- About
- Mission Statement
Education. Evidence. Regrowth.
- Education.
Prioritize knowledge. Make better choices.
- Evidence.
Sort good studies from the bad.
- Regrowth.
Get bigger hair gains.
Team MembersPhD's, resarchers, & consumer advocates.
- Rob English
Founder, researcher, & consumer advocate
- Research Team
Our team of PhD’s, researchers, & more
Editorial PolicyDiscover how we conduct our research.
ContactHave questions? Contact us.
Before-Afters- Transformation Photos
Our library of before-after photos.
- — Jenna, 31, U.S.A.
I have attached my before and afters of my progress since joining this group...
- — Tom, 30, U.K.
I’m convinced I’ve recovered to probably the hairline I had 3 years ago. Super stoked…
- — Rabih, 30’s, U.S.A.
My friends actually told me, “Your hairline improved. Your hair looks thicker...
- — RDB, 35, New York, U.S.A.
I also feel my hair has a different texture to it now…
- — Aayush, 20’s, Boston, MA
Firstly thank you for your work in this field. I am immensely grateful that...
- — Ben M., U.S.A
I just wanted to thank you for all your research, for introducing me to this method...
- — Raul, 50, Spain
To be honest I am having fun with all this and I still don’t know how much...
- — Lisa, 52, U.S.
I see a massive amount of regrowth that is all less than about 8 cm long...
Client Testimonials150+ member experiences.
 Scroll DownPopular Treatments
Scroll DownPopular Treatments- Treatments
Popular treatments. But do they work?
- Finasteride
- Oral
- Topical
- Dutasteride
- Oral
- Topical
- Mesotherapy
- Minoxidil
- Oral
- Topical
- Ketoconazole
- Shampoo
- Topical
- Low-Level Laser Therapy
- Therapy
- Microneedling
- Therapy
- Platelet-Rich Plasma Therapy (PRP)
- Therapy
- Scalp Massages
- Therapy
 More
More
IngredientsTop-selling ingredients, quantified.
- Saw Palmetto
- Redensyl
- Melatonin
- Caffeine
- Biotin
- Rosemary Oil
- Lilac Stem Cells
- Hydrolyzed Wheat Protein
- Sodium Lauryl Sulfate
 More
More
ProductsThe truth about hair loss "best sellers".
- Minoxidil Tablets
Xyon Health
- Finasteride
Strut Health
- Hair Growth Supplements
Happy Head
- REVITA Tablets for Hair Growth Support
DS Laboratories
- FoliGROWTH Ultimate Hair Neutraceutical
Advanced Trichology
- Enhance Hair Density Serum
Fully Vital
- Topical Finasteride and Minoxidil
Xyon Health
- HairOmega Foaming Hair Growth Serum
DrFormulas
- Bio-Cleansing Shampoo
Revivogen MD
- more
Key MetricsStandardized rubrics to evaluate all treatments.
- Evidence Quality
Is this treatment well studied?
- Regrowth Potential
How much regrowth can you expect?
- Long-Term Viability
Is this treatment safe & sustainable?
Free Research- Free Resources
Apps, tools, guides, freebies, & more.
- Free CalculatorTopical Finasteride Calculator
- Free Interactive GuideInteractive Guide: What Causes Hair Loss?
- Free ResourceFree Guide: Standardized Scalp Massages
- Free Course7-Day Hair Loss Email Course
- Free DatabaseIngredients Database
- Free Interactive GuideInteractive Guide: Hair Loss Disorders
- Free DatabaseTreatment Guides
- Free Lab TestsProduct Lab Tests: Purity & Potency
- Free Video & Write-upEvidence Quality Masterclass
- Free Interactive GuideDermatology Appointment Guide
- More
Articles100+ free articles.
-
Which Hormones Cause Hair Loss in Females?
-
Does Zepbound Cause Hair Loss?
-
Does Wegovy Cause Hair Loss?
-
Strut Health Review: 5 Things to Consider Before Purchasing
-
Does Tirzepatide Cause Hair Loss?
-
Musely Reviews for Hair Loss: Are They Trustworthy?
-
Best Minoxidil for Women: Top 6 Brands of 2026
-
Best Topical Finasteride: 5 Top Products of 2026
PublicationsOur team’s peer-reviewed studies.
- Microneedling and Its Use in Hair Loss Disorders: A Systematic Review
- Use of Botulinum Toxin for Androgenic Alopecia: A Systematic Review
- Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia
- Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results
- A Hypothetical Pathogenesis Model For Androgenic Alopecia:Clarifying The Dihydrotestosterone Paradox And Rate-Limiting Recovery Factors
Menu- AboutAbout
- Mission Statement
Education. Evidence. Regrowth.
- Team Members
PhD's, resarchers, & consumer advocates.
- Editorial Policy
Discover how we conduct our research.
- Contact
Have questions? Contact us.
- Before-Afters
Before-Afters- Transformation Photos
Our library of before-after photos.
- Client Testimonials
Read the experiences of members
Before-Afters/ Client Testimonials- Popular Treatments
-
Articles
Over the past few years, there has been a rapid rise in the use of GLP-1-based medications for obesity and metabolic health. It is estimated that 63.4 million GLP-1 prescriptions were dispensed in the United States between 2015 and 2020.{{Adhikari, R., Jha, K., Dardari, Z., Heyward, J., Blumenthal, R.S., Eckel, R.H., Alexander, G.C., Blaha, M.J., (2022). National Trends In Use Of Sodium-Glucose Cotransporter-2 Inhibitors And Glucagon-Like Peptide-1 Receptor Agonists By Cardiologists And Other Specialties, 2015 To 2020. Journal Of The American Heart Association. 11(9). e023811. Available at: https://doi.org/10.1161/JAHA.121.023811}} Ozempic, Wegovy, Mounjaro, and Zepbound represent just a few of these FDA-approved GLP-1 medications used to treat diabetes and chronic weight management.
With a rise in popularity, there is also a rise in users reporting side effects. Alongside well-known gastrointestinal effects, some users online report hair shedding or worsening hair loss with drugs like Zepbound, including new hair shedding, worsening of pattern hair loss (androgenic alopecia), and a “reversal” of prior hair regrowth!
But could this be true? In this article, we separate anecdotes from evidence. We’ll dive into the science behind Zepbound, the research discussing its association with hair loss, and discuss the ways you can monitor hair loss and reduce the risk of losing hair when you’re trying to lose weight.
[ulo_promo title=”Interested in Topical Minoxidil?” subtitle=”High-strength topical minoxidil available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-minoxidil?variant=42247221313615” prescription=”true” type=”topical” ]
What Is Zepbound?
Zepbound is one of the many GLP-1 medications FDA-approved for the treatment of chronic weight management. It is an injection, usually taken once weekly at a dosage of 2.5 mg to 5.0 mg.{{U.S. Food and Drug Administration. (2025). Tirzepatide Injection Label. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/217806Orig1s020lbl.pdf (Accessed: 04 March 2026)}}
Zepbound is a brand name. Chemically, it is the same as Mounjaro, with both containing the active ingredient tirzepatide, but Mounjaro is FDA-approved for the treatment of type 2 diabetes.
Tirzepatide mimics natural hormones found in the body – incretins (like GIP and GLP-1).{{Galindo, R.J., Cheng, A.Y.Y., Longuet, C. (2026). Insights Into The Mechanism Of Action Of Tirzepatide: A Narrative Review. Diabetes Therapy. 17. 19-40. Available at: https://doi.org/10.1007/s13300-025-01804-w}} By mimicking these incretins, tirzepatide has two key effects in the body:
- It’s a gastric inhibitory peptide (GIP) analog: It stimulates insulin secretion
- It’s a GLP-1 receptor agonist: It activates GLP-1 receptors, causing reduced blood sugar, appetite, and energy intake.
Figure 1: Zepbound
How Do GLP-1–Based Therapies Work For Weight Loss?
Let’s look deeper into how GLP-1 therapies like Zepbound really function to support weight loss.
As the title suggests, it’s the GLP-1 receptor agonist activity of these medications that makes these drugs suitable for weight management. GIP analog activity may enhance weight loss when combined with GLP-1 activity, but this action does not promote weight loss alone.
1st step: Activating the GLP-1 receptor
Tirzepatide mimics the incretin GLP-1 (found naturally in the body). By having the same shape and structure as GLP-1, tirzepatide can bind to GLP-1 receptors. Think of the GLP-1 receptors like a lock, and GLP-1 as the key. When they interact, GLP-1 (or tirzepatide, in this case) “unlocks” and activates GLP-1 receptors.
2nd step: Signalling
Activation of the GLP-1 receptors causes a series of effects in the body:
- It lowers blood glucose levels: GLP-1 receptor activation suppresses glucagon secretion (which normally stimulates the liver to release glucose into the bloodstream) and increases glucose-dependent insulin secretion, promoting the uptake of glucose from the bloodstream into tissues.{{Galindo, R.J., Cheng, A.Y.Y., Longuet, C. (2026). Insights Into The Mechanism Of Action Of Tirzepatide: A Narrative Review. Diabetes Therapy. 17. 19-40. Available at: https://doi.org/10.1007/s13300-025-01804-w}}
- It stimulates feelings of satiety: GLP-1 receptor activation contributes to gut-brain signaling that relaxes the stomach and slows emptying, both causing a feeling of “fullness”.{{Tack, J., Verbeure, W., Mori, H., Schol, J., Van den Houte, K., Huang, I.H., Balsiger, L., Broeders, B., Colomier, E., Scarpellini, E., Carbone, F. (2021). The Gastrointestinal Tract In Hunger And Satiety Signalling. United European Gastroenterology Journal. 9(6). 727-734. Available at: https://doi.org/10.1002/ueg2.12097}}
3rd step: Weight loss
Along with an appropriate diet and exercise, the increased satiety effects reduce food intake and promote higher energy expenditure than energy (calorie) intake. This leads to weight loss over time.
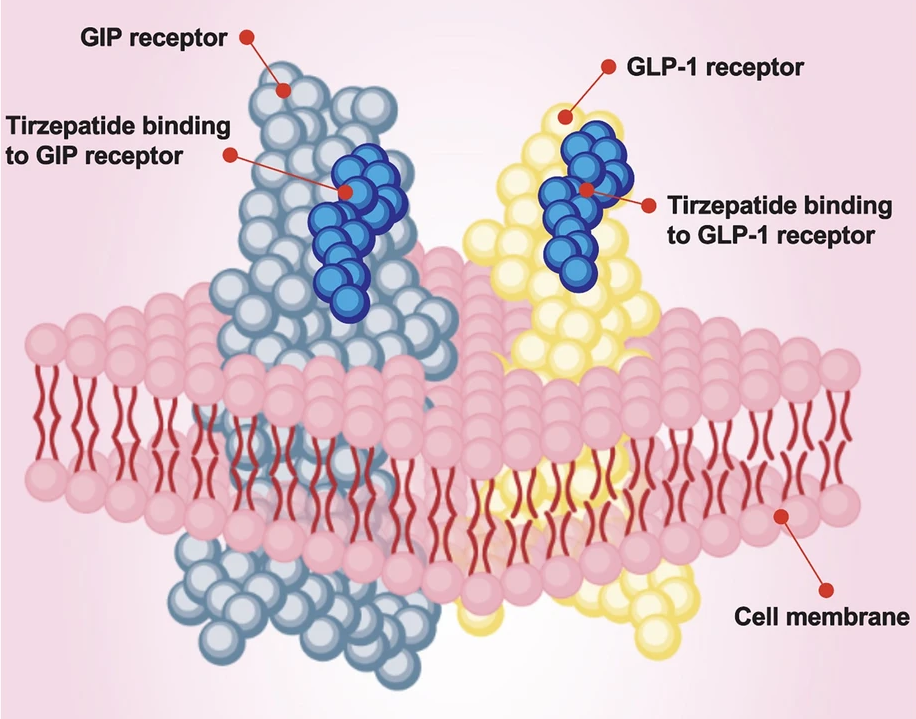
Figure 2: Diagram showing how Tirzepatide binds to GIP and GLP-1 receptors in the body. Adapted from Figure 2.{{Galindo, R.J., Cheng, A.Y.Y., Longuet, C. (2026). Insights Into The Mechanism Of Action Of Tirzepatide: A Narrative Review. Diabetes Therapy. 17. 19-40. Available at: https://doi.org/10.1007/s13300-025-01804-w}} Image used under the Creative Commons License.
Types of Hair Loss: Telogen Effluvium and Androgenic Alopecia
Before we get into the how and why behind Zepbound and weight loss, let’s establish two of the main types of hair loss: telogen effluvium and androgenic alopecia.
Telogen effluvium
In the normal hair cycle, there are four phases:- The growth phase (anagen phase)
- The transition phase (catagen phase)
- The resting phase (telogen phase)
- The shedding phase (exogen phase)
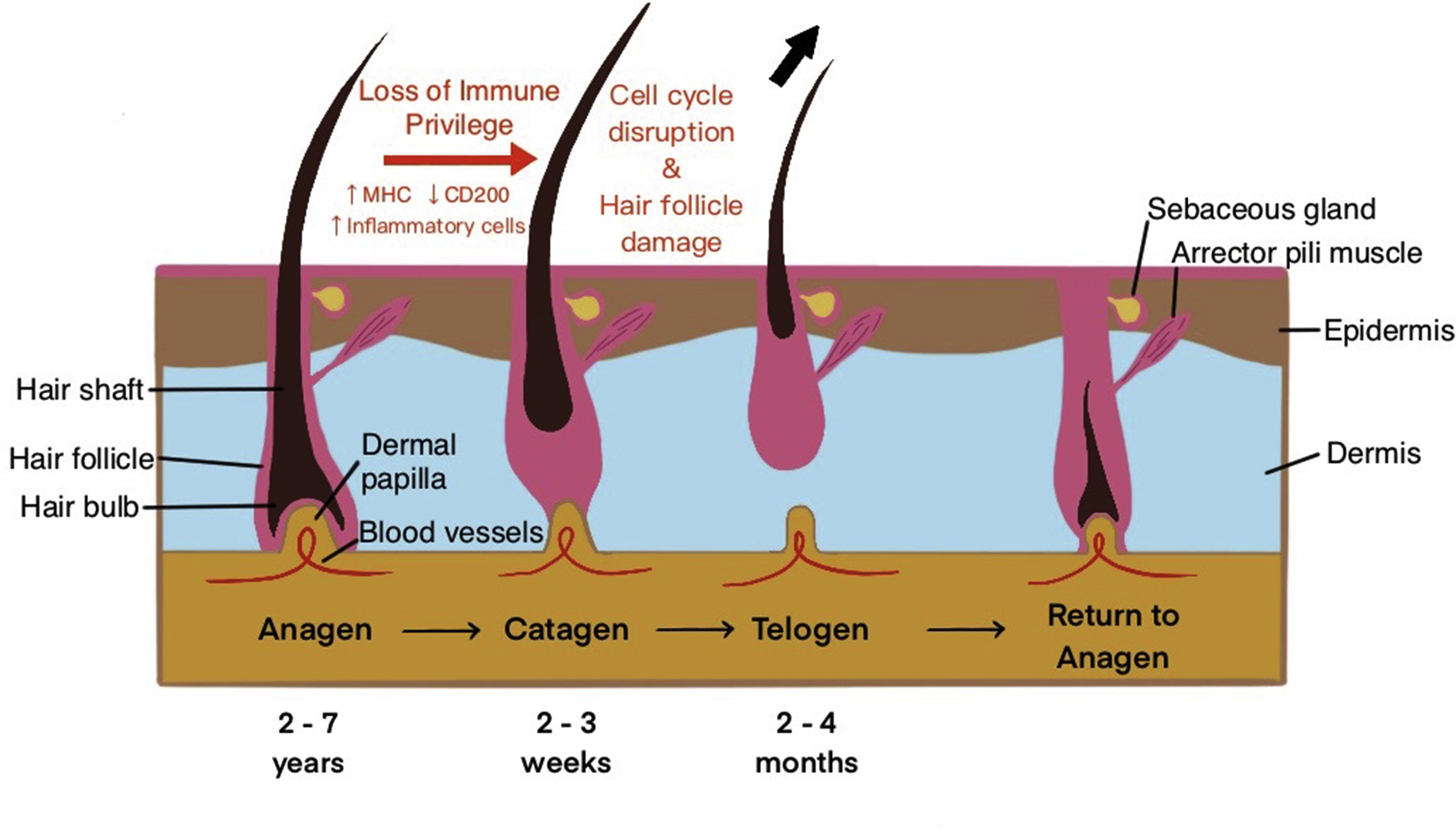
Figure 3: Hair growth phases. Adapted from Figure 2.{{Olayinka, J.T., Richmond, J.M., (2021). Immunopathogenesis Of Alopecia Areata. Current Research In Immunology. 2. 7-11. Available at: https://doi.org/10.1016/j.crimmu.2021.02.001}} Image used under the Creative Commons License.
Telogen effluvium is a condition where there are too many hairs in the telogen phase, causing diffuse premature hair shedding and a noticeable loss in hair density.
There are many reasons why this might happen. Usually, it is caused by a “negative event”, like illness, stress, diet, surgical trauma, childbirth, or even starting and stopping medications. The time between exposure to a trigger and actual hair loss can be rather long – often, people will experience telogen effluvium 2 to 8 months after they experience a trigger.{{Malkud, S., (2015). Telogen Effluvium: A Review. Journal Of Clinical And Diagnostic Research. 9(9). WE01-WE03. Available at: https://doi.org/10.7860/JCDR/2015/15219.6492}},{{Hussain, N., Agarwala, P., Iqbal, K., et al. (2022). A Systematic Review Of Acute Telogen Effluvium, A Harrowing Post-COVID-19 Manifestation. J Med Virol. 94. 1391-1401. Available at: https://doi.org/10.1002/jmv.27534}},{{Bin Dayel, S., Hussein, R.S., Atia, T., Abahussein, O., Al Yahya, R.S., Elsayed, S.H. (2024). Is Thyroid Dysfunction A Common Cause Of Telogen Effluvium?: A Retrospective Study. Medicine. 103(1). e36803. Available at: https://doi.org/10.1097/MD.0000000000036803}},{{Kang, D.H., Kwon, S.H., Sim, W.Y., Lew, B.L. (2024). Telogen Effluvium Associated With Weight Loss: A Single Center Retrospective Study. Ann Dermatol. 36(6). 384-388. Available at: https://doi.org/10.5021/ad.24.043}}
Fortunately, telogen effluvium is not permanent in most cases. Once the “negative event” causing it has been removed, hair usually regrows after 2 to 8 months.{{Malkud, S., (2015). Telogen Effluvium: A Review. Journal Of Clinical And Diagnostic Research. 9(9). WE01-WE03. Available at: https://doi.org/10.7860/JCDR/2015/15219.6492}}
Androgenic alopecia
This is a progressive hair loss condition, where more and more hair loss occurs with time. It is the most common type of progressive hair loss, and affects up to 50% of men and 30% of women.Androgenic alopecia is characterized by miniaturization of the hair follicle. This means that the hair follicle gets smaller over time. This causes long hairs that contribute to the cosmetic appearance of hair density (terminal hairs) to turn into “peach fuzz” hairs that do little to contribute to hair “fullness” (vellus hairs).
This happens because of an alteration to the normal hair growth cycle where the duration of the anagen phase decreases, while the telogen phase increases. The anagen phase determines hair length, so as it shortens, so does the length of hair. As the hair cycle repeats, this leads to more and more hair miniaturization and, eventually, a balding appearance.
You can often tell telogen effluvium apart from androgenic alopecia by examining the hairline. Androgenic alopecia typically starts with a widening part and receding hairline, while there is more diffuse hair thinning in telogen effluvium.
If you’d like to learn more about androgenic alopecia, read our article.
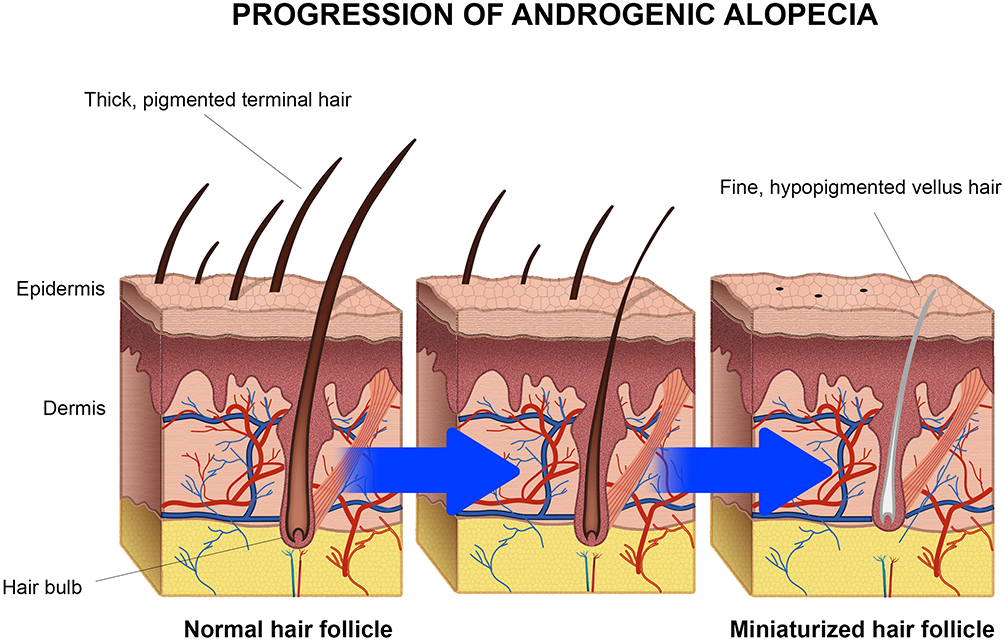
Figure 4: Miniaturization of the hair follicle during androgenic alopecia. Adapted from Figure 1.{{Cardoso, C.O., Tolentino, S., Gratieri, T., Cunha-Filho, M., Lopez, R.F.V., Gelfuso, G.M., (2021). Topical Treatment For Scarring And Non-Scarring Alopecia: An Overview Of The Current Evidence. Clinical, Cosmetic And Investigational Dermatology. 14. 485-499. Available at: https://doi.org/10.2147/CCID.S284435}} Image used under the Creative Commons License.
Research Deep Dive: Zepbound and Hair Loss
Prescribing information for Zepbound notes that common side effects include nausea, diarrhea, vomiting, and, interestingly, hair loss.{{U.S. Food and Drug Administration. (2025). Tirzepatide Injection Label. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/217806Orig1s020lbl.pdf (Accessed: 04 March 2026)}} There are only a few published clinical studies reporting the association between Zepbound and hair loss, so extensive evidence is limited. But let’s look deeper into the scientific evidence that we do have.
Randomized, Double-Blinded, Placebo-Controlled Trials
Unfortunately, there are no studies examining the direct link between human hair loss and GLP-1 medications. However, trials and reports are showing that hair loss is sometimes reported in those taking GLP-1 medications.
For example, there are two clinical trials reported in the FDA Zepbound documentation that have documented adverse reactions.{{U.S. Food and Drug Administration. (2025). Tirzepatide Injection Label. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/217806Orig1s020lbl.pdf (Accessed: 04 March 2026)}}
These trials included a total of 2,519 adults who were treated for up to 72 weeks with Zepbound (at 5 mg, 10 mg, or 15 mg), or a placebo. When pooling all the data of adverse reactions, we can see that:
- 1% of users on the placebo reported hair loss
- 5% of users on 5 mg Zepbound reported hair loss
- 4% of users on 10 mg Zepbound reported hair loss
- 5% of users on 15 mg Zepbound reported hair loss
- One participant receiving the placebo discontinued due to hair loss
- No Zepound patients discontinued the study due to hair loss
While hair loss is noted as an adverse reaction, the documentation doesn’t provide further detail. For example, did these participants already have pre-existing hair loss, or did they develop new hair loss? Reports could reflect hair loss that would have worsened naturally, with or without treatment with Zepbound.
Does this show Zepbound causes hair loss?
No. There seems to be a higher incidence of hair loss in those receiving Zepbound. But we can’t know whether Zepbound is a cause of hair loss, or if it accelerates hair loss in those already susceptible.
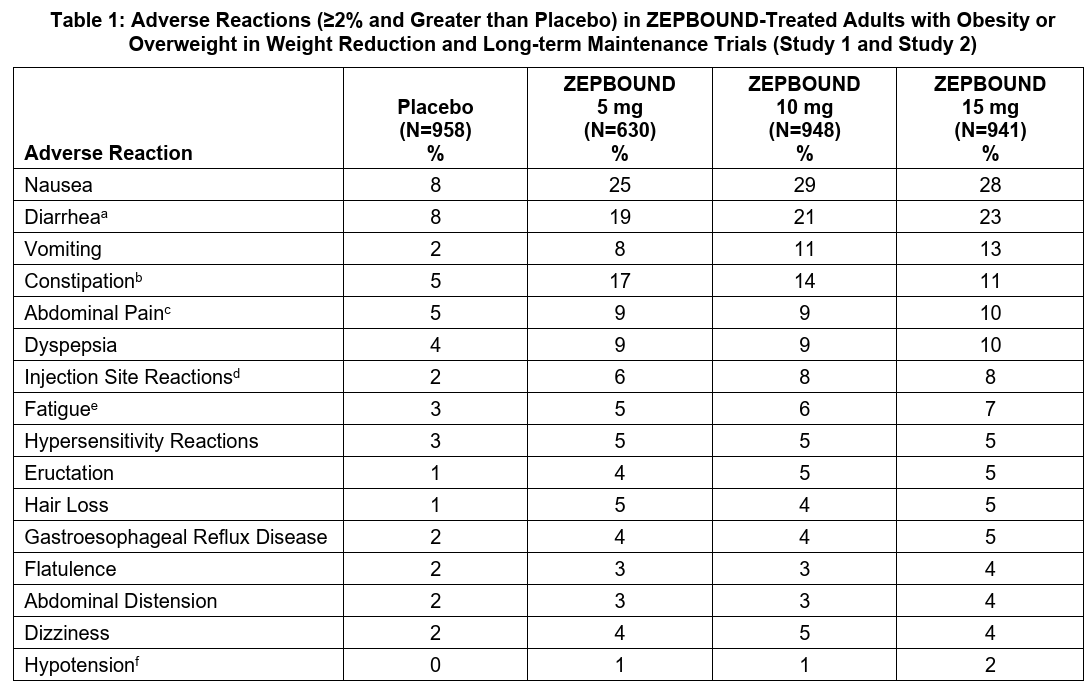
Figure 5: Adverse reactions in adults treated with Zepbound. Adapted from Table 1.{{U.S. Food and Drug Administration. (2025). Tirzepatide Injection Label. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/217806Orig1s020lbl.pdf (Accessed: 04 March 2026)}}
2024 FAERS Study
A 2024 study reported that alopecia is associated with the use of tirzepatide.{{Godfrey, H., Leibovit-Reiben, Z., Jedlowski, P., Thiede, R. (2025). Alopecia Associated With The Use Of Semaglutide And Tirzepatide: A Disproportionality Analysis Using The FDA Adverse Event Reporting System (FAERS) From 2022 To 2023. Journal Of The European Academy Of Dermatology And Venereology. 39. e153-e154. Available at: https://doi.org/10.1111/jdv.20197}}
The researchers searched the term “alopecia” in the FDA adverse reporting system (FAERS), which collects reports of side effects and adverse reactions from the use of FDA-approved drugs. They then isolated cases from 2022 to 2023 associated with GLP-1 agonist drugs.
They found that there were 179 reported cases of alopecia associated with tirzepatide, while semaglutide returned 199 cases. Other similar medications like liraglutide, dulaglutide, exenatide, and lixisenatide returned 0 to 65 cases.
A disproportionality analysis was then performed. This is a type of statistical test that assesses whether effects are reported more often in people using a drug than would occur in the general population. They concluded that the reporting odds for semaglutide and tirzepatide were higher.
But it’s important to remember that the FAERS is a public database where anyone can view and report adverse events – healthcare professionals as well as consumers, patients, and caregivers. That means reporting is vulnerable to:
- Media attention and amplification on social media
- Increased awareness leading to more reports
- Missing clinical details that determine hair loss type, severity, and other factors that could contribute to hair loss (i.e., androgenic alopecia vs. alopecia areata, hair counts before and after treatment, weight loss rate, diet…)
This could inflate reports of hair loss for a particular drug. When we look at the numbers, we see that 84% of alopecia reports were from consumers, and only 16% were from healthcare professionals. So, how do we truly know that these reports of hair loss are clinically legitimate? The answer is that we can’t know for sure.
Does this show Zepbound causes hair loss?
No. What this study does show is that there could be an association between hair loss and Zepbound. It does not show that Zepbound is proven to cause alopecia; it simply signals that this association is worth investigating further.
2025 Retrospective Studies
A retrospective study doesn’t generate new data; it looks back at old data (such as medical charts and databases) to identify patterns that weren’t previously seen. In 2025, two retrospective studies were conducted to find any association between hair loss and GLP-1 medications.{{Burke, O. (2025). Glucagon-Like Peptide-1 Receptor Agonist Medications And Hair Loss: A Retrospective Cohort Study. Journal Of The American Academy Of Dermatology. 92(5). 1141-1143. Available at: https://doi.org/10.1016/j.jaad.2025.01.046}},{{Akiska, Y.M., Vidal, S.I., Menta, N. (2025). Increased Incidence And Risk Of Hair Loss With Glucagon-Like Peptide 1 Receptor Agonists: A Real-World Multicentre Cohort Study. EMJ. 13(1). 52-54. Available at: https://doi.org/10.33590/emjdermatol/TYEW1122}}
In the first study, the researchers focused on two hair loss conditions: androgenic alopecia and telogen effluvium. They collected data from 2021 to 2023, including 283 patients aged over 18 years, who were on GLP-1 medications and also seen in the dermatology department at the University of Miami Hospital.{{Burke, O. (2025). Glucagon-Like Peptide-1 Receptor Agonist Medications And Hair Loss: A Retrospective Cohort Study. Journal Of The American Academy Of Dermatology. 92(5). 1141-1143. Available at: https://doi.org/10.1016/j.jaad.2025.01.046}}
Of all the GLP-1 agonist users:
- 84.1% reported no hair loss
- 1.2% reported new hair loss
In GLP-1 agonist users with pre-existing hair loss (13% of users):
- 11.9% reported worsening of hair loss
- 0.4% reported resolved hair loss
- 0.8% reported stabilization of hair loss
Interestingly, tirzepatide was most associated with patients with telogen effluvium. Semaglutide was found to be most associated with androgenic alopecia. The fact that these two GLP-1 medications were flagged adds credibility to the 2024 FAERS study, where both of these drugs showed strong associations with reports of alopecia.
However, it should be noted that the association between tirzepatide and telogen effluvium was not found to be statistically significant. This means it could be down to chance! What’s more, the report of 1.2% of users experiencing new hair loss is approximately the same rate as would be expected in the general population over two years. So, this is not a strong indication that GLP-1 treatment caused hair loss.
In the second study, the researchers pooled electronic health records of over 100 million patients and searched for those on GLP-1 medications without a prior history of alopecia. Among the resulting 500,000 patients, it was found that after 12 months of GLP-1 use, there was a significantly elevated risk of users developing androgenic alopecia, telogen effluvium, and non-scarring hair loss.{{Akiska, Y.M., Vidal, S.I., Menta, N. (2025). Increased Incidence And Risk Of Hair Loss With Glucagon-Like Peptide 1 Receptor Agonists: A Real-World Multicentre Cohort Study. EMJ. 13(1). 52-54. Available at: https://doi.org/10.33590/emjdermatol/TYEW1122}}
While retrospective data can be useful, we must consider that the design of these studies lacks some key components that allow us to make strong conclusions:
- It’s not randomized
- No untreated control group
- Hair outcomes were self-reported rather than objectively measured through hair counts
- The duration of medication use was not clearly tracked or standardized
Without these parameters in place, it’s difficult to say whether the patients are reporting a worsening of hair loss due to GLP-1 medications or simply due to pre-existing hair loss conditions and susceptibilities that are naturally progressing with age while they are taking the medication.
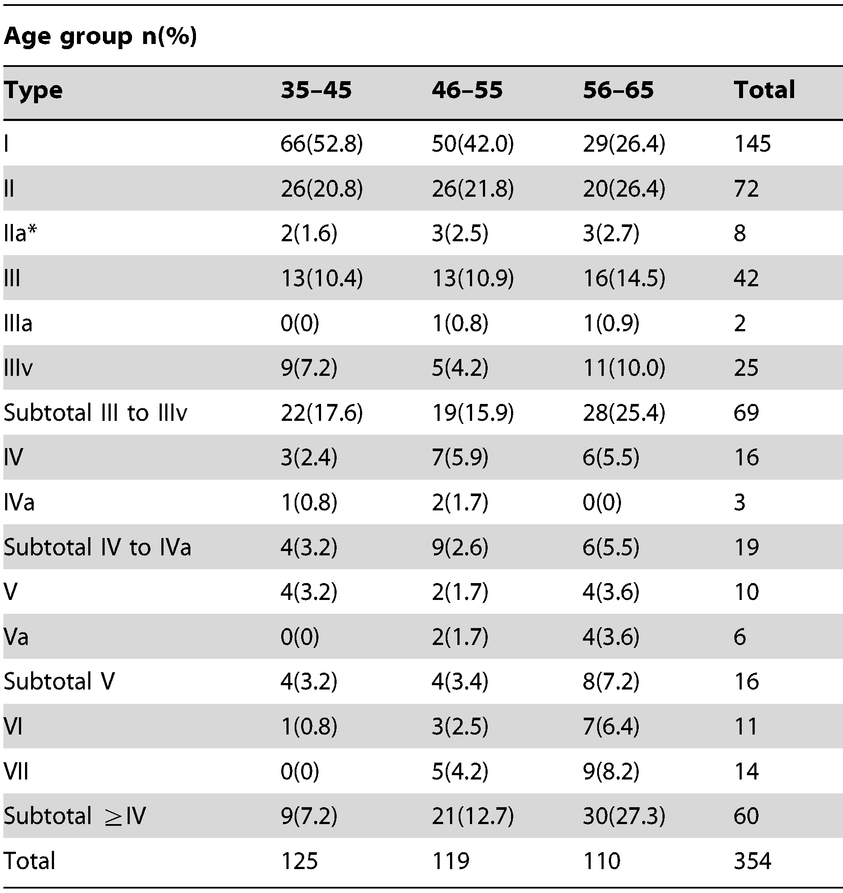
Figure 6: Increasing androgenic alopecia severity (Type I to VII) with age. Adapted from Table 1.{{Lai, C.H., Chu, N.F., Chang, C.W., Wang, S.L., Yang, H.C., Chu, C.M., Chang, C.T., Lin, M.H., Chien, W.C., Su, S.L., Chou, Y.C., Chen, K.H., Wang, W.M., Liou, S.H. (2013). Androgenic Alopecia Is Associated With Less Dietary Soy, Higher Blood Vanadium And rs1160312 1 Polymorphism In Taiwanese Communities. PLOS ONE. 8(12). Available at: https://doi.org/10.1371/journal.pone.0079789}} Image used under the Creative Commons License.
Does this show Zepbound causes hair loss?
No. The studies raise a hypothesis and support further investigation, but do not demonstrate a cause-and-effect relationship between Zepbound and hair loss.
How Might Zepbound Contribute to Hair Loss?
From the studies, it seems there is no evidence to suggest that Zepbound causes hair loss, but there is evidence to support that there may be an association between Zepbound and hair loss in a small number of users. Because Zepbound often produces meaningful weight loss, it raises a key question: Is any hair loss due to the drug itself or due to the weight loss?
No single mechanism has been confirmed, but several possible explanations exist.{{Desai, D.D., Sikora, M., Nohria, A., Bordone, L., Caplan, A.S., Shapiro, J., Lo Sicco, K.I. (2024). GLP-1 Agonists And Hair Loss: A Call For Further Investigation. International Journal Of Dermatology. 63. 1128-1130. Available at: https://doi.org/10.1111/ijd.17246}}
Direct Action Against The Hair Cycle
In one animal study that predates the first FDA-approved GLP-1 drug, Byetta, it was found that GLP-1 levels were heightened at the hair follicles within the skin of newborn mice.{{List, J.F., He, H., Habener, J.F. (2006). Glucagon-Like Peptide-1 Receptor And Proglucagon Expression In Mouse Skin. Regulatory Peptides. 134(2–3). 149-157. Available at: https://doi.org/10.1016/j.regpep.2006.02.007}} The study also found that, in skin cells, GLP-1 was found to activate the MAPK/ERK pathway, which is associated with cell proliferation.
The researchers conclude that GLP-1 could have a role in hair follicle development. Could this provide a potential link between GLP-1 medications and hair? If anything, the study shows that GLP-1 would contribute to hair growth, not decline.
The study does not include any testing on humans – what happens in an animal does not always translate to what happens in humans. So what we can take from this study is that there could be some involvement of GLP-1 in the hair cycle of mice, but we can’t conclude whether GLP-1 could have the same involvement in humans nor whether this mechanism is a plausible cause of the Zepbound and hair loss association.
Rapid Weight Loss, Caloric Deficit, and Nutritional Deficiencies
We know that telogen effluvium can be triggered by a variety of stressors, and one of the well-established triggers for telogen effluvium is rapid weight loss.{{Smolarczyk, K., Meczekalski, B., Rudnicka, E., Suchta, K., Szeliga, A. (2024). Association Of Obesity And Bariatric Surgery On Hair Health. Medicina. 60(2). 325. Available at: https://doi.org/10.3390/medicina60020325}}
For example, within the first three months after bariatric surgery (weight loss surgery), a case study of a 24-year-old woman noted the development of telogen effluvium.{{Cohen-Kurzrock, R.A., Cohen, P.R., (2021). Bariatric Surgery-Induced Telogen Effluvium (Bar SITE): Case Report And A Review Of Hair Loss Following Weight Loss Surgery. Cureus. 13(4). e14617. Available at: https://doi.org/10.7759/cureus.14617}}

