA.
- Increased number of catagen hairs. This study found that 93% of patients presented with an abnormally high number of hair follicles in the catagen phase – the phase in the hair cycle whereby nutrient supply is cut off and the hair prepares to shed. In healthy scalps, only 1% of hair follicles are typically in catagen. With AA, that percent can skyrocket.
Isn’t inflammation & hair follicle miniaturization part of androgenic alopecia (AGA)?
Yes.
Pattern hair loss, also known as androgenic alopecia (AGA), is also often defined by the presence of inflammation, hair follicle miniaturization, and even an increased number of catagen and telogen hairs. This begs the question: how can we distinguish between AGA and alopecia areata… especially in cases where alopecia areata is diffuse?
Well, there are some additional factors that can help us identify if we’re dealing with alopecia areata (AA) or androgenic alopecia (AGA).
What makes alopecia areata (AA) unique from androgenic alopecia (AGA)?
- The patterning of AA. In most AA cases, hair loss begins in a “patchy” fashion — a patterning that is exclusive to AA. In contrast, AGA occurs in a very different, yet still distinct manner. For men, it’s temple recession and crown thinning. For women, it’s most often a widening of the part while their hairline stays intact (also known as a “Christmas tree” pattern).
- Exclamation-point hairs in AA. Exclamation point hairs, pictured below, are a phenomenon only observed in AA. These hairs remain thick along the shaft but are noticeably thinner towards the opening of the follicle, creating an appearance akin to that of an exclamation mark ( ! ). This is only a defining factor if hair is still present.
-
Exclamation mark (!) hair

-
- Pigment casts in AA. Melanin is a substance produced by cells to create pigment for our skin and hair. Interestingly, in cases of AA, there are often “clumps” of melanin deposits throughout the follicular unit. This can appear like a small, dark tattoo where there should be a hair follicle. The incidence of pigment casts varies from study to study from 44% to 72%. Having said that, pigment casts by themselves aren’t a good indicator of AA – mostly because they’re often observed at similar rates in other hair loss disorders like trichotillomania (i.e., a “hair-pulling disorder”).
What causes alopecia areata?
To reiterate from earlier, inflammation seems to initiate of AA. The process looks like this:
- Inflammatory cells infiltrate the area surrounding a hair follicle stem cell bulge.
- This inflammation disrupts stem cell functionality, leading to stem cell dysfunction.
- These dysfunctional stem cells stop producing normal-looking hair follicles.
This leads to:
- Rapid hair follicle miniaturization (i.e., exclamation hairs).
- A loss of visible hair (i.e., slick-bald patches in alopecia areata focalis).
- Weaker, brittler hair that breaks off soon after growing out of the skin surface.
This begs the question… when it comes alopecia areata, what causes the inflammation that kickstarts the whole process?
What causes the inflammation in alopecia areata?
While the exact origin of inflammation isn’t known, researchers have a good idea of three contributing factors: genetics, environmental triggers, and loss of immune privilege in the follicle.
And though we don’t know the exact nature of these contributing factors, researchers have begun to uncover some of the details:
- Genetics. Studies have shown that AA is common among family members, affirming the role of a genetic component in certain cases. Specific genes affected include those that code for immune cell receptors, cell death coordination, immune-regulating cells, other proteins that regulate cellular communication.
- Environmental factors. Much like genetics, environmental elements faced by AA-affected families might also explain why this condition tends to appear multiple times within the same family. These environmental factors include
- Stress
- Infections
- Hormone fluctuations
- Dysbiosis of the gut flora
- Oxidative stress
- Soy consumption (implicated in animal studies, though not yet confirmed in human studies)
- Nutrient deficiencies (specifically, vitamin A and/or vitamin D deficiency.
- Loss of immune privilege. Under normal circumstances, a hair follicle produces its own “shield” from our own immune system. This shield is comprised of many immune-suppressing molecules. This is known as immune privilege, and it’s what make hair follicles incredibly unique mini-organs. However, in AA, researchers believe this immune privilege collapses – preventing the hair follicle from protecting itself against a damaging attack by the immune system. This would lead to inflammation and, thereby, the destruction of the hair follicle stem cell bulge. How this occurs is unknown, but researchers believe it is a result of proteins secreted by skin cells that the body forms an “antibody” to, leading to an immune attack.
What are the available treatments?
Currently, there are a variety of drug and non-drug treatments for AA. But before we reveal them, there are two things worth mentioning:
- Because we don’t fully understand why AA occurs, the most well-studied treatments primarily focus on suppressing the signals that lead to AA (as opposed to treating its root cause). More recent research has explored treatments that try to target some of these potential root causes. These studies show promise, but they’re also a little “out there” in terms of peoples’ comfortabilities. So, as you read on, keep this in mind.
- When it comes to reversing alopecia areata, 34-50% of cases resolve spontaneously. This makes it hard to know which treatments work, and which treatments just happened to coincide with spontaneous reversals. This is why control groups are so important in AA studies. Moreover, the likelihood of spontaneous reversal depends highly on the progression of the disease: as AA progresses, the likelihood of spontaneous resolution declines.
Regardless of these factors, it seems like treating AA in earlier stages leads to better outcomes and decreases the risk of future treatment resistance. So, if you’re facing AA right now, it’s best not to place your bets on a spontaneous reversal; rather, hedge those bets with the treatment options at your disposal (or at least the ones you’re comfortable trying).
The following sections detail many conventional and alternative treatments: the evidence, best practices, mechanisms of action, and more.
Drug-based treatments
Topical, intralesional, and systemic steroids (first line of treatment)
- Best candidates: Patchy AA may be controlled with topical or intralesional steroids. More severe or resistant cases (alopecia totalis, alopecia universalis, ophiasis) may require systemic steroid treatment or combination therapy (steroids + other treatments).
- Mechanisms of action: Reduction of inflammation.
- Dosages: For topical steroids, concentrations vary from 0.05% to 0.25%; for intralesional steroids, most commonly-used agent is triamcinolone acetonide, at concentrations of 2.5 mg/mL to 10 mg/mL; for systemic steroids, varying doses given as pulse doses, a.k.a large bolus doses for a specific period of time, administered in intervals.
- Outcomes: Results vary between methods of administration. Topical steroids are best suited to earlier stages of AA, with about 57% of these patients demonstrating complete regrowth. Intralesional steroids have a slight advantage over topicals, with 63% of patients achieving complete growth in one study. Systemic steroid treatment is primarily relegated to resistant cases.
- Problems: With topical and intralesional treatment, the main side effect is cutaneous atrophy or thinning of the skin. Systemic steroids come with a higher risk of side effects, and these risks may outweigh the benefits of hair growth. The relapse rate after steroid treatment ranges between 33% and 75%.
Janus kinase (JAK) inhibitors (oral and topical)
- Best candidates: Men, women, and children with patchy AA, alopecia universalis, alopecia totalis, according to preliminary evidence.
- Mechanisms of action: Blocks inflammatory signaling.
- Dosages: 5mg twice per day.
- Outcomes: Efficacy is similar in patchy alopecia areata, alopecia universalis, and alopecia totalis as well as in both men vs. women and adults vs. children. Oral administration is more likely to produce a good response when compared to the use of topical applications. Studies show initial hair growth occurs as soon as 2 months, with full regrowth occurring in an average of 6 months.
- Problems: Evidence is limited and primarily in the form of case reports. As such, though JAK inhibitors show promise, we don’t know a lot about the safety or efficacy of these medications in AA, yet. Drugs in this class have been linked to an increased risk of upper respiratory issues, latent virus reactivation, and cancer. The exact risk of these adverse effects in the treatment of AA is unknown, however, upper respiratory infection was the most common among available case studies. Like other therapies in AA, there is a high rate of relapse after cessation of the drug.