Figure 7: Diffuse hair loss following bariatric surgery. Adapted from Figure 2.{{Cohen-Kurzrock, R.A., Cohen, P.R., (2021). Bariatric Surgery-Induced Telogen Effluvium (Bar SITE): Case Report And A Review Of Hair Loss Following Weight Loss Surgery. Cureus. 13(4). e14617. Available at: https://doi.org/10.7759/cureus.14617}} Image used under the Creative Commons License.
This is not an isolated incident – hair loss has been noted in several cases following bariatric surgery.{{Rojas, P., Gosch, M., Basfi-Fer, K., (2011). Alopecia In Women With Severe And Morbid Obesity Who Undergo Bariatric Surgery. Nutricion Hospitalaria. 26(4). 856-862. Available at: https://doi.org/10.1590/s0212-16112011000400028}},{{Nadler, E.P., Youn, H.A., Ginsburg, H.B., Ren, C.J., Fielding, G.A., (2007). Short-Term Results In 53 US Obese Pediatric Patients Treated With Laparoscopic Adjustable Gastric Banding. Journal Of Pediatric Surgery. 42(1). 137-142. Available at: https://doi.org/10.1016/j.jpedsurg.2006.09.014}},{{Nadler, E.P., Youn, H.A., Ren, C.J., Fielding, G.A., (2008). An Update On 73 US Obese Pediatric Patients Treated With Laparoscopic Adjustable Gastric Banding: Comorbidity Resolution And Compliance Data. Journal Of Pediatric Surgery. 43(1). 141-146. Available at: https://doi.org/10.1016/j.jpedsurg.2007.09.035}}
The case study speculates that this hair loss may be the result of nutritional deficiencies, which can occur after bariatric surgery.{{Ruiz-Tovar, J., Oller, I., Llavero, C., Zubiaga, L., Diez, M., Arroyo, A., Calero, A., Calpena, R., (2014). Hair Loss In Females After Sleeve Gastrectomy: Predictive Value Of Serum Zinc And Iron Levels. The American Surgeon. 80(5). 466-471}},{{Almohanna, H.M., Ahmed, A.A., Tsatalis, J.P., Tosti, A., (2019). The Role Of Vitamins And Minerals In Hair Loss: A Review. Dermatology And Therapy. 9(1). 51-70. Available at: https://doi.org/10.1007/s13555-018-0278-6}} However, in this case, evaluation of her nutritional profile showed no deficiencies, and the hair loss was resolved within 14 months of surgery.
But it’s not just weight loss from bariatric surgery that can cause telogen effluvium. Those who have lost weight due to diet (calorie reduction) have also been shown to experience telogen effluvium.{{Kang, D.H., Kwon, S.H., Sim, W.Y., Lew, B.L., (2024). Telogen Effluvium Associated With Weight Loss: A Single Center Retrospective Study. Annals Of Dermatology. 36(6). 384-388. Available at: https://doi.org/10.5021/ad.24.043}}
Why might this be? There isn’t one specified cause of telogen effluvium from weight loss and diet change, but a few potential contributors include:
- Sustained calorie restriction
- Reduced protein intake
- Iron, zinc, or other micronutrient insufficiencies
- Physiologic stress from rapid fat loss or surgery
Calories, proteins, and nutrients are needed to sustain hair follicle growth, and stress is a known driver of hair loss. So, it’s possible these factors associated with weight loss and diet changes could act to trigger telogen effluvium.
When taking a medication like Zepbound, appetite suppression for prolonged periods could inadvertently create very low caloric intake and result in nutrient deficiencies. In line with this, studies have shown that GLP-1 users often do not eat adequate amounts of protein and have insufficient intake of multiple key nutrients.{{Johnson, B., Milstead, M., Thomas, O. (2025). Investigating Nutrient Intake During Use Of Glucagon-Like Peptide-1 Receptor Agonist: A Cross-Sectional Study. Frontiers In Nutrition. 12. 1566498. Available at: https://doi.org/10.3389/fnut.2025.1566498}} This may shift hairs prematurely into the telogen phase, increasing shedding and triggering telogen effluvium.
Telogen effluvium typically begins 2 to 4 months after the trigger and is often reversible, though regrowth can sometimes appear finer initially. The bad news is that telogen effluvium could also accelerate the onset or appearance of androgenic alopecia for susceptible individuals.
If shedding is increased, this means that hair follicle miniaturization is also accelerated, since hair follicle miniaturization occurs with repeated hair cycles. In this way, weight loss and reduced calorie intake promoted by Zepbound may appear to worsen androgenic alopecia. This hasn’t been demonstrated in research, but it is a plausible scenario.
Changes to Hormonal Pathways
Zepbound may affect the hormonal pathways that regulate hair growth. Insulin is known to increase the production of hormones like IGF-1.{{Brismar, K., Fernqvist-Forbes, E., Wahren, J., Hall, K., (1994). Effect Of Insulin On The Hepatic Production Of Insulin-Like Growth Factor-Binding Protein-1 (IGFBP-1), IGFBP-3, And IGF-I In Insulin-Dependent Diabetes. Journal Of Clinical Endocrinology And Metabolism. 79(3). 872-878. Available at: https://doi.org/10.1210/jcem.79.3.7521354}} IGF-1 stimulates hair follicle proliferation, promotes movement into the anagen phase, and reduces cell death of hair follicles.{{Hsieh, W.J., Qiu, W.Y., Percec, I., Chang, T.M., (2025). Insulin-Like Growth Factor 1 (IGF-1) In Hair Regeneration: Mechanistic Pathways And Therapeutic Potential. Current Issues In Molecular Biology. 47(9). 773. Available at: https://doi.org/10.3390/cimb47090773}}
In support of this, a 2021 case report documented hair shedding in a 54-year-old woman with diabetes and hair loss, demonstrating that insulin therapy, but not minoxidil, led to hair growth and reduced hair shedding.{{Kant, R., Barnwal, S., Sharma, S.K., Thakur, K. (2021). Reversal Of Alopecia By Insulin Therapy In Uncontrolled Type 2 DM: A Case Report. Journal Of Diabetology. 12(4). 533-537. Available at: https://doi.org/10.4103/jod.jod_66_21}}
However, this is just a case report. Much like the retrospective study discussed earlier, a report like this lacks:
- Multiple participants
- Randomization
- An untreated control group
- Objective measures of hair counts from before and after treatment
This doesn’t discredit the findings, but it doesn’t allow the results to be applied to a general population, and it’s difficult to conclude causality. What we can take from this is that, in this case, there may be an association between insulin and hair growth.
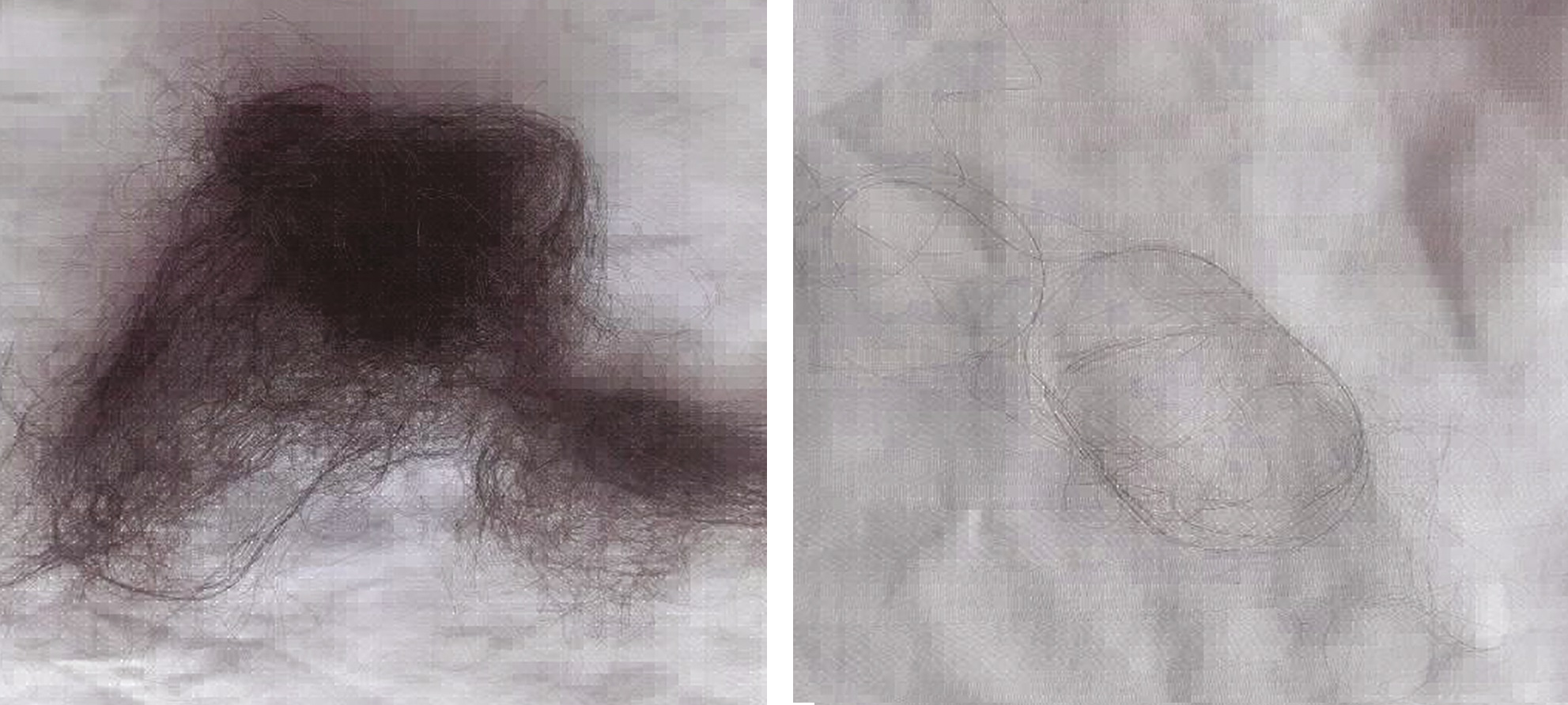
Figure 8: Hair shedding before and after insulin therapy in a woman with diabetes and hair loss. Adapted from Figure 2 and Figure 4.{{Kant, R., Barnwal, S., Sharma, S.K., Thakur, K. (2021). Reversal Of Alopecia By Insulin Therapy In Uncontrolled Type 2 DM: A Case Report. Journal Of Diabetology. 12(4). 533-537. Available at: https://doi.org/10.4103/jod.jod_66_21}} Image used under the Creative Commons License.
Why is this important?
Because we know that GLP-1 therapies increase glucose-dependent insulin secretion, promoting the uptake of glucose from the bloodstream into tissues. This means that when glucose is high (like after a meal), the insulin response is enhanced to rid the extra glucose. But with long-term use, the curbing of appetite, weight loss, and reduced food intake could reduce the amount of insulin produced by the body more than before treatment.{{{Jørgensen, S.W., Hjort, L., Gillberg, L., Justesen, L., Madsbad, S., Brøns, C., Vaag, A.A. (2021). Impact Of Prolonged Fasting On Insulin Secretion, Insulin Action, And Hepatic Versus Whole Body Insulin Secretion Disposition Indices In Healthy Young Males. American Journal Of Physiology Endocrinology And Metabolism. 320(2). E281-E290. Available at: https://doi.org/10.1152/ajpendo.00433.2020}},{{Alhowiti, A., Mirghani, H. (2025). The Effects Of GLP-1 Agonists On HbA1c And Insulin Dose Among Patients With Type 1 Diabetes. Frontiers In Endocrinology. 16. 1550938. Available at: https://doi.org/10.3389/fendo.2025.1550938}},{{Luo, Y., Yang, S., Zeng, H., Liu, S., Zhang, Y., Li, J.E., Liu, J. (2025). Both Subcutaneous Semaglutide And Calorie Restriction Improves Pancreatic Cell Hyperplasia And Gut Microbiota In High-Fat Diet-Induced Obese Mice. Nutrition And Metabolism. 22(1). 95. Available at: https://doi.org/10.1186/s12986-025-00987-0}} So, it’s possible GLP-1 medications like Zepbound may, in turn, inadvertently lower the activation of the pathways that insulin affects (like the IGF-1 pathway for hair follicle growth).
Insulin changes could also contribute to the onset of telogen effluvium. For those with a genetic susceptibility, this may trigger an earlier onset of androgenic alopecia, or just faster visibility of hair loss. However, it’s important to remember that this is just a theory for now – there’s no evidence to show that this does, in fact, happen.
Should You Be Concerned About Hair Loss If You’re Taking Zepbound?
If you’re taking Zepbound, you may be concerned about hair loss as a side effect. But the evidence suggests that, unless you already have pre-existing hair loss, you probably don’t have to worry.
If you have no signs of hair loss
- Current evidence suggests the risk of new-onset hair loss is likely low
- Most users in clinical observational data report no hair loss
If you have androgenic alopecia
- You may be more likely to notice worsening during rapid weight loss
- A shed can reduce density and make pattern thinning more obvious
- Some people may benefit from starting androgenic alopecia treatment alongside weight loss therapy, especially if hair preservation is a priority
Considering treatments for androgenic alopecia? Take a look at our articles on the FDA-approved treatments for this condition, topical minoxidil and oral finasteride.
If you have early or unnoticed androgenic alopecia
- Shedding related to weight loss can make thinning suddenly noticeable
- This may feel like the medication “caused” hair loss, when it may have revealed an underlying pattern
If you have a family history of baldness or are worried you might have androgenic alopecia, you may want to consult your doctor before taking a medication like Zepbound for a scalp assessment and to understand your potential for hair loss. Age, smoking, and obesity are also risk factors for androgenic alopecia.{{Liu, L.P., Wariboko, M.A., Hu, X., Wang, Z.H., Wu, Q., Li, Y.M., (2024). Factors Associated With Early-Onset Androgenetic Alopecia: A Scoping Review. PLOS ONE. 19(3). e0299212. Available at: https://doi.org/10.1371/journal.pone.0299212}}
[ulo_promo title=”Interested in Oral Finasteride?” subtitle=”Oral finasteride & minoxidil available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/oral-finasteride?variant=42292837711951” prescription=”true” type=”oral” ]
Practical Considerations While Taking Zepbound
If you have or suspect you may have androgenic alopecia, it doesn’t mean you have to avoid or stop using Zepbound.
There are two clear strategies to reduce hair loss when using GLP-1 medications:
- Aim for slower, steadier weight loss when possible: Slowly increase dosage over time so that weight loss occurs gradually, as opposed to rapidly
- If you have androgenic alopecia, start a hair loss treatment: Hair loss can be minimized with FDA-approved treatments for androgenic alopecia, like topical minoxidil or oral finasteride, along with a plethora of other treatments that are effective for stabilizing hair loss and promoting hair regrowth
You can also make sure to prioritize adequate protein intake, ensure you are getting sufficient iron and key micronutrients, and avoid extreme calorie deficits for long periods.
If shedding occurs, don’t panic.- Evaluate timing to assess whether it is telogen effluvium (often 2 to 4 months after rapid weight loss)
- Consider whether the pattern looks like telogen effluvium (diffuse thinning) or androgenic alopecia (typically starts with a widening part and receding hairline)
- Discuss your concerns with your doctor and determine the next steps
By doing this, you should be able to balance healthy weight loss with healthy hair outcomes.
Final Thoughts
Online anecdotes about Zepbound have amplified concern that this drug may cause hair loss, but the current clinical evidence does not establish this GLP-1 medication as a cause of hair loss. The answer likely isn’t the drug itself, but what the drug facilitates: weight loss. Weight loss is a known trigger of telogen effluvium, a temporary hair loss condition.
For those with diagnosed, early, or undiagnosed androgenic alopecia, telogen effluvium may accelerate the onset or progression of hair miniaturization. So, for most people without underlying hair loss, significant or permanent thinning from Zepbound appears unlikely. But for those with androgenic alopecia, it’s possible the rapid weight loss associated with this drug could promote worsening of your current condition.
The good news is you don’t have to avoid or stop taking Zepbound if you have androgenic alopecia. Monitor hair loss, ramp up dosage slowly to avoid rapid weight loss, and incorporate some hair loss interventions into your routine to help reduce the chance that weight loss from Zepbound could make hair loss more noticeable.
We have seen a rapid rise in GLP-1 medications for weight loss and diabetes. These medications are highly effective as well as convenient, with treatments requiring just a once-daily or once-weekly injection.
There are many different GLP-1 medications on the market: liraglutide, semaglutide, dulaglutide, exenatide, liraglutide, tirzepatide. From 2018 to 2023, it was estimated that semaglutide medications (like Ozempic and Wegovy) accounted for 60% of prescribed GLP-1 drugs.{{Ukhanova, M., Wozny, J.S., Truong, C.N., Ghosh, L., Krause, T.M. (2025). Trends In Glucagon-Like Peptide 1 Receptor Agonist Prescribing Patterns. Am J Manag Care. 31(8). e228-e234. Available at: https://doi.org/10.37765/ajmc.2025.89778}} While these treatments are effective, they are not without side effects. Common side effects include nausea, vomiting, and diarrhea, and more and more, there have been reports of hair loss.
Online discourse, as well as some published studies, report that semaglutide treatments like Ozempic and Wegovy are causing increased hair shedding, worsening of androgenic alopecia, and loss of prior hair regrowth.
But are these reports legitimate? Could semaglutide treatments really cause or influence hair loss? We dig deeper into the truth behind the anecdotes. In this article, we dissect the current evidence surrounding the relationship between Wegovy and hair loss. We discuss the plausibility of this association, how it might happen, and what you can do to minimize the risk of hair loss.
[ulo_promo title=”Interested in Topical Minoxidil?” subtitle=”High-strength topical minoxidil available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-minoxidil?variant=42247221313615” prescription=”true” type=”topical” ]
What Is Wegovy?
Wegovy is a brand name for the drug known as semaglutide. Wegovy is FDA-approved as a once-weekly injection for chronic weight management, and has also recently been approved as a daily oral pill for chronic weight management as well as to prevent adverse cardiovascular events. Ozempic is the same drug, but it is FDA-approved for the treatment of diabetes.
Wegovy works by acting as a GLP-1 receptor agonist. GLP-1 is a naturally occurring hormone found in the body, known as an incretin. “Agonist” is defined as: a substance that initiates a physiological response when combined with a receptor. So, as the name suggests, semaglutide activates GLP-1 receptors by mimicking GLP-1.

Figure 1: Wegovy
How Does Wegovy Work?
We’ve established that semaglutide mimics GLP-1, and this imitation allows semaglutide to activate GLP-1 receptors. How exactly does this lead to weight loss?
The binding of GLP-1 (or semaglutide) to GLP-1 receptors activates several biological responses:
- Increased insulin secretion after food intake, which improves blood glucose levels
- Reduced glucagon secretion, which limits glucose in the blood and helps reduce spikes in blood sugar
- Slowed emptying of the stomach, which helps people feel less hungry during the day
- Suppressed appetite, which again helps with feelings of satiety
All of these factors promote sustained food (and therefore calorie) reduction, supporting weight loss with time.{{Kommu, S., Whitfield, P., (2025), Semaglutide. Available at: http://www.ncbi.nlm.nih.gov/books/NBK603723/ (Accessed: 27 February 2026)}}
Semaglutide is highly effective for weight loss, with 2.4 mg once weekly injections, alongside appropriate diet and exercise, reducing mean body weight by 16% after use for 68 weeks.{{Wadden, T.A., Bailey, T.S., Billings, L.K., Davies, M., Frias, J.P., Koroleva, A., Lingvay, I., O’Neil, P.M., Rubino, D.M., Skovgaard, D., Wallenstein, S.O.R., Garvey, W.T. (2021). Effect Of Subcutaneous Semaglutide Vs Placebo As An Adjunct To Intensive Behavioral Therapy On Body Weight In Adults With Overweight Or Obesity: The STEP 3 Randomized Clinical Trial. JAMA. 325(14). 1403-1413. Available at: https://doi.org/10.1001/jama.2021.1831}} It’s clear that a semaglutide like Wegovy can support rapid weight loss, but anecdotal reports suggest that Wegovy may also contribute to hair loss. The key question is this: Does semaglutide itself cause hair loss, or are hair changes related to rapid weight loss?
Different Types of Hair Loss
Before we discuss the association between Wegovy and hair loss, we will first establish what hair loss is and the conditions that can cause it.
In the normal hair growth cycle, there are four key stages:
- The growth phase (anagen phase)
- The involuting phase (catagen phase)
- The resting phase (telogen phase)
- The shedding phase (exogen phase)
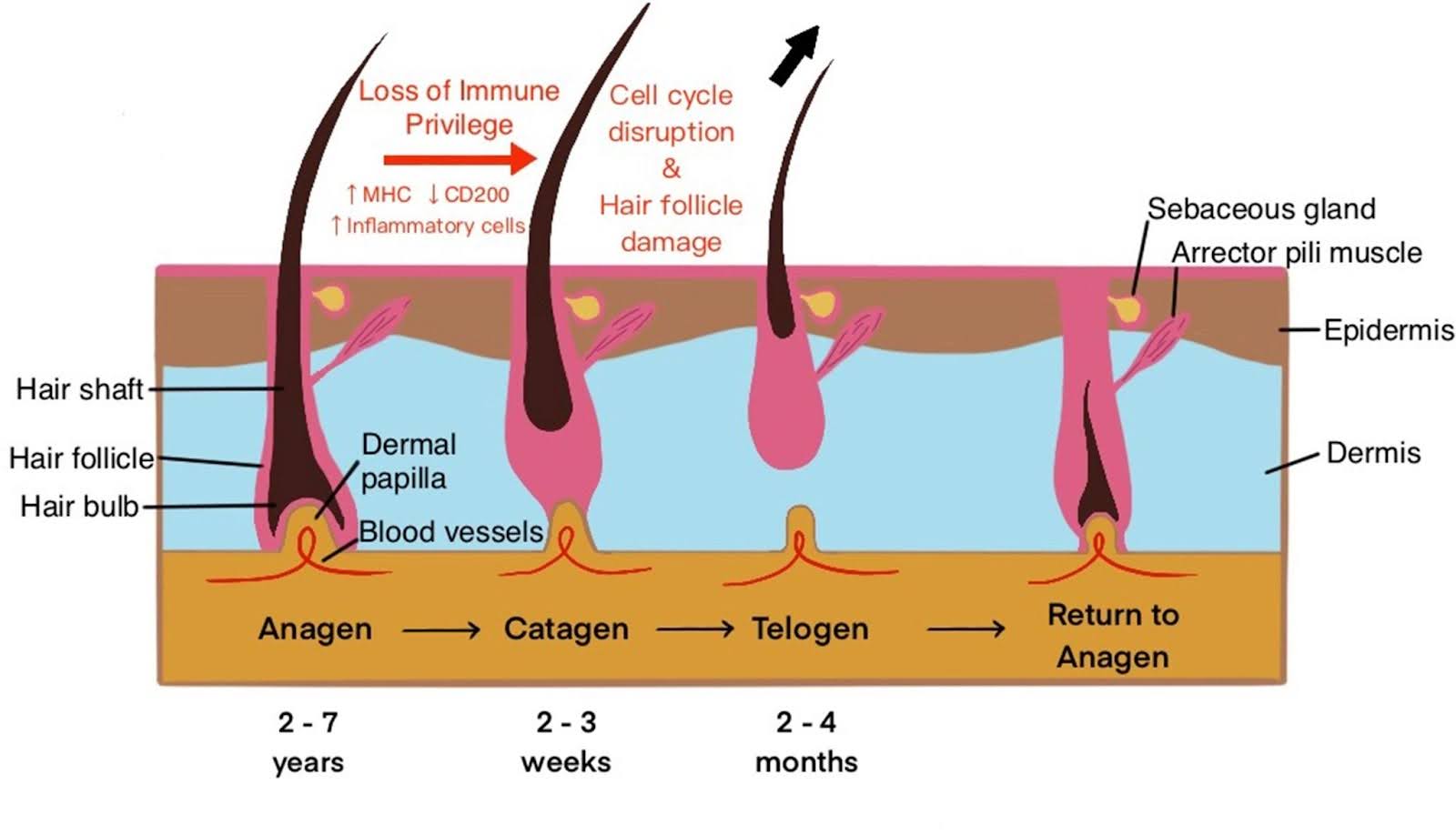
Figure 2: Hair growth phases. Adapted from Figure 2.{{Olayinka, J.T., Richmond, J.M., (2021). Immunopathogenesis Of Alopecia Areata. Current Research In Immunology. 2. 7-11. Available at: https://doi.org/10.1016/j.crimmu.2021.02.001}} Image used under the Creative Commons License.
Hair loss can happen when the cycling through these stages is disturbed or changed. There are three main conditions causing hair loss: androgenic alopecia, telogen effluvium, and alopecia areata.
Androgenic Alopecia
What is it? Also known as pattern hair loss, this is a progressive hair loss condition. It is one of the most common, affecting up to 50% of men and 30% of women. It causes terminal hairs that contribute to the appearance of hair “fullness” to become vellus hairs (i.e., “peach fuzz” hairs), ultimately leading to hair thinning, a process known as hair follicle miniaturization.{{Oiwoh, S.O., Enitan, A.O., Adegbosin, O.T., Akinboro, A.O., Onayemi, E.O. (2024). Androgenetic Alopecia: A Review. Niger Postgrad Med J. 31(2). 85-92. Available at: https://doi.org/10.4103/npmj.npmj_47_24}}
What does it look like? Hair thinning usually first appears as a receding hairline with a balding crown in men, or a widening part in women. Hair thinning occurs slowly over time, without scarring.
What causes it? There are several reasons hair follicle miniaturization can happen: genetics, age, and hormonal changes. The primary driver of androgenic alopecia is a change in dihydrotestosterone (DHT) levels at the scalp, which can cause the hair miniaturization process.

Figure 3: An example of androgenic alopecia in a female patient. Adapted from Figure 1.{{Ramos, P.M., Melo, D.F., Radwanski, H., Almeida, R.F.C., Miot, H.A. (2023). Female-Pattern Hair Loss: Therapeutic Update. Anais Brasileiros De Dermatologia. 98(4). 506-519. Available at: https://doi.org/10.1016/j.abd.2022.09.006}} Image used under the Creative Commons License.
Telogen Effluvium
What is it? This is a temporary hair loss condition in which too many hairs enter the telogen phase of the hair cycle, causing premature and excessive shedding. It often resolves within 2 to 8 months after onset.{{Malkud, S., (2015). Telogen Effluvium: A Review. Journal Of Clinical And Diagnostic Research. 9(9). WE01-WE03. Available at: https://doi.org/10.7860/JCDR/2015/15219.6492}}
What does it look like? Sudden diffuse thinning across the entire scalp.
What causes it? A “negative event” often triggers telogen effluvium. There isn’t one single cause, and the cause can be different for everyone, whether it be illness, stress, diet, surgical trauma, childbirth, or starting and stopping medications. The time between exposure to a trigger and the onset of telogen effluvium can vary, roughly between 2 and 8 months, similar to the recovery time.

Figure 4: An example of diffuse thinning from telogen effluvium. Adapted from Figure 1.{{Iancu, G.M., Molnar, E., Ungureanu, L., Șenilă, S.C., Hașegan, A., Rotaru, M. (2023). SARS-CoV-2 Infection—A Trigger Factor For Telogen Effluvium: Review Of The Literature With A Case-Based Guidance For Clinical Evaluation. Life. 13. 1576. Available at: https://doi.org/10.3390/life13071576}} Image used under the Creative Commons License
Alopecia Areata
What is it? This is an autoimmune condition in which the body begins to attack its own cells, specifically those of hair follicles. Research shows that there is an abnormally high number of hairs in the catagen phase with this condition, and hair follicles undergo miniaturization with time.{{Sibbald, C. (2023). Alopecia Areata: An Updated Review For 2023. J Cutan Med Surg. 27(3). 241-259. Available at: https://doi.org/10.1177/12034754231168839}}
What does it look like? Bald patches of hair that develop in a non-uniform fashion. Hair loss can sometimes extend beyond the scalp, and inflammation is often observed.
What causes it? Inflammation that is caused by genetics, environmental triggers (i.e., stress, infections, hormone fluctuations, nutrition), and/or loss of hair follicle immunity.

Figure 5: An example of alopecia areata. “Alopecia areata” by Thirunavukkarasye-Raveendran from Wikimedia Commons. Image used under the Creative Commons License.
The Science: Does Wegovy Cause Hair Loss?
Wegovy has shown great success in helping people manage their weight. However, every medication comes with risks and potential side effects. With semaglutide medications like Wegovy, there have been several studies and reports documenting how these treatments are sometimes associated with hair loss.
Online discussions also provide anecdotal evidence that this drug may be causing hair loss. But is it true? We will look deeper into the scientific evidence that may indicate a link between Wegovy and hair loss.
Randomized, Double-Blinded, Placebo-Controlled Trials
Clinical trials that are randomized, double-blinded, and placebo-controlled are the gold standard for testing the effectiveness of new treatments. We can see from the prescribing documentation for Wegovy that there were at least three randomized, double-blind, placebo-controlled trials with adults for this medication. Together, these trials included 3,377 adults with obesity or who were overweight. They were treated with either 2.4 mg Wegovy once weekly, or a placebo once weekly.{{U.S. Food and Drug Administration. (2025). Drug Label: 218316Orig1s000lbl. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/218316Orig1s000lbl.pdf Accessed: 05 March 2026)}}
These trials don’t just test effectiveness; they also evaluate safety and adverse reactions. When pooling the results of all the trials, we can see that there were some common side effects, like nausea, diarrhea, and vomiting, but interestingly, 3% of those receiving the Wegovy injection also reported hair loss. In the placebo group, 1% of users reported hair loss.
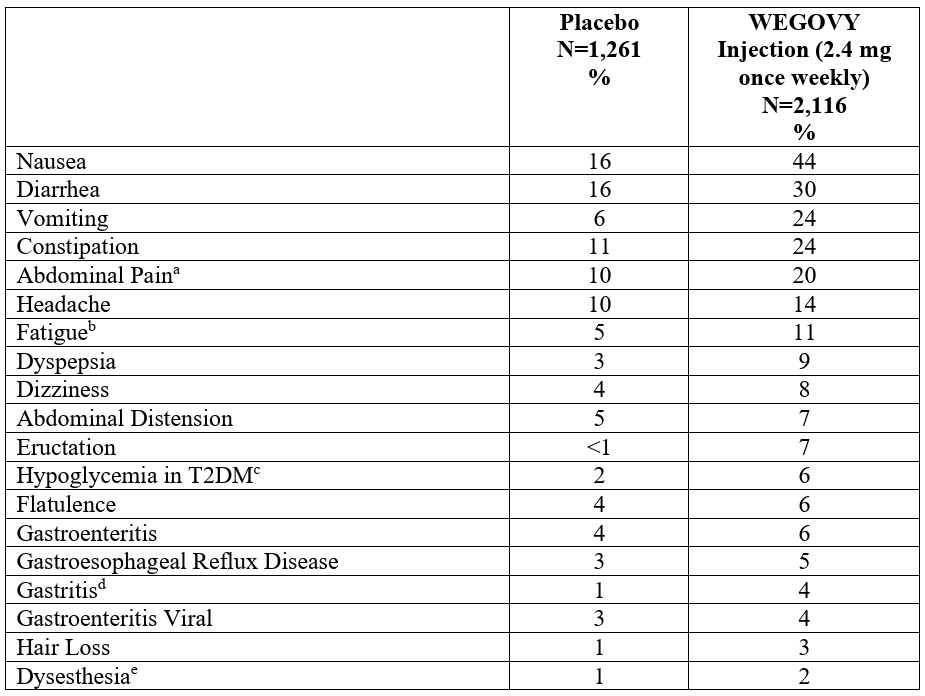
Figure 6: Adverse reactions reported in clinical trials with Wegovy. Adapted from Table 3.{{U.S. Food and Drug Administration. (2025). Drug Label: 218316Orig1s000lbl. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/218316Orig1s000lbl.pdf (Accessed: 05 March 2026)}}
We don’t know what kind of hair loss was reported (e.g., telogen effluvium, androgenic alopecia, alopecia areata) or whether the hair loss was clinically diagnosed or self-reported by the user. This makes it difficult to understand the validity of these results. However, it does bring up an important question: Is hair loss truly associated with Wegovy, or is there a natural progression of hair loss occurring while people are taking Wegovy, which they are attributing to the medication?
Overall conclusion: There may be an association between Wegovy and hair loss, but we don’t know whether Wegovy was the cause or what kind of hair loss it may have influenced.
2025 and 2026 Case Reports
Case reports describe the diagnosis, treatment, and follow-up of an individual patient. These types of reports are good for documenting rare or unexpected clinical outcomes. There are two recent case reports describing hair loss following treatment with semaglutide.
Before we get into the reports, let’s just discuss what we can and cannot take from case reports like these. Because they just follow one patient, the results aren’t generalizable to an entire population of people, and sometimes the lack of other study design parameters (like the use of controls, randomization) prevent strong conclusions on cause-and-effect to be made. However, we can use these reports to support the conclusion that there could be an association between the events described in the case.
2025 Case Report
This case report followed a 23-year-old obese female who had been using semaglutide for weight loss over the prior 4 months, injecting 0.25 mg once weekly for the first 2 months, and 0.5 mg once weekly for the remaining 2 months. As she entered her 3rd month of treatment, she noticed the sudden onset of hair loss, with multiple round patches of baldness appearing on the scalp.{{Alzahrani, W.S., Bahkali, S.A., Alharthy, R.F., Alsabban, A.S., (2025). Alopecia Areata Following Semaglutide Treatment For Weight Loss: A Case Report. JAAD Case Reports. 63. 44-46. Available at: https://doi.org/10.1016/j.jdcr.2025.06.012}}
Scalp analysis by a dermatologist revealed:
- Slight redness
- No scaling
- No noticeable changes in the scalp
The hair loss and hair examination were in line with a diagnosis of alopecia areata.
The patient was advised to stop semaglutide and to begin treatment for alopecia areata using a combination of intralesional corticosteroids, 2% ketoconazole shampoo, and 5% topical minoxidil. With the treatment, her hair regrew.
Overall conclusion: There may be an association between a semaglutide like Wegovy and alopecia areata, but there is no evidence that the semaglutide was the cause of alopecia areata.

Figure 7: Visible patches of hair loss following semaglutide treatment. Adapted from Figure 4.{{Alzahrani, W.S., Bahkali, S.A., Alharthy, R.F., Alsabban, A.S., (2025). Alopecia Areata Following Semaglutide Treatment For Weight Loss: A Case Report. JAAD Case Reports. 63. 44-46. Available at: https://doi.org/10.1016/j.jdcr.2025.06.012}} Image used under the Creative Commons License.
2026 Case Report
This 2026 case report followed a 33-year-old male who was receiving a 2.4 mg dose of semaglutide weekly. After 2 days, he noticed a small patch of hair loss. After 6 weeks, hair loss was noticeable as a 5 cm2 patch on the left side of his head.{{Cheng, J.-R., Zheng, J., Li, Y., Shi, H., Yang, N., Lei, Y., Wan, Y.-F. (2026). Weight Loss-Associated Alopecia Areata. American Journal of Therapeutics. Available at: https://doi.org/10.1097/MJT.0000000000001851}}
Semaglutide injections were stopped due to the diagnosis of alopecia areata, and the patient’s alopecia improved 2 months after discontinuing the injections.
Overall conclusion: There may be an association between a semaglutide like Wegovy and alopecia areata, but there is no evidence that the semaglutide was the cause of alopecia areata.
2024 FAERS Study
FAERS is the FDA Averse Event Reporting System, a publicly-accessible, searchable FDA system that collects reports of drug adverse events.
In 2024, a group of researchers explored the relationship between GLP-1 medications and hair loss by searching reports between 2022 and 2023 related to GLP-1 medications and hair loss.{{Godfrey, H., Leibovit-Reiben, Z., Jedlowski, P., Thiede, R. (2025). Alopecia Associated With The Use Of Semaglutide And Tirzepatide: A Disproportionality Analysis Using The FDA Adverse Event Reporting System (FAERS) From 2022 To 2023. Journal Of The European Academy Of Dermatology And Venereology. 39. e153-e154. Available at: https://doi.org/10.1111/jdv.20197}} They then carried out a disproportionality analysis, a type of statistical test that assesses whether side effects are reported more often in people using a drug than would occur in the general population. What they found was surprising.
Increased reporting odds of hair loss for:
- Semaglutide (199 cases)
- Tirzepatide (179 cases)
No increased reporting odds of hair loss for:
- Liraglutide (20 cases)
- Dulaglutide (65 cases)
- Exenatide (6 cases)
- Lixisenatide (0 cases)
There are a substantial number of reported cases of hair loss with the use of semaglutide and tirzepatide GLP-1 medications. But we have to be aware that this type of analysis is not without several caveats.
Caveat #1: Reports can be made by anyone
Reports to FAERS can be made by consumers (i.e., the general public) and healthcare professionals alike. That means you can have reports backed by clinical diagnosis, as well as subjective reports where there is no clinician-confirmed diagnosis of hair loss. The study reported that 84% of the reports were from consumers, and 16% were from healthcare professionals.
Caveat #2: Reports can be viewed by anyone
FAERS is publicly accessible. So, anyone can review the results, including the general public and the media. The public and the media may see reports of hair loss by some GLP-1 medications and then create social media posts or sensationalized headlines. This puts the concept of GLP-1 medications as a factor influencing hair loss into the public consciousness, which may increase self-diagnosed reports of hair loss.
Caveat #3: Reports lack clinical detail
All we see from these reports is that some hair loss occurred. We don’t know what type of hair loss was diagnosed, whether any objective measurements were used to facilitate a clinical diagnosis (e.g., hair counts), or whether there are any other factors in the user’s life that could have influenced this happening (genetics, stress, etc.). All these factors matter when determining an association between GLP-1 medications and hair loss.
Because of these caveats, it’s difficult to build a clear picture of how exactly GLP-1 medications like semaglutide are contributing to reports of hair loss.
Overall conclusion: This FAERS study identifies potential safety signals but does not demonstrate that semaglutide medications are a cause of hair loss in these individuals.
2025 Retrospective Studies
A retrospective study looks back at existing data, usually at medical records, to investigate relationships between past exposures and outcomes. Much like case studies, these types of studies lack randomization and control groups that would permit a cause-and-effect relationship to be established, but we can still draw some conclusions from them.
Retrospective Study #1
The first retrospective study analyzed the medical records of 283 adult patients who were taking GLP-1 medications and had also visited the dermatology department for hair loss between 2021 and 2023.{{Burke, O. (2025). Glucagon-Like Peptide-1 Receptor Agonist Medications And Hair Loss: A Retrospective Cohort Study. Journal Of The American Academy Of Dermatology. 92(5). 1141-1143. Available at: https://doi.org/10.1016/j.jaad.2025.01.046}}
Findings:
- 84.1% of users reported no hair loss
- 1.2% of users with no prior history of hair loss reported new hair loss
- Over 90% of the users with pre-existing hair loss (approximately 13%) experienced worsening of their hair loss
Let’s look at these numbers in more detail.
Most of the users did not report any hair loss. This shows that instances of hair loss are not common among those receiving GLP-1 medications, and suggests that, for many, hair loss shouldn’t be a concern if they are prescribed this treatment.
Approximately 1% of users experienced new hair loss, without a prior history of this previously. This might sound bad, but in reality, this matches the rate of hair loss that is expected in the general population over two years. So, are these instances of new hair loss really down to the GLP-1, or down to natural hair loss?
Most of the users with pre-existing hair loss experienced worsening of their condition. Namely, semaglutide was most strongly associated with androgenic alopecia. This is similar to the FAERS study, where semaglutide was identified as having a strong correlation with hair loss reports.
Aside from the common limitations with retrospective studies, the researchers did not include medication duration in their analysis, and hair loss was self-reported by patients instead of being objectively measured, like through hair counts. The time medications were taken matters, because hair loss conditions like telogen effluvium often occur 2 to 8 months after a “trigger”, like when a new medication is taken. Also, with self-reports, we can’t know whether the patients were truly experiencing hair loss as would be defined by a clinician.
Overall conclusion: These findings warrant further investigation into the relationship between semaglutide and hair loss, but do not demonstrate causation.
Retrospective Study #2
In this second retrospective study, the researchers searched health records of over 100 million patients. They isolated patients who had no prior history of hair loss, but were taking GLP-1 medications (liraglutide, semaglutide, dulaglutide, exenatide, lixisenatide, or tirzepatide).{{Akiska, Y.M., Vidal, S.I., Menta, N. (2025). Increased Incidence And Risk Of Hair Loss With Glucagon-Like Peptide 1 Receptor Agonists: A Real-World Multicentre Cohort Study. EMJ. 13(1). 52-54. Available at: https://doi.org/10.33590/emjdermatol/TYEW1122}} They identified over 500,000 people who met this criteria.
After 6 months of treatment, use of GLP-1 medications was associated with:
- Increased risk of androgenic alopecia
- Increased risk of non-scarring hair loss
- No significant change to the risk of telogen effluvium
- No significant change to the risk of alopecia areata
After 12 months of treatment, use of GLP-1 medications was associated with:
- Increased risk of androgenic alopecia
- Increased risk of non-scarring hair loss
- Increased risk of telogen effluvium
- No significant change to the risk of alopecia areata
Interestingly, no increased risk of alopecia areata was found, given that GLP-1 medications like semaglutide have been reported to be linked to this condition in case studies.
It is also interesting that telogen effluvium risk increased with use over 12 months, but not 6 months. With telogen effluvium, the onset of hair loss after experiencing a trigger can be between 2 and 8 months.{{Malkud, S., (2015). Telogen Effluvium: A Review. Journal Of Clinical And Diagnostic Research. 9(9). WE01-WE03. Available at: https://doi.org/10.7860/JCDR/2015/15219.6492}} These results would suggest that the onset of telogen effluvium was consistently greater than 6 months.
However, the study design here does not allow us to say whether GLP-1 medications were the cause of hair loss in those instances.
Overall conclusion: These findings warrant further investigation into the relationship between semaglutide and hair loss, but do not demonstrate causation.
What Does It All Mean?
The clinical trials are robust in their design, but they did not further explore the cause of the hair loss reported by some users of Wegovy.
Similarly, case reports are great for documenting rare events, and retrospective studies are useful for identifying patterns, but neither can establish a cause-and-effect relationship.
So, none of these studies suggest a cause-and-effect relationship between semaglutide medications and hair loss. But what they do show is that there may be an association between semaglutide medications and hair loss, and that this is an association worthy of further investigation.
How Might Wegovy Cause Hair Loss?
There is no evidence to suggest that a semaglutide like Wegovy is a cause of hair loss, but we have established that there could be some association between these two factors. What could cause this association? For now, we don’t know. But there are a few plausible biological explanations.{{Desai, D.D., Sikora, M., Nohria, A., Bordone, L., Caplan, A.S., Shapiro, J., Lo Sicco, K.I. (2024). GLP-1 Agonists And Hair Loss: A Call For Further Investigation. International Journal Of Dermatology. 63. 1128-1130. Available at: https://doi.org/10.1111/ijd.17246}}
Physiological Changes
Rapid weight loss from using a treatment like Wegovy can have a number of physiological effects on the body, and also introduce some dietary changes. These include:
- Calorie restriction
- Nutritional deficiencies
- Protein deficiences
- Physiological stress
These changes are interlinked. For example, calorie restriction can cause physiological stress and may also lead to nutritional and protein deficiencies. All of these stressors are possible when people undergo rapid weight loss. In line with this, studies have shown that GLP-1 users with weight loss often do not have adequate nutritional intake.{{Johnson, B., Milstead, M., Thomas, O. (2025). Investigating Nutrient Intake During Use Of Glucagon-Like Peptide-1 Receptor Agonist: A Cross-Sectional Study. Frontiers In Nutrition. 12. 1566498. Available at: https://doi.org/10.3389/fnut.2025.1566498}} Nutritional deficiencies like these could be a clear cause of hair loss, since protein, iron, and zinc are essential for normal hair cycles and hair growth. You can learn more about the vitamin deficiencies that cause hair loss in our article here.
But there is also a more nuanced perspective. These stressors could trigger telogen effluvium or alopecia areata.
Calorie restriction, nutritional deficiencies, protein deficiencies, and physiological stress can all be characterized as “negative events” or “environmental factors” that could trigger conditions like these because they disrupt the normal hair growth process. There is research to support this thought:
- Rapid weight loss is a well-known trigger for telogen effluvium. It is not unheard of that after patients have undergone bariatric surgery (weight loss surgery), they soon experience telogen effluvium.{{Cohen-Kurzrock, R.A., Cohen, P.R., (2021). Bariatric Surgery-Induced Telogen Effluvium (Bar SITE): Case Report And A Review Of Hair Loss Following Weight Loss Surgery. Cureus. 13(4). e14617. Available at: https://doi.org/10.7759/cureus.14617}},{{Rojas, P., Gosch, M., Basfi-Fer, K., (2011). Alopecia In Women With Severe And Morbid Obesity Who Undergo Bariatric Surgery. Nutricion Hospitalaria. 26(4). 856-862. Available at: https://doi.org/10.1590/s0212-16112011000400028}},{{Nadler, E.P., Youn, H.A., Ginsburg, H.B., Ren, C.J., Fielding, G.A., (2007). Short-Term Results In 53 US Obese Pediatric Patients Treated With Laparoscopic Adjustable Gastric Banding. Journal Of Pediatric Surgery. 42(1). 137-142. Available at: https://doi.org/10.1016/j.jpedsurg.2006.09.014}},{{Nadler, E.P., Youn, H.A., Ren, C.J., Fielding, G.A., (2008). An Update On 73 US Obese Pediatric Patients Treated With Laparoscopic Adjustable Gastric Banding: Comorbidity Resolution And Compliance Data. Journal Of Pediatric Surgery. 43(1). 141-146. Available at: https://doi.org/10.1016/j.jpedsurg.2007.09.035}}
- Telogen effluvium can be triggered by calorie deficit.{{Kang, D.H., Kwon, S.H., Sim, W.Y., Lew, B.L., (2024). Telogen Effluvium Associated With Weight Loss: A Single Center Retrospective Study. Annals Of Dermatology. 36(6). 384-388. Available at: https://doi.org/10.5021/ad.24.043}}
- Alopecia areata has been associated with deficient dietary protein and vitamin D.{{Pham, C.T., Romero, K., Almohanna, H.M., Griggs, J., Ahmed, A., Tosti, A. (2020). The Role Of Diet As An Adjuvant Treatment In Scarring And Nonscarring Alopecia. Skin Appendage Disord. 6(2). 88-96. Available at: https://doi.org/10.1159/000504786}},{{Bhat, Y.J., Latif, I., Malik, R., Hassan, I., Sheikh, G., Lone, K.S., Majeed, S., Sajad, P. (2017). Vitamin D Level In Alopecia Areata. Indian Journal Of Dermatology. 62(4). 407-410. Available at: https://doi.org/10.4103/ijd.IJD_677_16}}
We should also consider that symptoms like diarrhea are common in those taking Wegovy. Diarrhea is a result of intestinal inflammation. Is it possible, then, that this inflammation event could trigger an inflammation event of the scalp, like one that might onset alopecia areata? For now, we don’t know. These are all plausible biological explanations, but there is a lack of clinical trials to show a direct link between Wegovy-associated physiological changes and hair loss.
One curious thing is the association between Wegovy and androgenic alopecia. Why might this happen?
For those without underlying androgenic alopecia, hair loss from telogen effluvium may get better once the triggers (like rapid weight loss and dietary changes) are removed, and for those experiencing alopecia areata, hair regrowth may be initiated with the removal of triggers and intervention with autoimmune therapies. But, for those experiencing telogen effluvium combined with either androgenic alopecia or alopecia areata, the story might be a bit different.
Since hair follicle miniaturization can occur after each hair cycle, enhanced shedding could accelerate this process. Therefore, telogen effluvium triggered by rapid weight loss may actually accelerate hair thinning in those who already have androgenic alopecia or alopecia areata. This could explain the connection between hair loss and Wegovy.
[ulo_promo title=”All-Natural Hair Supplement” subtitle=”The top natural ingredients for hair growth, all in one supplement.” description=”Take the next step in your hair growth journey with a world-class natural supplement. Ingredients, doses, & concentrations built by science. ” button_text=”Shop Supplements” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/hair-growth-supplement?variant=42246589546575” prescription=”false” type=”otc-supplement” ]
Hormonal and Signaling Changes
In the normal growth cycle of hair follicles, hair growth is stimulated by a factor known as insulin-like growth factor 1 (IGF-1). IGF-1 not only stimulates hair follicle proliferation, but also inhibits hair follicle cell death, and stimulates the transition from the telogen phase to the anagen phase.{{Hsieh, W.J., Qiu, W.Y., Percec, I., Chang, T.M., (2025). Insulin-Like Growth Factor 1 (IGF-1) In Hair Regeneration: Mechanistic Pathways And Therapeutic Potential. Current Issues In Molecular Biology. 47(9). 773. Available at: https://doi.org/10.3390/cimb47090773}}
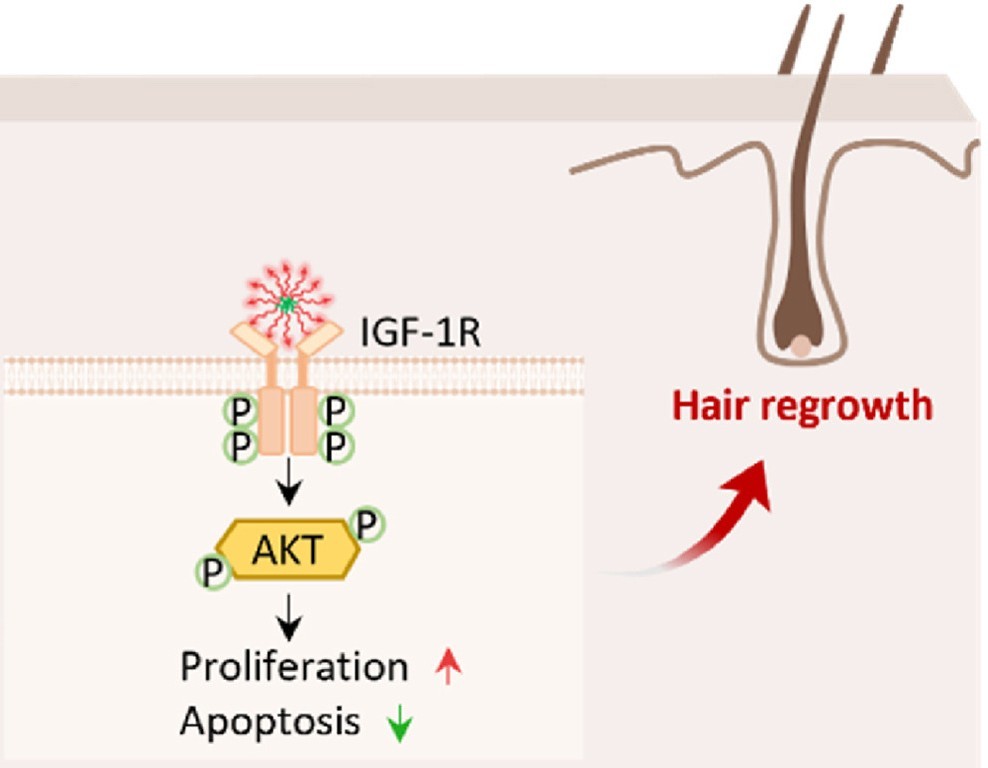
Figure 8: How an IGF-1 mimic can promote hair growth. Adapted from Figure 1.{{Hu, X., Guo, L., Ding, Y., Nie, S., Fang, J., Li, J., Han, Q., Ding, D., Zhang, Q., Wang, T., Wang, L., Wang, M., Yang, Z. (2025). Self-Assembling Peptide Inspired By Insulin And Type 1 Insulin-Like Growth Factor For The Treatment Of Androgenetic Alopecia. Bioactive Materials. 53. 819-830. Available at: https://doi.org/10.1016/j.bioactmat.2025.08.004}} Image used under the Creative Commons License.
If an outside influence were to disrupt the IGF-1 pathway, it would follow that this outside influence could also disrupt hair growth, and maybe that’s what happens with Wegovy.
We know that semaglutide can change insulin synthesis after food intake. Prolonged energy deficit and weight loss often reduce circulating insulin levels, and similar reductions in insulin have been observed for GLP‑1 agonist users.{{{Jørgensen, S.W., Hjort, L., Gillberg, L., Justesen, L., Madsbad, S., Brøns, C., Vaag, A.A. (2021). Impact Of Prolonged Fasting On Insulin Secretion, Insulin Action, And Hepatic Versus Whole Body Insulin Secretion Disposition Indices In Healthy Young Males. American Journal Of Physiology Endocrinology And Metabolism. 320(2). E281-E290. Available at: https://doi.org/10.1152/ajpendo.00433.2020}},{{Alhowiti, A., Mirghani, H. (2025). The Effects Of GLP-1 Agonists On HbA1c And Insulin Dose Among Patients With Type 1 Diabetes. Frontiers In Endocrinology. 16. 1550938. Available at: https://doi.org/10.3389/fendo.2025.1550938}},{{Luo, Y., Yang, S., Zeng, H., Liu, S., Zhang, Y., Li, J.E., Liu, J. (2025). Both Subcutaneous Semaglutide And Calorie Restriction Improves Pancreatic Cell Hyperplasia And Gut Microbiota In High-Fat Diet-Induced Obese Mice. Nutrition And Metabolism. 22(1). 95. Available at: https://doi.org/10.1186/s12986-025-00987-0}}
How does this relate to IGF-1? Well, insulin is a primary factor modulating the availability of IGF-1 in the body.{{Brismar, K., Fernqvist-Forbes, E., Wahren, J., Hall, K., (1994). Effect Of Insulin On The Hepatic Production Of Insulin-Like Growth Factor-Binding Protein-1 (IGFBP-1), IGFBP-3, And IGF-I In Insulin-Dependent Diabetes. Journal Of Clinical Endocrinology And Metabolism. 79(3). 872-878. Available at: https://doi.org/10.1210/jcem.79.3.7521354}} It is possible that by affecting insulin levels in the body, a drug like Wegovy may inadvertently affect the normal hair growth cycle.
A case study with a 54-year-old woman experiencing hair loss showed that treatment with insulin therapies was associated with a reduction in hair shedding. Hair shedding was not improved with minoxidil, suggesting usual causes of hair loss were not the underlying problem here. Although cause-and-effect can not be established, the case supports the notion that insulin and hair growth are linked.{{Kant, R., Barnwal, S., Sharma, S.K., Thakur, K. (2021). Reversal Of Alopecia By Insulin Therapy In Uncontrolled Type 2 DM: A Case Report. Journal Of Diabetology. 12(4). 533-537. Available at: https://doi.org/10.4103/jod.jod_66_21}}
It is not without mention that changes to insulin could also be a trigger for alopecia areata or telogen effluvium. With the latter, this may accelerate hair thinning in those with androgenic alopecia, as we’ve discussed.
Hair Cycle Changes
A 2006 study in mice found high levels of the hormone GLP-1 in the hair follicles of newborn mice. The researchers also discovered that GLP-1 activated a signalling pathway in skin cells called MAPK/ERK, which is known to be involved in cell growth and division.{{List, J.F., He, H., Habener, J.F. (2006). Glucagon-Like Peptide-1 Receptor And Proglucagon Expression In Mouse Skin. Regulatory Peptides. 134(2–3). 149-157. Available at: https://doi.org/10.1016/j.regpep.2006.02.007}}
Based on these findings, the scientists suggested that GLP-1 may play a role in the development of hair follicles. This raises the question of whether GLP-1 medications could have any effects on the hair cycle, a possible link between Wegovy and hair biology.
However, it’s important to note that this research was conducted only in animals and did not include human participants. Results seen in animal studies do not always apply to people. So while the study suggests GLP-1 may influence the hair cycle in mice, it does not show that the same process happens in humans.
Distinguishing Between Androgenic Alopecia, Telogen Effluvium, and Alopecia Areata
Hair loss can be distressing. If you are using Wegovy and are troubled about hair loss, it’s important to first assess what kind of hair loss you might have.
Gradual (over many years), patterned thinning, and possibly a family history of balding? The likely cause is androgenic alopecia.
Sudden diffuse hair shedding without thinning, that has onset 2 to 8 months after taking Wegovy, or follows another recent stressful event? The likely cause is telogen effluvium.
Sudden patchy hair loss with a smooth bald spot and hair thinning, possibly with previous similar episodes or a personal or family history of autoimmune disease? The likely cause is alopecia areata.
I’m Using Wegovy, Should I Be Concerned?
Signs Should I be concerned? I have no signs of hair loss or a family history of hair loss No, probably not. The evidence suggests that people with these signs are at a very low risk of developing new hair loss from Wegovy. I have signs of hair loss, and may or may not have a family history of hair loss Maybe. The evidence suggests that medications like Wegovy could worsen existing hair loss by causing telogen effluvium, although there is no clinical evidence directly showing that this is the case. I have early signs of hair loss, or haven’t noticed any ongoing hair loss, and may or may not have a family history of hair loss Maybe. If you haven’t noticed any hair loss, but are predisposed to androgenic alopecia or alopecia areata, a medication like Wegovy may progress thinning to a point where it is noticeable if telogen effluvium occurs. Again, there is no clinical evidence to back this theory, but it is a plausible scenario. What Can I Do To Prevent Hair Loss With Wegovy?
#1: Avoid rapid weight loss
When pursuing weight loss, it is important to avoid aggressive calorie restriction, as severe deficits can stress the body and contribute to unwanted side effects such as increased hair shedding.
#2: Eat a balanced diet, or take supplements
Aim for a balanced approach that ensures adequate intake of essential nutrients. In particular, sufficient protein is critical because hair is primarily made of keratin, a protein that depends on dietary amino acids for growth and maintenance.
Adequate micronutrients, including iron, zinc, vitamin D, and B vitamins, are also necessary to support healthy hair follicles and overall metabolic function.
#3: Monitor your hair
During periods of rapid weight loss, monitor for increased hair shedding, which can occur due to physiological stress or nutrient deficiencies. Tracking changes early can help identify problems before significant hair thinning develops.
#4: Get an opinion before starting Wegovy, and consider hair loss treatments
For individuals planning weight loss with Wegovy, it may be beneficial to obtain a baseline scalp evaluation from a healthcare professional to see whether there is any ongoing hair loss or whether there might be potential for hair loss in the future.
If you have a known predisposition to hair loss, talk to your doctor about early intervention with appropriate hair loss treatments like topical minoxidil or oral finasteride. These may be able to help preserve hair density while weight loss progresses. You can learn more about minoxidil, the side effects, and how to minimize them in our article here.
Final Thoughts
Online discussions and patient reports have caused concern that weight loss treatments like Wegovy may cause hair loss. Unfortunately, the current clinical evidence remains limited. A small number of case reports suggest that alopecia areata can occur in some individuals taking semaglutide, and larger retrospective studies indicate that, while most users do not experience significant hair loss during treatment, some with underlying hair loss conditions, like androgenic alopecia, experience a worsening of their condition.
We don’t know why or how this might happen. However, we can speculate that this may be caused by the onset of telogen effluvium. Rapid weight loss and nutrient deficiencies are well-established triggers for telogen effluvium, and are possible while taking a medication like Wegovy. So, the hair changes observed during Wegovy therapy are likely not a result of the drug itself, but rather the physiological effects of weight loss.
Large, randomized, and controlled clinical trials are needed to confirm the relationship between Wegovy and hair loss. But for now, we recommend that if you are considering Wegovy, consider evaluating your hair health first. Consult your doctor, and implement appropriate treatment routes, lifestyle changes, and hair loss treatments for the best chance to avoid sudden changes to your hair when you are trying to lose weight.
GLP-1 agonists, including tirzepatide, are the new “it drugs”, rapidly gaining popularity over the last few years. While other GLP-1 agonists have previously held market dominance, tirzepatide has emerged as the most prescribed GLP-1 drug in the U.S in 2025.{{Truveta Research, (2025), GLP-1 RA Prescription Trends: January 2018 – June 2025. Available at: https://www.truveta.com/blog/research/glp-1-ra-prescription-trends-january-2018-june-2025/ (Accessed: 13 March 2026)}} A survey completed in 2024 found that approximately one in eight adults had at some point used a GLP-1 agonist, with 6% taking the drugs at the time of the survey.{{Montero, A., Sparks, G., Presiado, M., Hamel, L., (2024), KFF Health Tracking Poll May 2024: The Public’s Use And Views Of GLP-1 Drugs. Available at: https://www.kff.org/health-costs/kff-health-tracking-poll-may-2024-the-publics-use-and-views-of-glp-1-drugs/ (Accessed: 27 February 2026)}} Numbers are likely to have risen even further since then, with tens of millions of people having taken the drugs.
However, the many positive reports of weight loss and blood sugar control on taking GLP-1 agonists have been accompanied by increasing reports of side effects. Gastrointestinal problems are the most well-established side effect, but reports of hair loss are emerging on social media and internet forums. These alarming stories are becoming more prevalent, but are they actually true?
[ulo_promo title=”Interested in Topical Minoxidil?” subtitle=”High-strength topical minoxidil available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-minoxidil?variant=42247221313615” prescription=”true” type=”topical” ]
In this article, we have searched through the clinical literature to find out whether these claims are supported by the science. We will cover what tirzepatide is and how it works, evidence supporting hair loss claims, and potential hair loss mechanisms influenced by tirzepatide.
What is Tirzepatide?
Tirzepatide is the active drug molecule used in brand-name medications such as Mounjaro and Zepbound. Originally produced for use in type 2 diabetes, tirzapetide is now widely used both for diabetes treatment and weight loss. It involves a once-weekly injection.
Unlike Ozempic (the other main GLP-1 agonist drug), tirzepatide binds to two hormone receptors: glucagon-like peptide-1 (GLP-1) receptors and glucose-dependent insulinotropic polypeptide (GIP) receptors, making it a dual agonist.{{Farzam, K., Patel, P. (2024). Tirzepatide. StatPearls. Available at: http://www.ncbi.nlm.nih.gov/books/NBK585056/ (Accessed: 16 March 2026)}}
Initial clinical trials with tirzepatide found that the drug successfully controlled type 2 diabetes while simultaneously resulting in significant weight loss in many users.{{Coskun, T., Sloop, K.W., Loghin, C. (2018). LY3298176, A Novel Dual GIP And GLP-1 Receptor Agonist For The Treatment Of Type 2 Diabetes Mellitus: From Discovery To Clinical Proof Of Concept. Molecular Metabolism. 18. 3-14. Available at: https://doi.org/10.1016/j.molmet.2018.09.009}} Large-scale clinical trials further demonstrated the effectiveness of tirzepatide, showing an average of 15% weight loss by week 72 with 5 mg weekly injections.{{Jastreboff, A.M., Aronne, L.J., Ahmad, N.N. (2022). Tirzepatide Once Weekly For The Treatment Of Obesity. New England Journal Of Medicine. 387(3). 205-216. Available at: https://doi.org/10.1056/NEJMoa2206038}}
Tirzepatide is available either as Mounjaro (FDA-approved for the treatment of type 2 diabetes) or as Zepbound (FDA-approved for chronic weight management in obese adults). Other related GLP-1 agonists include Ozempic and Liraglutide, but these do not contain tirzepatide as their active ingredient, are not dual agonists, and use slightly different mechanisms.

Figure 1. Tirzepatide is often sold as Mounjaro in the form of a pre-filled injection pen.
How Does Tirzepatide Work?
GLP-1 and GIP are both peptides found naturally within the body. They are released into the bloodstream in response to food consumption and act to increase insulin secretion, improving blood glucose levels.{{Wolfe, M.M., Boylan, M.O., Chin, W.W. (2025). Glucose-Dependent Insulinotropic Polypeptide In Incretin Physiology: Role In Health And Disease. Endocrine Reviews. 46(4). 479-500. Available at: https://doi.org/10.1210/endrev/bnaf006}}
Tirzepatide is a synthetic peptide with the ability to mimic natural GIP and GLP-1, resulting in the activation of their receptors. This results in a combined effect of:{{Holst, J.J. (2007). The Physiology Of Glucagon-Like Peptide 1. Physiological Reviews. 87(4). 1409-1439. Available at: https://doi.org/10.1152/physrev.00034.2006}},{{Drucker, D.J. (2022). GLP-1 Physiology Informs The Pharmacotherapy Of Obesity. Molecular Metabolism. 57. 101351. Available at: https://doi.org/10.1016/j.molmet.2021.101351}},{{Jiang, Y., Zhu, H., Gong, F. (2024). Why Does GLP-1 Agonist Combined With GIP And/Or GCG Agonist Have Greater Weight Loss Effect Than GLP-1 Agonist Alone In Obese Adults Without Type 2 Diabetes? Diabetes, Obesity And Metabolism. 27(3). 1079-1095. Available at: https://doi.org/10.1111/dom.16106}}
- Increased insulin secretion after eating.
- Inhibited glucagon secretion to reduce spikes in blood sugar.
- Slowing stomach emptying to help people feel fuller for longer.
- Suppressed appetite, resulting in reduced food cravings and decreased calorie intake.
When both the GLP-1 and GIP receptors are stimulated, their effects are magnified further than the activation of only one receptor. As such, tirzepatide is thought to be more effective than semaglutide (Ozempic), both for blood sugar control and weight loss.{{Frías, J.P., Davies, M.J., Rosenstock, J. (2021). Tirzepatide Versus Semaglutide Once Weekly In Patients With Type 2 Diabetes. New England Journal Of Medicine. 385(6). 503-515. Available at: https://doi.org/10.1056/NEJMoa2107519}},{{Rodriguez, P.J., Goodwin Cartwright, B.M., Gratzl, S. (2024). Semaglutide Vs Tirzepatide For Weight Loss In Adults With Overweight Or Obesity. JAMA Internal Medicine. 184(9). 1056-1064. Available at: https://doi.org/10.1001/jamainternmed.2024.2525}}
Does Tirzepatide Cause Hair Loss?
Although tirzepatide and other GLP-1 agonists have been approved by the FDA, they have not been used by the general public for very long. As a result, the understanding of long-term effects and the comprehensive analysis of side effects remains limited. As the number of people using the drugs rapidly rises, reports of side effects are becoming more prominent.
The most common side effects are gastrointestinal, including nausea, vomiting, and abdominal pain.{{Jastreboff, A.M., Aronne, L.J., Ahmad, N.N. (2022). Tirzepatide Once Weekly For The Treatment Of Obesity. New England Journal Of Medicine. 387(3). 205-216. Available at: https://doi.org/10.1056/NEJMoa2206038}} A small number of GLP-1 agonist users may experience serious side effects, including pancreatitis, gallbladder disease, or kidney injury.
Stories of hair thinning and hair loss as a result of taking GLP-1 agonists are gaining traction on social media and forums (such as Reddit). But are these accurate, or are they simply anecdotal reports?
Clinical Evidence
The existing clinical data linking tirzepatide to hair loss are limited. Throughout the process of progressing a drug to the market, side effects are comprehensively assessed to ensure the safety of the product. These side effects are publicly reported, and enable researchers to decide whether the benefits of the drug outweigh the potential harm caused by side effects.
In early tirzepatide clinical trials assessing its efficacy for treating type 2 diabetes, gastrointestinal adverse events were often reported, but there were no reports of alopecia.{{Frías, J.P., Davies, M.J., Rosenstock, J. (2021). Tirzepatide Versus Semaglutide Once Weekly In Patients With Type 2 Diabetes. New England Journal Of Medicine. 385(6). 503-515. Available at: https://doi.org/10.1056/NEJMoa2107519}} However, some of the earliest trials using tirzepatide for obesity reported alopecia as an adverse event occurring within the tirzepatide treatment group. In one study, alopecia was reported in 5.1% of people taking 5 mg tirzepatide, compared to only 0.9% in the placebo group.{{Jastreboff, A.M., Aronne, L.J., Ahmad, N.N. (2022). Tirzepatide Once Weekly For The Treatment Of Obesity. New England Journal Of Medicine. 387(3). 205-216. Available at: https://doi.org/10.1056/NEJMoa2206038}}
The reason for this disparity is unclear, but it may be due to the diabetes trial being shorter (only 40 weeks compared to 72 weeks for the obesity trial) or due to less stringent adverse event reporting.
With the approval of tirzepatide for weight loss, the use of this drug saw a rapid rise. However, this coincided with increasing reports of hair loss, leading to the FDA issuing a warning in 2023 that GLP-1 receptor agonists (such as tizepatide) may increase the risk of alopecia.{{Center for Drug Evaluation and Research, (2024), July – September 2023 | Potential Signals Of Serious Risks/New Safety Information Identified By The FDA Adverse Event Reporting System (FAERS). Available at: https://www.fda.gov/drugs/fda-adverse-event-monitoring-system-aems/july-september-2023-potential-signals-serious-risksnew-safety-information-identified-fda-adverse (Accessed: 16 March 2026)}} A small number of studies have investigated the link between tirzepatide and hair loss further.
Study #1
This study was conducted using the FDA Adverse Event Reporting System (FAERS), which collects reports of adverse drug events from consumers (i.e., the people taking the drug) and healthcare professionals. The study was published in 2025, but reported data from 2022-2023.{{Godfrey, H., Leibovit-Reiben, Z., Jedlowski, P., Thiede, R. (2025). Alopecia Associated With The Use Of Semaglutide And Tirzepatide: A Disproportionality Analysis Using The FDA Adverse Event Reporting System (FAERS) From 2022 To 2023. Journal Of The European Academy Of Dermatology And Venereology. 39(2). e153. Available at: https://doi.org/10.1111/jdv.20197}}
The researchers searched through the FAERS database to identify cases of alopecia linked to GLP-1 and GLP-1/GIP agonists. Within the time period assessed, 179 reports of alopecia were reported for tirzapetide, 199 reports for semaglutide (Ozempic), and fewer reports for other GLP-1 receptor agonists (GLP-1 RAs).
The researchers then carried out a statistical test on this data to assess whether alopecia was reported more often in people taking the GLP-1 RA than would normally occur in the FAERS database as a whole (this is known as a disproportionality analysis).
They found that tirzapetide and semaglutide showed an increase in reporting odds, so alopecia was reported more often in people taking either of these GLP-1 RAs than would be expected in the whole FAERS population.
This report highlighted the possibility of an association between tirzepatide and hair loss, but how much can we read into these results?
A few limitations exist within this study, which constrain our ability to make bold claims about tirzepatide and alopecia. These include:
- The methodology of this study and the disproportionality analysis used cannot prove a causal relationship.
- FAERS only uses voluntary reporting of adverse events, meaning that the data can be skewed by a heightened awareness of potential side effects (such as through attention in the news or reports on social media).
- 84% of the reports of alopecia made to FAERS were from consumers, and only 16% were from healthcare professionals, making it likely that users were self-diagnosing and had not received a clinician-confirmed report of alopecia.
- The type of hair loss was not reported.
Therefore, while this report contributes evidence supporting the association between tirzepatide and hair loss, it does not prove the connection. Additional studies must be carried out to determine whether tirzepatide (or other GLP-1 RAs) is directly causing hair loss.
Study #2
This study was conducted using a retrospective analysis of patients on GLP-1 RAs who had visited a dermatology department between 2021 and 2023. This consisted of 283 patients total, and used a real-world setting to assess reports of alopecia in GLP-1 RA users.{{Burke, O., Sa, B., Alvarez Cespedes, D., Sechi, A., & Tosti, A. (2025). Glucagon-like peptide-1 receptor agonist medications and hair loss: a retrospective cohort study. Journal of the American Academy of Dermatology. 92(5). 1141–1143. Available at: https://doi.org/10.1016/j.jaad.2025.01.046}}
Of the 283 patients on GLP-1 RAs who visited the dermatology clinic, the majority did not have hair loss (84.1%), but 35 presented with hair loss. Of these, only three (1.2%) were experiencing new hair loss (with no previous reports of hair loss). This is approximately in line with the rate that would be expected in the population as a whole over two years, so does not demonstrate any specific effects of GLP-1 RAs on new hair loss.
The results are more convincing for those with preexisting hair loss; of the 32 people presenting with preexisting hair loss (13%), 90% reported that their hair loss had worsened since using GLP-1 RA drugs. However, male pattern hair loss is a progressive condition, meaning that hair loss continues to worsen over time. The design of this trial (being retrospective) makes it impossible to distinguish between the effects that the drugs may be having on hair loss and the normal rate of hair loss that occurs with male pattern baldness.
Further analysis of the results from this trial failed to demonstrate any significant associations between GLP-1 RAs and hair loss, although a borderline significant value was found linking tirzepatide and a specific type of hair loss known as telogen effluvium, suggesting a potential contribution of tirzepatide to this condition.
While this study highlights a potential association between tirzepatide and hair loss, again, there are several limitations to the study, including:
- The work was retrospective, putting it at risk of selection bias, confounding variables, and missing data.
- There was no control group, meaning that a cause-and-effect relationship cannot be assessed, and it is not possible to separate the normal rate of hair loss from drug-induced hair loss.
- The length of time that patients were on GLP-1 RA medication was not recorded.
- There was no official alopecia diagnosis based on objective measures; instead, self-reported patient data was used.
Similar to the first study, a connection between tirzepatide and hair loss is possible based on the results of this work, but it cannot be conclusively proven.
Study #3
Another retrospective analysis study was carried out, this time using the TriNetX database. This is a data network of healthcare organizations around the world that pools patient data from anonymized electronic health records. It is a very large database, meaning that this study was able to look at the data of over 360,000 patients, of which ~60% had been prescribed GLP-1 RAs.{{Neubauer, Z., Ong, M.M., Singal, A., Lipner, S.R. (2025). Increased Risk Of Telogen Effluvium With Tirzepatide Compared To Other Weight Loss Medications: A Retrospective Cohort TriNetX Database Study. Journal Of The American Academy Of Dermatology. 93(6). 1612-1614. Available at: https://doi.org/10.1016/j.jaad.2025.08.033}}
This study was specifically investigating a type of hair loss known as telogen effluvium, not any other types of hair loss (such as male pattern baldness). Tirzepatide-treated patients were shown to have an increased risk of telogen effluvium, whereas other GLP-1 RAs did not show increased risk. The authors suggested that this was due to the superior weight loss effects of tirzepatide.
Again, this work suggests a link between tirzepatide and hair loss, but due to its retrospective nature, a cause-and-effect relationship cannot be established.
Study #4
This study was also conducted using the TriNetX database. They carried out two analyses, one of which was specifically using the TriNetX U.S. database (consisting only of healthcare organizations in the U.S.), and the second was a worldwide analysis. Similarly to the previous study, due to the large sizes of these databases, they were able to get over 500,000 matched patients in the U.S. analysis and over 600,000 in the worldwide analysis.{{Herrera, H.O., Bordeaux, J.S. (2026). Risk Of New-Onset Hair Loss With Semaglutide And Tirzepatide: A TriNetX Cohort Study. Journal Of The American Academy Of Dermatology. 0(0). Available at: https://doi.org/10.1016/j.jaad.2026.02.042}}
The researchers found that the use of tirzapetide and semaglutide was associated with an increased risk of hair loss, including androgenic alopecia and telogen effluvium. While promising, this study was limited by the lack of information on hair loss severity, the lack of an official hair loss diagnosis using imaging techniques, and its retrospective nature.
How Might Tirzepatide Contribute to Hair Loss?
While evidence is growing supporting an association between tirzepatide (and other GLP-1 RAs) and hair loss, the exact mechanisms through which this occurs are essentially all speculation at this point. They include:
Direct Effects on the Hair Cycle
It is possible that tirzepatide may directly influence the hair growth cycle. GLP-1 receptors have been found to be localized around hair follicles in the skin, although this has only been demonstrated in research animals so far. In one study, GLP-1 was shown to activate a signaling pathway in skin cells, leading to cell proliferation.{{List, J.F., He, H., Habener, J.F. (2006). Glucagon-Like Peptide-1 Receptor And Proglucagon Expression In Mouse Skin. Regulatory Peptides. 134(2). 149-157. Available at: https://pubmed.ncbi.nlm.nih.gov/16631262/}} This could have an impact on hair growth; however, this has not been proven in any animal or human studies so far.
Tirzepatide may also disrupt metabolic and hormonal signalling pathways involved in the hair cycle, such as the insulin/insulin-like growth factor-1 (IGF-1) pathway. Interference with such pathways may play a role in accelerating follicle shrinkage, the key mechanism in the development of AGA. This could then accelerate the onset or progression of hair loss in those predisposed to AGA.
Telogen Effluvium
Tirzepatide has been linked to hair loss in general, but has been specifically associated with telogen effluvium. Telogen effluvium is a form of alopecia where a physiological stress can cause excessive, diffuse shedding (i.e., hairs across the whole scalp are affected, not only those in certain areas).
The hair growth cycle consists of several phases, including anagen (the growth phase) and telogen (the resting phase). In a healthy scalp, approximately 85% of all of the hair on the head is in anagen, and 15% is in telogen.{{Hughes, E.C., Syed, H.A., Saleh, D., (2025), Telogen Effluvium. Available at: http://www.ncbi.nlm.nih.gov/books/NBK430848/ (Accessed: 16 March 2026)}}
When exposed to a physiological stress, many hairs abruptly and prematurely switch from anagen to telogen. Hair growth of these hairs ceases, and approximately three months later, the hairs are shed.
Physiological triggers can include metabolic stress from rapid weight loss. Telogen effluvium has been shown to occur in response to multiple causes of weight loss, including crash dieting and bariatric surgery.{{Kang, D.H., Kwon, S.H., Sim, W.Y., Lew, B.L. (2024). Telogen Effluvium Associated With Weight Loss: A Single Center Retrospective Study. Annals Of Dermatology. 36(6). 384-388. Available at: https://doi.org/10.5021/ad.24.043}},{{Zhang, W., Fan, M., Wang, C. (2021). Hair Loss After Metabolic And Bariatric Surgery: A Systematic Review And Meta-Analysis. Obesity Surgery. 31(6). 2649-2659. Available at: https://doi.org/10.1007/s11695-021-05311-2}}
Tirzepatide causes rapid weight loss in many users, with patients seeing as much as 25% weight reduction within 88 weeks.{{Aronne, L.J., Sattar, N., Horn, D.B. (2023). Continued Treatment With Tirzepatide For Maintenance Of Weight Reduction In Adults With Obesity: The SURMOUNT-4 Randomized Clinical Trial. JAMA. 331(1). 38-48. Available at: https://doi.org/10.1001/jama.2023.24945}} This rapid weight loss and metabolic stress from long-term calorie deficit may be the root-cause of the hair loss seen in many individuals taking tirzepatide.
While other GLP-1 RAs may also result in telogen effluvium, the additional weight loss thought to occur with tirzepatide may explain why tirzepatide in particular has been associated with telogen effluvium.
Telogen effluvium is a reversible condition in the majority of cases. As such, the removal of the physiological stressor (i.e., the sudden, rapid weight loss) will slow hair shedding, and hair will return to its original density.
Nutritional Deficiencies
GLP-1 RAs cause a reduction in appetite and cravings, resulting in a notable decrease in the amount of food eaten. As a result, people on these medications must carefully plan their diet to ensure that they are taking in all of the vitamins and minerals that are essential for normal bodily function and remaining healthy. In addition, they must ensure that sufficient protein is being consumed to retain muscle mass.{{Ida, S., Kaneko, R., Imataka, K. (2021). Effects Of Antidiabetic Drugs On Muscle Mass In Type 2 Diabetes Mellitus. Current Diabetes Reviews. 17(3). 293-303. Available at: https://doi.org/10.2174/1573399816666200705210006}}
One study investigating nutrient intake in GLP-1 RA users found that they were significantly under the recommended daily intake for several important nutrients, including vitamin B2, vitamin D, and iron.{{Johnson, B., Milstead, M., Thomas, O. (2025). Investigating Nutrient Intake During Use Of Glucagon-Like Peptide-1 Receptor Agonist: A Cross-Sectional Study. Frontiers In Nutrition. 12. 1566498. Available at: https://doi.org/10.3389/fnut.2025.1566498}}
Severe deficiencies in several nutrients have been implicated in hair loss, including vitamin D, iron, and vitamin B2.{{Almohanna, H.M., Ahmed, A.A., Tsatalis, J.P., Tosti, A. (2018). The Role of Vitamins And Minerals In Hair Loss: A Review. Dermatology And Therapy. 9(1). 51-70. Available at: https://doi.org/10.1007/s13555-018-0278-6}} This may be contributing to hair loss seen on GLP-1 RA use, but more research is needed to provide direct evidence for this.
Telogen Effluvium vs Androgenetic Alopecia
The existing evidence for tirzepatide-induced hair loss is limited; however, the small amount of evidence available indicates that tirzepatide may be influencing telogen effluvium and AGA. Both of these hair loss mechanisms have overlapping symptoms, so if you are experiencing hair loss, how can you tell the difference?
- Telogen effluvium occurs fairly quickly, about 3 months after a trigger (such as rapid weight loss). AGA occurs gradually over many years.
- The hairs shed via telogen effluvium look like normal hairs, with a standard hair shaft thickness. Hairs shed via AGA are often thinner, vellus-like hairs due to the miniaturization of the hair follicle altering the hair structure.
- Telogen effluvium causes hair shedding and reduced hair density across the whole scalp (diffuse shedding). AGA hair loss happens in a particular pattern, commonly a receding hairline and bald patch at the crown of the head.
It is possible that users of tirzepatide may experience either AGA or telogen effluvium, neither, or both simultaneously. The diffuse shedding of telogen effluvium may make AGA more obvious, and so it may seem that AGA has occurred very suddenly, when in fact it has been gradually progressing since before taking tirzepatide.
Should You Be Concerned?
If you have not experienced hair loss in the past, then there is probably little reason to be concerned.
The existing evidence so far suggests that people who have not previously experienced hair loss are unlikely to see a sudden onset of hair loss in response to taking tirzepatide. It is possible that rapid weight loss may trigger telogen effluvium, but this is often only temporary, and full hair density will be restored once the physiological trigger is removed.
If you have AGA, then you may be slightly more concerned. The studies carried out so far have shown a worsening of existing hair loss in some people taking tirzepatide. However, no placebo-controlled trials investigating this have been carried out, meaning that the effects seen may just be the natural progression of AGA over time.
Rapid weight loss-induced telogen effluvium may reveal AGA hair thinning that was previously unnoticed. As such, people with a genetic predisposition to AGA and with the early signs of it may suddenly appear to have experienced a dramatic loss of hair, when in actual fact this had been slowly progressing for years and has only now become noticeable.
If you are starting on tirzepatide:
- Avoid extreme calorie restriction.
- Ensure that you are taking in sufficient nutrients, including protein, vitamins, and minerals.
- Monitor your hair from the start, noting if you already have thinning areas, and tracking hair shedding (particularly considering the timing, as this could indicate telogen effluvium).
- If you already have AGA or know that you are likely predisposed to AGA, consider addressing hair loss early, such as through the use of hair loss treatments.
Hair loss treatments can be safely used alongside weight-loss treatments to reduce visible hair loss, maintain hair density, and give you peace of mind. Topical minoxidil, finasteride, and dutasteride are all viable options for encouraging hair growth. You should discuss with your provider which of these is most appropriate for you, as some may have additional safety concerns.
FAQs
Q: Does Mounjaro Cause Hair Loss?
A: Mounjaro is the brand name for tirzepatide. The data discussed in this article will apply to both Mounjaro and tirzepatide.
Q: Does Zepbound Cause Hair Loss?
A: Zepbound is another brand name for tirzepatide, and so the data discussed in this article can apply to Zepbound as well as tirzepatide.
Q: If I notice hair thinning while taking tirzepatide, what should I do?
A: You should monitor your hair shedding and speak to your doctor. You may be able to start on hair loss treatments alongside tirzepatide to reduce hair loss.
Q: If I lose weight quickly, will I experience hair loss?
Tirzepatide often causes rapid weight loss, potentially even more dramatic than that seen with Ozempic. Rapid weight loss may result in telogen effluvium and temporary hair shedding.
Final Thoughts
Tirzepatide and other GLP-1 RAs provide significant benefits for weight loss and type 2 diabetes treatment, but concerns about side effects – including hair loss – are still under investigation. The evidence so far does not prove a direct causal link between tirzepatide and hair loss, but there is a degree of evidence supporting the association, particularly in those genetically predisposed to male pattern hair loss.
Shedding may be temporary and linked to rapid weight loss-induced telogen effluvium; the extreme weight loss seen on tirzepatide treatment compared to other GLP-1 RAs may further implicate it in this mechanism of hair loss. Nutrient deficiencies and the natural progression of AGA are also likely mechanisms.
More long-term research into the side effects of tirzepatine is needed for definite conclusions to be drawn, but for the time being, the benefits of tirzepatide appear to outweigh the potential risk of hair loss.
Female hair loss remains a widely misunderstood and often under-treated condition, affecting nearly one-third of all women at some point in their lives and up to two-thirds after menopause. Unlike male pattern hair loss, research and treatment options for women have historically lagged, resulting in limited specialized solutions and significant emotional distress for those afflicted.
Minoxidil stands as the only FDA-approved medication for female pattern hair loss. Its efficacy is supported by robust data, particularly at the 2 and 5% concentrations for women. In this guide, we will showcase the six best minoxidil products for women, including the best overall, best value, and top specialized choices.
Quick Look: Top 6 Minoxidil Brands for Women 2026
Product Strength Format Customization Price Best Ulo Women’s Rx Minoxidil 7% Solution High $41.65 Overall Musely 8% Solution High $99 Strength Rogaine Women’s Foam 5% Foam None $49.97 Sensitivity Hers 2%-5% Solution/Foam None $30 Value Happy Head (Women’s Formula) 6% Solution High $79 Alternative Winona 7% Solution None $150 Woman-centered care Before we get into our list, let’s first take a look at what female pattern hair loss is and how minoxidil works for women.
[ulo_promo title=”Interested in Topical Minoxidil?” subtitle=”High-strength topical minoxidil available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-minoxidil?variant=42247221313615″ prescription=”true” type=”topical” ]
What is Female Pattern Hair Loss?
Female pattern hair loss (FPHL) is a chronic, non-scarring alopecia where genetically susceptible follicles on the central scalp progressively minaturize, leading to reduced hair density over time. Clinically, women usually show diffuse thinning over the crown and midline part with relative preservation of the frontal hairline rather than “bald patches”.{{Bhat, Y.J., Saqib, N-U., Latif, I., Hassan, I. (2020). Female Pattern Hair Loss – An Update. Indian Dermatology Online Journal. 11(4). 493-501. Available at: https://doi.org/10.4103/idoj.IDOJ_334_19}}
The Ludwig scale grades this pattern from I-III: mild central thinning (I), moderate widening of the part and density loss (II), and advanced, see-through vertex thinning (III). Trichoscopy and histology show increased hair shaft diameter variability and replacement of terminal hairs by finer, vellus-like hairs.{{Kothari, C.R., Shivakumar, P. (2024). Trichoscopic Features in Female Pattern Hair Loss: 1-Year Hospital-Based Cross-Sectional Study. Clinical Dermatology Review. 8(2). 95-101. Available at: https://doi.org/10.4103/cdr.cdr_123_21}}
FPHL arises from a mix of genetics, hormones, low-grade inflammation, oxidative stress, and microvascular and aging-related changes around the follicle. Unlike classic male pattern hair loss, many women have normal serum androgens, suggesting that local androgen sensitivity and non-androgen mechanisms both contribute.{{Ramos, P.M., Miot, H.A. (2015). Female Pattern Hair Loss: a clinical and pathophysiological review. Anais Brasileiros de Dermatologia. 90(4). 529-543. Available at: https://doi.org/10.1590/abd1806-4841.20153370}}
How Minoxidil Works
Minoxidil functions as a potassium channel opener that promotes vasodilation, increasing blood flow and improving microcirculation around hair follicles.{{Hussein, R.S., Dayel, S.B., Abahussein, O., El-Sherbiny, A.A. (2024). Applications and efficacy of minoxidil in dermatology. Skin Health and Disease. 4(6). E472. Available at: https://doi.org/10.1002/ski2.472}}
It is also a prodrug that must be converted by the sulfotransferase enzyme into its active form, minoxidil sulfate. This conversion helps extend the anagen (growth) phase while shortening the telogen (resting) phase, thereby shifting a greater number of follicles into active growth cycles.{{Pietrauszka, K., Bergler-Czop, B. (2020). Sulfotransferase SULT1A1 activity in hair follicle, a prognostic marker of response to the minoxidil treatment in patients with androgenetic alopecia: a review. Advances in Dermatology and Allergology. 39(3). 472-478. Available at: https://doi.org/10.5114/ada.2020.99947}}
Additional evidence indicates that minoxidil stimulates the expression of growth-promoting factors, such as vascular endothelial growth factor (VEGF), and activates the Wnt/β-catenin signaling pathway, both of which further support hair regrowth.{{Gupta, A.K., Talukder, M., Shemer, A., Piraccini, B.M., Tosti, A. (2023). Low-Dose Oral Minoxidil for Alopecia: A Comprehensive Review. Skin Appendage Disorders. 9(6). 423-437. Available at: https://doi.org/10.1159/0000531890}}
While minoxidil does not directly address dihydrotestosterone (DHT), it can enhance the effectiveness of other therapies by targeting different biological pathways involved in hair loss. When used alongside anti-DHT treatments such as finasteride, which reduces the underlying hormonal driver of androgenic alopecia, minoxidil offers a complementary, non-hormonal mechanism of action. Clinical research demonstrates that the combined use of topical finasteride and minoxidil produces greater improvements in hair density in men compared to minoxidil alone.{{Asad, N., Naseer, M., Ghafoor, R. (2024). Efficacy of Topical Finasteride 0.25% with Minoxidil 5% versus Topical Minoxidil 5% Alone in Treatment of Male Pattern Androgenic Alopecia. Journal of Drugs in Dermatology. 23(11). 1003-1008. Available at: https://doi.org/10.36849/JDD.7826}}
Why Women Respond Differently
In women, pattern hair loss is generally less strictly DHT-driven than in men, so microcirculation, oxidative stress, and local inflammatory pathways play a proportionately greater role.{{Fabbrocini, G., Cantelli, M., Masara, A., Annunziata, M.C., Marasca, C., Cacciapuoti, S. (2018). Female pattern hair loss: A clinical, pathophysiologic, and therapeutic review. International Journal of Women’s Dermatology. 4(4). 203-211. Available at: https://doi.org/10.1016/j.ijwd.2018.05.001}} This helps explain why a vasodilatory, pro-anagen agent like minoxidil is often effective even when anti-androgens alone are insufficient.
Hormonal transitions like perimenopause/menopause, thyroid dysfunction, and polycystic ovary syndrome (PCOS) commonly unmask or accelerate FPHL by altering estrogen-androgen balance and cycling dynamics.{{Aksenenko, M., Palkina, N., Komina, A., Ruksha, T. (2019). MiR-92a-1-5p and miR-328-3p Are Up-Regulated in Skin of Female Pattern Hair Loss Patients. Annals of Dermatology. 31(2). 256-259. Available at: https://doi.org/10.5021/ad.2019.31.2.256}}
OTC vs Prescription Minoxidil for Women
Over-the-counter (OTC) minoxidil for women typically comes at 2-5% concentrations, while prescription or compounded products may use 5-8% or higher strengths in customized products.
2% minoxidil is the classic, label-approved strength for women, with clear evidence of a benefit versus placebo.{{van Zuuren, E.J., Fedorowicz, Z., Schoones, J. (2016). Interventions for female pattern hair loss. Cochrane Database of Systematic Reviews. 2016(5). CD007628. Available at: https://doi.org/10.1002/14651858.CD007628.pub4}}
Compounded “high-strength” minoxidil (5-8%+) is prescription only and relies in part on carrier agent formulation.{{Sattur, S.S., Sattur, I.S. (2021). Pharmacological Management of Pattern Hair Loss. Indian Journal of Plastic Surgery. 54(4). 422-434. Available at: https://doi.org/10.1055/s-0041-1739254}} Simply raising the percentage does not guarantee better results and may raise the risk of irritation, hypertrichosis, or systemic absorption of the drug.{{Ghonemy, S., Alarawi, A., Bessar, H. (2021). Efficacy and safety of a new 10% topical minoxidil versus 5% topical minoxidil and placebo in the treatment of male androgenetic alopecia: a trichoscopic evaluation. Journal of Dermatological Treatment. 32(2). 236-241. Available at: https://doi.org/10.1080/09546634.2019.1654070}}
So, with that in mind, let’s take a look at our top six minoxidil brands of 2026.
Best Minoxidil Brands for Women
#1 Best Overall: Ulo Women’s Rx Minoxidil (7%)