Immunotherapy (dinitrochlorobenzene, squaric acid dibutylester and diphenylcyclopropenone, with diphenylcyclopropenone)
- Best candidates: Mild to moderate patchy alopecia areata.
- Mechanisms of action: Immunogenic compound “distracts” the immune system with a more stimulating antigen than the self-antigen the mediates the autoimmune reaction.
- Dosages: Concentration sufficient enough to induce an allergic response.
- Outcomes: Response rates as reported in the literature range widely, from about 9% to 87%. About 20% to 30% of patients are able to achieve significant hair growth, such that they are able to manage their hair loss without a wig. This specific therapy may require longer treatment times, as evidenced by over a two-fold increase in response rate at 32 months versus 6 months. So, ask your doctor about whether a longer treatment period might be right for you. In over 30 years of use, long-term side effects have not been reported with immunotherapy, however, some side effects can occur during therapy. The most common side effect is cervical and occipital lymphadenopathy and severe dermatitis, however, these only last for the duration of the therapy. Moreover, dermatitis can be avoided by using the proper concentration of the antigenic compounds. Vitiligo and itching have also been reported but are considered rare. Overall, the treatment appears to be well-tolerated and effective.
- Problems: As with most treatments, relapse rates are high at around 62%. Response rates are somewhat low when administered for the same treatment periods as other treatments. In other words, immunotherapy takes longer to work than other treatments.
Minoxidil
- Best candidates: Mild patchy AA, AA patients tapering off of steroid therapy
- Mechanisms of action: Not fully known, but is believed to stimulate the “anagen” growth phase of the hair cycle, thereby promoting regrowth of lost hairs.
- Dosages: 2% or 5% minoxidil, two to three times daily.
- Outcomes: In one study, 85% of patients using 5% minoxidil alone experienced regrowth, however, this regrowth wasn’t cosmetically significant. Another study demonstrated that the application of 2% minoxidil, when applied three times daily, helped retain hair regrowth after tapering off of steroid treatment.
- Problems: Minoxidil doesn’t seem to be that effective outside of post-steroid hair retention.
Methotrexate
- Best candidates: Moderate to severe AA, including universalis, diffuse, and totalis phenotypes.
- Mechanisms of action: Suppression of the immune system.
- Dosage: 10-25mg per week + folate/folic acid supplements (methotrexate depletes folic acid).
- Outcomes: One study reported that 44.4% of subjects taking methotrexate were able to regain 50% or more of their hair as observed in a follow-up period ranging from 3 to 51 months. The best responders were males, those with multifocal patchy AA (followed by totalis, then universalis, and, lastly, diffuse), and those who used a cumulative dose of 1,000 to 1,500mg. When corticosteroids were used alongside methotrexate, the number of patients regrowing at least 50% of their hair increased to 77.3%.
- Problems: Methotrexate isn’t well-studied for AA — the evidence is primarily made up of case studies. 3-24% of patients can expect to experience side effects like mild to moderate leukopenia, thrombocytopenia, and megaloblastic anemia. There is also the risk of liver fibrosis, with an incidence ranging from 7% to 71.8%. Such a wide range makes the true risk hard to quantify. Myelosuppression is also a dangerous side effect and its risk associated with methotrexate use is unpredictable. Relapse rates vary from 33% to 80%, with some studies suggesting the rate is associated with how much hair is gained during treatment — more hair regrowth during treatment is associated with a lower risk of relapse after treatment.
Non-drug based treatments
Fecal microbiota transplant (FMT)
Fecal microbiota transplant (FMT) is a procedure whereby gut bacteria are isolated from a donor’s feces, purified, and then transplanted into an FMT candidate. This is the only procedure in which bacterial strains that have been lost from the gut can be reinoculated.
Currently, the procedure is elective in Europe (anyone can elect to have it performed). But in the U.S., it’s only available for chronic C. difficile infections. In the U.K., Taymount Clinic is one of the most popular worldwide-serving clinics for elective FMT.
- Best candidates: Evidence is limited but FMT has been used to treat patchy AA and alopecia universalis. May also be effective in treatment-resistant cases.
- Mechanisms of action: Unknown, but probably a normalization of the gut flora, leading to reduced autoimmune activity.
- Dosage: N/A; donor transplant is performed in one procedure, although people often elect for multiple procedures (depending on the delivery method).
- Outcomes: There are currently three case studies (studies here and here) investigating the efficacy of FMT in AA: two in alopecia universalis and one in patchy AA. Of the 3 case studies, all patients showed marked improvement following FMT — with two cases of almost full regrowth (one in universalis alopecia and one in patchy AA) and one case of partial regrowth. In all cases, this hair regrowth was sustained for at least 1.5 to 3 years. Considering the relapse of AA for most treatments is high, this sustained regrowth is promising. However, whether or not this regrowth was sustained beyond the follow-up period is unknown.
- Problems: FMT is still considered an investigative treatment in the U.S. and is, therefore, not elective for individuals with AA, unless a patient is also dealing with chronic C. difficile infection. As such, US residents wanting to explore the treatment must travel for the procedure and pay for it out-of-pocket — these costs can rack up (but may be worth it in the long run).
FMT before & after photos
Case #1: (A) 1 month, (B) 4 months, (C) 1.5 years after FMT in patchy AA

Case #2: (A) The patient’s scalp when his AA first began (B) a few months, (C) 1.5 years after FMT in alopecia universalis

Case #3: The beginning of hair regrowth after FMT in a case of long-standing alopecia universalis

Essential oils
- Best candidates: Evidence is limited, however, efficacy has been demonstrated for general AA in one study. In this specific study, the authors did not specify which kind of AA patients were dealing with.
- Mechanisms of action: Unknown, but probably a reduction in inflammation.
- Dosage: 2 drops thyme essential oil (EO), 3 drops lavender EO, 3 drops rosemary EO, 2 drops cedarwood EO diluted in 3mL jojoba oil and 20mL grapeseed oil.
- Outcomes: In this study, 54% of AA patients in the active group experienced hair regrowth over 7 months while 46% experienced no change (however, hair loss also did not get worse). A majority of these patients achieved hair regrowth in the 10-30% range, followed by 81-100%. In contrast, 78% of the placebo group did not improve, suggesting the essential oil mixture did, indeed, have an effect. It’s likely that the remaining 22% were experiencing spontaneous remission. Neither group experienced adverse side effects.
- Problems: It’s not clear just how many patients may benefit from EO application given that spontaneous resolution is a common occurrence. We see evidence of this in the placebo group, which may be a confounding factor in the measurement of treatment efficacy (since we don’t know how many in the active group would have resolved without intervention). Taking this into account, the response rate, when compared to other treatments for AA, is relatively low. Another issue is the fact that the study did not have a designated follow-up period to measure the rate of relapse. Therefore, we can’t be sure of just how effective this treatment is in the long run. Moreover, the treatment period was quite long in comparison to what is normally employed with other therapies. Given that AA can become more treatment-resistant as time goes on, using topical EOs may delay appropriate treatment and, as a result, require more aggressive therapies in the future.
Onion juice
- Best candidates: Men and women with patchy AA.
- Mechanisms of action: Unknown, but researchers believe it could work similarly to immunotherapy.
- Dosage: Application sufficient to cover the affected area(s) twice daily.