Pros: Cons: ✓ Prescription-only 7% minoxidil, higher than standard OTC strengths ✗Prescription products are only available in the USA ✓ Optional evidence-based add-ons ✓ Quality-tested ingredients free of irritants ✓ Includes medical consultation and ongoing monitoring Ulo Women’s Rx Minoxidil+ is our go-to product for topical minoxidil treatment. It is designed for those who want more than “pink-labeled” 2-5% solutions and are comfortable with a prescription approach guided by specialists. The 7% concentrated and layered actives (including cetirizine 1%, tretinoin 0.01%, melatonin 0.01%, and caffeine 0.2%) target multiple facets of hair loss with a level of customization that goes beyond typical off-the-shelf products.
Bottom Line: Ulo offers the most precise, clinically guided minoxidil-based treatment for women in 2026, combining higher-strength therapy with thoughtful formulation and ongoing medical oversight.
#2 Best for Strength: Musely The Hair Topical Solution-Classic

Pros: Cons: ✓ High-strength 8% prescription minoxidil. ✗ Use of corticosteroids increases the risk of skin thinning. ✓ Optional evidence-based add-ons like dutasteride and spironolactone for hormonal control. ✗ Propylene glycol and ethyl alcohol base, which can sting or dry out sensitive scalps. ✓ Additional scalp-supporting actives like tretinoin, ketoconazole, caffeine, and melatonin. ✗ More expensive than simpler OTC or lower-strength prescription options. ✓ Includes periodic medical follow-up. Musely’s 8% “Classic” Hair Topical is designed for women with advanced thinning or those who have plateaued on conventional strengths, combining high-dose minoxidil with potent anti-androgens and supportive ingredients in a single solution, including optional add-ons such as dutasteride 0.3%, spironolactone 0.075%, tretinoin 0.01%, ketoconazole 2%, hydrocortisone 1%, plus adjuncts like caffeine and melatonin.
It functions more as an intensive, prescription-only protocol than a starter product, and is best reserved for users willing to tolerate a stronger propylene glycol/ethyl alcohol vehicle, and possible skin thinning if using long-term due to the addition of corticosteroids.
Bottom line: For women with stubborn, progressive hair loss who have outgrown basic 5% formulas, Musely’s high-strength, multi-active topical offers one of the most powerful at-home options, provided they are comfortable with higher cost and higher irritation risk.
#3 Best for Sensitivity: Rogaine Women’s Foam

Pros: Cons: ✓ Propylene-glycol-free foam vehicle, often better tolerated on sensitive or irritated scalps. ✗No medical consultation or follow-up after buying ✓ Widely available OTC ✗ No customization. Rogaine Women’s Foam is a classic choice for those looking for a gentle-on-the-scalp option of minoxidil. The propylene-glycol-free foam base, robust clinical evidence, and once-daily 5% option make it a gentle yet effective starting point for treating female pattern thinning. It should be noted that if you wanted to try the lower dose option (2%), you need to buy the solution, which contains propylene glycol, and so may not be as beneficial for those with sensitive skin.
Bottom Line: Get the foam if you have a sensitive scalp or are a beginner, wanting a low-irritant minoxidil option.
#4 Best Value: Hers Minoxidil Foam and Solution

Pros: Cons: ✓ Budget-friendly option at around $30 for a 2-month supply. ✗No advanced customization available. ✓ Offers both 2% and 5% strengths at the same price. ✓ Available in solution and foam formats. Hers Minoxidil is designed for women who want a clinically supported minoxidil treatment without paying premium prices for branding or heavy telehealth layering. With standard 2 and 5% options in familiar vehicles, it delivers an approachable, budget-conscious package for those comfortable managing a simple daily routine themselves.
Bottom Line: For cost-conscious women who want an easy, no-frills entry into proven minoxidil therapy, Hers Minoxidil offers standard concentrations with good value.
#5 Best Alternative: Happy Head Minoxidil and Spironolactone for Women

Pros: Cons: ✓ Prescription-strength 6% minoxidil, higher than standard OTC options but below ultra-high-dose protocols. ✗ Uses a propylene glycol-containing vehicle, which can increase irritation, dryness, or stinging on sensitive scalps. ✓ Customizable blends that include spironolactone, tretinoin, and hydrocortisone ✗ Inclusion of topical corticosteroids carries a risk of skin thinning and barrier damage if used long-term. ✓ Strong telehealth model with online prescribing and adjustments to treatments over time. ✗ More expensive than generic 5% minoxidil and some standard telehealth offerings. ✓ Good fit for women who need more than basic 2-5% formulas but do not want to jump straight to 8%+ multi-drug cocktails. Happy Head’s 6% formulas are aimed at women who want a personalized, prescription-only topical that goes beyond standard strengths while still staying below the most aggressive high-dose regimens. By combining minoxidil with spironolactone, retinoic acid, and short-term hydrocortisone in a single bottle, it offers a modular approach that can be tuned to individual tolerance and response rather than a one-size-fits-all solution. It should be noted that Happy Head uses corticosteroids in their topicals to offset the potential irritation from propylene glycol usage. However, this can cause skin thinning with long-term use.
Bottom line: For women who need a tailored, mid-high-strength minoxidil blend with added anti-androgens and supportive ingredients, but prefer not to escalate to ultra-high-dose, steroid-heavy cocktails, Happy Head provides a strong option.
#3 Best for Woman-Centered Care: Winona 7% Minoxidil

Pros: Cons: ✓ Women-focused clinic model that addresses broader menopausal health alongside hair loss. ✗ Uses a propylene glycol-containing vehicle, which can increase irritation, dryness, or stinging on sensitive scalps. ✓ Prescription-strength 7% minoxidil specifically targeted to menopausal and perimenopausal thinning. ✗ No customization ✓ Guided supportive care pathway, with structured programs, check-ins, and follow-up. ✗ Premium pricing at around $150 for a 3-month supply. ✓ Treatment plans that can integrate other menopause therapies where appropriate Winona’s 7% minoxidil is designed for women who want more than a stand-alone bottle and value a structured, woman-centered approach that fits into a broader menopause-care framework. The higher-strength prescription formula, combined with clear guidance, follow-up, and attention to hormonal context, makes it particularly suited to postmenopausal and perimenopausal hair loss rather than general early thinning. However, it should be noted that its carrier agent, propylene glycol, may be irritating for sensitive scalps.
Bottom line: For women seeking a guided, menopause-focused program built around prescription-strength minoxidil, Winona offers a structured, woman-centered care pathway, albeit at a higher price and with a more irritant-prone vehicle.
Regrowth Timeline
Setting realistic expectations is essential when beginning topical minoxidil for female pattern hair loss. Unlike quick cosmetic fixes, minoxidil works by gradually altering the hair growth cycle, and visible changes take time to develop.
Timeframe What to Expect Clinical Evidence Months 0-3 An initial increase in shedding may occur as follicles shift out of the resting (telogen) phase and re-enter growth. This temporary “dread shed” phase typically improves within 4–8 weeks and is considered a normal response to treatment initiation. {{Nohria, A., Desai, D., Sikora, M., Mandal, S., Shapiro, J., Lo Sicco, K. (2024). Combating “dread shed”: The impact of overlapping topical and oral minoxidil on temporary hair shedding during oral minoxidil initiation. JAAD International. 15. 220-224. Available at: https://doi.org/10.1016/j.jdin.2024.03.005}} Months 3-6 Early visible signs of improvement may appear, including reduced shedding and the emergence of fine, new hairs (vellus to terminal transformation), particularly along the part line and crown. {{Amit, K., Mansukh, G., Satyaprakash, M., Dhiraj, D., Hanmant, B. (2023). Real-World Effectiveness, Safety, and Tolerability of Cetosomal Minoxidil 5% Alone and a Fixed Drug Combination of Cetosomal Minoxidil 5% With Finasteride 0.1% in the Management of Androgenetic Alopecia (Inbilt Study). Cureus. 15(7). E41681. Available at: https://doi.org/10.7759/cureus.41681}} Months 6-12 More noticeable cosmetic improvements are typically seen, including increased overall density, thickening of existing strands, and improved scalp coverage in areas of diffuse thinning. For many women, this is the point at which changes become easily visible in the mirror and in photos. {{Katz, H.I., Hien, N.T., Prawer, S.E., Goldman, S.J. (1987). Long-term efficacy of topical minoxidil in male pattern baldness. Journal of the American Academy of Dermatology. 16(3). 711-718. Available at: https://doi.org/10.1016/s0190-9622(87)70092-9}} Months 12+ Hair density gains typically plateau. At this point, continued use is required to maintain results and prevent gradual regression back toward baseline. Stopping treatment may allow thinning to resume over time. {{Katz, H.I., Hien, N.T., Prawer, S.E., Goldman, S.J. (1987). Long-term efficacy of topical minoxidil in male pattern baldness. Journal of the American Academy of Dermatology. 16(3). 711-718. Available at: https://doi.org/10.1016/s0190-9622(87)70092-9}} Why Do I Need to Stay Consistent When Using Minoxidil?
Topical minoxidil works by extending the anagen (growth) phase of the hair cycle and shortening the telogen (resting) phase, thereby increasing the amount of time that follicles spend actively producing hair. Maintaining this effect requires regular, consistent application. When doses are frequently missed, follicles spend less cumulative time in a growth-biased state, which reduces the likelihood of noticeable improvement.{{Messenger, A.G., Rundegren, J. (2004). Minoxidil: mechanisms of action on hair growth. British Journal of Dermatology. 2(1). 186-194. Available at: https://doi.org/https://doi.org/10.1111/j.1365-2133.2004.05785.x}}
This principle is especially important in women, whose hair loss is often more diffuse and gradual, making subtle changes harder to notice in the early months. Because the human scalp hair cycle progresses slowly, with the anagen phase potentially lasting several years, many follicles need prolonged, uninterrupted exposure to minoxidil before visible gains in density and coverage can be achieved.{{Hoover E, Alhajj M, Flores JL. Physiology, Hair. [Updated 2023 Jul 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499948/ (Accessed: November 2025)}}
For this reason, most clinical guidance advises committing to at least six months of daily, consistent use before evaluating the effectiveness of treatment, with continued use required to sustain and build upon results.
What Minoxidil Formulations Are Available?
You can find topical minoxidil in several different delivery vehicles, each with its own advantages in terms of scalp tolerability, ease of use, and fit for a woman’s lifestyle and hair type. In most cases, the “best” option is not defined by pure strength alone, but by how well the formula matches skin sensitivity, styling habits, and consistency of application.
Foam – Best for Sensitive Skin
Propylene glycol–free foam formulations were developed to reduce the risk of contact dermatitis, itching, and dryness that can occur with traditional liquid solutions. Clinical observations suggest that foam is generally better tolerated and faster-drying, making it a strong choice for women with sensitive scalps or those who wash and style their hair frequently.{{Purnak, T., Senel, E., Sahin, C. (2011). Liquid formulation of minoxidil versus its foam formulation. Indian Journal of Dermatology. 56(4). 462. Available at: https://doi.org/10.4103/0019-5154.84714}}
Liquid – Best for Cost and Precision
Classic liquid solutions, usually formulated with alcohol and propylene glycol, remain widely available and affordable. While effective, they may cause itching, dryness, or flaking in some women. These solutions can work well for individuals without scalp sensitivity who prefer a more targeted, dropper-based application, especially along the part line.
Spray – Best for Quick, Even Coverage
Spray or mist-style applicators make it easier to cover larger areas of diffuse thinning, such as along the crown or upper scalp. However, they can be less precise, with some product landing on the hair shafts or surrounding skin rather than directly on the scalp.
Gel – Best for Targeted Areas
Gel or cream-gel formulations tend to stay in place, minimizing runoff and improving control. These are helpful for women treating specific areas of thinning, such as the temples, frontal hairline, or post-partum thinning zones.
Liposomal Delivery
Some prescription and premium products use liposomal or phospholipid-based carriers that are designed to improve follicular penetration while reducing irritation and systemic absorption. These advanced bases may be especially attractive for women who need stronger formulations but have experienced irritation with traditional vehicles.
How Safe is Minoxidil?
Topical minoxidil is generally well tolerated by women, but like any active medication, it can produce local scalp irritation, a brief increase in shedding during the early treatment phase, and, in very rare cases, systemic side effects, particularly in individuals with underlying skin or cardiovascular conditions.
Common local reactions may include:
- Mild itching
- Flaking or dryness
- Redness
- Burning or stinging
- Temporary increase in shedding
These symptoms are typically mild, tend to improve as the scalp adapts, and can often be reduced by switching to a foam-based formula, lowering concentration, or using a gentler vehicle.
Systemic and heart-related reactions are extremely uncommon with proper topical use. However, isolated case reports and safety data recommend seeking medical attention if symptoms such as chest tightness, heart palpitations, lightheadedness, dizziness, or unexplained swelling develop, as these could indicate increased systemic absorption or accidental ingestion. The risk of cardiovascular effects is significantly higher with oral minoxidil or improper dosing, where hypotension, tachycardia, and even heart failure have been reported.{{Tripathee, S., Benyovszky, A., Devbhandari, R., Quiza, K., Boris, J. (2024). A Very Bad Hair Day: Minoxidil Ingestion Causing Shock and Heart Failure. Cureus. 16(8). E66039. Available at: https://doi.org/10.7759/cureus.66039}}
To minimize the risk of side effects, many clinicians recommend starting with once-daily application, gradually increasing only if tolerated. Women with reactive skin often benefit from foam formulations, lower-alcohol bases, or liposomal delivery systems, which can reduce irritation and improve comfort during long-term use.
Individuals with active inflammatory scalp conditions, such as psoriasis, eczema, or severe seborrheic dermatitis, are generally advised to first address the underlying condition before beginning minoxidil therapy. Applying treatment to an inflamed or compromised skin barrier can increase irritation, worsen symptoms, and lead to unpredictable absorption patterns.{{Junge, A., Jic-Hoesli, S.R., Bossart, S., Simon, D., de Viragh, P., Hunger, R.E., Heidemeye, K., Seyed Jafari, S.M. (2025). Contact Dermatitis Caused by Topical Minoxidil: Allergy or Just Irritation. Acta Dermato-Venereologica. 105. 42401. Available at: https://doi.org/10.2340/actadv.v105.42401}}
Although topical minoxidil has lower systemic absorption than oral formulations, it is generally not recommended during pregnancy or while breastfeeding unless specifically advised by a healthcare provider. Women who are pregnant, trying to conceive, or nursing should consult a qualified medical professional to fully review potential risks and alternative treatment options.
Final Verdict
A range of minoxidil-based options is available to support different needs among women experiencing hair thinning, from strength-focused prescriptions to gentle, sensitivity-friendly alternatives and highly customized compounded formulas. While each product relies on the same core ingredient, differences in concentration, delivery vehicle, add-on actives, and level of medical support can significantly influence both tolerability and long-term adherence.
Whichever option you choose, consistent use of minoxidil remains one of the most evidence-backed ways to slow progression and improve hair density in women with pattern hair loss. With today’s expanded access to prescription platforms, foam-based formulations, and individualized treatment models, it is now easier than ever to find an approach that aligns with your scalp sensitivity, stage of hair loss, and lifestyle needs.
Finding the right hair loss treatment can feel overwhelming, and expert guidance is essential to identify the best formula for your needs. The PhD-led team at Perfect Hair Health leverages emerging research and close collaborations with top innovators to provide readers with the most accurate and actionable reviews of hair restoration offerings. Topical finasteride is one of the most sought-after treatments on the market, boasting clinical support, targeted results, and easy application.
This comprehensive guide to the top-rated topical finasteride products is based on extensive research, expert recommendations, and the latest consumer feedback. Whether you’re just beginning your hair health journey or searching for better hair loss solutions, this article provides valuable information on safe and effective treatment options. Our recent partnership with Ulo enhances this guide with privileged insights on clinical findings and state-of-the-art protocols.
Read on for specialized guidance, insightful reviews, and proven recommendations of topical finasteride preparations from today’s leading brands.
[ulo_promo title=”Interested in Topical Finasteride?” subtitle=”Low-dose & full-strength finasteride available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-finasteride?variant=42249746186319″ prescription=”true”]
Quick Look: 5 Best Topical Finasteride Products
Here’s a side-by-side comparison of our top recommended topical finasteride treatments. Read on for more details on each of these excellent products.
Product Price Finasteride % Customization Application Ulo $64+/month 0.005% – 0.2% High Solution Strut Health $59 0.1-0.25% Medium Solution/Gel Happy Head $59-99/month 0.3% Medium Liposomal Gel Roman $50/month 0.3% Low Spray Hims $35+/month 0.3% Low Spray Topical Finasteride: What It Is & Why It’s Better
First, we will briefly explore the science behind topical finasteride, including its mechanism of action in treating hair loss and the advantages of topical formulations.
What Is Topical Finasteride?
Topical finasteride is a clinically proven treatment for androgenic alopecia (AGA), a type of hair loss that affects more than 50% of men by the age of 50.{{Jang, W.S., Son, I.P., Yeo, I.K., Park, K.Y., Li, K., Kim, B.J., Seo, S.J., Kim, M.N., Hong, C.K. (2013). The Annual Changes of Clinical Manifestation of Androgenetic Alopecia Clinic in Korean Males and Females: A Outpatient-Based Study. Annals of Dermatology. 25(2). 181-188. Available at: https://doi.org/10.5021/ad.2013.25.2.181}} AGA is caused by dihydrotestosterone (DHT), a testosterone-derived hormone that damages hair follicles, causing them to shrink and produce thinner hair. Finasteride reduces DHT levels by inhibiting the enzyme 5-alpha-reductase, protecting the hair follicles to stop hair loss and encourage new growth.{{Duran, R, C-D., Martinez-Ledesma, E., Garcia-Garcia, M., Gauzin, D.B., Sarro-Ramirez, A., Gonzalez-Carillo, C., Rodriguez-Sardin, D., Fuentes, A., Cardenas-Lopez. (2024). The Biology and Genomics of Human Hair Follicles: A Focus on Androgenetic Alopecia. International Journal of Molecular Sciences. 25(5). 2542. Available at: https://doi.org/10.3390/ijms25052542}}
While orally administered finasteride has been in use since 1997, topical formulations are a relatively new development. When applied to the scalp, finasteride provides targeted treatment with a reduced risk of systemic side effects associated with oral preparations. Topical finasteride is shown to reduce DHT levels on the scalp for greater hair count and density with comparable effectiveness to oral finasteride.{{Lee, S.W, Juhasz, M., Mobasher, P., Ekelem, C., Mesinkovska, N.A. (2018). A Systematic Review of Topical Finasteride in the Treatment of Androgenetic Alopecia in Men and Women. Journal of Drugs in Dermatology. 17(4). 457-463. Available at: PMID: 29601622}}
Numerous studies confirm that topical finasteride slows and reverses hair loss by boosting hair thickness, density, and growth cycles. These results are enhanced when combined with other topical treatments like minoxidil. Due to minimal systemic absorption and attendant side effects, topical formulas are considered a safer choice for prolonged use. Overall, topical finasteride is prized among clinicians and patients as a safe, effective, and convenient solution to pattern hair loss.{{Lee, S.W, Juhasz, M., Mobasher, P., Ekelem, C., Mesinkovska, N.A. (2018). A Systematic Review of Topical Finasteride in the Treatment of Androgenetic Alopecia in Men and Women. Journal of Drugs in Dermatology. 17(4). 457-463. Available at: PMID: 29601622}},{{Piraccini, B.M., Blume-Peytavi, U., Scarci, F., Jansat, J.M., Falques, M., Otero, R., Tamarit, M.L., Galvan, J., Tebbs, V., Massana, E. (2021). Efficacy and safety of topical finasteride spray solution for male androgenetic alopecia: a phase III, randomized, controlled clinical trial. Journal of the European Academy of Dermatology and Venereology. 36(2). 286-294. Available at: https://doi.org/10.1111/jdv.17738}}
Why Choose Topical Over Oral?
Because topical finasteride is applied directly to the scalp, it offers localized therapy and avoids the side effects associated with oral finasteride’s systemic exposure. Here is a brief overview of this and other primary advantages of topical formulas:
- Better Safety Profile: Oral finasteride is absorbed into the bloodstream and can have global side effects like sexual dysfunction, hormone disruption, and mood swings. In contrast, topical formulas target the scalp directly and minimally affect plasma levels. Topicals are consistently shown to have fewer systemic side effects. If present, side effects tend to be mild and temporary, such as scalp irritation.
- Individualized Dosing: While the oral finasteride dose is a standardized 1 mg, topical formulas enable tailored dosages and greater precision through potency titration. This is especially important given the dose-dependent outcomes of finasteride treatment. The finasteride concentration in topicals can range from a maintenance dose of 0.005% to a more aggressive protocol of 2.5%.
- Greater Customization: Topical formulas often combine other proven treatments, such as tretinoin, minoxidil, and caffeine. Studies demonstrate that finasteride-minoxidil combinations deliver superior results compared to single-agent treatments. Plus, the range of available delivery methods (e.g., solutions, sprays, gels) can improve convenience, satisfaction, and adherence.
- Long-Term Use: With a better safety profile and lower systemic impact, topical finasteride is more suitable for prolonged use, which is often necessary to maintain the benefits of hair loss treatment.
In short, research data indicate that topical finasteride yields comparable results with a more favorable safety profile than oral finasteride, making it a better option for long-term treatment. Further benefits of topical formulations include greater dose precision, synergistic adjuvants like minoxidil, and a range of delivery methods to support compliance.{{Lee, S.W, Juhasz, M., Mobasher, P., Ekelem, C., Mesinkovska, N.A. (2018). A Systematic Review of Topical Finasteride in the Treatment of Androgenetic Alopecia in Men and Women. Journal of Drugs in Dermatology. 17(4). 457-463. Available at: PMID: 29601622}},{{Piraccini, B.M., Blume-Peytavi, U., Scarci, F., Jansat, J.M., Falques, M., Otero, R., Tamarit, M.L., Galvan, J., Tebbs, V., Massana, E. (2021). Efficacy and safety of topical finasteride spray solution for male androgenetic alopecia: a phase III, randomized, controlled clinical trial. Journal of the European Academy of Dermatology and Venereology. 36(2). 286-294. Available at: https://doi.org/10.1111/jdv.17738}}
Evaluation Criteria: What Makes the Best?
When selecting the best topical finasteride products, we adhered to the following evaluation criteria, which are thoroughly supported by clinical findings and customer feedback.{{Piraccini, B.M., Blume-Peytavi, U., Scarci, F., Jansat, J.M., Falques, M., Otero, R., Tamarit, M.L., Galvan, J., Tebbs, V., Massana, E. (2021). Efficacy and safety of topical finasteride spray solution for male androgenetic alopecia: a phase III, randomized, controlled clinical trial. Journal of the European Academy of Dermatology and Venereology. 36(2). 286-294. Available at: https://doi.org/10.1111/jdv.17738}},{{Suchonwanit, P., Iamsumang, W., Leerunyakul, K. (2020). Topical finasteride for the treatment of male androgenetic alopecia and female pattern hair loss: a review of the current literature. Journal of Dermatological Treatment, 33(2), 643–648. Available at: https://doi.org/10.1080/09546634.2020.1782324}}
✓ Effectiveness
We assessed scientific data, DHT decrease rates, and real-world testimonies of hair count increases. The top products deliver measurable results in 3-6 months with continuous improvements in hair density throughout the first year and beyond.
✓ Safety
Because finasteride is a prescription-only treatment, we verified that providers adhere to all safety regulations, including proper prescribing and monitoring protocols. Leading suppliers also provide full ingredient transparency to help assess potential side effects.
✓ Customization
Premium brands offer treatment customization options tailored to patients’ needs and preferences, maximizing outcomes beyond those achieved with traditional, standardized approaches. These include concentration adjustments, synergistic add-on ingredients such as minoxidil, and various delivery methods.
✓ Convenience
Successful treatment outcomes depend on long-term compliance and a positive user experience. Factors such as ease of application, clear instructions, manageable dose frequency, and responsive support help ensure uninterrupted treatment.
✓ Value
The best providers balance superior quality with transparent and affordable pricing models that cover doctor consultations, prescriptions, and follow-up care. These are especially important concerns in the telehealth landscape, where many subpar platforms employ opaque billing practices to stack on hidden fees and unexpected charges.
How to Choose the Right Product for Your Needs
When choosing the product that best meets your hair loss treatment needs, consider the extent of your hair loss and treatment aims, such as basic upkeep or intensive restoration. Also account for your preferred delivery method (i.e., gel, solution, or spray), desired add-ons, medical support requirements, and budget.
Reviewing the Best Topical Finasteride Products
With the above key factors in mind, let’s turn now to our top recommended options that each offer unique advantages sure to satisfy.
#1: Ulo Finasteride + Minoxidil Plus Rx

Pros: Cons: ✓ Clinically-proven combination therapy ✗ Prescription products are only available in the USA ✓ True personalization with custom concentrations and medical consultations ✓ PhD-scientist formulated ✓ Ongoing medical monitoring and a user-friendly platform ✓ Quality-tested ingredients free of irritants Ulo’s combination formula of high-strength finasteride with prescription-grade minoxidil takes the top spot, reflecting the platform’s commitment to providing safe, scientifically proven hair loss treatments tailored to meet individual needs. Every Ulo product is developed by a team of PhD scientists who deliver innovative interventions in hair restoration.
Their advanced finasteride and minoxidil solution blocks DHT and stimulates new growth in a targeted dual treatment that is proven superior to monotherapies in clinical trials. Ulo’s finasteride formulas are uniquely customizable and available in different concentrations (0.005% for maintenance and 0.2% for stronger protocols), with a series of synergistic add-ons like caffeine to boost circulation, tretinoin for better absorption, and melatonin for antioxidant protection.
The deluxe treatment begins at $64 per month, which includes an onboarding medical consultation to assess each client’s needs, a physician-crafted treatment plan, and continued dermatologist oversight. All Ulo products are strictly sourced from pharmacies that adhere to safety and quality regulations. The clinic’s licensed dermatologists provide customized treatment regimens with free home prescription deliveries and ongoing support.
Bottom Line: Ulo’s individualized hybrid treatment is the ultimate in advanced hair restoration technology. With precise formulation and continuous medical supervision, this tailored solution delivers exceptional results for a low monthly subscription fee starting at $64. Ulo’s guiding dedication to safety and efficacy makes this full-service platform the best option for those who are serious about combating hair loss.
#2 Strut Finasteride Hair Loss Formula

Pros: Cons: ✓ Custom-compounded topical finasteride formulas (with optional add-ons) ✗ Not available internationally, and currently cannot ship to Arkansas ✓ Online consult and prescriptions from U.S. board-certified physicians ✗ Auto-refills by default; some reviews report difficulty canceling and customer service gaps ✓ Multiple formulation options (gel or solution; adjustable finasteride strength) ✓ Convenient telehealth model with free, discreet shipping in most U.S. states. Strut Health is a U.S.-based telehealth provider offering customized topical finasteride for AGA. After an online questionnaire and photo-based evaluation, a board-certified clinician designs a compounded formula that may contain finasteride alone or in combination with other actives like minoxidil, tretinoin, fluocinolone, or biotin. The company’s finasteride hair-loss formulas typically use 0.1-0.25% topical finasteride, with optional minoxidil concentrations up to 7.5% and tretinoin in a gel or solution base, giving flexibility to tailor potency and tolerability.
Our in-house lab testing showed that Strut Health’s finasteride product contained the correct concentrations of ingredients (finasteride, minoxidil, and tretinoin), indicating that they can be trusted to provide a quality product.
However, there are trade-offs. Strut does not accept insurance, and pricing for topical finasteride (often around the mid-range of the telehealth market) may add up for long-term use. The company currently ships to nearly all U.S. states but cannot ship to Arkansas, and there is no international service. Public reviews highlight convenience for many users but also recurring concerns about auto-refills and difficulty canceling, as well as frustration with customer support responsiveness and refund policies.
Bottom Line: Strut Health’s topical finasteride offers a flexible, telehealth-delivered alternative for patients who want DHT-targeted treatment without taking a daily pill, with customizable formulas that can include or exclude minoxidil and other actives. Its convenience, physician oversight, and compounding flexibility are strong advantages, but subscription-based pricing and mixed customer service reviews may give more budget-conscious patients pause.
#3 Happy Head Topical Super Solution: Finasteride, Minoxidil & Liposomal

Pros: Cons: ✓ Medical oversight by board-certified dermatologists ✗ Price rises from $59 to $99 after the first six months ✓ Higher concentrations of 0.3% finasteride + 8% minoxidil ✗ Higher concentrations may increase side effect risk ✓ Made with a delayed-release liposomal base ✗ Gel formula cannot be customized ✓ User-friendly platform and follow-up care ✗ May irritate sensitive skin ✓ Affiliate programs available ✗ Possible shipping and customer service concerns Our next selection is from Happy Head, known for unique formulations and dermatologist oversight. The Topical Super Solution features a more concentrated combination of 0.3% finasteride with 8% minoxidil for targeted hair restoration.
Available in a mess-free pump dispenser, this gel is made with the brand’s proprietary liposomal delivery base that boosts scalp penetration with timed medication release and once-daily application. This helps minimize bloodstream absorption, reducing potential side effects, and is a notable safety feature for higher finasteride doses. That said, some ingredients in the carrier base should not be used on sensitive skin. Other products from the brand are more customizable and can be adapted to sensitive skin.
The starting price of Happy Head’s treatment is competitive at $59 for a monthly subscription that covers dermatologist oversight and prescription deliveries. However, the price increases to $99 after the first six months. Some reviews cite a lack of transparency regarding potential side effects, as well as intermittent shipping delays and inconsistent customer service.
Bottom Line: Happy Head’s potent dual therapy is a useful option for patients with intermediate to severe hair loss and normal skin. The delayed-release gel base increases medication absorption for more targeted treatment while decreasing systemic side effects and requires application only once a day. Advantages include dermatologist support and attractive pricing, but patients should be aware of reviews citing shipping and customer service issues.
#4: Roman (Ro) Hair Solution Rx

Pros: Cons: ✓ Transparent and competitive price of $50 per month ✗ Contains potential irritants not suitable for sensitive skin ✓ High finasteride concentration (0.3%) for aggressive treatment ✗ High fixed concentration with a greater risk of side effects ✓ Includes minoxidil and tretinoin for synergistic effects ✗ Limited customization options ✓ Convenient once-daily application ✗ Standard delivery system lacks advanced features ✓ Established telehealth provider with medical supervision Roman offers a simple topical finasteride formula designed for convenient, once-daily use and focused intervention. The spray contains three active ingredients: high-dose 0.3% finasteride with 6% minoxidil and tretinoin to enhance absorption. This product delivers a potent dose of finasteride on par with premium rivals through a no-frills spray system.
While tretinoin may improve minoxidil absorption, Roman’s spray has some drawbacks for users with sensitive skin or systemic side effect concerns. The 0.3% finasteride concentration cannot be tailored to individual response, and the standard delivery system does not have delayed-release technology to offset the risk of systemic absorption as seen in Happy Head’s liposomal gel. Inactive ingredients like ethyl alcohol and propylene glycol are also known irritants.
Roman is an accessible option for many users. The transparent and fixed monthly fee of $50 covers doctor consultations, prescription deliveries, and unlimited follow-ups. However, users with sensitive skin or more complex treatment needs may find Roman’s standardized and less gentle formulation to be unsuitable for long-term compliance.
Bottom Line: Roman offers a potent and affordable dual finasteride therapy with telehealth support features. Although it is not customizable like leading alternatives, this spray is a convenient choice for individuals with moderate to severe hair loss who can tolerate high dosages and potential irritants.
#5: Hims Topical Finasteride & Minoxidil Spray

Pros: Cons: ✓ Lowest starting rate of $35+/month ✗ Standardized approach that lacks customization ✓ Well-known brand with recognized platform ✗ Minimal ongoing medical support ✓ Simple ordering process and rapid shipping ✗ Contains irritants not suitable for sensitive skin and fixed high dose ✓ No lengthy consultations required ✗ Basic telehealth features without specialist care ✓ High-dose dual treatment ✗ Concerns about the price transparency of subscription tiers Hims is a well-known brand that offers topical finasteride through its streamlined telemedicine platform. Their fixed-dose spray of 0.3% finasteride and 6% minoxidil is a convenient and affordable option without the customization features of premium competitors, appealing to those who value simplicity over tailored care.
Like similar high-dose sprays, this standardized formula from Hims is not suitable for patients with sensitive skin, complex treatment needs, or those requiring a lower maintenance dose.
This provider’s appeal is its wide accessibility. With low prices starting at just $35 per month, quick doctor consultations, and shipping in all 50 states, Hims is a gateway brand for many new hair loss patients. However, this entry-level approach lacks the treatment personalization and close medical supervision of established specialty providers.
Bottom Line: Hims’ topical finasteride spray is an affordable and easily accessible option backed by a recognized brand name. Although Hims fails to offer the precision treatment and close medical oversight of premium alternatives, it is a mainstay for patients who prioritize low costs and convenience.
Final Verdict: Our Topical Finasteride Picks
After a comprehensive evaluation, Ulo emerges as our top choice for topical finasteride in 2026. Their genuine customization, science-backed formulations, and ongoing dermatologist supervision set the gold standard for personalized hair restoration.
While competitors offer standardized protocols or unproven technologies, Ulo delivers verified results through precision medicine tailored to individual needs. For patients seeking the highest quality care, Ulo’s scientific rigor and safety-first approach make it the clear winner.
What to Expect: Timeline and Results
Realistic treatment expectations facilitate long-term compliance and successful outcomes. Medical research has established the following evidence-based benchmarks of expected improvements with topical finasteride use as prescribed to treat androgenetic alopecia.
Clinical Timeline for Topical Finasteride Results
Timeframe What to Expect Clinical Evidence 3 Months Terminal hair count starts to improve; increases in total hair count may not yet be observable {{B. Piraccini et al. (2021). Efficacy and safety of topical finasteride spray solution for male androgenetic alopecia: a phase III, randomized, controlled clinical trial. Journal of the European Academy of Dermatology and Venereology, 36: 286 – 294. https://doi.org/10.1111/jdv.17738}},{{Cheng Zhou et al. (2025). Efficacy and safety of topical finasteride spray solution in the treatment of Chinese men with androgenetic alopecia: A phase III, multicenter, randomized, double-blind, placebo-controlled study. Chinese medical journal. Available at: https://doi.org/10.1097/CM9.0000000000003495}} 6 Months Noteworthy increases in hair counts (total and terminal); visible increase in vertex hair growth {{B. Piraccini et al. (2021). Efficacy and safety of topical finasteride spray solution for male androgenetic alopecia: a phase III, randomized, controlled clinical trial. Journal of the European Academy of Dermatology and Venereology, 36: 286 – 294. https://doi.org/10.1111/jdv.17738}},{{Cheng Zhou et al. (2025). Efficacy and safety of topical finasteride spray solution in the treatment of Chinese men with androgenetic alopecia: A phase III, multicenter, randomized, double-blind, placebo-controlled study. Chinese medical journal. Available at: https://doi.org/10.1097/CM9.0000000000003495}},{{A. Rossi et al. (2020). Efficacy of Topical Finasteride 0.5% vs 17α-Estradiol 0.05% in the Treatment of Postmenopausal Female Pattern Hair Loss: A Retrospective, Single-Blind Study of 119 Patients. Dermatology Practical & Conceptual, 10 (2020). https://doi.org/10.5826/dpc.1002a39}} 12-18 Months Maximum improvement is typically observed; continuous improvements in hair coverage and density {{A. Rossi et al. (2020). Efficacy of Topical Finasteride 0.5% vs 17α-Estradiol 0.05% in the Treatment of Postmenopausal Female Pattern Hair Loss: A Retrospective, Single-Blind Study of 119 Patients. Dermatology Practical & Conceptual, 10 (2020). https://doi.org/10.5826/dpc.1002a39}} - Early Treatment Phase (Months 1-3): During early treatment, visible changes are minimal, which may be disappointing for new patients. The therapy begins to suppress scalp DHT levels, creating shifts that are not yet cosmetically evident. Studies show that improvements in terminal hair count begin around 3 months, though total hair count is not yet typically impacted.
In the first 6-8 weeks, some experience a temporary increase in shedding as finasteride prompts new growth cycles to start. This is expected and is an encouraging indication that the treatment is taking effect.
- Visible Improvement Phase (Months 3-6): Visible results begin to appear during this period. Studies show notable increases in hair counts and density by 6 months. Patients tend to note particular improvements in the crown or vertex region.
- Optimization Phase (Months 6-18): The most significant benefits occur during this phase. Research indicates that maximum improvements arise around 12 months of continued treatment, as hair density and new growth quality increase.
- Long-Term Maintenance: According to clinical data, benefits stabilize around 18-24 months, and treatment transitions from active regrowth to maintenance. Because treatment cessation can lead to the gradual return of hair loss within 6-12 months, continued daily compliance is essential to maintain long-term therapeutic outcomes.
Topical Delivery Formats
There are several different topical finasteride delivery formats that each offer unique advantages to suit individual needs and preferences, as follows:
- Solutions are liquid formulas typically applied using a dropper for targeted administration on desired scalp areas. These lightweight preparations are valued for their excellent absorption and residue-free finish. Because solutions may contain irritating excipients such as propylene glycol, sensitive patients should opt for gentle blends like Ulo’s prescription topicals.
- Sprays are a lighter, more fluid type of solution applied using an aerosol or pump. This form enables misting over larger or difficult-to-reach scalp areas. However, sprays are not as precise as droppers, as the liquid may run off and fail to effectively reach the hair follicles.
- Gels offer a more controlled application with a thicker consistency than solutions. They often include advanced delivery bases such as liposome carriers with delayed-release technology, designed to enhance penetration and reduce systemic absorption. However, customization options are typically limited due to compounding practices. Additionally, gel formulas can leave a sticky residue that some users find undesirable.
- Foams may be beneficial for patients with sensitive skin, as they dry quickly and generally lack harsh additives. However, their capacity for targeted application is limited compared to other formulations.
- Creams and lotions are appropriate for sensitive or dry scalps, featuring thick, emollient-laden bases with moisturizing benefits. Lotions are generally faster-absorbing, more spreadable, and lighter than creams.
The best formulation choice depends on hair and skin type, lifestyle, and personal preferences. Patients are encouraged to consult a doctor to determine the ideal format for their individual needs.
Safety and Side Effects
Topical finasteride is noted for its favorable safety profile, especially in contrast to oral formulations; however, understanding potential risks and proper monitoring practices is recommended.
- Common Mild Side Effects: The most common side effects are transient and mild scalp irritation or dryness. Though these reactions often resolve on their own, they also respond well to dose adjustment or calming adjunctive treatments. Patients with sensitive skin should avoid formulas containing irritants like propylene glycol or parabens.{{Lee, S.W, Juhasz, M., Mobasher, P., Ekelem, C., Mesinkovska, N.A. (2018). A Systematic Review of Topical Finasteride in the Treatment of Androgenetic Alopecia in Men and Women. Journal of Drugs in Dermatology. 17(4). 457-463. Available at: PMID: 29601622}},{{Piraccini, B.M., Blume-Peytavi, U., Scarci, F., Jansat, J.M., Falques, M., Otero, R., Tamarit, M.L., Galvan, J., Tebbs, V., Massana, E. (2021). Efficacy and safety of topical finasteride spray solution for male androgenetic alopecia: a phase III, randomized, controlled clinical trial. Journal of the European Academy of Dermatology and Venereology. 36(2). 286-294. Available at: https://doi.org/10.1111/jdv.17738}}
- When to Contact Your Doctor: More serious side effects or reactions are rare but possible and require prompt medical intervention. These include severe scalp irritation, allergic reactions (blistering, swelling, and redness), and systemic effects like mood changes, sexual dysfunction, or gynecomastia.{{Suchonwanit, P., Iamsumang, W., Leerunyakul, K. (2020). Topical finasteride for the treatment of male androgenetic alopecia and female pattern hair loss: a review of the current literature. Journal of Dermatological Treatment, 33(2), 643–648. Available at: https://doi.org/10.1080/09546634.2020.1782324}},{{Cheng Zhou et al. (2025). Efficacy and safety of topical finasteride spray solution in the treatment of Chinese men with androgenetic alopecia: A phase III, multicenter, randomized, double-blind, placebo-controlled study. Chinese medical journal. Available at: https://doi.org/10.1097/CM9.0000000000003495}}
- Topical vs. Oral Finasteride Safety: Clinical data show that topical finasteride has a significantly lower risk of sexual side effects, typically less than 2% compared to 8-15% with oral formulations. This is attributed to the targeted delivery of topical preparations that limit systemic exposure while providing localized scalp treatment.{{Mysore, V. (2012). Finasteride and sexual side effects. Indian Dermatology Online Journal, 3(1), 62. https://doi.org/10.4103/2229-5178.93496.}}
- Who Should Avoid Topical Finasteride: Topical finasteride is not suitable for women who are pregnant or nursing due to the risk of birth defects or infant harm. Additionally, individuals with known sensitivity, scalp infections, or certain autoimmune diseases may be ineligible for use. Consult with a doctor before beginning treatment.
Closing Thoughts
Topical finasteride is an important development in hair loss therapeutics, providing comparable results with a superior safety profile to oral medications. In today’s market, Ulo’s individualized, clinically rigorous approach sets a benchmark for comprehensive care, outperforming competitors primarily focused on budget or convenience factors.
Successful treatment with topical finasteride requires patience and persistence. Advances in hair restoration technology suggest that tailored medicine, rather than standardized approaches, represents the future. Ready to begin your own journey toward hair restoration?
Visit Ulo today to see how customized topical finasteride can enhance your results.
Frequently Asked Questions
Do I need a prescription for topical finasteride?
Yes, topical finasteride is a prescription-only medication in the USA. This ensures proper diagnosis, medical supervision, dosage, and quality control. Reputable telehealth providers like Ulo make the prescription process quick and easy via video consultations with licensed doctors specialized in hair restoration therapies. These elite platforms also offer ongoing medical supervision to monitor side effects and adjust treatment for optimization.
Avoid online platforms that market finasteride products without a prescription or those that fail to perform a proper medical consultation before prescribing treatment. Reputable platforms employ board-certified doctors licensed to practice in your state of residence with credentials clearly displayed or offered upon request. Sourcing topical finasteride products from unauthorized vendors without a prescription risks hazardous side effects and ineffectiveness.
Can topical finasteride be used with other hair loss treatments?
Yes, topical finasteride can be beneficially combined with treatments like minoxidil, a popular additive in many available products. These formulas often pair finasteride with additional synergistic ingredients such as antioxidants, vasodilators, antifungals, and absorption enhancers.
Topical finasteride can also be safely used in conjunction with most non-prescription hair products, hair transplants, and low-level laser treatments. However, it should not be combined with oral DHT blockers (i.e., oral finasteride or dutasteride) due to the risk of systemic side effects. Medical approval is necessary before starting new treatments.
When will I see results with topical finasteride?
Most patients report stabilization of hair loss after 3-4 months, with notable regrowth in 6-12 months. Shedding within the first 6-8 weeks of starting treatment is considered normal and indicative of the treatment’s efficacy. Because DHT suppression takes time to significantly impact hair growth cycles, consistency and patience are essential for optimal treatment outcomes.
Treatment outcomes can vary between individuals. Consult a doctor to discuss influencing factors and form realistic treatment expectations. This grounded approach facilitates better long-term adherence and more desirable results.
Is topical finasteride suitable for women?
Although the FDA has not yet authorized topical finasteride to treat AGA in women, it is occasionally prescribed for off-label use in postmenopausal patients with female pattern hair loss (FPHL). Because topical finasteride risks fewer hormonal adverse effects than oral finasteride, it is considered a safer option in these cases.
However, women of reproductive age are often recommended to completely avoid finasteride due to the risk of severe birth defects from exposure while pregnant. Non-pregnant women who may plan for pregnancy in the future should abstain from finasteride use unless under strict medical supervision with suitable contraception established. Newer low-dose formulations designed for women show promise, although more study is needed to verify long-term viability.
Ultimately, women considering finasteride therapy should speak with an experienced clinician to go over their medical history, weigh the benefits and risks, and review alternative treatment options, such as FDA-approved topical minoxidil.
What is the cost of topical finasteride without insurance?
The average monthly cost of topical finasteride without insurance can vary from $35 to $90, depending on the source, formulation, and services rendered. Direct-pay telehealth providers tend to offer lower rates than conventional in-person dermatology clinics with combined pharmacy fees. Bespoke formulas with advanced excipients can command higher prices. Patients should account for continued costs to budget for long-term treatment, which is often required for beneficial outcomes.
What will happen if I stop using topical finasteride?
If regular topical finasteride treatment is discontinued, hair loss is expected to return gradually within 2-3 months of cessation. Most patients report a rebound to their baseline hair loss level within 6-12 months. Because this regression is gradual, patients have some flexibility regarding therapy breaks or medication transitions if needed.
Does topical finasteride have any drug interactions?
Compared to oral finasteride, topical formulations have few contraindications due to lower systemic absorption rates. For your safety, inform your prescribing doctor of all current medications, especially blood thinners and other hormonal drugs. While topical finasteride is often safely combined with common medications, there may be exclusions.
How do I store topical finasteride?
Topical finasteride should be kept at room temperature out of direct light, moisture, and heat. With proper storage, most products maintain stability for 12-24 months. While refrigeration isn’t required, it may boost shelf life in temperate climates. Be sure to check expiration dates and safely dispose of expired products.
Can I travel while on topical finasteride?
Yes, prescribed topical finasteride may be stored in carry-on luggage during domestic travel. When traveling internationally, it is recommended to bring the original prescription and label. Be mindful of TSA restrictions on liquid volumes over 3.4 oz.
How is topical finasteride applied?
Topical finasteride is applied directly to a clean and dry scalp with the product applicator. While specific instructions vary with delivery method, in general, the hair should be parted to expose the scalp and allow targeted application to the desired areas. Patients should consult product instructions for precise indications and dosing protocols. Avoid wetting hair for several hours after application, and thoroughly wash hands after use.
Millions worldwide experience hair loss, with androgenic alopecia (AGA) as the leading cause. Also known as male- or female-pattern hair loss, AGA becomes more prevalent with age. It affects a majority of men over the age of 50 and a substantial number of postmenopausal women. Hair thinning and balding due to AGA is not just a cosmetic concern but can significantly detract from self-esteem and overall quality of life.
Among popular hair restoration treatments, topical dutasteride is a breakthrough solution to the serious side effects and plateaued results many experience. This potent DHT blocker offers more targeted therapeutic benefits with minimal systemic exposure and reduced risk. However, not all topical dutasteride products meet quality standards, so specialized guidance is key to selecting the right formula.
The PhD-directed board of experts at Perfect Hair Health draws from the latest clinical data and verified customer feedback to deliver this comprehensive guide to the best topical dutasteride products available in 2026. Through our research collaboration with leading innovators in the field, including our partnership with Ulo, we provide unique insights into the most advanced hair restoration protocols.
Read on for our detailed analysis and evidence-based product recommendations.
[ulo_promo title=”Interested in Topical Dutasteride?” subtitle=”Hair gains bigger than finasteride? Dutasteride makes this possible, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-dutasteride?variant=42249748349007″ prescription=”true” type=”topical” ]
Quick View: 8 Best Topical Dutasteride Products
Here’s a brief comparison of our most highly recommended topical dutasteride products. Continue reading for in-depth reviews.
Product Price Dutasteride % Delivery Method Key Feature Ulo $84+/month 0.02%-0.2% Solution PhD-developed extensive customization XYON Health $129+/month 2% Gel Patented controlled-release technology Strut Health $69/month Up to 0.1% Gel Alcohol-free and customizable Blends ~$45/month (90-day supply) 0.3% Gel Proprietary hydrating formula Happy Head $59-89+/month Up to 0.3% Solution Potency and customization Maximus $54.99 0.1% Gel Customizability, including the addition of antihistamines Miiskin $30-59 + Rx cost Variable, custom Solution No subscription required Musely $33/month 0.3% Solution Lowest cost option Science and Benefits of Topical Dutasteride
To begin, we will briefly explore the scientific background of topical dutasteride, including how it works to treat AGA and the distinct benefits of topical preparations.
Mechanism of Action
Topical dutasteride is valued as a breakthrough treatment for AGA due to its powerful and targeted effects on the molecular levels of hair loss. The root cause of AGA is the testosterone-derived hormone dihydrotestosterone (DHT), which adheres to hair follicles and leads to follicular degeneration and hair loss over time. Dutasteride is classified as a DHT blocker, reducing DHT levels on the scalp to combat hair loss.{{R. Cuevas-Díaz Durán., Martinez-Ledesma, E., Garcia-Garcia, M., Gauzin, D.B., Sarro-Ramirez, A., Gonzalez-Carrillo, C., Rodriguez-Sardin, D., Fuentes, A., Cardenas-Lopez, A. (2024) The Biology and Genomics of Human Hair Follicles: A Focus on Androgenetic Alopecia. International Journal of Molecular Sciences, 25. Available at: https://doi.org/10.3390/ijms25052542.}},{{Dhurat, R., Sharma, A., Rudnicka, L., Kroumpouzos, G., Kassir, M., Galadari, H., Wollina, U., Lotti, T., Golubović, M., Binic, I., Grabbe, S., & Goldust, M. (2020). 5‐Alpha reductase inhibitors in androgenetic alopecia: Shifting paradigms, current concepts, comparative efficacy, and safety. Dermatologic Therapy, 33. Available at: https://doi.org/10.1111/dth.13379.}}
Among DHT-blocking treatments, dutasteride is considered the most potent due to its dual enzyme activity. Testosterone is converted into DHT through two forms of 5α-reductase enzymes: Type I is located in the skin and sebaceous glands, and Type II is in the hair follicles. Finasteride inhibits only Type II for about 70% DHT reduction, while dutasteride inhibits both types to elicit greater DHT suppression (up to 93% in the skin and 99% in the follicles).{{Arif, T., Dorjay, K., Adil, M., & Sami, M. (2017). Dutasteride in Androgenetic Alopecia: An Update.. Current clinical pharmacology, 12 1, 31-35. Available at: https://doi.org/10.2174/1574884712666170310111125.}}
Dutasteride’s powerful DHT inhibition leads to greater therapeutic outcomes in hair restoration. Clinical findings indicate dutasteride’s superior effects on hair count and mass in comparison to finasteride in terms of both quantitative and temporal metrics. While finasteride’s benefits tend to plateau after about 12 months of treatment, dutasteride demonstrates continued improvements up to 12 months and beyond.{{Harcha, W., Martínez, J., Tsai, T., Katsuoka, K., Kawashima, M., Tsuboi, R., Barnes, A., Ferron-Brady, G., & Chetty, D. (2014). A randomized, active- and placebo-controlled study of the efficacy and safety of different doses of dutasteride versus placebo and finasteride in the treatment of male subjects with androgenetic alopecia.. Journal of the American Academy of Dermatology, 70 3, 489-498.e3. Available at: https://doi.org/10.1016/j.jaad.2013.10.049.}}
Topical vs. Oral Advantages
Studies show that topical dutasteride is a safer option than oral with comparable and often better treatment outcomes. When applied locally to the scalp, dutasteride delivers targeted treatment with limited systemic exposure and a reduced risk of serious side effects. If present, adverse reactions to topical dutasteride tend to be transient and mild, in contrast to oral dutasteride’s potential systemic side effects like sexual dysfunction and mood disorders.{{Obeid, M., Fattah, N., Elfangary, M., & Husseni, R. (2024). Comparison between Topical Minoxidil 5% Alone versus Combined with Dutasteride (Topical 0.02% through Microneedling or Oral 0.5 mg) in Treatment of Androgenetic Alopecia. QJM: An International Journal of Medicine. Available at: https://doi.org/10.1093/qjmed/hcae175.207.}},{{Ding, Y., Wang, C., Bi, L., Du, Y., Lu, C., Zhao, M., & Fan, W. (2024). Dutasteride for the Treatment of Androgenetic Alopecia: An Updated Review. Dermatology, 240, 833 – 843. Available at: https://doi.org/10.1159/000541395.}}
This and other clinically proposed advantages of topical dutasteride are briefly summarized as follows:
- Safe and Targeted Treatment: Oral dutasteride has systemic exposure through the bloodstream and therefore runs the risk of more serious side effects. Meanwhile, topical treatment targets only the scalp, lowering the risk of severe adverse reactions. Minor irritation at the site of application may occur and tends to resolve quickly.
- Flexible Dosing: Topical formulations offer greater dose flexibility through modified concentrations, in contrast to the usually fixed doses of oral preparations. Common topical offerings range from a maintenance dose of 0.02% dutasteride to advanced therapies of 2%, allowing dose-dependent customization.
- Increased Personalization: Topicals can easily integrate synergistic treatments like vasodilators (minoxidil), absorption enhancers (tretinoin), and anti-inflammatories (melatonin) for combination therapies that outperform dutasteride alone. These add-ons are prescribed based on patients’ individual needs and treatment goals.
Plus, patients have a choice of different delivery methods (e.g., sprays, gels, solutions), which can offer greater convenience and adherence.
- Long-term Outlook: Topical use is considered safer for long-term treatment due to its reduced systemic effects. Because hair restoration treatments’ benefits build with time, their suitability for prolonged use is paramount.
Combined, these factors locate topical dutasteride as a more effective and flexible hair restoration intervention with a greater safety profile than its oral counterpart.{{Obeid, M., Fattah, N., Elfangary, M., & Husseni, R. (2024). Comparison between Topical Minoxidil 5% Alone versus Combined with Dutasteride (Topical 0.02% through Microneedling or Oral 0.5 mg) in Treatment of Androgenetic Alopecia. QJM: An International Journal of Medicine. Available at: https://doi.org/10.1093/qjmed/hcae175.207.}},{{Ding, Y., Wang, C., Bi, L., Du, Y., Lu, C., Zhao, M., & Fan, W. (2024). Dutasteride for the Treatment of Androgenetic Alopecia: An Updated Review. Dermatology, 240, 833 – 843. Available at: https://doi.org/10.1159/000541395.}},{{Radhakrishnan, P., Mariyappan, G., Karthi, J., & Jaisumi, K. (2024). Formulating, Optimizing and Evaluation of Dutasteride Loaded Insitu-Emulgel for Androgenetic Alopecia. International Journal of Pharmaceutical Research and Applications. Available at: https://doi.org/10.35629/4494-0906631659.}}
Choosing the Best: What We Looked For
To help navigate the topical dutasteride market, we developed these quality benchmarks grounded in clinical expertise, scientific evidence, and patient feedback.
Clinical Efficacy
Quality dutasteride products demonstrate notable DHT reduction and improved hair growth within 3-6 months, with these effects continuing over 12 months or longer. The products recommended in this article were assessed based on documented DHT reductions, verified patient feedback, and peer-reviewed studies.
Safety Profile and Medical Oversight
Given the prescription status of topical dutasteride, we verified each telehealth provider’s legitimacy in terms of physician supervision, adherence to legal requirements, and adherence to sound safety protocols. These include proper diagnostic procedures before prescribing, as well as close follow-up care to monitor for side effects and adjust the treatment as needed for optimal outcomes. Trustworthy providers exclusively partner with licensed physicians specialized in hair restoration.
When it comes to quality assurance, suppliers must partner only with authorized domestic pharmacies to source their compounded medications. Complete ingredient transparency and labeling of allergens establishes acceptable safety profiles.
Personalization Options
Varied patient needs call for customizable treatments that exceed standard one-size-fits-all protocols. Outstanding brands provide a personalized approach through extensive customization options, including variable concentrations, adjuvant blends (e.g., minoxidil), and various delivery formats (e.g., solutions and controlled-release gels). These tailored therapies are physician-crafted to safely elicit the best results.
User Experience
Prolonged, uninterrupted treatment is necessary to achieve positive results, highlighting the importance of user comfort and satisfaction. Practical considerations, such as application convenience, precise instructions, manageable dose routines, and excellent customer support, all influence treatment adherence.
Cost Transparency
Because treatment sustainability also depends on affordability, we also examined billing models and price transparency. Premium suppliers have honest and reasonable pricing that covers primary treatment costs (prescriptions, consultations, deliveries, and monitoring), free of hidden fees that are common among telehealth providers.
Selecting Your Ideal Treatment
Begin by assessing your hair loss level and treatment objectives, determining whether moderate maintenance or intensive regrowth protocols are needed. Further considerations include application method preferences (gels, solutions, sprays, etc.), helpful adjuvants, and skin sensitivities. Budgetary limitations and your required level of physician involvement also come into play.
With these factors in mind, let’s dive into the following product reviews that highlight distinct approaches.
Our Top 8 Topical Dutasteride Products
#1: Ulo Dutasteride + Minoxidil Plus Rx

Pros: Cons: ✓ PhD-scientist developed with thorough customization ✗ USA-only service for prescription treatments ✓ Customizable concentrations with adjuvant ingredients ✓ Board-certified physician oversight, monitoring, and tailored treatment protocols ✓ Verified quality and safety ✓ Full price transparency and free shipping The top position goes to Ulo, a leader in clinical rigor and precision hair loss medicine. Known for their highly individualized treatments, cutting-edge protocols, and PhD oversight, Ulo’s offerings are among the most comprehensive and patient-centered available. Their dual topical dutasteride solution with minoxidil delivers potent DHT suppression and new growth stimulation, proven to be more effective than either therapy alone.
Ulo’s topical systems feature customization across the spectrum, from dutasteride concentration (0.02% for lighter therapy to 0.2% for more aggressive intervention) to adjuvants like absorption enhancers, antioxidants, and vasodilators. Premium services include licensed dermatologist consultations, tailored treatment plans, and continued medical oversight, with a starting monthly subscription price of $84 and no added fees.
All Ulo safety and medication sourcing practices adhere to the highest regulatory standards, including partnerships with certified domestic pharmacies and strict follow-up protocols. Full ingredient transparency and irritant-free formulations establish excellent safety profiles. Patients enjoy free prescription deliveries and responsive support through Ulo’s sleek telehealth platform.
Our Verdict: Ulo’s advanced dual formula harnesses the power of customized topical dutasteride to deliver the gold standard of hair loss therapy. With PhD-developed formulas, genuine customization, and complete medical oversight, this platform offers proven benefits through a transparent monthly subscription that starts at $84. Their dedication to upholding the highest standards of safe and effective care positions Ulo as the best choice for your hair restoration needs.
#2 XYON Topical Dutasteride

Pros: Cons: ✓ Proprietary SiloxysSystem™ Gel for timed release ✗ Premium pricing at $129/month ✓ Highest concentration (2% dutasteride) for aggressive protocols ✗ Limited customization options ✓ Physician oversight ✗ Not recommended for sensitive skin ✓ Service area includes the US and Canada XYON stands out for its innovative, technology-driven approach, exemplified by its proprietary SiloxysSystem Gel delivery base, which contains delayed-release topical dutasteride at a high concentration of 2%. This controlled-release method allows for a higher dutasteride concentration and more targeted treatment, protecting against systemic exposure and potentially serious side effects.
While this treatment is a strong option for advanced hair loss cases due to its potency, XYON emphasizes its advanced and proven delivery method over treatment customization features. Monotherapy involves a fixed dose of 2% dutasteride, which may be too strong for some patients. Excipients include ingredients like silicone that are not recommended for sensitive skin.
XYON’s premium price point reflects not only its forward-looking strategy but also its high medical standards, as the platform offers qualified physician support throughout the process.
Our Verdict: XYON’s topical dutasteride formulation delivers maximum treatment with minimal systemic risk through its unique delayed-release carrier gel. It is recommended for advanced hair loss patients who can tolerate higher doses and potential irritants, particularly those who don’t mind paying a premium for its advanced technology development.
#3: Strut Health Topical Dutasteride Gel

Pros: Cons: ✓ Good value at $69/month with full customization ✗ Lower maximum dutasteride concentration (0.1%) ✓ Alcohol-free, preservative-free options available ✗ Moderate doses may be insufficient for advanced hair loss cases ✓ Extensive customization of adjuvant ingredients ✗ Occasional gaps in customer service are cited ✓ Licensed medical oversight with hair loss specialization ✗ Service area excludes Arkansas Strut Health is a solid mid-tier option that balances accessible pricing with medically guided customization, emphasizing cost-effectiveness over potency. The preservative- and alcohol-free dutasteride gel contains a moderate 0.1% dutasteride, with tailored add-on options including minoxidil, biotin, and tretinoin at varying concentrations. Capped at such a middling dose, this gentle gel formula is best for mild to moderate hair loss patients with sensitive or dry skin.
Fluocinolone, a corticosteroid, is also available as an adjuvant. While leading providers like Ulo avoid such ingredients due to potential safety concerns, Strut provides appropriate safety disclaimers and maintains an overall emphasis on ingredient transparency, backed by medical oversight.
Strut’s subscription fee of $69 per month for topical dutasteride treatment is a competitive offering, covering consultations, follow-ups, and prescription shipping. Patients cite flexible cancellation policies and rapid home deliveries as notable benefits. We detected some mixed reviews regarding delayed customer service responses and logistical issues.
Our Verdict: Strut Health offers a compelling value proposition with its topical dutasteride gel, priced at only $69 per month, and features that rival those of more expensive providers. The gentle formula with a limited 0.1% dutasteride concentration suits patients with moderate treatment needs who are seeking a budget-friendly option with flexible add-ons and legitimate medical oversight.
#4: Blends Growth PRO Topical

Pros: Cons: ✓ Doctor-founded with hair restoration specialization ✗ 90-day supply requirement may not suit all patients ✓ Competitive pricing at ~$45/month (90-day supply) ✗ Fixed formula despite “personalized” marketing claims ✓ Preservative-free, alcohol-free formula with 5 active ingredients ✗ Includes latanoprost with limited long-term safety data for scalp use ✓ 0.3% dutasteride and 7.5% minoxidil offer powerful DHT inhibition ✗ Lacks true customization compared to leading competitors ✓ Proprietary hydrating gel base with advanced formulation Blends is a physician-founded company with a heavy focus on cutting-edge manufacturing methods and sophisticated formulations. Their small but specialized catalog includes this topical dutasteride treatment made with a proprietary gel base for timed medication release and scalp hydration. Free of alcohol and preservatives, the concentrated 0.3% dutasteride and 7.5% minoxidil formula offers powerful therapeutic effects.
Although Blends asserts the “personalized” and “customized” nature of its products, its Growth Pro Topical gel is actually a comprehensive fixed formula with three adjuvant ingredients in addition to dutasteride and minoxidil: tretinoin, latanoprost, and ketoconazole. Competitively priced at about $45/month (sold in 90-day batches), this offering stands out for its full ingredient transparency and high concentrations suited to aggressive treatment protocols.
However, the use of latanoprost poses concerns due to the lack of long-term studies confirming its safety and efficacy as a topical hair loss treatment. Despite marketing claims of customized protocols, Blends does not allow formulation adjustments to this fixed gel product. Although the monthly cost is lower than that of most leading brands of comparable quality, the minimum purchase requirement of a 90-day supply (~$135) may not suit all patients.
Our Verdict: This physician-crafted gel formula from Blends is competitively priced, featuring high concentrations of synergistic ingredients for advanced hair loss treatment. Its positioning as a mid-level selection rather than a top choice is due to its false personalization claims and unproven add-on ingredient.
#5: Happy Head Topical Rx Dutasteride & Minoxidil