- Outcomes: This study found that patients with patchy AA were able to see hair regrowth as early as 2 weeks into the study period. Full hair regrowth was seen in 86.9% of patients after 8 weeks. Contrastingly, hair regrowth was only observed in 13% of the control group, making the findings of this study statistically significant.
- Problems: This study, unfortunately, had no follow-up period. As such, we don’t know how many patients experienced a relapse after cessation of treatment. Moreover, the smell of onion juice may make this treatment hard to adhere to long-term.
Garlic gel
- Best candidates: Men and women with mild patchy AA.
- Mechanisms of action: Unknown, but researchers believe it could work similarly to immunotherapy.
- Dosage: 5% garlic gel with 0.1% betamethasone valerate gel, twice daily.
- Outcomes: This study found that garlic was able to enhance the hair growth-promoting effects of a corticosteroid, betamethasone valerate. After 3 months, the active group was able to achieve a significant reduction of hair loss patches — more so than the corticosteroid topical alone.
- Problems: Like the onion juice study, this study (1) did not measure the rate of relapse after cessation of therapy and (2) fails to account for the smell, which may make the treatment difficult to adhere to in real-world settings.
Capsaicin
- Best candidates: Patients with patchy AA and, possibly, alopecia totalis.
- Mechanisms of action: Unknown, but researchers suspect neuroimmunological modulation in the hair follicle.
- Dosage: 0.075% capsaicin topical applied daily.
- Outcomes: Studies employing the use of capsaicin have show varying results. Some studies report the regrowth of vellus hairs, but no appreciable regrowth sufficient to justify its use over other treatments, while others report hair growth in just 3 weeks.
- Problems: Evidence suggests capsaicin may promote some degree of regrowth, but not enough to justify its use over other treatments — especially considering that AA becomes increasingly treatment-resistant over time. Thus, capsaicin use may delay appropriate treatment and, thus, increase the risk of refractory AA in the long-run.
Vitamin D repletion
- Best candidates: Patients with patchy AA and vitamin D deficiency and/or genetically reduced vitamin D receptor expression.
- Mechanisms of action: Likely a modulation of autoimmune activity in the follicle, due to vitamin D’s widespread effects on balancing the immune system.
- Dosage: For oral vitamin D use, the dosage will vary depending on the severity of vitamin D deficiency and whether your practitioner decides to opt for weekly bolus or daily doses. For topical vitamin D therapy, topical applications range from 0.005% calcipotriol twice daily to 50 micrograms/mL calcipotriol once daily.
- Outcomes: Evidence from meta-analyses show that AA patients are more likely to be vitamin D deficient than healthy controls. This would suggest that vitamin D could be beneficial to AA patients, however, no studies have been conducted to assess clinical benefit. The topical application of vitamin D-like, conversely, has been investigated as a treatment avenue. These studies show that twice daily application of various concentrations results that vary from 50% regrowth all the way to clinical remission (full hair regrowth). One study found that efficacy was associated with lower vitamin D levels at the beginning of the study, suggesting that lower vitamin D levels may be a marker of a good candidate. Additionally, one case report demonstrated full clinical remission in a patient with AA and reduced vitamin D receptor expression. Thus, AA patients with low vitamin D levels or reduced vitamin D receptor expression may have the best response to treatment. Studies also show minimal risk of adverse side effects.
- Problems: Studies do not currently show benefit in more severe cases of AA, like alopecia totalis or alopecia universalis. There is limited evidence investigating the therapeutic potential of oral supplements.
Zinc
- Best candidates: Patients with mild AA and zinc deficiency.
- Mechanisms of action: Unknown, but could be attributed to antioxidant regulation and anti-inflammatory activity.
- Dosage: Dosage depends on the severity of the deficiency, however, doses between 50 and 220mg have been used in the literature.
- Outcomes: Studies suggest AA patients have lower zinc levels compared to healthy controls. Interestingly, evidence also suggests a correlation between zinc levels and treatment resistance, meaning zinc deficiency may have an emerging role in refractory AA. However, some studies have failed to find a relationship between zinc and AA. Moreover, some studies show no benefit with zinc supplementation while others suggest zinc therapy may be beneficial in the context of mild AA with zinc levels below 70 μg/dL. Overall, the role of zinc therapy in AA is unclear other than zinc deficiency is more common among AA patients. Nonetheless, zinc repletion may confer health benefits in the presence of deficiency, even if clinical regrowth is not achieved.
- Problems: Research is mixed, with some studies suggesting benefit and others suggest a net zero effect. Thus, there is no conclusive evidence to support the use of zinc in AA.
Azelaic acid
- Best candidates: Patients with patchy AA.
- Mechanisms of action: Unknown, but preliminary evidence suggests it may act similarly to that of immunotherapy.
- Dosage: 20% azelaic acid topical applied twice daily.
- Outcomes: Evidence supporting the use of azelaic acid in patients with AA is lacking. However, one pilot study demonstrates efficacy on par with anthralin, a medication used to treat psoriasis (another autoimmune disease that affects the skin). Just over half of the patients tested achieved complete regrowth with both treatments with no report of adverse events.
- Problems: Research is limited and, as such, the true efficacy of azelaic acid is not known. Moreover, the aforementioned study did not employ a follow-up period, which is necessary to estimate the rate of relapse.
Platelet-rich plasma (PRP)
- Best candidates: Patients with ophiasis-pattern AA resistant to steroid treatment or AA patients who develop side effects with steroid treatment.
- Mechanisms of action: Unknown, possibly immunomodulatory effects.
- Dosage: 9 mL injection.
- Outcomes: In one case study of steroid-resistant ophiasis AA, a form of AA which is generally hard to treat, the patient was able to achieve regrowth by month 1 with significant regrowth by month 3. The patient reported no side effects. Another study demonstrated the superiority of PRP over steroid injections for patchy AA.
- Problems: Unfortunately, there is limited evidence available. The rate of relapse is unknown. The procedure is also costly.
Case study: ophiasis-type AA before and 3 months after PRP treatment.

Brotzu Lotion
Brotzu lotion is a topical formulated by Dr. Brotzu. It contains three main compounds: dihomo-gamma-linoleic acid, S-Equol, and propionyl-L-carnitine — ingredients designed to target inflammation and decreased blood flow in follicles.
There is currently no clinical evidence to support the efficacy of Brotzu lotion in AA. Nonetheless, some initial case studies do show promise. Take, for example, these two before-and-afters:
Brotzu Lotion: a child with alopecia universalis

And here’s a case of near-complete recovery of patchy AA in just 16 months from Dr. Brotzu’s presentation at this conference — start at 10:30):
Brotzu Lotion: alopecia areata recovery

While these are the only case studies we have pictures of, Dr. Brotzu’s patent cites more case studies. This is encouraging for AA patients — especially given it seems confer benefit even in more severe cases, of which are generally more likely to be resistant to treatment.
But it bears repeating: even Dr. Brotzu has claimed it’s difficult to know just how effective the lotion is for AA – mainly because of the spontaneous recoveries.
Helminthic therapy
Helminths, better known as hookworms, are tiny parasites that embed themselves in the small intestines of their hosts.
Helminths are unique in that they have a novel survival mechanism — one that might actually to a broader, modulatory effect on the whole immune system!
The specifics? Helminths “mute” the activity of T-cells, protecting them from destruction by the host’s immune system. This is accomplished through the stimulation of Tregs, a group of cells that reduce the inflammatory potential of the immune system.