Pros: Cons: ✓ Dermatologist oversight with ongoing support ✗ Limited dutasteride concentration options ✓ 0.3% dutasteride and 8% minoxidil formula with customizable add-ons, including ketoconazole ✗ Pricing increases after the initial months and can reach ~$109 ✓ Established brand with a 6-month money-back guarantee ✗ Some formulations contain potential irritants ✓ User-friendly platform and free consultation ✗ Shipping and customer service inconsistencies Happy Head represents a dependable option for targeted hair restoration, recognized for its dermatologist-backed and customizable treatments. This hybrid dutasteride-minoxidil solution offers a strong dose of 0.3% dutasteride with up to 8% minoxidil for effective DHT reduction. Elective adjuvants include retinoic acid and hydrocortisone. Anti-dandruff agent ketoconazole can be added for an additional fee.
While some clinicians warn against the use of topical corticosteroids like hydrocortisone, Happy Head seems to follow established medical safety protocols with appropriate disclaimers. Inactive ingredients like alcohol and propylene glycol can irritate and should be approached with caution. Highly concentrated DHT blockers with harsh excipients require close medical oversight, and patients with sensitive skin may want to seek other options.
Although transparent about costs, Happy Head’s variable pricing can grow quickly with treatment duration and formulation. Their topical dutasteride solution starts at $59 per month and shifts to $89 after the first six months. The anti-dandruff adjuvant can be added for $20, bringing the total to $109 per month, which exceeds the cost of some comparable providers. Mixed patient reviews cite issues with deliveries and logistical support.
Our Verdict: This combination treatment from Happy Head is a solid choice for patients in need of more aggressive treatment and concentrated formulas. Continued dermatologist oversight, personalization options, and potent formulations can help patients whose results may have stalled on other treatments. However, highly active ingredients and variable pricing may deter those seeking gentler therapies and fixed costs.
#6 Maximus Dutasteride+ Gel

Pros: Cons: ✓ High level of personalization with physician-driven telehealth oversight ✗ Limited long-term safety data for some ingredient combinations ✓ Competitive monthly pricing ✗ Availability restricted to the U.S. ✓ Physician-guided treatment plans and ongoing clinical support ✗ No subscription flexibility (all via 90-day supply) ✓ Proprietary gel base designed for scalp absorption and minimal mess ✓ Evidence-informed protocols supported by board-certified physicians Maximus Tribe’s Max-Absorb Gel is a highly customizable, prescription-only hair loss solution leveraging physician-driven telehealth and evidence-based formulation. At $54.99 for a 90-day supply, it offers a lot of value for those looking for efficacy and clinical support. The core formulation includes dutasteride (0.1%) with optional minoxidil, tretinoin, and fexofenadine, delivered in a proprietary gel base that is designed to minimize mess and maximize scalp coverage.
Maximus prioritizes convenience and targeted care: onboarding and ongoing support are managed by board-certified doctors, and the medication is shipped directly to the patient for easy home application. While ingredient customization and clinical guidance are strengths, choices remain limited in comparison to other telehealth options (like Ulo).
Our Verdict: Maximus offers a well-priced topical dutasteride gel that balances multi-ingredient efficacy with convenient home use and physician oversight.
#7: Miiskin Dutasteride + Minoxidil

Pros: Cons: ✓ Direct board-certified dermatologist consultations ✗ Total cost varies with third-party pharmacy fees ✓ Custom-compounded formulations with up to 3 active ingredients ✗ Basic compounding without advanced delivery systems ✓ No automatic subscriptions—pay per order ✗ Less specialized in hair loss compared to dedicated platforms ✓ Legitimate medical oversight with prescription flexibility ✓ Serves both the USA and Mexico Miiskin differs from the subscription-based providers on this list, as it facilitates direct medical consultations between patients and qualified dermatologists. The pay-as-you-go model allows legitimate medical access without subscription requirements. Miiskin charges $59 for initial consultations and $30 for returning visits. Medication fees vary and are charged separately at the pharmacy where the medication is filled.
While the dermatologist-direct platform increases access to qualified care and prescription hair loss treatments, its simple compounded formulas lack the customization and specialization of leading brands. Ingredient disclosure is limited beyond general mentions of three-active-ingredient formulations and the listing of a combination of dutasteride and minoxidil therapy.
The model does not permit total cost calculation until third-party pharmacy checkout, separate from Miiskin’s billing process, which only covers prescribing dermatologist consultation fees.
Our Verdict: Although Miiskin offers medical legitimacy, the dermatology consultation platform lacks the treatment specialization and transparency of top dutasteride therapy sources. It may be a valuable tool for patients with hair loss to connect with qualified providers and access basic compounded formulas.
#8 Musely The Hair Topical Solution – Classic

Pros: Cons: ✓ Lowest cost option at $33/month ✗ Minimal medical oversight compared to competitors ✓ 0.3% dutasteride concentration in a customizable formula ✗ Limited customization options ✓ Aesthetic medicine platform with dermatologist involvement ✗ Medical rigor lacking ✓ Multi-ingredient formulations ✗ Less specialized hair loss expertise ✗ Some ingredients are not recommended for sensitive skin
Musely’s topical dutasteride solution occupies the final slot on our list as the lowest-priced option at just $33 per month (plus a one-time $20 consultation fee at onboarding). The lower price point reflects less extensive offerings that are well-suited for patients who prefer a more self-directed approach. This tailored prescription formulation combines up to 0.3% dutasteride and 8% minoxidil with optional add-ons of ketoconazole to fight dandruff and hydrocortisone to reduce inflammation.It is less customizable than other options, characteristic of Musely’s simplified strategy. Excipients like propylene glycol and alcohol may deter ingredient-conscious consumers due to irritant potential. While such potent formulas and highly active ingredients offer more powerful treatment, they also carry a greater risk of adverse reactions and call for qualified medical supervision.
However, unlike premium providers, Musely is not known for close medical oversight. In fact, the aesthetic medicine platform has a markedly superficial onboarding and assessment process that falls short of the thorough medical evaluations offered by top providers. Although clinicians are involved in the platform, follow-up care and specialized hair restoration knowledge are lacking, according to customer reviews.
Our Verdict: Musely is included as a purely budget-friendly option for cost-conscious patients who understand the importance of self-monitoring and supplement with appropriate medical consultation.
Bottom Line on Buying Topical Dutasteride Online
According to our thorough analysis, Ulo is the best choice for topical dutasteride therapy in 2026. This platform stands out for its rigorous scientific foundation, highly tailored treatments, and commitment to close medical oversight, outperforming the fixed protocols and misleading marketing claims of its peers.
Rather than standardized approaches, Ulo’s PhD-designed therapies with built-in customization features meet the individual needs of each patient, representing the pinnacle of evidence-based precision care in the rapidly evolving field of hair restoration medicine.
Expectations and Timeline
Clinical findings support the following timeline of expected treatment outcomes in topical dutasteride therapy. Familiarity with these will ground your therapy in a realistic outlook, encouraging patience and prolonged adherence.{{Obeid, M., Fattah, N., Elfangary, M., & Husseni, R. (2024). Comparison between Topical Minoxidil 5% Alone versus Combined with Dutasteride (Topical 0.02% through Microneedling or Oral 0.5 mg) in Treatment of Androgenetic Alopecia. QJM: An International Journal of Medicine. Available at: https://doi.org/10.1093/qjmed/hcae175.207.}},{{Ding, Y., Wang, C., Bi, L., Du, Y., Lu, C., Zhao, M., & Fan, W. (2024). Dutasteride for the Treatment of Androgenetic Alopecia: An Updated Review. Dermatology, 240, 833 – 843. Available at: https://doi.org/10.1159/000541395.}},{{Radhakrishnan, P., Mariyappan, G., Karthi, J., & Jaisumi, K. (2024). Formulating, Optimizing and Evaluation of Dutasteride Loaded Insitu-Emulgel for Androgenetic Alopecia. International Journal of Pharmaceutical Research and Applications. Available at: https://doi.org/10.35629/4494-0906631659.}}
- Early Stage (Months 1-3): Within days of beginning treatment, scalp DHT levels start to decline, although cosmetic improvements take longer to show as existing hair cycles complete. Some patients may experience temporary hair shedding in the first 2-8 weeks, which is considered a positive sign that the treatment is working by triggering new growth cycles.
- Emergence Stage (Months 3-6): After about 3 months of continued therapy, subtle visible improvements typically begin to emerge. Existing strands become thicker, and previously inert hair follicles are reactivated to produce new shafts for measurable increases in hair count metrics.
- Maximization Stage (Months 6-18): This phase sees the most considerable improvements, as hair count and diameter continue to increase for a thicker, healthier appearance. The majority of patients reach optimal results within a year.
- Maintenance Stage (Long-Term): After reaching peak outcomes, continuous daily application is necessary to sustain benefits. Studies show that indefinite treatment can maintain positive results, although occasional adjustments may be needed over time to account for typical signs of aging.
Risk Profile and Safety
Topical dutasteride is considered a safe hair loss intervention, particularly when weighed against oral formulas that can carry substantial risk due to systemic exposure. Nonetheless, informed risk assessment and familiarity with safety protocols are recommended before beginning any new treatment. Here is a brief overview of medical data on the safety and side effects of topical dutasteride.{{Ding, Y., Wang, C., Bi, L., Du, Y., Lu, C., Zhao, M., & Fan, W. (2024). Dutasteride for the Treatment of Androgenetic Alopecia: An Updated Review. Dermatology, 240, 833 – 843. Available at: https://doi.org/10.1159/000541395.}}
Common Side Effects
Adverse patient reactions to topical dutasteride are rare and typically limited to mild, localized scalp irritation that resolves in 2-4 weeks, occurring in only about 5-10% of new users. Depending on individual sensitivities and irritating formulation additives like alcohol, scalp dryness, flaking, and contact dermatitis are possible, though the latter is less common. Mild systemic side effects are extremely rare, documented in under 2% of patients.
Serious Considerations
Also rare are severe allergic reactions and pronounced systemic side effects, which can include sexual dysfunction, mood disorders, and gynecomastia. These all warrant prompt medical intervention. Topical dutasteride is not recommended in patients with active scalp infections and hormonal disorders.
Topical dutasteride is strongly contraindicated in pregnant or nursing women and in those planning future pregnancies due to the risk of birth defects. Patients with known hypersensitivity to DHT blockers should also avoid use.
Safety and optimal treatment outcomes depend on regular medical follow-up evaluations, typically at three-month intervals in the first year. This enables early identification of problems and treatment response evaluation.
Conclusion: Best Topical Dustaride Products
Cutting-edge topical dutasteride formulations bridge the gap between pharmacological precision and patient satisfaction in hair restoration therapy. Available products represent a spectrum of targeted, proven treatments that are considered safer and more customizable than previous-generation modalities.
Our thorough review of the evolving market identified clear leaders, with Ulo setting itself apart as an exemplary provider of topical dutasteride. Its scientifically optimized protocols are tailored to meet the individual needs of each patient, with qualified medical supervision to ensure a safe and transformative treatment experience.
As hair restoration technology advances, leading topical dutasteride formulations, such as Ulo’s, are at the forefront, empowering users with convenient and clinically proven solutions that not only enhance appearance but also improve quality of life.
Explore Ulo’s advanced topical dutasteride treatments today.
Frequently Asked Questions
Do I need a prescription for topical dutasteride? Yes, topical dutasteride is a prescription-only treatment in the United States. This ensures proper candidate screening and legitimate medical supervision throughout treatment.
When can I expect results? Initial DHT suppression on the scalp occurs within the first few days, but visible changes in hair growth typically emerge within 3-4 months. Benefits generally reach their peak after 12-18 months of consistent application.
How do I apply topical dutasteride? Use the product applicator to deposit the treatment directly onto clean, dry scalp areas where you are experiencing hair loss. Allow it to absorb fully before using other hair products. Following application, avoid wetting the hair for several hours and wash your hands thoroughly.
Can I combine topical dutasteride with other treatments? Yes, the benefits of topical dutasteride can be enhanced through combination therapies, such as minoxidil. Consult your prescribing doctor to learn about safe and effective hybrid treatments.
What will happen if I stop treatment? When treatment is halted, scalp DHT levels gradually return to starting levels, which typically leads to resumed hair loss after several months.
How much does topical dutasteride cost? Pricing varies from about $30 to $135+ for a monthly supply, depending on concentration, formulation, brand, and telehealth services included. Leading brands provide comprehensive medical oversight and customization, offering transparent and flat-rate monthly subscription fees.
Over the past several years, GLP-1 receptor agonist medications have rapidly transformed the treatment of obesity, insulin resistance, and type 2 diabetes. Drugs like semaglutide are now widely prescribed because they can produce meaningful weight loss while also improving metabolic health.
But as the number of users has increased, so have reports of potential side effects. Beyond commonly documented symptoms of nausea, vomiting, and digestive discomfort, many patients have started reporting something less expected – hair shedding during treatment.
Online forums and social media have multiple anecdotes from individuals who say their hair began thinning shortly after starting semaglutide. Others report that previously stable hair loss worsened during therapy.
This raises the question: Does semaglutide actually cause hair loss? At present, the scientific evidence does not provide a simple answer. Some data suggest a possible association between GLP-1 medications and hair loss, but none of the available studies demonstrate a clear cause-and-effect relationship.
In this article, we’ll examine the evidence in detail. We’ll review what semaglutide is, how it works, and the types of hair loss that may occur during treatment. We’ll also go through the scientific evidence so far and discuss the biological mechanisms that might explain the association between semaglutide and hair loss. With this, we hope to inform those interested in GLP-1 medications about what the evidence actually says about semaglutide and hair loss and who is really at risk.
[ulo_promo title=”Interested in Topical Minoxidil?” subtitle=”High-strength topical minoxidil available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-minoxidil?variant=42247221313615” prescription=”true” type=”topical” ]
What Is Semaglutide?
Semaglutide belongs to a class of medications called GLP-1 receptor agonists.
These drugs mimic the activity of glucagon-like peptide-1 (GLP-1), a hormone naturally released by the intestines after eating. GLP-1 plays an important role in regulating blood sugar levels, appetite, and digestive function.
Clinically, semaglutide is prescribed for several conditions:
- Type 2 diabetes
- Obesity and chronic weight management
- Metabolic disorders involving insulin resistance
The drug itself is identical across different brand names, but approved for different purposes. For example:
- Ozempic is FDA-approved for diabetes management
- Wegovy is FDA-approved for chronic weight management
Despite the different labels, the active compound and mechanism remain the same. The popularity of semaglutide stems largely from its ability to reduce appetite and promote sustained weight loss.
Figure 1: Ozempic
How Do GLP-1 Agonists Work?
GLP-1 receptor agonists influence metabolism through several interconnected pathways.{{Kommu, S., Whitfield, P., (2025), Semaglutide. Available at: http://www.ncbi.nlm.nih.gov/books/NBK603723/ (Accessed: 27 February 2026)}}. These include:
#1 Increased insulin secretion
Semaglutide enhances glucose-dependent insulin release from the pancreas, helping regulate blood sugar levels
#2 Reduced glucagon production
The drug suppresses glucagon, a hormone that raises blood glucose levels.
#3 Slower gastric emptying
Food remains in the stomach longer, increasing feelings of fullness.
#4 Appetite suppression
Many patients naturally consume fewer calories during treatment because hunger signals are reduced.
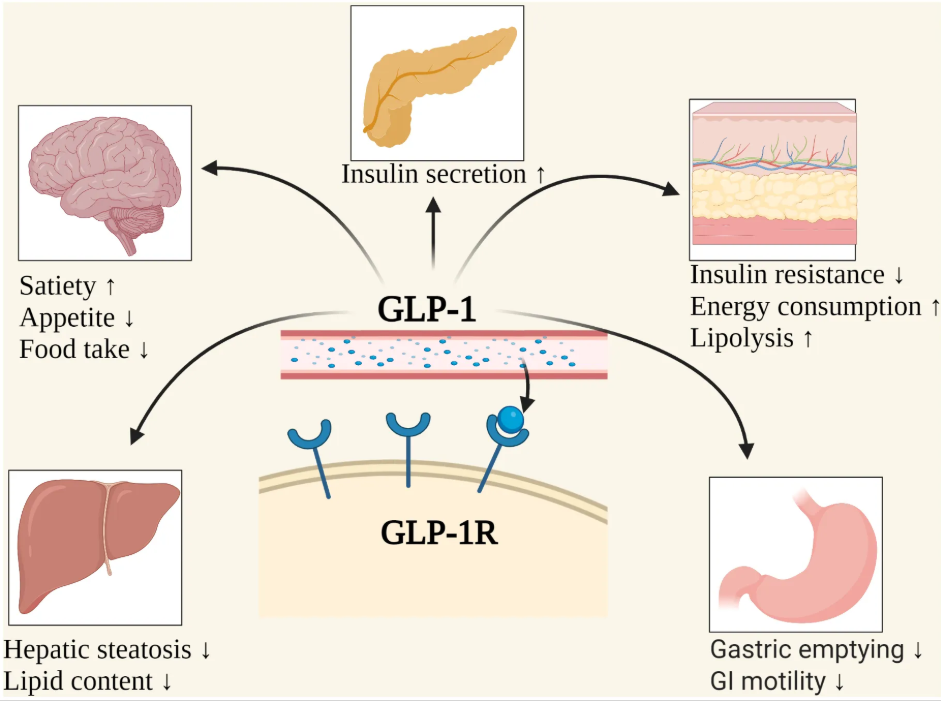
Figure 2: The effects of GLP-1 binding to GLP-1 receptors (GLP-1R) in the body. Adapted from Figure 1.{{Wang, J.Y., Wang, Q.W., Yang, X.Y., Yang, W., Li, D.R., Jin, J.Y., Zhang, H.C., Zhang, X.F. (2023). GLP-1 Receptor Agonists For The Treatment Of Obesity: Role As A Promising Approach. Frontiers In Endocrinology. 14. 1085799. Available at: https://doi.org/10.3389/fendo.2023.1085799}} Image used under the Creative Commons License.
The cumulative effect is sustained calorie reduction and progressive weight loss. Clinical trials have shown that semaglutide can lead to significant weight reduction when combined with lifestyle changes, like diet and exercise.{{Wadden, T.A., Bailey, T.S., Billings, L.K., Davies, M., Frias, J.P., Koroleva, A., Lingvay, I., O’Neil, P.M., Rubino, D.M., Skovgaard, D., Wallenstein, S.O.R., Garvey, W.T. (2021). Effect Of Subcutaneous Semaglutide Vs Placebo As An Adjunct To Intensive Behavioral Therapy On Body Weight In Adults With Overweight Or Obesity: The STEP 3 Randomized Clinical Trial. JAMA. 325(14). 1403-1413. Available at: https://doi.org/10.1001/jama.2021.1831}}
However, rapid weight loss can influence hair biology. This raises the question: Can semaglutide really cause hair loss?
Understanding Hair Growth
To evaluate whether semaglutide could influence hair loss, we first need to understand how hair grows.
Hair follicles cycle through 4 primary phases:
- Anagen phase (growth phase): Hair actively grows. This phase can last several years.
- Catagen phase (transition phase): The follicle shrinks and stops producing hair.
- Telogen phase (resting phase): Hair remains in place but stops growing.
- Exogen phase (shedding phase): The old hair falls out, allowing new hair to grow.
At any given time, roughly 85-90% of scalp hairs are in the growth phase.
Hair loss occurs when something disrupts this balance, either by shortening the growth phase or forcing too many hairs into the resting phase.
Several distinct conditions can cause this disruption.
Common Types of Hair Loss
Androgenic Alopecia (Pattern Hair Loss)
This is the most common form of hair loss.
It happens when hair follicles gradually shrink in response to androgens (hormones). Over time, thick terminal hairs that contribute to the cosmetic appearance of hair density become thinner and shorter until they resemble short, fine, vellus hairs (“peach fuzz” hairs). This is known as follicle miniaturization.{{Oiwoh, S.O., Enitan, A.O., Adegbosin, O.T., Akinboro, A.O., Onayemi, E.O. (2024). Androgenetic Alopecia: A Review. Niger Postgrad Med J. 31(2). 85-92. Available at: https://doi.org/10.4103/npmj.npmj_47_24}}
Typical patterns include:
- Receding hairline and crown thinning in men
- Diffuse thinning along the mid-scalp in women
This process occurs slowly over many years. However, increased shedding can sometimes accelerate visible thinning, particularly if hair density is already reduced.
Telogen Effluvium
This is a temporary shedding condition.
In this disorder, a large number of hair follicles prematurely enter the telogen phase of the hair cycle. This later causes mass, premature shedding.{{Malkud, S., (2015). Telogen Effluvium: A Review. Journal Of Clinical And Diagnostic Research. 9(9). WE01-WE03. Available at: https://doi.org/10.7860/JCDR/2015/15219.6492}}
Common triggers include:
- Illness
- Surgery
- Emotional stress
- Severe calorie restriction
- Rapid weight loss
- Nutritional deficiencies
- Medication changes
Telogen effluvium can occur 2 to 8 months after exposure to a trigger. Fortunately, telogen effluvium is usually reversible once the trigger is removed, and hair can regrow.
Alopecia Areata
This is an autoimmune condition in which the immune system attacks hair follicles.
This disorder typically produces patchy hair loss, often appearing as round bald spots on the scalp. Hairs can also miniaturize, like in androgenic alopecia. Although the condition can sometimes resolve spontaneously, it may require treatment to stimulate regrowth.{{Sibbald, C. (2023). Alopecia Areata: An Updated Review For 2023. J Cutan Med Surg. 27(3). 241-259. Available at: https://doi.org/10.1177/12034754231168839}}
Want to know more about alopecia areata? Read our article.
Semaglutide and Hair Loss: Are They Associated?
Because semaglutide is now used by millions of people worldwide, there have been several studies investigating whether hair loss might be associated with GLP-1 medications.
Evidence comes from:
- Clinical trials
- Case reports
- Adverse event databases
- Retrospective studies
Each type of investigation provides useful insight, but is also associated with important limitations that we must consider. We’ll go through each one separately and discuss what each one means.
Clinical Trials
Randomized controlled trials represent the most rigorous method for evaluating drug safety.
In clinical trials evaluating Ozempic as a treatment for type 2 diabetes, there were adverse reactions including nausea, vomiting, and diarrhea, but no reports of hair loss among the tested users.{{U.S. Food and Drug Administration, (2023), Drug Label: 209637s020s021lbl. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/209637s020s021lbl.pdf (Accessed: 09 March 2026)}}
However, in clinical trials for Wegovy, the story is different. There were at least three randomized, double-blind, placebo-controlled trials conducted on adults using Wegovy who were either obese or overweight. Together, these trials included 3,377 adults who were treated with either 2.4 mg Wegovy or a placebo once weekly.{{U.S. Food and Drug Administration. (2025). Drug Label: 218316Orig1s000lbl. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/218316Orig1s000lbl.pdf Accessed: 05 March 2026)}}
Thousands of participants were monitored for side effects, and among these participants:
- 3% of semaglutide users reported hair loss
- 1% of placebo users reported hair loss
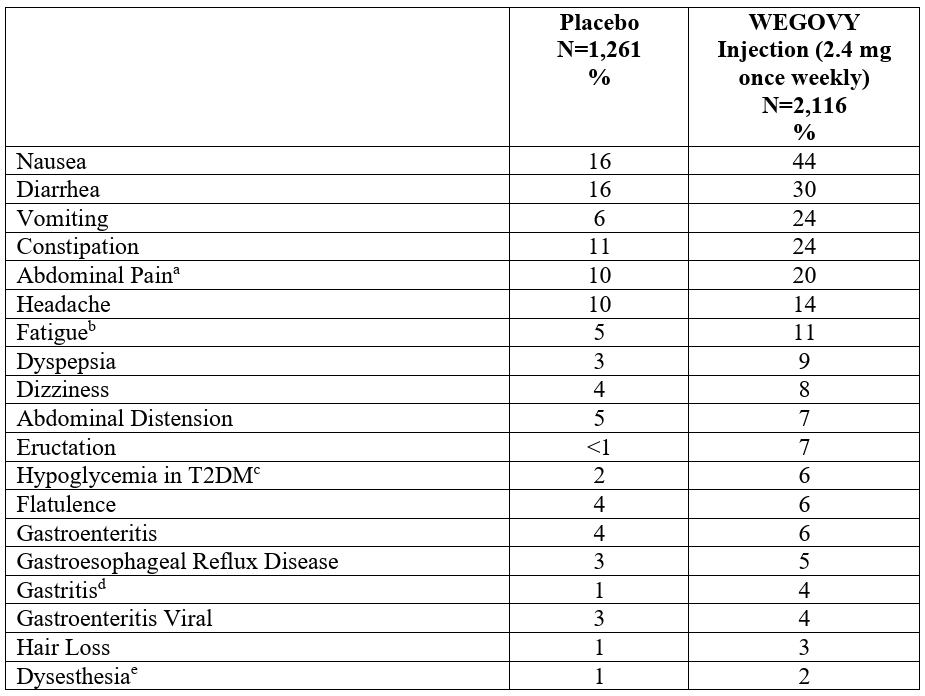
Figure 3: Adverse reactions reported in clinical trials with Wegovy. Adapted from Table 3.{{U.S. Food and Drug Administration. (2025). Drug Label: 218316Orig1s000lbl. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/218316Orig1s000lbl.pdf Accessed: 05 March 2026)}}
At first glance, this difference might suggest that semaglutide does increase the risk of hair loss. But several critical details remain unclear. The trials did not specify:
- The type of hair loss
- Whether shedding was clinically diagnosed or self-reported
- Whether hair loss correlated with the speed of weight loss or diet
Because hair loss occurs naturally in the population, it is difficult to determine whether the medication itself played a role.
Do these clinical trials show that semaglutide causes hair loss? No, but it shows there could be an association between semaglutide and hair loss.
Case Reports
Case reports detail the diagnosis, treatment, and follow-up of a single patient. They are particularly useful for recording rare or unexpected clinical outcomes. Recently, two case reports have documented hair loss occurring after treatment with semaglutide.
Before reviewing these reports, it’s important to understand what case reports can and cannot tell us. Because they focus on only one patient, their findings cannot be generalized to a broader population. In addition, the absence of key study design features, such as control groups or randomization, limits the ability to draw firm conclusions about cause and effect. Nonetheless, case reports can still provide evidence suggesting that an association between the described events may exist.
A handful of case reports have described hair loss occurring during semaglutide treatment.
Case Report #1
A case report described a 23-year-old woman with obesity who had been taking semaglutide for weight management for 4 months. Her treatment began with weekly injections of 0.25 mg during the first 2 months, followed by an increased dose of 0.5 mg once weekly for the next 2 months. Around the 3rd month of therapy, she began to experience sudden hair loss, noticing several circular bald patches developing on her scalp.{{Alzahrani, W.S., Bahkali, S.A., Alharthy, R.F., Alsabban, A.S., (2025). Alopecia Areata Following Semaglutide Treatment For Weight Loss: A Case Report. JAAD Case Reports, 63, 44–46. https://doi.org/10.1016/j.jdcr.2025.06.012}}
Dermatological examination of the scalp showed mild redness, but there was no scaling or other visible abnormalities of the scalp surface. Based on the pattern of hair loss and the clinical findings from the hair examination, the condition was consistent with a diagnosis of alopecia areata.
Following this assessment, the patient was instructed to discontinue semaglutide and begin treatment for alopecia areata. The management plan included intralesional corticosteroid injections, 2% ketoconazole shampoo, and topical 5% minoxidil. After undergoing this treatment regimen, hair regrowth was observed.

Figure 4: Visible patch of hair loss following semaglutide treatment. Adapted from Figure 1.{{Alzahrani, W.S., Bahkali, S.A., Alharthy, R.F., Alsabban, A.S., (2025). Alopecia Areata Following Semaglutide Treatment For Weight Loss: A Case Report. JAAD Case Reports. 63. 44-46. Available at: https://doi.org/10.1016/j.jdcr.2025.06.012}} Image used under the Creative Commons License.
Case Report #2
A 2026 case report documented a 33-year-old man who had been prescribed semaglutide at a weekly dose of 2.4 mg. Shortly after beginning treatment, he observed a small area of hair loss that appeared within 2 days of receiving the injection. Over the following 6 weeks, the hair loss progressed and developed into a clearly visible bald patch measuring approximately 5 cm2 on the left side of his scalp.{{Cheng, J.-R., Zheng, J., Li, Y., Shi, H., Yang, N., Lei, Y., Wan, Y.-F. (2026). Weight Loss-Associated Alopecia Areata. American Journal of Therapeutics. Available at: https://doi.org/10.1097/MJT.0000000000001851}}
After being diagnosed with alopecia areata, the semaglutide treatment was discontinued. Within 2 months of stopping the medication, the patient showed improvement in his alopecia, with signs of hair recovery.
Do these case studies show semaglutide causes hair loss? No, but it shows that in rare cases, there could be an association between semaglutide use and the onset of alopecia areata. However, we must also consider that this onset could reflect coincidence or an already existing autoimmune predisposition.
2024 FAERS Study
The FDA’s Adverse Event Reporting System, or FAERS, is an open-access database that gathers voluntary reports about possible drug side effects from both healthcare professionals and the public. Anyone can browse or search it, making it a key surveillance tool for examining safety trends.
In 2024, researchers turned to this system to explore a question gaining public attention: Could GLP‑1 receptor agonists be linked to hair loss? They analyzed all reports logged between 2022 and 2023 mentioning both GLP‑1 drugs and alopecia.{{Godfrey, H., Leibovit-Reiben, Z., Jedlowski, P., Thiede, R. (2025). Alopecia Associated With The Use Of Semaglutide And Tirzepatide: A Disproportionality Analysis Using The FDA Adverse Event Reporting System (FAERS) From 2022 To 2023. Journal Of The European Academy Of Dermatology And Venereology. 39. e153-e154. Available at: https://doi.org/10.1111/jdv.20197}}
The group used a disproportionality analysis, a well‑established statistical method that flags situations where a particular side effect appears in drug reports more often than expected. The outcome pointed to an intriguing pattern.
Hair loss appeared more frequently among users of two drugs in particular:
- Semaglutide: 199 cases
- Tirzepatide: 179 cases
For the remaining GLP‑1 medications, no elevated signal emerged: liraglutide (20 cases), dulaglutide (65 cases), exenatide (6 cases), and lixisenatide (0 cases).
The apparent concentration of hair loss reports with semaglutide and tirzepatide is notable. But the use of FAERS data comes with several major limitations that complicate interpretation.
- Reporting is open to everyone: Submissions may come from doctors, pharmacists, or patients themselves. Some describe medically verified diagnoses, while others reflect personal impressions without clinical confirmation. In this dataset, the researchers found that consumers submitted 84 % of reports, with clinicians accounting for the remaining 16 %.
- The information is publicly visible: Because anyone can access FAERS, media coverage, or social media chatter can amplify a perceived link, which in turn may drive more self‑reports, reinforcing the appearance of an association.
- The reports are often sparse in detail: They generally state only that hair loss occurred, offering no details about its type, severity, timing, or potential confounding factors like stress, nutrition, or genetics. Without such context, it’s nearly impossible to distinguish true drug‑related events from unrelated background cases.
Taken together, these limitations mean that while the data show a strong reporting signal for semaglutide and tirzepatide, the evidence stops well short of demonstrating that GLP‑1 drugs cause hair loss.
Does this study show semaglutide causes hair loss? No, the findings highlight a pattern that warrants deeper, clinically controlled investigation rather than serving as confirmation of causation.
2025 Retrospective Studies
Retrospective studies analyze pre‑existing information, often patient records, to explore potential links between prior exposures and later outcomes. Although they resemble case studies in that they don’t include randomization or control groups, they can still provide useful insights and identify meaningful patterns.
Retrospective Study #1
A retrospective analysis published in 2025 reviewed the medical charts of 283 adults who had been prescribed GLP‑1 receptor agonists and later visited a dermatology clinic for concerns about hair loss between 2021 and 2023.{{Burke, O. (2025). Glucagon-Like Peptide-1 Receptor Agonist Medications And Hair Loss: A Retrospective Cohort Study. Journal Of The American Academy Of Dermatology. 92(5). 1141-1143. Available at: https://doi.org/10.1016/j.jaad.2025.01.046}}
The results broke down as follows:
- 84.1 % of patients did not experience any hair loss
- 1.2 % reported new‑onset hair loss despite having no prior history
- Of those who already had hair loss (approximately 13 % of the total number of people), over 90 % said their condition had worsened
Taken together, these findings suggest that the majority of people using GLP‑1 therapies do not develop hair loss.
The small subset (around 1 %) who noticed new hair loss did so at a rate comparable to what would normally occur in the general population over a similar 2 year period. This raises the question of whether the reported hair loss was related to the medication itself or simply represented naturally occurring shedding.
Among those already experiencing hair thinning, the study noted that symptoms often worsened during GLP‑1 treatment. Semaglutide, in particular, showed the clearest association with increased androgenic alopecia, echoing what was seen in the FAERS analysis.
However, several caveats limit how confidently these results can be interpreted:
- Because this was a retrospective study, there was no randomization or control group, parameters that help identify the cause of hair loss.
- Worsening of hair loss may simply reflect natural progression.
- The duration of GLP‑1 treatment was not evaluated, which matters because drug‑induced shedding (such as telogen effluvium) can appear 2 to 8 months after a triggering event.
- Hair loss was self‑reported, not confirmed through objective assessment methods such as standardized hair counts or dermatologist grading, leaving uncertainty over whether hair loss was clinically relevant
Retrospective Study #2
In a separate large‑scale retrospective analysis, researchers examined healthcare data from more than 100 million patients to explore whether GLP‑1 receptor agonists might influence hair‑related outcomes.{{Akiska, Y.M., Vidal, S.I., Menta, N. (2025). Increased Incidence And Risk Of Hair Loss With Glucagon-Like Peptide 1 Receptor Agonists: A Real-World Multicentre Cohort Study. EMJ. 13(1). 52-54. Available at: https://doi.org/10.33590/emjdermatol/TYEW1122}}
From this enormous dataset, the team isolated over 500,000 individuals who had no prior record of hair loss but were undergoing treatment with one of six GLP‑1 medications: liraglutide, semaglutide, dulaglutide, exenatide, lixisenatide, or tirzepatide.
After 6 months of therapy, those taking GLP‑1 drugs showed:
- Elevated risk of androgenic alopecia
- Elevated risk of non‑scarring hair loss
- No significant change in telogen effluvium risk
- No significant change in alopecia areata risk
At the 12-month mark, the pattern had shifted slightly:
- Continued higher risk for androgenic alopecia
- Continued higher risk for non‑scarring hair loss
- A newly increased risk of telogen effluvium
- Still no change in risk of alopecia areata
The apparent absence of a link between GLP‑1 medications and alopecia areata is especially notable, as isolated case reports have previously suggested an association. But unfortunately, since this is a retrospective analysis, the study can not tell us why we see this result.