As such, in theory, T-cell activity is modulated as a whole, reducing our reactivity to other reactive compounds — including our own tissue. Because auto-reactivity to our own tissue is what mediated autoimmunity (including in AA) reduced T-cell activity may also mean a reduced risk of autoimmunity.
And though research on helminth therapy is still in its infancy, preliminary studies suggest that this evidence might just translate to real-world efficacy. In fact, the therapy has shown promise for a variety of disorders, ranging from inflammatory bowel disorders to allergy all the way to mouse models of multiple sclerosis, an autoimmune disorder.
Considering this evidence, it’s not surprising that Moises Velasquez-Manoff, a male with alopecia totalis, reported hair growth for the first time in years following his experimentation with helminth therapy. He details his experience with helminth self-infection, alongside a historical perspective of helminth eradication, in his book: An Epidemic of Absence.
While this evidence alone is certainly not enough to warrant self-experimentation with helminth self-infection, this emerging research is compelling and underscores the growing importance of the symbiotic relationship of humans and microbes.
Success rates
As seen in the outcomes of the different studies, the likelihood of significant (or complete) recovery is relatively high. And, again, a large proportion of AA patients (34-50%) will spontaneously recover within one year.
This is great news! But, it also makes it difficult to effectively estimate the true success rate of treatments. So, is there any way that someone with AA might be able to gauge their likelihood of recovery (or lack thereof)?
Yes. In clinical practices, there are criteria for AA known as “poor prognostic factors” – i.e., things that might make you less likely to experience full hair recovery. According to the literature, these include:
- Bald patches that persist for longer than 1 year.
- Onset of hair loss before puberty.
- A family history of AA.
- Ophiasis pattern of AA.
- Associated nail changes, a.k.a when nail changes occur alongside AA.
- Atopy, a.k.a a propensity to developing allergic diseases like eczema, asthma, and allergic rhinitis.
So, if you fit into these categories, chances are your AA might be more treatment-resistant. That being said, it doesn’t mean you can’t recover your hair; it just means that you may need to explore more treatment avenues (or combination therapies) to find what works for your hair loss specifically. Your practitioner can help guide you through identifying these treatment avenues.
With that, you’ll also want to consult your doctor early into the process – as treatment resistance can increase as the condition progresses. As such, it’s better to forego experimental / home remedies and begin a treatment plan right away.
This isn’t to say natural therapies might not be an option for you, but, rather that you should discuss the evidence of those treatments with your doctor and, if suited to you, explore the therapy under their supervision.
This will help avoid treatment resistance that may result from delayed treatment, which would partly mitigate a major poor prognostic factor that is within your control.
Summary
Alopecia areata (AA) is a form of autoimmune hair loss characterized by inflammation, exclamation mark hairs, patchy hair loss (in early stages), and hair follicle miniaturization (in later stages). The condition can progress to alopecia totalis (loss of eyebrow and eyelash hairs) or alopecia universalis (loss of hair all over the body). But in many cases, it spontaneously reverses.
An autoimmune attack near the hair follicle stem cell bulge is what triggers AA-related hair loss. This results in inflammation, stem cell dysfunction, a malformed hair follicle, and thereby thiner, brittler hair that is prone to breakage. Eventually, hair cycling also becomes dysfunctional, leading to continued hair growth dysfunction and premature hair fall.
Thankfully, a large proportion of AA cases will spontaneously resolve within a year of onset. Having said that, it’s not a guarantee. So, while “waiting it out” may mean you need no treatment at all, it also poses a risk of progression. The further AA progresses, the higher the likelihood of treatment resistance.
So, it’s important that talk to your doctor when you first notice the hair loss. The earlier you catch it, the better your chances of regrowth. This is especially true if:
- Your hair loss began before puberty
- You have a family history of AA.
- Your hair loss is in the “ophiasis” pattern.
- Your hair loss is associated with nail changes.
- You have concurrent atopy (eczema, asthma, allergic rhintis).
Nevertheless, a wide array of treatment options do exist — both drug-based and non-drug-based – for manageable and refractory cases alike. Generally, corticosteroids are one of the first-line treatments. When corticosteroids aren’t effective, immunotherapy, methotrexate, JAK inhibitors, and alternative treatments (aromatherapy, vitamins/minerals, microbial modulation, and more) are usually explored.
Overall, the prognosis for most AA patients is good. Having said that, the risk of relapse is still high. This is mainly attributed to the fact that most treatments are confined to suppressing the signaling that leads to AA hair loss, as opposed to mitigating the root cause of AA. We just don’t know enough about the origin of AA to target these causes (yet).
The one exception to this rule might be fecal microbiota transplants (FMT) — a treatment that has shown major hair recoveries for long-standing AA patients (who typically don’t respond well to treatment), and no signs of relapse for those responders (at least within study windows of 1.5 to 3 years). However, evidence on FMT is incredibly limited. Moreover, the treatment is currently not readily accessible in the US (unless you have AA and you’re seeking treatment for a chronic C. difficile infection).
Overall, hair regrowth is absolutely possible for most AA patients — whether through natural or conventional means. Just make sure to get in touch with a doctor as soon as you notice your hair loss, so that they can help direct a treatment plan that’s going to be best suited to your condition.
If you have any questions, please feel free to leave them in the comments!
Scarring alopecias make up about 7% of patients seen in hair loss clinics. This means almost 1 in 10 hair loss cases are attributed to scarring alopecia.
In this article, we’ll outline what scarring alopecias are, what makes them unique, and why they might develop. Then we’ll uncover why this classification of hair loss – scarring vs. non-scarring – might be a bit outdated.
Finally, we’ll reveal new research that’s changing the way we think about scarring forms of hair loss. Historically, scarring alopecias have been considered irreversible. But new case reports are showing just the opposite: that some people with scarring alopecias can achieve significant – and sometimes complete – hair regrowth.
We’ll dive into why this is important, how this may impact treatment avenues, and what you can do to start combatting the progression of scarring alopecias today, both naturally and conventionally.
What are scarring alopecias?
Scarring alopecias are an umbrella term for hair loss from the rapid destruction and scarring of hair follicles.
There are several types of scarring alopecias (1), and each type varies by its presentation and causes:
- Central centrifugal cicatricial alopecia (CCCA). A type of hair loss that occurs predominantly in African American women. Characterized by a progressive thinning that begins in the center of the scalp and gradually expands to the peripheral regions. The only feature that distinguishes it from female pattern hair loss is the lack of visible follicles in the affected areas and a shiny, smooth scalp. It was once believed to be caused by hair styling techniques; however, recent data (2) has refuted that claim.
- Frontal fibrosing alopecia. This type of scarring alopecia occurs in a band-like distribution in the front of the hair and may also be present in the eyebrows. It mostly affects postmenopausal women. It predominantly affects the hairline, leading to uniform recession as if the hairline marched backward.
- Lichen planopilaris. Patchy hair loss with itchiness, scaling, and visible redness in affected areas. It might also affect non-scalp areas. It sometimes presents as diffuse thinning.
- Chronic cutaneous lupus erythematosus. Patchy, scarring hair loss as a result of an autoimmune disorder: lupus. Onset of this type of scarring alopecia may result from UV exposure, though research hasn’t yet confirmed this.
- Pseudopelade of Brocq. Small and/or large irregular patches of hair loss with no signs of inflammation.
- Folliculitis decalvans. A single patch of hair loss that progressively expands. Typically found on the peripheral regions of the scalp. Affected areas may have pustules, honey-colored crusting, and tufting.
- Dissecting cellulitis of the scalp. Multiple, red, inflamed, and interconnected nodules that erupt from various scalp regions in somewhat of a web-like pattern. It may also be associated with acne conglobota.