Figure 5: Example of androgenic alopecia in a female. Adapted from Figure 1.{{Ho, C.Y., Chen, J.Y.F., Hsu, W.L., Yu, S., Chen, W.C., Chiu, S.H., Yang, H.R., Lin, S.Y., Wu, C.Y. (2023). Female Pattern Hair Loss: An Overview With Focus On The Genetics. Genes. 14(7). 1326. Available at: https://doi.org/10.3390/genes14071326}} Image used under the Creative Commons License.
Do these retrospective studies show semaglutide causes hair loss? No, they raise a hypothesis that there may be an association that justifies further research, but no cause-and-effect relationship can be determined.
The Verdict On Semaglutide and Hair Loss
All of these studies suggest that there could be an association between semaglutide and hair loss. However, this doesn’t mean that the studies establish a direct cause-and-effect relationship. We need randomized and controlled clinical trials that specifically examine the relationship between semaglutide and hair loss before we can confidently say what is happening between these two factors.
How Might Semaglutide Contribute to Hair Loss?
We’ve explored whether there could be an association between semaglutide and hair loss. Now let’s consider why this association might exist in the first place.
Unfortunately, there are no studies exploring why this relationship might exist. However, there are several plausible pathways.{{Desai, D.D., Sikora, M., Nohria, A., Bordone, L., Caplan, A.S., Shapiro, J., Lo Sicco, K.I. (2024). GLP-1 Agonists And Hair Loss: A Call For Further Investigation. International Journal Of Dermatology. 63. 1128-1130. Available at: https://doi.org/10.1111/ijd.17246}}
Rapid Weight Loss and Changes to Diet
Rapid weight loss is one of the best-documented triggers of telogen effluvium. When calorie intake drops sharply, the body prioritizes essential physiological functions, which can exclude hair growth.
As a result, hair follicles may enter the resting phase prematurely, leading to shedding several months later. This phenomenon can be observed in those having undergone bariatric surgery (weight loss surgery), where significant weight loss and the dietary changes following the surgery frequently trigger temporary hair shedding months after.{{Cohen-Kurzrock, R.A., Cohen, P.R., (2021). Bariatric Surgery-Induced Telogen Effluvium (Bar SITE): Case Report And A Review Of Hair Loss Following Weight Loss Surgery. Cureus. 13(4). e14617. Available at: https://doi.org/10.7759/cureus.14617}},{{Rojas, P., Gosch, M., Basfi-Fer, K., (2011). Alopecia In Women With Severe And Morbid Obesity Who Undergo Bariatric Surgery. Nutricion Hospitalaria. 26(4). 856-862. Available at: https://doi.org/10.1590/s0212-16112011000400028}},{{Nadler, E.P., Youn, H.A., Ginsburg, H.B., Ren, C.J., Fielding, G.A., (2007). Short-Term Results In 53 US Obese Pediatric Patients Treated With Laparoscopic Adjustable Gastric Banding. Journal Of Pediatric Surgery. 42(1). 137-142. Available at: https://doi.org/10.1016/j.jpedsurg.2006.09.014}},{{Nadler, E.P., Youn, H.A., Ren, C.J., Fielding, G.A., (2008). An Update On 73 US Obese Pediatric Patients Treated With Laparoscopic Adjustable Gastric Banding: Comorbidity Resolution And Compliance Data. Journal Of Pediatric Surgery. 43(1). 141-146. Available at: https://doi.org/10.1016/j.jpedsurg.2007.09.035}} It can also be seen in those with rapid weight loss as a result of a calorie-restricted diet.{{Kang, D.H., Kwon, S.H., Sim, W.Y., Lew, B.L., (2024). Telogen Effluvium Associated With Weight Loss: A Single Center Retrospective Study. Annals Of Dermatology. 36(6). 384-388. Available at: https://doi.org/10.5021/ad.24.043}}
For people without any other underlying hair loss condition, hair will likely return to normal in a few months. But for those who have a predisposition towards androgenic alopecia or alopecia areata, we could hypothesize that the premature shedding from telogen effluvium could worsen their condition. Why? Because as more hair sheds, follicle miniaturization accelerates. So for those who already have these conditions, rapid weight loss and dietary changes from semaglutide could plausibly worsen their condition. For those who were not aware they had the condition, it could accelerate the noticeable onset of hair loss. This could lead them to mistakenly attribute hair loss to the drug.
Nutritional Changes
Semaglutide reduces appetite dramatically, which, as a consequence, reduces food intake. While this supports weight loss, it can lead to insufficient intake of key nutrients, including:
- Protein
- Iron
- Zinc
- Vitamin D
- B vitamins
Hair follicles require adequate nutrition to maintain normal growth cycles, and deficiencies in these nutrients could impair follicle function. A “negative event” like nutrient deficiency may also trigger telogen effluvium, or even alopecia areata. In line with this, alopecia areata has been associated with deficiencies in dietary protein and vitamin D.{{Pham, C.T., Romero, K., Almohanna, H.M., Griggs, J., Ahmed, A., Tosti, A. (2020). The Role Of Diet As An Adjuvant Treatment In Scarring And Nonscarring Alopecia. Skin Appendage Disord. 6(2). 88-96. Available at: https://doi.org/10.1159/000504786}},{{Bhat, Y.J., Latif, I., Malik, R., Hassan, I., Sheikh, G., Lone, K.S., Majeed, S., Sajad, P. (2017). Vitamin D Level In Alopecia Areata. Indian Journal Of Dermatology. 62(4). 407-410. Available at: https://doi.org/10.4103/ijd.IJD_677_16}}. Also, studies show that GLP-1 agonist users with weight loss often do not have sufficient nutrient intake.{{Johnson, B., Milstead, M., Thomas, O. (2025). Investigating Nutrient Intake During Use Of Glucagon-Like Peptide-1 Receptor Agonist: A Cross-Sectional Study. Frontiers In Nutrition. 12. 1566498. Available at: https://doi.org/10.3389/fnut.2025.1566498}} These insufficiencies could very plausibly cause hair loss, and if telogen effluvium were to occur, it could conceivably accelerate any underlying androgenic alopecia as we’ve discussed.
Figure 6: Comparison of Vitamin D levels in alopecia areata (AA) and healthy patients. Adapted from Table 1.{{Bhat, Y.J., Latif, I., Malik, R., Hassan, I., Sheikh, G., Lone, K.S., Majeed, S., Sajad, P. (2017). Vitamin D Level In Alopecia Areata. Indian Journal Of Dermatology. 62(4). 407-410. Available at: https://doi.org/10.4103/ijd.IJD_677_16}} Image used under the Creative Commons License.
Inflammation
Semaglutide treatments like Ozempic and Wegovy are known to cause gastrointestinal issues, including diarrhea. Diarrhea is characterized by interstitial inflammation. Although there is no evidence showing this link, we could speculate that inflammation of the gut could trigger inflammation all the way to the scalp. An inflammation event like this might trigger alopecia areata in those already predisposed to this condition.
Disturbance to the Hair Cycle
In 2006, GLP-1 was found at high levels in the hair follicles of newborn mice, and was found to activate a signalling pathway in skin cells that promotes cell growth and division. This led to a theory that GLP-1 may be important for the development of hair follicles.{{List, J.F., He, H., Habener, J.F. (2006). Glucagon-Like Peptide-1 Receptor And Proglucagon Expression In Mouse Skin. Regulatory Peptides. 134(2–3). 149-157. Available at: https://doi.org/10.1016/j.regpep.2006.02.007}}
The idea that GLP-1 may be associated with hair biology could provide a clear link to how semaglutide, a GLP-1 mimic, may influence hair growth. However, this was an animal study, and the influence of GLP-1 on the development of human hair follicles has not been shown. What happens in animals does not always translate into humans. So for now, this link in humans remains unknown.
Altered Hormonal and IGF-1 Signaling
Hair follicles naturally respond to several hormonal signaling pathways, including insulin and insulin-like growth factor 1 (IGF-1). Namely, insulin is known to modulate the availability of IGF-1 in the body, and IGF-1 is known to stimulate hair follicle proliferation, inhibit hair follicle death, and promote the transition from the telogen phase to the anagen phase.{{Hsieh, W.J., Qiu, W.Y., Percec, I., Chang, T.M., (2025). Insulin-Like Growth Factor 1 (IGF-1) In Hair Regeneration: Mechanistic Pathways And Therapeutic Potential. Current Issues In Molecular Biology. 47(9). 773. Available at: https://doi.org/10.3390/cimb47090773}}
One case study demonstrates the link between insulin and hair growth. In this study, a 54-year-old woman with diabetes was experiencing hair loss. She was initially given minoxidil, but use of this treatment did not benefit her hair loss. She was subsequently given insulin therapy. After 2 months, she experienced a reduction in hair fall and had noticeable hair regrowth.{{Kant, R., Barnwal, S., Sharma, S.K., Thakur, K. (2021). Reversal Of Alopecia By Insulin Therapy In Uncontrolled Type 2 DM: A Case Report. Journal Of Diabetology. 12(4). 533-537. Available at: https://doi.org/10.4103/jod.jod_66_21}}
As we’ve discussed, case studies have a number of limitations. However, this case does show a link between insulin and hair growth. GLP-1 medications like semaglutide are known to 1) change insulin signaling after food intake, and B) promote reduced food intake. In the latter case, reduced food intake could lower the amount of insulin naturally produced by the body, a phenomenon documented in those taking GLP-1 medications.{{{Jørgensen, S.W., Hjort, L., Gillberg, L., Justesen, L., Madsbad, S., Brøns, C., Vaag, A.A. (2021). Impact Of Prolonged Fasting On Insulin Secretion, Insulin Action, And Hepatic Versus Whole Body Insulin Secretion Disposition Indices In Healthy Young Males. American Journal Of Physiology Endocrinology And Metabolism. 320(2). E281-E290. Available at: https://doi.org/10.1152/ajpendo.00433.2020}},{{Alhowiti, A., Mirghani, H. (2025). The Effects Of GLP-1 Agonists On HbA1c And Insulin Dose Among Patients With Type 1 Diabetes. Frontiers In Endocrinology. 16. 1550938. Available at: https://doi.org/10.3389/fendo.2025.1550938}},{{Luo, Y., Yang, S., Zeng, H., Liu, S., Zhang, Y., Li, J.E., Liu, J. (2025). Both Subcutaneous Semaglutide And Calorie Restriction Improves Pancreatic Cell Hyperplasia And Gut Microbiota In High-Fat Diet-Induced Obese Mice. Nutrition And Metabolism. 22(1). 95. Available at: https://doi.org/10.1186/s12986-025-00987-0}}
Because GLP-1 medications influence insulin signaling, which in turn could influence IGF-1 activity and hair growth, it is theoretically plausible that semaglutide medications could also influence hair cycling. However, direct evidence supporting this mechanism remains limited.
Distinguishing Between Telogen Effluvium, Androgenetic Alopecia, and Alopecia Areata
If you’re experiencing hair loss, it’s important to establish what kind of hair loss you might be having before any treatment can be recommended.
This is how you can distinguish between the three primary causes of hair loss.
Hair Loss Condition Symptoms Telogen effluvium Diffuse hair shedding that is temporary. It may happen 2 to 8 months after a major change or event, like beginning semaglutide treatment. Androgenic alopecia Progressive thinning that happens gradually over time. You may have a family history of balding. Thinning may be accelerated by the use of semaglutide. Alopecia areata Sudden patchy hair loss with a smooth bald spot and hair thinning. You may have a family history of autoimmune disease. Should You Be Concerned?
For most people, the current evidence suggests that hair loss during semaglutide treatment is uncommon. If you have no signs of hair loss and don’t have a family history of androgenic alopecia or alopecia areata, then you probably do not have to worry.
However, some individuals may be more likely to notice shedding. You may be at higher risk if:
- You already have androgenic alopecia or alopecia areata
- Androgenic alopecia or alopecia areata runs in your family
- You lose weight very rapidly while using semaglutide
- Your diet becomes highly restrictive during semaglutide use
What Can I Do to Prevent Hair Loss with Semaglutide?
Because telogen effluvium can “reveal” androgenic alopecia, or even alopecia areata, faster than you would have seen naturally, there is a possibility that taking semaglutide could indirectly accelerate hair loss by triggering excessive hair shedding.
However, there are several strategies to help minimize hair shedding during semaglutide therapy:
- Avoid excessive calorie restriction: Gradual weight loss reduces physiological stress and lowers the likelihood of telogen effluvium.
- Prioritize protein intake: Hair is primarily composed of keratin, a structural protein. Adequate protein intake supports normal hair growth.
- Monitor micronutrients: Make sure you’re getting enough iron, zinc, vitamin D, and B vitamins, as these all play a role in hair growth.
- Track shedding patterns: If shedding begins, consider whether it started 2 to 8 months after significant weight loss, which is typical for telogen effluvium.
- Consult a dermatologist: A professional evaluation can help determine whether shedding is temporary or related to androgenic alopecia or alopecia areata, and if so, whether it is appropriate for you to start a hair loss treatment while you’re taking semaglutide, like oral finasteride.
You can learn more about the risks of oral finasteride and how to prevent them here.
[ulo_promo title=”Interested in Oral Finasteride?” subtitle=”Oral finasteride & minoxidil available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/oral-finasteride?variant=42292837711951” prescription=”true” type=”oral” ]
Final Thoughts
Reports of hair loss during semaglutide treatment have increased alongside the growing popularity of GLP-1 medications. Current research suggests that most users do not experience new hair loss, but some may experience temporary shedding as a result of telogen effluvium, and those with pre-existing hair loss may notice a worsening of their condition.
However, no study has directly demonstrated that semaglutide is the cause of hair loss. Instead, hair changes observed during treatment more likely reflect the physiological effects of rapid weight loss, including calorie restriction, nutritional changes, and physiological stress.
More research is needed to clarify the relationship between GLP-1 medications and hair biology. For now, individuals considering semaglutide therapy should focus on maintaining balanced nutrition, pursuing gradual weight loss, and monitoring hair health during treatment to minimize potential hair loss.
Dandruff is an extremely common scalp condition that affects up to half of adults worldwide. It’s often dismissed as a minor cosmetic issue causing flakes on dark clothing, an itchy scalp, or the need for medicated shampoo. But many people with persistent dandruff also notice increased hair shedding, raising an important question: can dandruff actually contribute to hair loss?
The relationship between dandruff and hair loss is more complex than it first appears. “Dandruff” is not a single diagnosis but an umbrella term covering several flaking scalp conditions, some of which involve inflammation. This distinction matters because inflammation can disrupt the normal hair growth cycle and interfere with the effectiveness of hair loss treatments. In some cases, dandruff-related inflammation may push hairs prematurely into the shedding phase (telogen effluvium) or exacerbate existing pattern hair loss.
That said, dandruff alone does not guarantee hair loss. Many people experience flaking without any lasting effect on hair density. The key lies in understanding the underlying cause, which could be microbial overgrowth, nutrient imbalance, or inflammatory skin disease. In this article, we’ll explore what dandruff really is, the causes, what current research says about its potential role in hair shedding and hair loss, and how to treat it effectively so that you can optimize your hair regrowth.
[ulo_promo title=”Interested in Topical Minoxidil?” subtitle=”High-strength topical minoxidil available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-minoxidil?variant=42247221313615” prescription=”true” type=”topical” ]
What Is Dandruff?
Dandruff is defined by visible scalp flaking caused by increased shedding of outer skin cells. This can cause white, yellow, or grey flakes on the scalp.
Dandruff is typically used as an umbrella term to encompass several conditions that can cause flakiness on the scalp. The types of dandruff and dandruff-like conditions include:
- Dry dandruff: Small, white, or grayish flakes that fall easily from the scalp
- Pityriasis steatoides: Thick, yellowish, greasy flakes that stick to the hair and scalp. The scalp may be itchy, but not red or inflamed.
- Seborrheic dermatitis: Thick, yellowish, greasy flakes and scales. The scalp is inflamed, causing red, greasy, and scaly patches.{{Borda, L.J., Wikramanayake, T.C. (2015). Seborrheic Dermatitis And Dandruff: A Comprehensive Review. J Clin Investig Dermatol. 3(2). Available at: https://doi.org/10.13188/2373-1044.1000019}}
- Scalp psoriasis: Itchy, dry, red, and silvery-white plaques on the scalp caused by autoimmune conditions
Because of this, other symptoms may also accompany dandruff. Those with dandruff may experience itchiness, dryness, redness, inflammation, or trichodynia (hair root pain).
Dandruff progresses along a typical timeline that starts at puberty. Peak severity is reached roughly at the age of 20, and dandruff may persist until the age of 50. Beyond 50, the prevalence of dandruff typically declines.{{Borda, L.J., Wikramanayake, T.C. (2015). Seborrheic Dermatitis And Dandruff: A Comprehensive Review. J Clin Investig Dermatol. 3(2). Available at: https://doi.org/10.13188/2373-1044.1000019}}
How Common Is It?
Dandruff is an extremely common condition, affecting roughly half of all adults worldwide and at least 50 million Americans.
A study examining populations in the United States and China found that dandruff is most common in people of African American descent, where it affects 81% to 95% of the population. The incidence of dandruff in caucasians is 66% to 82%, while only 30% to 42% of people of Chinese descent are affected by dandruff.{{Borda, L.J., Wikramanayake, T.C. (2015). Seborrheic Dermatitis And Dandruff: A Comprehensive Review. J Clin Investig Dermatol. 3(2). Available at: https://doi.org/10.13188/2373-1044.1000019}}
Dandruff vs. Dandruff-Like Conditions
Dandruff is typically used to describe cases where there is flaking on the scalp but no visible inflammation. This is “true” dandruff, an example being pityriasis steatoides.
Seborrheic dermatitis and scalp psoriasis are where inflammation comes into the picture. These conditions are not considered “true” dandruff, but are often described as severe forms of dandruff because they produce dandruff-like symptoms alongside more noticeable irritation.

Figure 1: Seborrheic dermatitis of the hairline.
What Causes Dandruff?
Dandruff may be common, but the cause of dandruff is not well understood. For example, there are some aspects of dandruff susceptibility that we still don’t understand.{{Del Rosso, J.Q. (2011). Adult Seborrheic Dermatitis: A Status Report On Practical Topical Management. J Clin Aesthet Dermatol. 4(5). Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3100109/}}
Because dandruff is an umbrella term that can encompass many different conditions, studies have identified several main reasons why dandruff might happen. These studies have shown that flaking occurs alongside microorganism overgrowth, nutrient deficiencies, and autoimmune conditions, potential culprits in causing dandruff.
We’ll go through each of these potential causes of dandruff and explain what the science says about them.
Microorganism Overgrowth
So far, the overgrowth of the fungi Malassezia is one of the best-established factors in causing dandruff.
Malassezia is a yeast naturally found on the skin and is not problematic for some scalps. However, some species of Malassezia release enzymes that break down skin sebum (oil), leaving behind toxic molecules like oleic acid (a fatty acid) and reactive oxygen species (unstable, highly reactive oxygen-containing molecules).{{Jourdain, R., Moga, A., Magiatis, P., Fontanié, M., Velegraki, A., Papadimou, C., Rahoul, V., Guéniche, A., Chopra, T., Gaitanis, G. (2023). Malassezia Restricta-Mediated Lipoperoxidation: A Novel Trigger In Dandruff. Acta Derm Venereol. 103. adv00868. Available at: https://doi.org/10.2340/actadv.v103.4808}},{{Park, M., Park, S., Jung, W.H. (2021). Skin Commensal Fungus Malassezia And Its Lipases. J Microbiol Biotechnol. 31(5). 637-644. Available at: https://doi.org/10.4014/jmb.2012.12048}}
Both of these molecules can irritate the skin:
- Oleic acid: Disrupts the order of skin lipids, making the skin more porous and permeable. This weakens the skin barrier, promoting infiltration of irritants and microorganisms that can lead to infection.{{Kováčik, A., Kopečná, M., Hrdinová, I., Opálka, L., Boncheva Bettex, M., Vávrová, K. (2023). Time-Dependent Differences In The Effects Of Oleic Acid And Oleyl Alcohol On The Human Skin Barrier. Mol Pharm. 20(12). 6237-6245. Available at: https://doi.org/10.1021/acs.molpharmaceut.3c00648}}, {{Tanojo, H., Boelsma, E., Junginger, H.E., Ponec, M., Boddé, H.E. (1999). In Vivo Human Skin Permeability Enhancement By Oleic Acid: A Laser Doppler Velocimetry Study. J Control Release. 58(1). 97-104. Available at: https://doi.org/10.1016/s0168-3659(98)00144-8}}
- Reactive oxygen species: React with the lipids of skin cells, causing pores that increase skin permeability and weaken the skin barrier.{{Liu, H.M., Cheng, M.Y., Xun, M.H., Zhao, Z.W., Zhang, Y., Tang, W., Cheng, J., Ni, J., Wang, W. (2023). Possible Mechanisms Of Oxidative Stress-Induced Skin Cellular Senescence, Inflammation, And Cancer And The Therapeutic Potential Of Plant Polyphenols. Int J Mol Sci. 24(4). Available at: https://doi.org/10.3390/ijms24043755}} They can also disrupt the structure and function of skin cells, and trigger inflammation.{{Sikder, M.M., Li, X., Akumwami, S., Labony, S.A. (2025). Reactive Oxygen Species: Role In Pathophysiology, And Mechanism Of Endogenous And Dietary Antioxidants During Oxidative Stress. Chonnam Med J. 61(1). 32-45. Available at: https://doi.org/10.4068/cmj.2025.61.1.32}},{{Kim, M.J., Woo, S.W., Kim, M.S., Park, J.E., Hwang, J.K. (2014). Anti-Photoaging Effect Of Aaptamine In UVB-Irradiated Human Dermal Fibroblasts And Epidermal Keratinocytes. Journal Of Asian Natural Products Research. 16(12). 1139-1147. Available at: https://doi.org/10.1080/10286020.2014.983092}}
The actions of these molecules can therefore encourage irritation, skin dryness, flakiness, and itchiness. With this in mind, it’s by no coincidence that higher levels of Malassezia have been found in people with more severe dandruff.{{Rudramurthy, S.M., Honnavar, P., Dogra, S., Yegneswaran, P.P., Handa, S., Chakrabarti, A. (2014). Association Of Malassezia Species With Dandruff. Indian J Med Res. 139(3). 431-437. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4069738/}},{{Clavaud, C., Jourdain, R., Bar-Hen, A., Tichit, M., Bouchier, C., Pouradier, F., El Rawadi, C., Guillot, J., Ménard-Szczebara, F., Breton, L., Latgé, J.P., Mouyna, I. (2013). Dandruff Is Associated With Disequilibrium In The Proportion Of The Major Bacterial And Fungal Populations Colonizing The Scalp. PLoS One. 8(3). e58203. Available at: https://doi.org/10.1371/journal.pone.0058203}}
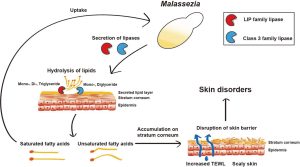
Figure 2: The role of Malassezia in promoting skin disorders (like dandruff). Adapted from Figure 1.{{Park, M., Park, S., Jung, W.H. (2021). Skin Commensal Fungus Malassezia And Its Lipases. J Microbiol Biotechnol. 31(5). 637-644. Available at: https://doi.org/10.4014/jmb.2012.12048}} Image used under the Creative Commons License.
However, it’s not really about the total Malassezia count. It’s about the type of Malassezia species present. For example, counts of Malassezia furfur were found to be the same between people with dandruff and those with healthy scalps.{{Ashbee, H.R., Ingham, E., Holland, K.T., Cunliffe, W.J. (1993). The Carriage Of Malassezia Furfur Serovars A, B And C In Patients With Pityriasis Versicolor, Seborrhoeic Dermatitis And Controls. British Journal Of Dermatology. 129(5). 533-540. Available at: https://doi.org/10.1111/j.1365-2133.1993.tb00480.x}} In contrast, the counts of Malassezia globosa and Malassezia restricta have been found to be higher on scalps with dandruff.{{Dawson, T.L. Jr. (2007). Malassezia Globosa And Restricta: Breakthrough Understanding Of The Etiology And Treatment Of Dandruff And Seborrheic Dermatitis Through Whole-Genome Analysis. J Investig Dermatol Symp Proc. 12(2). 15-19. Available at: https://doi.org/10.1038/sj.jidsymp.5650049}}
The concept of Malassezia as the primary cause of dandruff is supported by the fact that antifungals often work as a treatment, and improvements in dandruff often correlate with lower Malassezia counts.{{Piérard-Franchimont, C., Piérard, G.E., Arrese, J.E., De Doncker, P. (2001). Effect Of Ketoconazole 1% And 2% Shampoos On Severe Dandruff And Seborrhoeic Dermatitis: Clinical, Squamometric And Mycological Assessments. Dermatology. 202(2). 171-176. Available at: https://doi.org/10.1159/000051628}}
So why do some people have these overgrowths of certain Malassezia species, while others don’t? In truth, we are not entirely sure. It could be that:
- Lowered zinc and vitamin D3 levels, which have been correlated with seborrheic dermatitis, prevent healthier Malassezia diversity.{{Aktaş Karabay, E., Aksu Çerman, A. (2019). Serum Zinc Levels In Seborrheic Dermatitis: A Case-Control Study. Turk J Med Sci. 49(5). 1503-1508. Available at: https://doi.org/10.3906/sag-1906-72}},{{Rahimi, S., Nemati, N., Shafaei-Tonekaboni, S.S. (2021). Serum Levels Of 25-Hydroxyvitamin D In Patients With Seborrheic Dermatitis: A Case-Control Study. Dermatol Res Pract. 2021. 6623271. Available at: https://doi.org/10.1155/2021/6623271}}
- Genetic predispositions leave some with a weakened scalp barrier naturally, opening up the possibility of Malassezia overgrowth.{{Borda, L.J., Wikramanayake, T.C. (2015). Seborrheic Dermatitis And Dandruff: A Comprehensive Review. J Clin Investig Dermatol. 3(2). Available at: https://doi.org/10.13188/2373-1044.1000019}}
However, the research so far is limited.
Nutrient Deficiencies
Studies show that deficiencies in vitamin B2, vitamin B3, vitamin B6, and vitamin B7 can cause changes to the skin similar to seborrheic dermatitis and general dermatitis in animals and humans.{{Jen, M., Yan, A.C. (2010). Syndromes Associated With Nutritional Deficiency And Excess. Clinics In Dermatology. 28(6). 669-685. Available at: https://doi.org/10.1016/j.clindermatol.2010.03.029}},{{Stone, O.J. (1989). Pyridoxine Deficiency And Antagonism Produce Increased Ground Substance Viscosity With Resulting Seborrheic Dermatitis And Increased Tumor Resistance. Med Hypotheses. 30(4). 277-280. Available at: https://doi.org/10.1016/0306-9877(89)90037-6}},{{Redzic, S., Hashmi, M.F., Gupta, V. (2023). Niacin Deficiency. StatPearls [Internet]. Available at: https://www.ncbi.nlm.nih.gov/books/NBK557728/}},{{Balnave, D. (1977). Clinical Symptoms Of Biotin Deficiency In Animals. The American Journal Of Clinical Nutrition. 30(9). 1408-1413. Available at: https://doi.org/10.1093/ajcn/30.9.1408}}
We have also established that lowered zinc and vitamin D3 levels have been found in those with seborrheic dermatitis. But could nutrient deficiency be a cause of dandruff, or a consequence of Malassezia overgrowth?
Both of these possibilities are plausible, and, unfortunately, we don’t know the answer to this question either.
A cause? Zinc, for example, has anti-inflammatory properties that can reduce sebum production, improve immune response, and initiate wound repair.{{Demetree, J.W., Safer, L.F., Artis, W.M. (1980). The Effect Of Zinc On The Sebum Secretion Rate. Acta Derm Venereol. 60(2). 166-169. Available at: https://pubmed.ncbi.nlm.nih.gov/6155029/}},{{Lin, P.H., Sermersheim, M., Li, H., Lee, P.H.U., Steinberg, S.M., Ma, J. (2017). Zinc In Wound Healing Modulation. Nutrients. 10(1). 16. Available at: https://doi.org/10.3390/nu10010016}},{{Arribas Lopez, E., Zand, N., Ojo, O., Kochhar, T. (2025). Systematic Review And Meta-Analysis Of The Effect Of Zinc On Wound Healing. BMJ Nutr Prev Health. 8(1). e000952. Available at: https://doi.org/10.1136/bmjnph-2024-000952}},{{Haase, H., Schomburg, L. (2019). You’d Better Zinc-Trace Element Homeostasis In Infection And Inflammation. Nutrients. 11(9). 2078. Available at: https://doi.org/10.3390/nu11092078}} Less sebum means less oleic acid and reactive oxygen species produced by Malassezia. A better immune response means less risk of dandruff-causing infections and a more effective response to irritants.
A consequence? Pathogenic organisms (like Malassezia) are known to compete for nutrients with their host and deplete nutrients at the tissue sites where they grow.{{Bachman, M.A., Weiser, J.N. (2015). Competition For Metals Among Microbes And Their Host. Trace Metals And Infectious Diseases [Internet]. Available at: https://www.ncbi.nlm.nih.gov/books/NBK569680/}},{{Potrykus, J., Ballou, E.R., Childers, D.S., Brown, A.J.P. (2014). Conflicting Interests In The Pathogen–Host Tug Of War: Fungal Micronutrient Scavenging Versus Mammalian Nutritional Immunity. PLoS Pathogens. Available at: https://doi.org/10.1371/journal.ppat.1003910}} The inflammation caused by overgrowth can also increase nutritional demand (to strengthen the immune response).{{Gupta, S., Read, S.A., Shackel, N.A., Hebbard, L., George, J., Ahlenstiel, G. (2019). The Role Of Micronutrients In The Infection And Subsequent Response To Hepatitis C Virus. Cells. 8(6). 603. Available at: https://doi.org/10.3390/cells8060603}},{{Roth-Walter, F., Berni Canani, R., O’Mahony, L., Peroni, D., Sokolowska, M., Vassilopoulou, E., Venter, C. (2024). Nutrition In Chronic Inflammatory Conditions: Bypassing The Mucosal Block For Micronutrients. Allergy. 79(2). 353-383. Available at: https://doi.org/10.1111/all.15972}} This creates a situation where pathogenic organisms cause nutrient deficiencies, while also increasing the requirement for more nutrients.
[ulo_promo title=”All-Natural Hair Supplement + Topical” subtitle=”The top natural ingredients for hair growth, all in one serum & supplement.” description=”Take the next step in your hair growth journey with a world-class natural serum & supplement. Ingredients, doses, & concentrations built by science. ” button_text=”Shop Combo” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/hair-growth-bundle” prescription=”false” type=”otc-combo” ]
Autoimmunity
Autoimmunity is when your body’s defense system mistakenly attacks your own healthy cells, causing inflammation. Since inflammation can produce irritation, this helps explain why autoimmune scalp conditions can sometimes be responsible for dandruff-like symptoms.
Several autoimmune or immune-related conditions can produce dandruff-like conditions:
- Scalp eczema: Known to cause dry, itchy, and irritated skin at the scalp, and is often triggered by genetics, environmental factors (i.e., skin barrier dysfunctions, hypersensitivity to irritants, allergens), or microbial imbalances.{{Magnifico, I., Petronio Petronio, G., Venditti, N., Cutuli, M.A., Pietrangelo, L., Vergalito, F., Mangano, K., Zella, D., Di Marco, R. (2020). Atopic Dermatitis As A Multifactorial Skin Disorder. Can The Analysis Of Pathophysiological Targets Represent The Winning Therapeutic Strategy? Pharmaceuticals (Basel). 13(11). 411. Available at: https://doi.org/10.3390/ph13110411}}
- Scalp psoriasis: A condition characterized by thick, scaly, itchy, or painful patches of skin. It is often triggered by genetics, infections, stress, or injury.{{Armstrong, A.W., Read, C. (2020). Pathophysiology, Clinical Presentation, And Treatment Of Psoriasis: A Review. JAMA. 323(19). 1945-1960. Available at: https://doi.org/10.1001/jama.2020.4006}}
- Scarring alopecia: A disease where the immune system destroys hair follicles, replacing them with scar tissue, causing permanent hair loss often accompanied by severe dandruff-like scales, itching, burning, and pain.{{Lepe, K., Nassereddin, A., Syed, H.A., et al. (2024). Lichen Planopilaris. StatPearls [Internet]. Available at: https://www.ncbi.nlm.nih.gov/books/NBK470325/}}
- Seborrheic dermatitis: This is also a condition that isn’t classed as autoimmune. But, studies show that seborrheic dermatitis can produce specific immune dysregulations, which exaggerate inflammation.{{Navarro Triviño, F.J., Velasco Amador, J.P., Rivera Ruiz, I. (2025). Seborrheic Dermatitis Revisited: Pathophysiology, Diagnosis, And Emerging Therapies-A Narrative Review. Biomedicines. 13(10). 2458. Available at: https://doi.org/10.3390/biomedicines13102458}}

Figure 3: Patient with lichen planopilaris, the most frequent primary scarring alopecia. Adapted from Figure 9.{{Umar, S., Kan, P., Carter, M.J. (2022). Lichen Planopilaris Responsive To A Novel Phytoactive Botanical Treatment: A Case Series. Dermatology And Therapy. 12. 1697-1710. Available at: https://doi.org/10.1007/s13555-022-00749-3}} Image used under the Creative Commons License.
Dandruff-like symptoms caused by autoimmune conditions tend to be more persistent and treatment-resistant than other causes of dandruff. Why? Because the root cause of the problem is an internal, chronic issue. Compared to an external overgrowth of Malassezia, this makes it a lot harder to treat.
Autoimmune diseases that cause dandruff-like symptoms usually arise in genetically susceptible people after a combination of environmental exposures. Contributing factors may include diet, lifestyle (i.e., activity level), or certain environmental triggers (i.e., allergies, an irritating beauty product).
The typical Western diet of processed foods, sugar, and unhealthy fats, in addition to smoking, are two well‑studied examples that can negatively impact the gut microbiome and keep the body in a low‑grade inflammatory state.{{Manzel, A., Muller, D.N., Hafler, D.A., Erdman, S.E., Linker, R.A., Kleinewietfeld, M. (2014). Role Of “Western Diet” In Inflammatory Autoimmune Diseases. Curr Allergy Asthma Rep. 14(1). 404. Available at: https://doi.org/10.1007/s11882-013-0404-6}},{{Perricone, C., Versini, M., Ben-Ami, D., Gertel, S., Watad, A., Segel, M.J., Ceccarelli, F., Conti, F., Cantarini, L., Bogdanos, D.P., Antonelli, A., Amital, H., Valesini, G., Shoenfeld, Y. (2016). Smoke And Autoimmunity: The Fire Behind The Disease. Autoimmunity Reviews. 15(4). 354-374. Available at: https://doi.org/10.1016/j.autrev.2016.01.001}} This makes it easier for the immune system to start attacking the body’s own tissues in vulnerable people.
Does Dandruff Cause Hair Loss?
This is the big question. The short answer is: we’re not sure. Researchers have not yet identified the exact mechanism by which dandruff connects to hair loss.
Having dandruff does not guarantee hair loss, but inflammation associated with dandruff can increase shedding. We do know that there are two hair loss conditions commonly tied to dandruff:
- Telogen effluvium
- Pattern hair loss
Let’s look deeper into the science behind this.
Dandruff and Telogen Effluvium
Telogen effluvium is a condition where there are too many hairs in the telogen phase, causing premature hair shedding. This usually happens after a “negative event”, like high fever, illness, childbirth (postpartum), severe surgical trauma, sudden weight loss, thyroid issues, iron deficiencies, and starting or stopping medication.{{Hussain, N., Agarwala, P., Iqbal, K., et al. (2022). A Systematic Review Of Acute Telogen Effluvium, A Harrowing Post-COVID-19 Manifestation. J Med Virol. 94. 1391-1401. Available at: https://doi.org/10.1002/jmv.27534}},{{Bin Dayel, S., Hussein, R.S., Atia, T., Abahussein, O., Al Yahya, R.S., Elsayed, S.H. (2024). Is Thyroid Dysfunction A Common Cause Of Telogen Effluvium?: A Retrospective Study. Medicine. 103(1). e36803. Available at: https://doi.org/10.1097/MD.0000000000036803}},{{Kang, D.H., Kwon, S.H., Sim, W.Y., Lew, B.L. (2024). Telogen Effluvium Associated With Weight Loss: A Single Center Retrospective Study. Ann Dermatol. 36(6). 384-388. Available at: https://doi.org/10.5021/ad.24.043}}