How do scarring alopecias happen?
No one is quite sure. However, many researchers believe scarring alopecias are caused by an interaction between inflammation, our immune systems, and (potentially) our hormones.
Similar to other hair loss disorders, the step-process for developing a scarring alopecia seems to be:
Inflammation >> scarring >> hair loss
You might see this step-process and think it looks a lot similar to other hair loss disorders, like androgenic alopecia (AGA). At face-value, you’re right. But there are a few differences that make scarring alopecias unique.
- In scarring alopecias, the location of inflammation is in the hair follicle stem cell bulge; in androgenic alopecia, it’s in the infundibulum (upper third of the hair follicle) and likely deeper below the hair follicles, but above the galea aponeurotica.
- In scarring alopecias, the nature of inflammation in unknown and/or autoimmune-related; in androgenic alopecia, the inflammation is likely related to scalp tension, pathogenic microorganisms, and accelerated hair cycling.
It might seem absurd to distinguish scarring alopecias from androgenic alopecia by the nature and location of inflammation. After all, our hair follicles are already tiny “mini-organs”. What difference does it make if one hair loss disorder’s source of inflammation is just a couple of nanometers away from another’s?
Apparently, a lot. And this is because across hair loss disorders, the location of inflammation predicts where scarring will occur, which predicts what these hair loss disorders will end up looking like.
This is why, in the later stages, androgenic alopecia and scarring alopecias look so different:

With scarring alopecias, the inflammation is far more widespread, so the scarring ends up wiping out the entire hair follicle – the stem cell bulges, sebaceous glands, arrector pili muscles, and hair shaft.
In androgenic alopecia, the scarring remains clustered around the hair follicle. Subsequently, the scarring doesn’t wipe out these other components of our hair follicles until many years into AGA’s progression.
In scarring alopecias, why do a hair follicle’s stem cell bulges become inflamed?
No one is quite sure. While researchers have identified dozens of potential triggers (3) across patients with scarring alopecias…
- Sebaceous gland dysfunction
- Substance P transmission (a neuropeptide released during stress)
- Deficiency in PPAR signaling
- Collapse of hair follicle immune privilege (the hair follicle is generally resistant against to damage by the immune system)
- Bacterial infection
- Abnormal cellular changes
- Genetic factors
- Hairstyling
- Certain drugs (anticonvulsants, hepatitis B vaccine, cyclosporin)
- Autoimmunity
- Sunscreen use on the forehead
…It’s still unclear which causes might apply to each case, why our hair follicle’s stem cell bulges become inflamed, and why this inflammation becomes persistent in the first place.
It all seems to begin with a miscommunication between an inflammatory stimulant, our immune systems, and our hair.
The miscommunication: inflammatory stimulants, myofibroblasts, and beyond
During a normal inflammatory process, the body encounters some sort of inflammatory stimulus – a wound, a virus, or even an environmental irritant. This stimulus is identified by the immune system as foreign, at which point our immune system recruits cells to “attack” the foreign invader. This leads to inflammation (i.e., tissue swelling), which in many cases, is enough to kill off the foreign invader. Once the threat is gone, the immune system signals these cells to stop attacking, and the inflammation dissipates, leaving us the same as we were prior to the attack.
In scarring alopecias, this process does not go according to plan.
During scarring alopecias, our immune system picks up on a foreign threat and sends a group of cells called myofibroblasts to start attacking. These myofibroblasts have a number of roles in the body – three of which are (1) enhancing the inflammatory response, (2) supporting the healing process, and (3) producing proteins like collagen (which, if produced in a disorganized fashion, form the building blocks of scar tissue).
Under normal settings, myofibroblasts would help enhance the inflammatory response until the foreign threat is destroyed, at which point the myofibroblasts would no longer be needed. At this point, the myofibroblasts would then help to repair the damage caused by inflammation by laying down new collagen fibers (i.e., skin tissues). Then, these myofibroblasts would die off.
However, in the case of scarring alopecias, myofibroblasts fail to die off. To put it simply, there’s a disruption in the normal cell signaling that tells our myofibroblasts that they’re no longer needed. As a result, they continue to lay down collagen, which becomes excessive and disorganized, which then turns to scar tissue.
Subsequently, functional tissue begins to be replaced by poorly-functioning scar tissue. As the fibrosis continues, the affected organs continue to lose functionality. We see this in conditions like cirrhosis, scleroderma, and pulmonary fibrosis (fibrosis of the lungs) – for example, where fibrosis makes it difficult for the liver, skin, and lungs to do their job.
This is exactly what happens in the hair follicle during scarring alopecia.
Infection and sustained inflammation begin to severely damage the hair follicle. And unfortunately, this scarring process ends up destroying our hair follicle stem cell bulges. This stem cell bulge is incredibly important; it contains the “blueprints” – or the building blocks – of each hair follicle. And without a hair follicle stem cell bulge, our hair follicles have no blueprints to follow for replication.
This leads to the complete destruction of the hair follicle… and the scarring of its surrounding skin. And as you can imagine, this is not a position most hair loss sufferers want to be in.
Are scarring alopecias reversible?
Traditionally, researchers have generally held the stance that scarring alopecias aren’t reversible.
This is because of the fact that scarring alopecias (1) lead to widespread scarring of an entire skin region, and thereby (2) wipe out the hair follicle stem cell bulges. For these reasons, many researchers have held onto the belief that scarring alopecias are irreversible – and that the best we can do is slow or stop their progression.
Encouragingly, this belief is now changing. Why? Because new evidence is showing that scarring alopecias are not only theoretically reversible, but that we actually have case studies of this happening. It’s all a matter of unlocking how to do it on a consistent basis.
Here’s why we believe this is possible.
#1: AGA, which also leads to scarring, is reversible even in its latest stages.
To reiterate from earlier, end-stage AGA closely resembles that of end-stage scarring alopecias. In both conditions, we see so much fibrosis (scarring), that there’s a total loss of follicular integrity.

Having said that, even in late stages of androgenic alopecia, we’ve seen pretty significant hair regrowth. This is obvious with examples from a few of our case studies from our membership community – like Mike and Raul – who used natural methods to see regrowth beyond what is typically observed with conventional treatments.
Mike’s Regrowth

Raul’s Regrowth


But perhaps the most impressive example of hair regrowth from advanced AGA happened entirely by accident.
In 1986, a 78-year man who’d been bald for 30+ years fell asleep in his rocking chair. Inadvertently, he slumped over, landed head-first onto hot coals, and received second degree burns across much of his scalp.
He refused to be treated at the hospital and was eventually sent home as an outpatient. Four months later, he returned for a checkup. During that time from the injury, he’d accidentally regrown his entire juvenile hairline (4).

Remember: in advanced cases of AGA, a hair follicle’s stem cell bulges appear either scarred or completely depleted. This implies an inability for hair recovery. Yet here, we see a case of complete hair recovery… just the opposite of what we’d expect.
And as we dig deeper into the research on scarring alopecias, we can find plenty of cases where recoveries happen, too.
#2: scarring alopecias have been reversed before!
There are several case studies of people with scarring alopecias regrowing significant amounts of hair. In some cases, the hair recovers completely.
In some cases, this has happened with interventions as simple as stopping the use of facial sunscreen (5). In other cases, significant regrowth came after using topical metformin (6). In one case of lupus-related scarring alopecia, complete hair regrowth was observed within three months following the use of hydroxychloroquine (7). And in cases of frontal fibrosing alopecia, oral finasteride led to near-complete hairline regrowth after just 12 months (8).
In light of these findings, there are really only two explanations:
- In scarring alopecias, stem cell bulges aren’t totally lost. Therefore, the hair is still recoverable. Or…
- Our understanding of hair follicle stem cell bulges needs to be revised. Maybe hair follicles can regenerate in the absence of stem cells, and through not-yet-discussed processes, like that of follicle-to-follicle communication.
Let’s explore that second idea for a second, as it may shape the next decade of hair loss research.
What do we know about follicle-to-follicle communication?
Follicle-to-follicle communication is a phenomenon that was originally observed in one fascinating study (9) – the findings of which we described in this article. To summarize:
In 2015, researchers wanted to see if hair follicles could communicate with each other to coordinate behaviors – like making new hair follicles. So they set up a test…
They plucked 200 hairs from the backs of mice… but did so while controlling for the diameter of a plucking region. In some cases, 200 hairs were plucked in a 2.4mm region. In other cases, 200 hairs were plucked from an 8mm region. The smaller the region, the higher-density the plucking – and vice-versa.
The goal: to see if hair follicle behavior changed on how closely hairs were plucked from one another. So they measured hair growth over the next several weeks.
The results were fascinating.
With low-density plucking, hair follicles either didn’t grow back at all… or grew back to their normal pre-plucking densities. That’s what we would expect to happen.
But with higher-density plucking, additional hair follicles were created… to the tune of a five-fold increase.
What’s more interesting is why this happened. The researchers theorized that higher-density plucking created more inflammatory signaling, which led to more cross-communication between hair follicles directly next to each other, which signaled to hair follicles to start regenerating – regardless of whether they’d been plucked.
The end-result: a huge increase in hair.
The implications? That nearby hair follicles can communicate with one another (!), and that these communications must include signaling for hair follicle regeneration. Based on this study, it’s clear that healthy hair follicles can coordinate regeneration with damaged hair follicles.
So, how does this relate to scarring alopecia?
Considering hair loss from scarring alopecia is a result of complete hair follicle destruction, and considering that this destruction has puzzlingly reversed itself across many case studies…
We can presume that follicle-to-follicle communication is playing a role here, and that understanding this role (and harnessing this cellular crosstalk) is probably one way people with scarring alopecias can unlock huge hair recoveries.
So, how do we do this?
We don’t yet know! Research is still emerging, and as it continues to evolve, we’ll update this article.
In the meantime, there’s plenty we can do to stop the progression of scarring alopecias – and potentially even see major recoveries.
What are the current treatments for scarring alopecias?
Step 1: connect with a dermatologist
The first step is always making an appointment with a dermatologist. By understanding what kind of scarring alopecia you have, you can better target your treatment regimens to save yourself time, effort, and money.
Step 2: identify and remove any potential inflammatory “triggers”
Once you’ve scheduled your appointment, one of the most critical next steps is to make your best effort to identify and remove some of the most common triggers of scarring alopecias. This will be highly individual and dependent, again, on the type of scarring alopecia with which you’re diagnosed.
Here are a few of the common inflammatory stimulants suspected in scarring alopecias:
- Sunscreen use: there is a weak link between sunscreen use and frontal fibrosing alopecia (FFA) (5). Some researchers hypothesize this could be due to decreased sebum production during the time in which a woman is most likely to be affected by FFA, menopause. This results in an inability to clear topical products, like sunscreen, from the follicle, potentially leading to an autoimmune reaction. Other researchers have proposed an alternate view: with the anti-inflammatory, immunomodulatory effects of UV light, blocking UV light (using sunscreen) may actually encourage autoimmunity in the follicle. Cessation of sunscreen use has been shown to produce noticeable regrowth in as little as 6 months with an almost full recovery in 36+ months.
- Hairstyling: While studies have failed to establish hairstyling as the sole cause of CCCA, certain hairstyling techniques may contribute to at least some cases of scarring alopecia. If you find yourself dealing with a potential case of scarring alopecia and you regularly receive hair relaxant treatments, employ hot combing, or style your hair in braids, cornrows, or using other traction styling methods (10) – it might be best to avoid these treatments and/or stylings (or at least reduce their frequency) until you can rule out their potential involvement.
- Environmental toxins as inducers of autoimmunity: Autoimmunity is one of the purported causes underpinning the development of scarring alopecia. This is due to the fact that the stem cell bulge of the follicle is normally a site of immune privilege, meaning it is usually protected from the action of the immune system. However, autoimmune processes can actually cause this immune privilege to be lost. Interestingly, environmental toxins have the ability to induce autoimmunity. For this reason, avoidance of environmental triggers linked to autoimmunity, like rancid vegetable oils, mineral oils, and sources of heavy metals, is a good precautionary measure (11).
- UV exposure: Some causes of scarring alopecia, like chronic cutaneous lupus erythematosus, are exacerbated by UV exposure. Use of sunscreen or UV-blocking clothing/hats may be needed to prevent the worsening of lesions that contribute to hair loss.
Step 3: settle on a treatment approach
There are two ways we can approach this: drug-based treatments and non-drug treatments.
We’ve divided these interventions into their respective sections and described who these treatments might be best for, which dosages are used in the literature (where applicable), the outcomes of the research, and what potential issues might arise with each given treatment.
Drug-based treatments
Topical, intralesional, and oral corticosteroids:
- Best candidates: Most forms of scarring alopecia, patients with CCCA not related to traumatic hair styling.
- Dosages: 10mg/mL for intralesional injections every 6-8 weeks; 25-40mg per day for 2-4 months with oral corticosteroids (1).
- Outcomes: Corticosteroid treatment, in any form of administration is mostly limited to halting the progression of disease as it doesn’t address the scarring that impedes hair follicle regeneration. Can promote regrowth in some patients with dissecting cellulitis (12).
- Problems: Oral corticosteroids are limited to severe/rapidly progressing disease; topical corticosteroid treatment can result in skin atrophy, a.k.a thinning of the skin.
Hydroxychloroquine:
- Best candidates: Patients with frontal fibrosing alopecia, lichen planopilaris, and chronic cutaneous lupus erythematosus.
- Dosages: Below 7.5/mg/kg for lichen planopilaris and frontal fibrosing alopecia, 400mg daily during summer months with chronic cutaneous lupus erythematosus and smaller doses during winter (1).
- Outcomes: Effective at decreasing signs and symptoms of lichen planopilaris and frontal fibrosing alopecia and preventing further hair loss, effectively resolve lesions related to chronic cutaneous lupus erythematosus (13), full hair regrowth has been observed with hydroxychloroquine in at least one case of lupus-related alopecia (7).
- Problems: Studies are often too short to estimate the true incidence of retinopathy at dosages used for these conditions.
Antibiotics (Minocycline, rifampicin, fusidic acid):
- Best candidates: Patients with folliculitis decalvans.
- Dosages: 300mg rifampicin 2x daily (should not be used as a monotherapy, which can promote antibiotic resistance), combination of 300mg rifampicin, 300mg clindamycin, and fusidic acid along with topical corticosteroid lotion for 3 months has been used with success, topical clindamycin or benzoyl peroxide can control mild cases, oral antibiotics are needed for more severe cases (1).
- Outcomes: Effective at addressing the infection that leads to folliculitis decalvans, but not restoring the hair lost.
- Problems: Rifampicin is the preferred antibiotic because it is highly lipid-soluble (the scalp environment is very lipidic) and accumulates in high quantities in the hair follicle, however, antibiotic resistance is a major issue with its use.
Topical metformin:
- Best candidates: Who topical metformin might be best for is still unclear, as research is preliminary, but case studies have demonstrated success in CCCA patients (6).
- Dosages: 10% topical metformin with the potential for higher concentrations if the patient responds well to the treatment.
- Outcomes: Although research is preliminary, there have been two cases of partial regrowth in CCCA – traditionally believed to be irreversible (and notoriously difficult to treat) (6).
- Problems: Preliminary research suggests there is little to no systemic side effects. Instead, side effects are usually superficial and limited to scalp dryness and irritation.
Oral Isotretinoin (Accutane®):
- Best candidates: Patients with dissecting cellulitis and cases of chronic cutaneous lupus erythematosus resistant to antimalarial therapies like hydroxychloroquine.
- Dosages: 0.5-1mg/kg daily for dissecting cellulitis (1).
- Outcomes: Usually produces rapid results in chronic cutaneous lupus erythematosus, treatment for 6-11 months in dissecting cellulitis shrinks lesions and can even induce periods of long remission.
- Problems: Oral isotretinoin can cause large quantities of hair follicles to prematurely enter the telogen phase, which can lead to diffuse shedding (1). The risk of disease progression should be weighed carefully against the potential risk of increased shedding.
Finasteride:
- Best candidates: Patients with frontal fibrosing alopecia.
- Dosages: 2.5mg daily (14).
- Outcomes: Some studies suggest finasteride is the most effective therapy for treating frontal fibrosing alopecia. Patients with this condition can expect a response rate of about 50% with finasteride alone (14). At least one case report demonstrated marked regrowth and a reversal of skin atrophy (i.e., skin thinning) (8).
- Problems: In women with already low or normal androgen levels, finasteride could produce sexual/mental side effects.
Non-drug treatments
Microneedling + platelet-rich plasma:
- Best candidates: Unknown.
- Methods: 20 sessions spaced 2 weeks apart.
- Outcomes: Clinical improvement in one case of general scarring alopecia – the details of this clinical improvement aren’t specified (i.e., improvement of inflammatory lesions vs. actual hair regrowth)
- Problems: Likely cannot be used to treat some forms of scarring alopecia like folliculitus decalvans, at least in their active infection phase, due to the bacterial nature of the condition.
Low level light/laser therapy (LLLT):
- Best candidates: Patients with lichen planopilaris.
- Methods: 272 pulsed laser diode cap with 1360 mW total output
- Outcomes: Case reports suggest lichen planopilaris patients may be able to achieve hair regrowth with the use of LLLT (15).
Excimer laser (UV-B light)
- Best candidates: Patients with lichen planopilaris and some cases of frontal fibrosing alopecia.
- Methods: Sessions as frequent as twice weekly with an average of 10 sessions reported in the literature.
- Outcomes: Studies have demonstrated a decrease in inflammation, as well as some instances of hair regrowth (16).
Hair Transplants
We know from the literature that there are some cases of scarring alopecia that are reversible. But, what if your hair doesn’t grow all the way back, even with the best-of-the-best treatment?
This is where hair transplants might be useful.
Hair transplants in scarring alopecias are different than hair transplants for non-scarring hair loss disorders. While grafts in non-scarring alopecias have a 90% survival rate, scarring alopecias may only have an average 50% survival rate.
But, transplants don’t have to be a stab in the dark. We can usually predict whether or not a transplant is going to be successful by (1) understanding what kind of scarring alopecia you have, and (2) performing a pre-surgery transplant test.
We’ve compiled the types of scarring alopecias that are more likely to see success from a transplant vs. those that might not:
Scarring alopecias more likely to receive transplants successfully
Scarring alopecias where hair transplants are less likely to survive Central centrifugal cicatrial alopecia (CCCA) Lichen planopilaris Discoid lupus erythematosus Frontal fibrosing alopecia Pseudopelade brocq Folliculitis decalvans However, the safest way to estimate your individual tolerance to a hair transplant is to have a dermatologist perform a pre-surgery transplant test.
But, what if your chances of hair transplant survival end up being low? Or what if hair transplants are too expensive? Or too invasive? What are the options, then?
In these cases, there is one additional option.
Artificial hair integrations
For treatment-resistant and/or transplant-intolerant cases or for those who aren’t comfortable with the price or the procedure, the next best option is artificial hair integrations.
The good news is that these are inexpensive and readily accessible – and something you can begin to use right away. But, you’ll want to be absolutely sure that these integrations aren’t putting any additional strain on existing hair, as this can do more harm than good. In some cases, it may trigger a case of traction alopecia or, worse, a new case of scarring alopecia.
So, to recap, here’s a sequential approach you should consider for treatment:
- Make a dermatologist appointment to identify what kind of scarring alopecia you might have (if any).
- Identify and remove any potential triggers.
- Based on what type of scarring alopecia you have, explore some treatment avenues provided and discuss them with your dermatologist.
- If you aren’t able to achieve full recovery, explore hair transplants. Performing a pre-surgery transplant test can help you gauge whether or not a transplant will survive on your scalp.
- If you are intolerant to transplants and/or aren’t comfortable with the price or the procedure itself, artificial hair integrations are relatively inexpensive and very accessible.
Summary
Scarring alopecias are relatively uncommon; they constitute just 7% of hair loss diagnoses in hair loss clinics. Having said that, they’re characterized by aggressive scarring. This scarring leads to the destruction of skin tissue surrounding hair follicles, as well as the destruction of stem cell bulges which make hair follicles and the hair follicles themselves. Consequently, many researchers have historically considered that scarring alopecias are irreversible.
This is no longer the case. Case reports of full hair recoveries from scarring alopecias, alongside evidence that healthy hair follicles and unhealthy hair follicles can actually communicate with each other, now leads researchers to believe that scarring alopecias are reversible… we just don’t know how to do it consistently (yet).
Because scarring alopecias are less common, there are still many questions researchers have yet to answer:
- Why are some cases of scarring alopecias reversible, if all scarring alopecias are believed to result in a loss of the stem cell bulge?
- If there are at least some scarring alopecias that happen to retain stem cells, could there be an overlap in treatments with AGA? In other words, could some scarring alopecia patients benefit from AGA treatments that address fibrosis?
- If stem cells aren’t retained, is there some other regenerative process, like follicle-to-follicle communication, at play?
As researchers attempt to answer these questions, there are still some great treatments out there for scarring alopecia patients – both drug-based and drug-free, that have shown clear benefit. While most are limited to improving symptoms and slowing or halting the progression of hair loss, some patients are seeing partial and/or full recoveries.
For those who find their hair loss is treatment-resistant or want to restore hair lost to scarring alopecia, hair transplants are a decent option. However, they can be a hit or miss, being that the transplant survival rate is around 50% (vs. 90% for other hair loss types). You can maximize your chances of survival by identifying what kind of scarring alopecia you’re dealing with as well as performing a pre-surgery transplant test.
Artificial hair integrations are also a great option — and one much cheaper and more accessible than hair transplants. However, it is of the utmost importance that these are applied correctly to avoid undue strain on healthy hair (which may trigger the onset of new hair loss).
Have any questions about the new treatments for or emerging research on scarring alopecia? Please let us know in the comments section below.
References
- Filbrandt R, Rufaut N, Jones L, Sinclair R. Primary cicatricial alopecia: diagnosis and treatment. CMAJ. 2013;185(18):1579-1585. doi:10.1503/cmaj.111570
- Subash J, Alexander T, Beamer V, McMichael A. A proposed mechanism for central centrifugal cicatricial alopecia. Exp Dermatol. 2020;29(2):190-195. doi:10.1111/exd.13664
- Harries MJ, Paus R. The pathogenesis of primary cicatricial alopecias. Am J Pathol. 2010;177(5):2152-2162. doi:10.2353/ajpath.2010.100454
- Buckland R, Wilson GR, Sully L. Effect of scalp burns on common male pattern baldness. Br Med J (Clin Res Ed). 1986;293(6562):1645. doi:10.1136/bmj.293.6562.1645-a
- Robinson G, McMichael A, Wang SQ, Lim HW. Sunscreen and frontal fibrosing alopecia: A review. J Am Acad Dermatol. 2020;82(3):723-728. doi:10.1016/j.jaad.2019.09.085
- Araoye EF, Thomas JAL, Aguh CU. Hair regrowth in 2 patients with recalcitrant central centrifugal cicatricial alopecia after use of topical metformin. JAAD Case Rep. 2020;6(2):106-108. Published 2020 Jan 22. doi:10.1016/j.jdcr.2019.12.008
- Igari S, Yamamoto T. Dramatic effect of hydroxychloroquine on lupus alopecia. J Dermatol. 2018;45(2):194-197. doi:10.1111/1346-8138.14069
- Donovan JC. Finasteride-mediated hair regrowth and reversal of atrophy in a patient with frontal fibrosing alopecia. JAAD Case Rep. 2015;1(6):353-355. Published 2015 Sep 30. doi:10.1016/j.jdcr.2015.08.003
- Chen CC, Wang L, Plikus MV, et al. Organ-level quorum sensing directs regeneration in hair stem cell populations. Cell. 2015;161(2):277-290. doi:10.1016/j.cell.2015.02.016
- Herskovitz I, Miteva M. Central centrifugal cicatricial alopecia: challenges and solutions. Clin Cosmet Investig Dermatol. 2016;9:175-181. Published 2016 Aug 17. doi:10.2147/CCID.S100816
- Pollard KM, Hultman P, Kono DH. Toxicology of autoimmune diseases. Chem Res Toxicol. 2010;23(3):455-466. doi:10.1021/tx9003787
- Whiting DA. Cicatricial alopecia: clinico-pathological findings and treatment. Clin Dermatol. 2001;19(2):211-225. doi:10.1016/s0738-081x(00)00132-2
- Takezawa K, Ueda-Hayakawa I, Yamazaki F, Kambe N, Son Y, Okamoto H. Successful treatment with hydroxychloroquine for systemic lupus erythematosus with cutaneous involvement accompanied by a xanthomatous reaction. Lupus. 2020;29(1):79-82. doi:10.1177/0961203319890677
- Fertig R, Tosti A. Frontal fibrosing alopecia treatment options. Intractable Rare Dis Res. 2016;5(4):314-315. doi:10.5582/irdr.2016.01065
- Randolph MJ, Salhi WA, Tosti A. Lichen Planopilaris and Low-Level Light Therapy: Four Case Reports and Review of the Literature About Low-Level Light Therapy and Lichenoid Dermatosis. Dermatol Ther (Heidelb). 2020;10(2):311-319. doi:10.1007/s13555-020-00359-x
- Gamret AC, Potluri VS, Krishnamurthy K, Fertig RM. Frontal fibrosing alopecia: efficacy of treatment modalities. Int J Womens Health. 2019;11:273-285. Published 2019 Apr 29. doi:10.2147/IJWH.S177308
IngredientsPharmaceuticalsNatural RemediesCompany Reviews
By Sarah King, PhDAug 21, 2024NR3C1: Can This Gene Predict Responsiveness to Glucocorticoids?
The NR3C1 gene codes for the glucocorticoid receptor, a key player in the regulation of metabolism, immune response, and stress adaptation. Variations in the NR3C1 gene, such as the rs6198 SNP, have been linked to differences in glucocorticoid sensitivity with some variants leading to increased expr...
By Sarah King, PhDAug 21, 2024PTGES2: Can This Gene Predict Regrowth from Minoxidil?
The PTGES2 gene encodes the enzyme prostaglandin E synthase 2, which is crucial for converting prostaglandin H2 to prostaglandin E2 (PGE2). This enzyme plays a significant role in various physiological processes, including inflammation and hair growth. Research has indicated that an SNP in the PTGES...
By Sarah King, PhDAug 21, 2024PGTFR: Can This Gene Predict Regrowth From PGF2a Analogs?
Can your genes predict the effectiveness of PGF2α analogs for hair loss? The PGFTR gene, encoding the prostaglandin F2 alpha (PGF2α) receptor, is a potential target in hair loss treatment. Prostaglandin F2α and its analogs like latanoprost have been shown to stimulate hair follicle growth, making PG...
By Ben Fletcher, PhDAug 20, 2024IGF1R: Can This Gene Predict Regrowth From IGF-1?
The IGF1R gene encodes the insulin-like growth factor-1 receptor, which is integral to the IGF signaling pathway, particularly in processes like growth and development. Variations in the IGF1R gene, such as the rs2229765 polymorphism, have been linked to differences in circulating IGF-1 levels, with...
By Ben Fletcher, PhDAug 6, 2024SRD5A1 & 2: Can These Genes Predict Regrowth From 5-Alpha-Reductase Inhibitors?
Can your genes predict the effectiveness of 5α-reductase inhibitors for hair loss? The SRD5A1 and SRD5A2 genes, encoding type I and type II 5α-reductase respectively, are central to DHT production, a key factor in the pathogenesis of androgenic alopecia. Genetic testing companies suggest certain SR5...
By Sarah King, PhDJul 16, 2024GPR44: Can This Gene Predict Hair Regrowth From PGD2 Inhibitors?
Can your genes predict the effectiveness of PGD2 inhibitors for hair loss? The GPR44 gene, encoding the prostaglandin D2 receptor (DP2), is a potential target in hair loss treatment. Elevated levels of prostaglandin D2 (PGD2) have been linked to hair growth inhibition, making GPR44 a key player. How...
By Sarah King, PhDJul 16, 2024SULT1A1: Can This Gene Predict Hair Regrowth From Minoxidil? | The Evidence
Can your genes predict minoxidil effectiveness? The SULT1A1 gene, which encodes sulfotransferase, might hold the key, at least according to gene testing companies. SULT1a1 codes for an enzyme that activates minoxidil, a common hair loss treatment. While some studies suggest certain SULT1A1 variants ...
By Sarah King, PhDMay 31, 2024Microneedling the Scalp: Does it Cause Scarring?
Can repeated microneedling on the scalp cause scarring? There aren’t yet long-term studies answering this question. On the one hand, microneedling increases neocollagenesis (i.e., the formation of new collagen, or skin tissue). On the other hand, studies show that microneedling-induced collage...
By Sarah King, PhDMay 9, 2024Pyrilutamide (KX-826): A Promising Future Treatment For Hair Loss?
Pyrilutamide, also known as KX-826, is an anti-androgen topical currently being tested for the treatment of androgenic alopecia (AGA). Initial studies suggested that pyrilutamide might help reverse hair loss. However, larger-scale clinical studies have found no significant differences in hair regrow...
By Sarah King, PhDMay 9, 2024HMI-115: What We Know So Far
HMI-115 lowers prolactin levels and is currently in clinical trials for the treatment of androgenic alopecia (AGA). Internal, non-peer-reviewed research suggests that HMI-115 may promote hair regrowth in monkeys. Anecdotes from its phase I trials in humans imply that HMI-115 may also regrow hair in ... - Mission Statement
 Scroll Down
Scroll Down More
More More
More