Figure 4: A patient with telogen effluvium following COVID infection. Adapted from Figure 2.{{Monari, P., Gualdi, G., Bettoni, G., Costa, R., Ragni, G., Zani, F., Bianchi, G., Casella, S., Casella, E., Crippa, M., Calzavara Pinton, P., Di Nicola, M., Porreca, A., Amerio, P., Guizzi, P. (2022). Post-SARS-CoV-2 Acute Telogen Effluvium: An Expected Complication. Journal Of Clinical Medicine. 11(5). 1234. Available at: https://doi.org/10.3390/jcm11051234}} Image used under the Creative Commons License.
Hair growth and shedding are a cycle, and by causing premature shedding, telogen effluvium disrupts this cycle, leaving a gap between when hairs fall out and grow in. The good news is that telogen effluvium is temporary, and when the cause is identified, it can be treated appropriately. Usually, hair shedding stops within 3 to 6 months of removing the trigger, and regrowth will occur over the following 3 to 6 months.{{Malkud, S. (2015). Telogen Effluvium: A Review. J Clin Diagn Res. 9(9). WE01-3. Available at: https://doi.org/10.7860/JCDR/2015/15219.6492}}
Could dandruff be a “negative event”? Studies show that excess dandruff can, in fact, disrupt the hair cycle. This suggests dandruff may be able to trigger telogen effluvium.
The process from dandruff to hair loss could occur like this:
- Microbes like Malassezia and Propionibacterium acnes colonize the scalp and feed on sebum.
- The toxic by-products (like porphyrins) produced by sebum feeding by Malassezia and P. acnes react with UV radiation and increase free radical activity, causing oxidative stress and inflammation at the scalp.
- The body responds to this stress by producing more sebum and accelerating turnover of the scalps outer skin layer, creating more dead skin cells.
- The additional sebum acts as more food for Malassezia and P. acnes, increasing their numbers.
- The cycle repeats as microbial numbers grow, and inflammation increases.
- Eventually, this chronic inflammation causes hairs to shed before completion of the normal growth cycle (telogen effluvium).
Research shows that Malassezia is associated with hair shedding.{{Nematian, J., Ravaghi, M., Gholamrezanezhad, A., Nematian, E. (2006). Increased Hair Shedding May Be Associated With The Presence Of Pityrosporum Ovale. Am J Clin Dermatol. 7(4). 263-266. Available at: https://doi.org/10.2165/00128071-200607040-00008}}
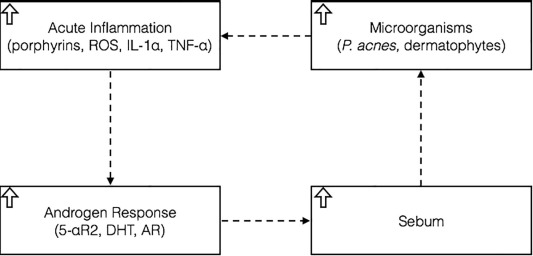
Figure 5: A feedback loop triggering excessive hair shedding. Adapted from Figure 2.{{English, R.S. (2018). A Hypothetical Pathogenesis Model For Androgenic Alopecia: Clarifying The Dihydrotestosterone Paradox And Rate-Limiting Recovery Factors. Medical Hypotheses. 111. 73-81. Available at: https://doi.org/10.1016/j.mehy.2017.12.027}} Image used under the Creative Commons License.
Dandruff and Pattern Hair Loss
Pattern hair loss is not temporary. Known as androgenic alopecia, this is a chronic, progressive hair loss condition that is triggered by genetics, androgen levels, and the scalp environment.{{Chen, S., Li, L., Ding, W., Zhu, Y., Zhou, N. (2025). Androgenetic Alopecia: An Update On Pathogenesis And Pharmacological Treatment. Drug Des Devel Ther. 19. 7349-7363. Available at: https://doi.org/10.2147/DDDT.S542000}}
Pattern hair loss progresses through cycles of hair growth (the anagen phase) and hair rest (the telogen phase), followed by shedding (the exogen phase). However, in each cycle, the anagen phase becomes shorter, and the telogen phase becomes longer. Over time, a progressively finer hair shaft is produced (follicle miniaturization). Hair follicles need to complete shedding before they miniaturize. So in essence, if there is no hair shedding, there is no follicle miniaturization, and androgenic alopecia will not progress.
We’ve discussed how dandruff could trigger telogen effluvium and excess shedding. It’s reasonable, then, to speculate that this excess shedding could also accelerate hair follicle miniaturization in those with androgenic alopecia. More shedding means more hair follicle miniaturization. This hasn’t been demonstrated in research, but it is a plausible scenario.
For diffuse alopecia conditions (like telogen effluvium), studies show that there is a positive correlation between dandruff severity and the number of hairs in the telogen phase.{{Piérard-Franchimont, C., Xhauflaire-Uhoda, E., Loussouarn, G., Saint Léger, D., Piérard, G.E. (2006). Dandruff-Associated Smouldering Alopecia: A Chronobiological Assessment Over 5 Years. Clin Exp Dermatol. 31(1). 23-26. Available at: https://doi.org/10.1111/j.1365-2230.2005.02026.x}} Perhaps dandruff could also exacerbate telogen phase lengthening caused by androgenic alopecia as well.
So while dandruff does not cause androgenic alopecia, it could exaggerate hair loss caused by this condition, and so addressing any dandruff or inflammation is crucial to support better regrowth outcomes when treating this condition.
Why Resolving Scalp Inflammation Matters for Hair Growth Treatments
There are several FDA-approved treatments for androgenic alopecia. However, inflammation at the scalp could stop these treatments from working effectively.
In a study of 64 men with androgenic alopecia, low-light laser therapy (LLLT) was found to reduce inflammatory molecules at the scalp. Subsequent use of LLLT before 2% minoxidil was found to boost hair regrowth similar to use of 5% minoxidil.{{Mahe, Y.F., Cheniti, A., Tacheau, C., Antonelli, R., Planard-Luong, L., de Bernard, S., Buffat, L., Barbarat, P., Kanoun-Copy, L. (2021). Low-Level Light Therapy Downregulates Scalp Inflammatory Biomarkers In Men With Androgenetic Alopecia And Boosts Minoxidil 2% To Bring A Sustainable Hair Regrowth Activity. Lasers Surg Med. 53. 1208-1219. Available at: https://doi.org/10.1002/lsm.23398}} The result was just a correlation (i.e., other factors could have boosted hair regrowth other than reduced inflammation), but suggests a link between lowered inflammation markers and improved hair regrowth outcomes.
This evidence suggests that if you are looking for hair loss treatments and you have dandruff or an inflamed scalp, don’t ignore it! It’s important to treat dandruff and inflammation first, or alongside regrowth regimens.
Identify Your Dandruff Driver
Knowing the cause of your dandruff is the first step in choosing the right treatment.
Do you experience:
- Small, white, powdery, and dry flakes?
- A scalp that feels tight, itchy, and dry?
Likely cause: Dehydrated scalp
Do you experience:
- Large, yellow or white flakes that feel greasy or waxy?
- A scalp feels greasy quickly, and oily hair?
- Intense itching, redness, or scaly patches?
Likely cause: Too much sebum and microbial overgrowth
Do you experience:
- Persistent redness on the scalp?
- Persistent pain in the scalp area?
- Persistent “dandruff” that doesn’t resolve with the use of shampoos?
Likely cause: An underlying autoimmune condition
But you shouldn’t self-diagnose. Speak with a dermatologist if you are experiencing dandruff or dandruff-like symptoms. A healthcare professional can often diagnose dandruff simply by looking at your hair and scalp, and may be able to advise on possible causes.
Treatments That Could Work
Once you’ve identified the likely culprit of your dandruff, you can now seek out the most appropriate treatments. We’ll walk through the different types of treatments available for each cause of dandruff.
For Microorganism-Driven Dandruff
When dandruff is driven by the overgrowth of microorganisms, the aim is to lower the levels of these organisms on the scalp and make it a less hospitable place for them to grow. There are several products available to support this mission.
Zinc pyrithione 1% shampoo
Zinc pyrithione is a potent antimicrobial and antifungal agent. It is a very common ingredient in shampoos targeted at dandruff, like Head & Shoulders products.
Figure 6: Head & Shoulders shampoo containing zinc pyrithione.
Zinc pyrithione acts in three key ways to disrupt microbial growth:
- It increases the zinc levels and copper levels within individual cells of microbes, like Malassezia, which can damage the structure and formation of iron-sulphur clusters.{{Park, M., Cho, Y.J., Lee, Y.W., Jung, W.H. (2018). Understanding The Mechanism Of Action Of The Anti-Dandruff Agent Zinc Pyrithione Against Malassezia Restricta. Sci Rep. 8(1). 12086. Available at: https://doi.org/10.1038/s41598-018-30588-2}},{{Reeder, N.L., Xu, J., Youngquist, R.S., Schwartz, J.R., Rust, R.C., Saunders, C.W. (2011). The Antifungal Mechanism Of Action Of Zinc Pyrithione. Br J Dermatol. 165 Suppl 2. 9-12. Available at: https://doi.org/10.1111/j.1365-2133.2011.10571.x}}
- In addition to damaging iron-sulphur clusters, it disrupts the synthesis process for iron-sulphur clusters.{{Park, M., Cho, Y.J., Lee, Y.W., Jung, W.H. (2018). Understanding The Mechanism Of Action Of The Anti-Dandruff Agent Zinc Pyrithione Against Malassezia Restricta. Sci Rep. 8(1). 12086. Available at: https://doi.org/10.1038/s41598-018-30588-2}}
- It disrupts the production of lipid-eating enzymes (like those needed to “eat” sebum).{{Park, M., Cho, Y.J., Lee, Y.W., Jung, W.H. (2018). Understanding The Mechanism Of Action Of The Anti-Dandruff Agent Zinc Pyrithione Against Malassezia Restricta. Sci Rep. 8(1). 12086. Available at: https://doi.org/10.1038/s41598-018-30588-2}}
Why is this important? Iron-sulphur clusters are contained within mitochondria, the “powerhouse of the cell”. Iron-sulphur clusters, alongside other cellular components, are needed to produce energy from mitochondria. Without energy, the microbes can not grow or survive.
The clinical evidence shows that zinc pyrithione is effective against dandruff and may even support hair regrowth, possibly by supporting a healthier scalp environment.
Study Subjects and Treatment Outcome Notes Marks et al. 1985.{{Marks, R., Pearse, A.D., Walker, A.P. (1985). The Effects Of A Shampoo Containing Zinc Pyrithione On The Control Of Dandruff. Br J Dermatol. 112(4). 415-422. Available at: https://doi.org/10.1111/j.1365-2133.1985.tb02314.x}} 32 subjects with dandruff, one half of the head was washed with 1% zinc pyrithione and the other half without. Progressive reduction in dandruff on the side of the head washed with zinc pyrithione, and the difference between the placebo side was statistically significant. Small subject number, but results suggest a positive influence that may be generalizable to larger groups. Berger et al. 2003.{{Berger, R.S., Fu, J.L., Smiles, K.A., Turner, C.B., Schnell, B.M., Werchowski, K.M., Lammers, K.M. (2003). The Effects Of Minoxidil, 1% Pyrithione Zinc And A Combination Of Both On Hair Density: A Randomized Controlled Trial. Br J Dermatol. 149(2). 354-362. Available at: https://doi.org/10.1046/j.1365-2133.2003.05435.x}} 200 men with Hamilton-Norwood type III vertex or type IV baldness, treated with either 1% zinc pyrithione, 5% minoxidil, or a combination of both. Minoxidil produced the most substantial outcome, but all treatments resulted in a significant increase in hair counts. The benefit of the 1% pyrithione zinc shampoo used alone tended to be apparent only to the investigator, users did not notice a cosmetic change. Schwartz et al. 2013.{{Schwartz, J.R., Bacon, R.A., Shah, R., Mizoguchi, H., Tosti, A. (2013). Therapeutic Efficacy Of Anti-Dandruff Shampoos: A Randomized Clinical Trial Comparing Products Based On Potentiated Zinc Pyrithione And Zinc Pyrithione/Climbazole. Int J Cosmet Sci. 35(4). 381-387. Available at: https://doi.org/10.1111/ics.12055}} 620 subjects with scalp flaking, treated with either a “potentiated” zinc pyrithione (a formula that maximizes delivery of zinc pyrithione at the scalp), or a dual-active shampoo containing zinc pyrithione and another antifungal, climbazole Potentiated zinc pyrithione was more effective than the dual-active shampoo at reducing flaking. The treatment was used for 4 weeks, so only short-term benefits can be seen here. Zinc pyrithione shampoos are widely available. You should be able to purchase this shampoo easily over-the-counter at any pharmacy or supermarket.
Ketoconazole 1% or 2% shampoo
Ketoconazole is another antifungal medication. Ketoconazole shampoo is often recommended in conjunction with hair loss products, such as minoxidil or finasteride. This is because it doesn’t just help reduce dandruff, it can also reduce androgens at the scalp, which drive androgenic alopecia.
Ketoconazole fights pathogenic scalp microbes in two key ways:
- It blocks the production of a lipid needed to maintain the outer structure (cell wall) of fungi cells, which ultimately damages them.{{Tynes, B.E., Johnson, C.D., Vaish, M.H., Abbott, B., Vučenović, J., Varrassi, G., Potharaju, P., Lopez Torres, Y., Lee, Z., Ahmadzadeh, S., Shekoohi, S., Kaye, A.D. (2024). Ketoconazole Shampoo For Seborrheic Dermatitis Of The Scalp: A Narrative Review. Cureus. 16(8). e67532. Available at: https://doi.org/10.7759/cureus.67532}}
- It changes the lipids present on the scalp, and reduces sebum production, both of which block the “food” available for Malassezia overgrowth and promote the growth of more friendly microbes.{{Goularte-Silva, V., Paulino, L.C. (2022). Ketoconazole Beyond Antifungal Activity: Bioinformatics-Based Hypothesis On Lipid Metabolism In Dandruff And Seborrheic Dermatitis. Exp Dermatol. 31. 821-822. Available at: https://doi.org/10.1111/exd.14505}}
Like zinc pyrithione, the clinical evidence for ketoconazole shows that it is an effective treatment against dandruff, with 2% ketoconazole having the greatest impact.
Study Subjects and Treatment Outcome Notes Piérard-Franchimont et al. 2001.{{Piérard-Franchimont, C., Piérard, G.E., Arrese, J.E., De Doncker, P. (2001). Effect Of Ketoconazole 1% And 2% Shampoos On Severe Dandruff And Seborrhoeic Dermatitis: Clinical, Squamometric And Mycological Assessments. Dermatology. 202(2). 171-176. Available at: https://doi.org/10.1159/000051628}} 66 subjects with severe dandruff or seborrhoeic dermatitis, treated with either 1% ketoconazole or 2% ketoconazole Both resulted in clear benefits, but flakiness, Malassezia count, and dandruff score were reduced more with 2% ketoconazo le compared to 1% ketoconazole.
Treatment lasted only 4 weeks. Longer trials are needed to determine whether this is a long-term solution. Also, the results may not be relevant to milder cases. Piérard-Franchimont et al. 2002.{{Piérard-Franchimont, C., Goffin, V., Decroix, J., Piérard, G.E. (2002). A Multicenter Randomized Trial Of Ketoconazole 2% And Zinc Pyrithione 1% Shampoos In Severe Dandruff And Seborrheic Dermatitis. Skin Pharmacol Appl Skin Physiol. 15(6). 434-441. Available at: https://doi.org/10.1159/000066452}} 331 subjects with severe dandruff or seborrhoeic dermatitis, treated with either 1% ketoconazole or 2% ketoconazole Both treatments resulted in clear benefits, but the benefits were greater with 2% ketoconazole. There was a 73% improvement in total dandruff severity score with 2% ketoconazole, and instances of disease reccurrence was fewer. Treatment lasted only 4 weeks. Longer trials are needed to determine whether this is a long-term solution. Also, the results may not be relevant to milder cases. Lorette and Ermosilla 2006.{{Lorette, G., Ermosilla, V. (2006). Clinical Efficacy Of A New Ciclopiroxolamine/Zinc Pyrithione Shampoo In Scalp Seborrheic Dermatitis Treatment. Eur J Dermatol. 16(5). Available at: https://pubmed.ncbi.nlm.nih.gov/17101479/}} 189 subjects with seborrheic dermatitis, treated with either 1.5% ciclopiroxolamine and 1% zinc pyrithione, or 2% ketoconazole All treatments reduced itching, redness, and inflammation, and it was found that both treatments were efficient in treating seborrheic dermatitis. Whether the results are relevant to “true” dandruff cases and cases of milder dandruff is unclear. Ketoconazole at 1% is available over-the-counter, but 2% requires a prescription. If you have mild to moderate dandruff, try 1% zinc pyrithione or 1% ketoconazole shampoo first. If you don’t see results or have more severe dandruff, contact your physician to see whether you can escalate to 2% ketoconzole.
Tea tree oil 5% shampoo
For those who seek out more natural remedies, tea tree oil is a widely used ingredient for treating dandruff naturally. It can be found in shampoos, conditioners, scalp oils, hair masks, lotions, and many other products of this sort.
Tea tree oil contains a compound known as terpinen-4-ol. This compound can disrupt the cell membrane of fungal cells, which disrupts their growth and ability to replicate.{{Yu, D., Wang, J., Shao, X., Xu, F., Wang, H. (2015). Antifungal Modes Of Action Of Tea Tree Oil And Its Two Characteristic Components Against Botrytis Cinerea. J Appl Microbiol. 119(5). 1253-1262. Available at: https://doi.org/10.1111/jam.12939}}
Unlike zinc pyrithione or ketoconazole, there is only one study supporting the use of tea tree oil against dandruff. However, it’s a well-designed study, so the validity of the conclusions are strong.
In this randomized, single-blind, and controlled study, 126 subjects with mild to moderate dandruff were treated either with 5% tree tea oil shampoo or a placebo. After 4 weeks, areas of the scalp showed a 41% improvement in severity score with 5% tea tree oil, while just a 11% improvement in the placebo group. Itchiness and greasiness were also significantly reduced with the 5% tea tree oil shampoo.{{Satchell, A.C., Saurajen, A., Bell, C., Barnetson, R.S. (2002). Treatment Of Dandruff With 5% Tea Tree Oil Shampoo. J Am Acad Dermatol. 47(6). 852-855. Available at: https://doi.org/10.1067/mjd.2002.122734}}
If you’re interested in trying tea tree oil as a natural solution to dandruff, you can find it at many pharmacies or online, but just make sure the concentration (5%) is clearly stated on the label!
Black seed oil 0.5% topical
Black cumin seed oil, also known as Nigella sativa, is a “trending” ingredient that you may see touted for its anti-aging properties. For dandruff, black cumin seed oil is not known to inhibit the growth of Malassezia like the other products in this list. Instead, it may:
- Reduce inflammation through its active component, thymoquinone.{{Amin, B., Hosseinzadeh, H. (2016). Black Cumin (Nigella sativa) and Its Active Constituent, Thymoquinone: An Overview on the Analgesic and Anti-inflammatory Effects. Planta Medica 82(01/02):8-16. Available at: 10.1055/s-0035-1557838}},{{Arshad, M.T., Maqsood, S., Ikram, A., Abdullahi, M.A. (2025). Functional, Nutraceutical, And Pharmacological Properties Of Black Seed. Food Science & Nutrition. 13(8). e70725. Available at: https://doi.org/10.1002/fsn3.70725}}
- Support a stronger skin barrier by delivering linoleic acid to the scalp, which stimulates ceramide synthesis (a key skin barrier lipid), thus reducing the impact of inflammatory molecules and microbes.{{Rahim, M.A., Shoukat, A., Khalid, W., Ejaz, A., Itrat, N., Majeed, I., Koraqi, H., Imran, M., Nisa, M.U., Nazir, A., Alansari, W.S., Eskandrani, A.A., Shamlan, G., Al-Farga, A. (2022). A Narrative Review On Various Oil Extraction Methods, Encapsulation Processes, Fatty Acid Profiles, Oxidative Stability, And Medicinal Properties Of Black Seed (Nigella Sativa). Foods. 11(18). 2826. Available at: https://doi.org/10.3390/foods11182826}},{{Coderch, L., López, O., de la Maza, A., Parra, J.L. (2003). Ceramides And Skin Function. Am J Clin Dermatol. 4(2). 107-129. Available at: https://doi.org/10.2165/00128071-200304020-00004}}
These effects counteract the adverse actions of Malassezia.
Unfortunately, there haven’t been any clinical trials testing the effect of black seed oil on subjects with dandruff. But, a randomized, double-blinded pilot study of 20 people with telogen effluvium suggested that this oil could reduce inflammation and hair shedding.{{Rossi, A., Priolo, L., Iorio, A., Vescarelli, E., Gerardi, M., Campo, D., Nunno, D.D., Ceccarelli, S., Calvieri, S., Angeloni, A., Marchese, C. (2013). Evaluation Of A Therapeutic Alternative For Telogen Effluvium: A Pilot Study. Journal Of Cosmetics, Dermatological Sciences And Applications. 2013. 9-16. Available at: https://file.scirp.org/pdf/JCDSA_2013081513583870.pdf}}
In the study, subjects were treated either with a topical product containing 0.5% black seed oil and 0.4% lavender oil, or a placebo with only 0.4% lavender oil. After 6 months, the following results were found:
- 90% of subjects using the 0.5% black seed oil and 0.4% lavender oil topical saw an increase in the number of hairs, while 60% of those using the placebo continued to lose hair
- Hair density significantly increased in 70% of subjects using the 0.5% black seed oil and 0.4% lavender oil topical, but only 30% in those using the placebo
- Subjects with scalp inflammation using the 0.5% black seed oil and 0.4% lavender oil topical were found to have total regression of their scalp inflammation, while none of the subjects with inflammation using the placebo saw any resolution to their inflammation
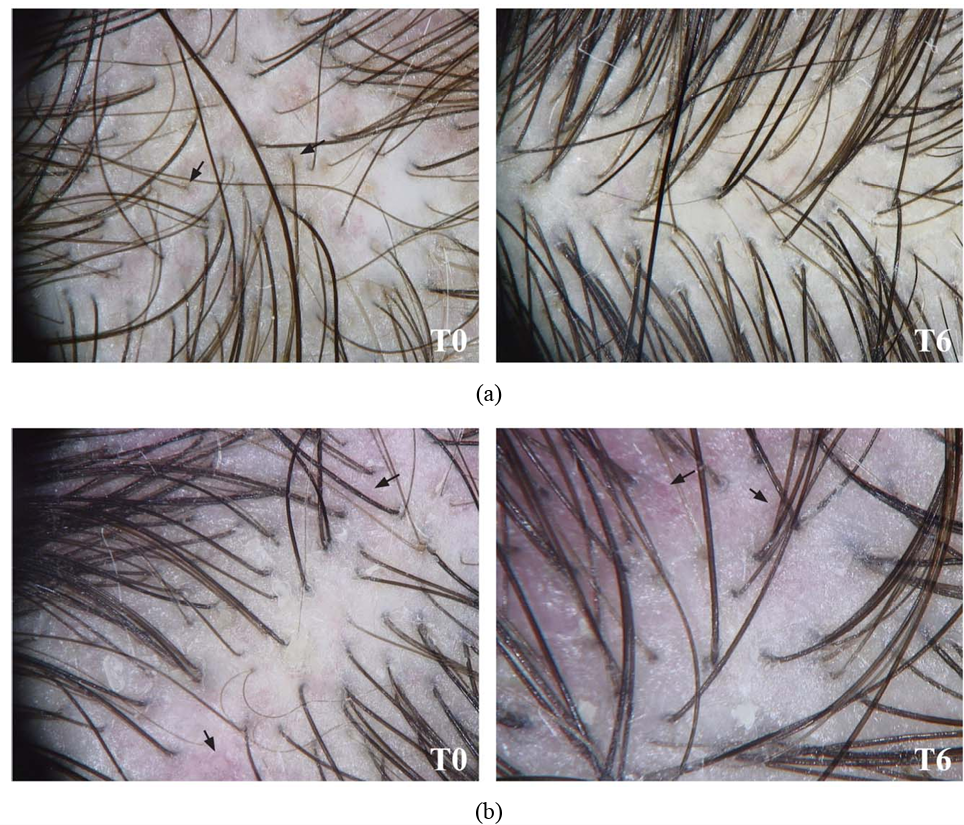
Figure 7: Scalp inflammation at baseline (T0) and after 6 months of treatment (T6) with either black seed oil (a) or a placebo (b). Patients treated with the placebo showed persistent scalp inflammation. Adapted from Figure 2.{{Rossi, A., Priolo, L., Iorio, A., Vescarelli, E., Gerardi, M., Campo, D., Nunno, D.D., Ceccarelli, S., Calvieri, S., Angeloni, A., Marchese, C. (2013). Evaluation Of A Therapeutic Alternative For Telogen Effluvium: A Pilot Study. Journal Of Cosmetics, Dermatological Sciences And Applications. 2013. 9-16. Available at:https://file.scirp.org/pdf/JCDSA_2013081513583870.pdf}} Image used under the Creative Commons License.
We know that Malassezia causes inflammation, and that inflammation is related to hair loss, so by counteracting these effects, black seed oil could be an effective addition to any anti-dandruff regimen, or even any anti-hair shedding regimen.
Because the active ingredient is thymoquinone, using black seed oil for dandruff and hair loss is less about the concentration of the black seed oil and more about the overall thymoquinone content in the formula. Since black seed oil is well-tolerated, you could probably go higher than 0.5% and make your own formula at a concentration of 2-5%. This will increase the likelihood that you’re getting enough of this anti-inflammatory compound.
For Nutrient-Linked Dandruff
If your dandruff is due to nutrient deficiencies, the obvious answer is to supplement your diet with foods that contain these missing vitamins, or alternatively look towards taking daily supplements.
We know that those with seborrheic dermatitis have been found with lowered levels of B vitamins, as well as vitamin D3 and zinc.{{Aktaş Karabay, E., Aksu Çerman, A. (2019). Serum Zinc Levels In Seborrheic Dermatitis: A Case-Control Study. Turk J Med Sci. 49(5). 1503-1508. Available at: https://doi.org/10.3906/sag-1906-72}},{{Rahimi, S., Nemati, N., Shafaei-Tonekaboni, S.S. (2021). Serum Levels Of 25-Hydroxyvitamin D In Patients With Seborrheic Dermatitis: A Case-Control Study. Dermatol Res Pract. 2021. 6623271. Available at: https://doi.org/10.1155/2021/6623271}},{{Jen, M., Yan, A.C. (2010). Syndromes Associated With Nutritional Deficiency And Excess. Clinics In Dermatology. 28(6). 669-685. Available at: https://doi.org/10.1016/j.clindermatol.2010.03.029}},{{Stone, O.J. (1989). Pyridoxine Deficiency And Antagonism Produce Increased Ground Substance Viscosity With Resulting Seborrheic Dermatitis And Increased Tumor Resistance. Med Hypotheses. 30(4). 277-280. Available at: https://doi.org/10.1016/0306-9877(89)90037-6}},{{Redzic, S., Hashmi, M.F., Gupta, V. (2023). Niacin Deficiency. StatPearls [Internet]. Available at: https://www.ncbi.nlm.nih.gov/books/NBK557728/}},{{Balnave, D. (1977). Clinical Symptoms Of Biotin Deficiency In Animals. The American Journal Of Clinical Nutrition. 30(9). 1408-1413. Available at: https://doi.org/10.1093/ajcn/30.9.1408}}
There is no clinical evidence to show that supplementation will treat dandruff in those who are nutrient-deficient. However, there is evidence to show that nutrient supplementation can reverse adverse effects in those who are nutrient-deficient.
For example, biotin deficiency is a cause of hair thinning in women who are biotin-deficient. The supplementation of biotin to biotin-deficient individuals has been found to restore hair growth.{{Patel, D.P., Swink, S.M., Castelo-Soccio, L. (2017). A Review Of The Use Of Biotin For Hair Loss. Skin Appendage Disord. 3(3). 166-169. Available at: https://doi.org/10.1159/000462981}} So, it stands to reason that vitamin supplementation may also support the reduction or elimination of dandruff if this is the cause.
If you’re interested in learning more about the connection between nutrient deficiencies and hair loss, read our article here.
For Autoimmune and Inflammatory Dandruff
Unfortunately, if you think you might have dandruff caused by an autoimmune disorder, this is a lot harder to treat. The problem is internal, not just at the surface of the scalp, and the cause of an autoimmune disorder can be both complex and very personal.
Autoimmune disorders are often treated with immunosuppressive drugs. But you can also look at altering your diet, lifestyle, or environment to support a journey back to normalcy.
- Diet: Maintain a diet high in nutrients, and minimize exposure to any food allergens.{{Mazzucca, C.B., Raineri, D., Cappellano, G., Chiocchetti, A. (2021). How To Tackle The Relationship Between Autoimmune Diseases And Diet: Well Begun Is Half-Done. Nutrients. 13(11). 3956. Available at: https://doi.org/10.3390/nu13113956}} An elimination diet can work well to see which foods may be causing dandruff for you – eliminate a food from your diet for a few weeks and record the results. Blood tests can reveal nutrients that you might be deficient in, but a visit to your doctor may be needed to rule out malabsorption or other disease states causing nutrient deficiency.
- Lifestyle: Incorporate low-grade physical activity into your daily routine, ensure you are having regular sunlight exposure (for vitamin D!), and try to have consistent, high-quality sleep.{{Blank, M., Israeli, D., Shoenfeld, Y. (2024). Exercise, Autoimmune Diseases And T-Regulatory Cells. Journal Of Autoimmunity. 149. 103317. Available at: https://doi.org/10.1016/j.jaut.2024.103317}},{{Yang, C.Y., Leung, P.S.C., Adamopoulos, I.E. (2013). The Implication Of Vitamin D And Autoimmunity: A Comprehensive Review. Clinical Reviews In Allergy And Immunology. 45. 217-226. Available at: https://doi.org/10.1007/s12016-013-8361-3}},{{Hsiao, Y.H., Chen, Y.T., Tseng, C.M., Wu, L.A., Lin, W.C., Su, V.Y.F., Perng, D.W., Chang, S.C., Chen, Y.M., Chen, T.J., Lee, Y.C., Chou, K.T. (2015). Sleep Disorders And Increased Risk Of Autoimmune Diseases In Individuals Without Sleep Apnea. Sleep. 38(4). 581-586. Available at: https://doi.org/10.5665/sleep.4574}}
- Environment: Reduce your exposure to environmental toxins, like heavy metals, plastic chemicals, and persistent organic pollutants like dioxins and polychlorinated biphenyls, triclosan, and food colorings. Foreign substances like this can increase susceptibility to autoimmune diseases.{{Pollard, K.M., Christy, J.M., Cauvi, D.M., Kono, D.H. (2018). Environmental Xenobiotic Exposure And Autoimmunity. Current Opinion In Toxicology. 10. 15-22. Available at: https://doi.org/10.1016/j.cotox.2017.11.009}} You can test for “toxic overload” using blood tests, and can even test your hair for heavy metals to assess your current toxin exposure.
Autoimmune disorders can affect your quality of life. If you think you might have an autoimmune or inflammatory disorder, speak with your physician to discuss suitable treatment routes.
What to Avoid If You Have Dandruff
#1 – Oleic acid
Organisms like Malassezia and P. acnes can break down sebum and produce oleic acid, which we have established can be harmful to the skin barrier. This lipid is not only harmful but can also encourage the growth of microorganisms like these, so it follows that those with dandruff should avoid any topical products containing oleic acid.{{Trompezinski, S., Weber, S., Cadars, B., Larue, F., Ardiet, N., Chavagnac-Bonneville, M., Sayag, M., Jourdan, E. (2016). Assessment Of A New Biological Complex Efficacy On Dysseborrhea, Inflammation, And Propionibacterium Acnes Proliferation. Clinical, Cosmetic And Investigational Dermatology. 9. 233-239. Available at: https://doi.org/10.2147/CCID.S110655}}
Oleic acid can be found naturally in vegetable oils (i.e., olive oil, corn oil, canola oil, avocado oil) and animal fats (i.e., tallow and lard), but you don’t have to avoid eating oleic acid if you have dandruff. There is no evidence to suggest eating oleic acid causes more oleic acid at the scalp, and in fact studies show that eating oleic acid can reduce inflammation and reduce the activity of stearoyl-CoA desaturase (the enzyme that produces oleic acid in the body).{{Wang, Q., Liu, R., Chang, M., Zhang, H., Jin, Q., Wang, X. (2022). Dietary Oleic Acid Supplementation And Blood Inflammatory Markers: A Systematic Review And Meta-Analysis Of Randomized Controlled Trials. Critical Reviews In Food Science And Nutrition. 62(9). 2508-2525. Available at: https://doi.org/10.1080/10408398.2020.1854673}},{{Dobrzyn, P., Pyrkowska, A., Jazurek, M., Dobrzyn, A. (2012). Increased Availability Of Endogenous And Dietary Oleic Acid Contributes To The Upregulation Of Cardiac Fatty Acid Oxidation. Mitochondrion. 12(1). 132-137. Available at: https://doi.org/10.1016/j.mito.2011.05.007}}
#2 – Allergenic foods
For autoimmune-prone individuals, there may be a particular source driving seborrheic dermatitis, eczema, or scalp psoriasis. In these cases, it may be worthwhile to review your dietary choices and try to determine any potential causes. Anecdotally, several people we have worked with have reported that dietary overhauls (including the elimination of gluten, dairy, and seed oils) significantly improved their dandruff problems.
What If My Dandruff Is Resistant to Treatment?
PHH members with treatment-resistant dandruff have reported success when rotating shampoos with different active ingredients.
An example rotation may look like this:
2% ketoconazole (2-3 days) → selenium sulfide (2-3 days) → coal tar (2-3 days) → zinc pyrithione (2-3 days) → 2% ketoconazole (2-3 days)…
Rotating treatments like these can be effective because each active ingredient targets dandruff in a distinct way, creating a more comprehensive approach to addressing its underlying causes:
- Ketoconazole: Fights pathogenic scalp microbes by inhibiting fungal cell wall synthesis.{{Borda, L.J., Wikramanayake, T.C. (2015). Seborrheic Dermatitis And Dandruff: A Comprehensive Review. Journal Of Clinical And Investigative Dermatology. 3(2). 10.13188/2373-1044.1000019. Available at: https://doi.org/10.13188/2373-1044.1000019}},{{Koc, E., Arca, E., Kose, O., Akar, A. (2009). An Open, Randomized, Prospective, Comparative Study Of Topical Pimecrolimus 1% Cream And Topical Ketoconazole 2% Cream In The Treatment Of Seborrheic Dermatitis. Journal Of Dermatological Treatment. 20(1). 4-9. Available at: https://doi.org/10.1080/09546630802286993}}
- Selenium sulfide: Stops the growth and proliferation of cells, and is also keratolytic – it exfoliates the outer layer of skin by breaking down keratin.{{Borda, L.J., Wikramanayake, T.C. (2015). Seborrheic Dermatitis And Dandruff: A Comprehensive Review. Journal Of Clinical And Investigative Dermatology. 3(2). 10.13188/2373-1044.1000019. Available at: https://doi.org/10.13188/2373-1044.1000019}},{{Danby, F.W., Maddin, W.S., Margesson, L.J., Rosenthal, D. (1993). A Randomized, Double-Blind, Placebo-Controlled Trial Of Ketoconazole 2% Shampoo Versus Selenium Sulfide 2.5% Shampoo In The Treatment Of Moderate To Severe Dandruff. Journal Of The American Academy Of Dermatology. 29(6). 1008-1012. Available at: https://doi.org/10.1016/0190-9622(93)70282-X}}
- Coal tar: This is an anti-fungal, anti-inflammatory, and keratolytic compound that can also reduce sebum production.{{Borda, L.J., Wikramanayake, T.C. (2015). Seborrheic Dermatitis And Dandruff: A Comprehensive Review. Journal Of Clinical And Investigative Dermatology. 3(2). 10.13188/2373-1044.1000019. Available at: https://doi.org/10.13188/2373-1044.1000019}},{{Davies, D., Boorman, G.C., Shuttleworth, D. (1999). Comparative Efficacy Of Shampoos Containing Coal Tar (4.0% W/W; TarmedTM), Coal Tar (4.0% W/W) Plus Ciclopirox Olamine (1.0% W/W; TarmedTM AF) And Ketoconazole (2.0% W/W; NizoralTM) For The Treatment Of Dandruff/Seborrhoeic Dermatitis. Journal Of Dermatological Treatment. 10(3). 177-183. Available at: https://doi.org/10.3109/09546639909056025}}
- Zinc pyrithione: Interferes with iron-sulfur proteins and energy metabolism in microbes.{{Borda, L.J., Wikramanayake, T.C. (2015). Seborrheic Dermatitis And Dandruff: A Comprehensive Review. Journal Of Clinical And Investigative Dermatology. 3(2). 10.13188/2373-1044.1000019. Available at: https://doi.org/10.13188/2373-1044.1000019}},{{Reeder, N.L., Xu, J., Youngquist, R.S., Schwartz, J.R., Rust, R.C., Saunders, C.W. (2011). The Antifungal Mechanism Of Action Of Zinc Pyrithione. Br J Dermatol. 165 Suppl 2. 9-12. Available at: https://doi.org/10.1111/j.1365-2133.2011.10571.x}}
Final Remarks
Dandruff is a multifactorial condition influenced by microbes, the skin barrier, nutrition, and immune activity. Although it does not directly cause permanent hair loss, the inflammation and scalp imbalance associated with dandruff can increase shedding and potentially accelerate pattern hair loss in susceptible individuals. Encouragingly, addressing dandruff often improves overall scalp health and may enhance the effectiveness of hair growth treatments. The most successful strategy is to first identify the underlying driver of dandruff, whether it be microbial, nutritional, or inflammatory, and then select the most appropriate treatment. By doing this, you can build a healthier scalp environment that can support normal hair cycling, and hopefully stronger hair regrowth as well, over time.
Finasteride is among the most effective drugs for androgenic alopecia. And while side effects are often overstated, it can lead to reduced libido or lowered sperm counts in some men. For this reason, many choose topical versus oral finasteride, hoping to limit the drug’s DHT-reducing effects to the scalp. But at certain doses, even topical finasteride can become systemic. So, to minimize side effects, which finasteride dosage, formula and application is best?
In this article, we’ll review
- About oral versus topical finasteride
- Why topical finasteride can still go systemic
- Why choosing the lowest percentage solution isn’t the only answer
- How to maximize finasteride gains, while minimizing side effects
[ulo_promo title=”Interested in Topical Finasteride?” subtitle=”Low-dose & full-strength finasteride available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-finasteride?variant=42249746186319″ prescription=”true”]
About Finasteride
Finasteride, also known under the brand name Propecia or Proscar, is a prescription medication approved by the FDA for the treatment of androgenic alopecia (AGA). The anti-androgen works by reducing the production of Dihydrotestosterone (DHT), a hormone linked to pattern hair loss. In use since 1992, Finasteride is among the most powerful and well-studied drugs for hair loss.
Oral Finasteride
Oral finasteride stops AGA progression in 80-90% of men and, on average, leads to a 10% increase in hair count over two years.{{https://www.sciencedirect.com/science/article/pii/S0022202X15529357}} For men wanting a “hands-off” approach to hair maintenance, oral finasteride can be an excellent option. With a once-daily pill, it’s expected that hair loss will stop at approximately 6 months, and thereafter, improve.
However, oral finasteride isn’t for everyone. While the risk of side effects are often overstated online, the drug appears to reduce libido in a certain percentage of men. Oral finasteride can also temporarily lower sperm counts, which might make conception more difficult during its first six months of use. In some men, the use of finasteride appears to increase anxiety and/or depression. While the true incidence and magnitude of these reports are hard to discern, it’s understandable that many are weary of taking this once daily pill.
Fortunately, recent improvements in finasteride’s delivery may mean we no longer need to throw the proverbial baby out with the bathwater.
Topical Finasteride
The biggest reason people seek out topical finasteride (instead of oral finasteride) is because they want to minimize systemic exposure to the drug, and in doing so, localize finasteride’s effects to the scalp.
While research is still in the early stages, evidence suggests that topical finasteride can produce similar levels of hair regrowth compared to oral finasteride, with a significantly reduced incidence of side effects.
Topical finasteride works identically to its oral counterpart: by inhibiting the type II 5-alpha reductase enzyme to reduce DHT. It is designed to target scalp DHT instead of systemic DHT levels.
However, limiting finasteride’s reach to scalp, not serum, DHT is harder than perhaps anticipated. To understand why, let’s take a closer look at scalp versus serum DHT.
Serum vs Scalp DHT
There’s a lot of evidence that the hormone DHT is directly implicated in androgenic alopecia. In fact, research directly links DHT to all three of AGA’s defining characteristics:
- Increased telogen:anagen ratio. DHT’s influence on DKK-1 expression increases hair shedding
- Increased anagen cycling. DHT’s effects on signaling pathways limit the growth phase of hairs
- Hair follicle miniaturization. DHT’s effects on dermal papilla sizing thins hair with each cycle
There are a wide variety of DHT reducers available, including prescription drugs, over-the-counter products, intradermal injections, and even herbal supplements. Finasteride reduces DHT in two ways.
- Oral finasteride reduces DHT everywhere in the body. Beyond just the scalp, it reduces DHT in the blood, brain, and prostate.
- Topical finasteride attempts to reduce DHT only where it is applied – in the scalp – with minimal effects on DHT levels elsewhere.
However, it’s far easier than most realize for topical finasteride to go systemic. And when it does, it potentially reduces DHT everywhere – leading to the very side effects it’s meant to prevent.
Topical Finasteride Can Still Go Systemic
Why? When it comes to lowering DHT (the goal of the drug), finasteride has a highly-sensitive, dose-dependent response curve. This means that while 0.01 mg of finasteride barely reduces any DHT at all, 0.1 mg reduces almost as much DHT as 5 mg, a much larger dose.
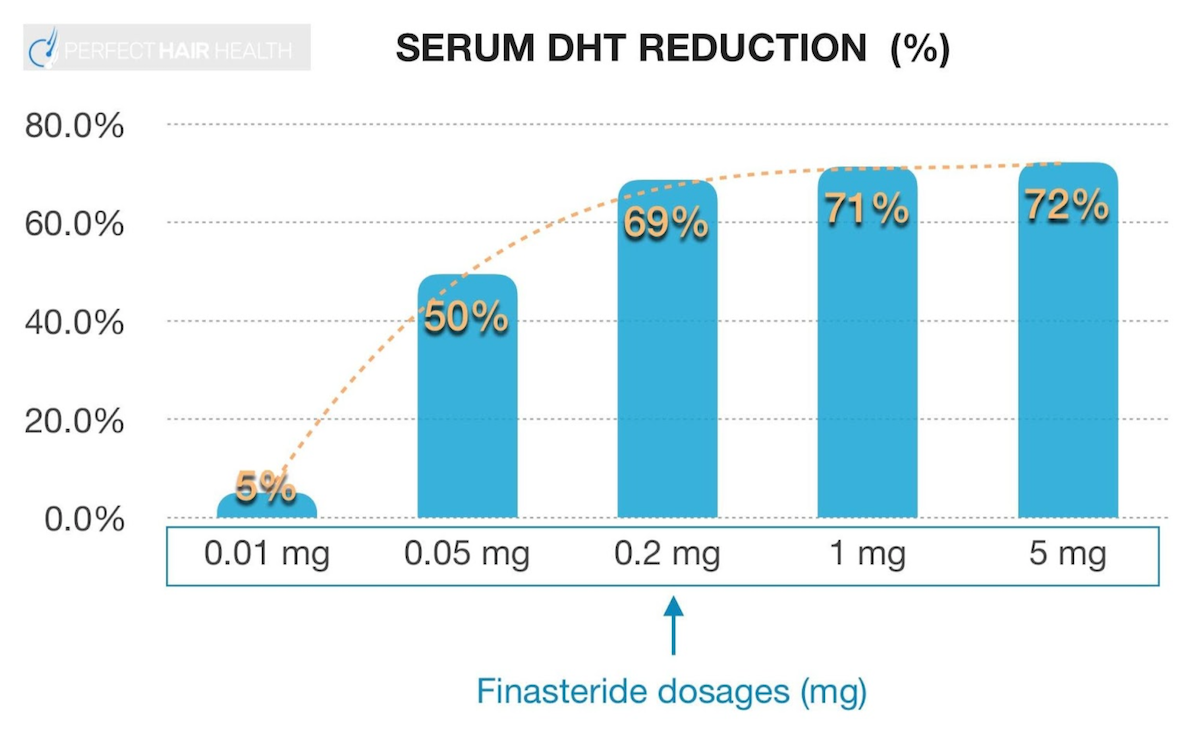
This implies that when applying topical finasteride, only a tiny fraction of it needs to go systemic in order to produce the same DHT-lowering effects as oral finasteride. If this happens, the purpose of using the topical formulation is completely defeated.
Research suggests a 1% topical finasteride formulation, applied twice daily, is ‘non-inferior,’ meaning equivalent, to 1 mg oral finasteride tablets.{{https://www.ncbi.nlm.nih.gov/pubmed/19172031}} And while that’s a positive in terms of hair growth, using this amount topically twice daily pretty much guarantees systemic absorption. In other words, if 1% topical is the equivalent of 1 mg oral, we can expect it to reduce serum DHT levels by 71%.
So what if we choose a formula with even lower percentages of the active drug? A study on 0.25% topical finasteride showed just a 35% reduction in serum DHT levels versus 55% for the oral medication, and yet similar outcomes for hair regrowth in both oral and topical groups.{{https://onlinelibrary.wiley.com/doi/10.1111/jdv.17738}}
So what if we go even lower? A study on 0.005% alcohol-based topical finasteride instructed participants to use the formulation twice daily, with 1 mL applied per session.{{https://dx.doi.org/10.3109%2F09546639709160517}} This led to no appreciable changes in serum DHT levels… meaning that for this ultra-low topical formulation, there was little-to-no systemic absorption (and presumably, few-to-no side effects). The good news? This group still experienced great hair growth outcomes.
So Just Reach for the Lowest Percentage, Yes?
It’s tempting from the above to infer we’ve reached the end of our story. As long as we reach for the lowest percentage of topical finasteride, we can be free from worries about the drug’s systemic effects. But, reality is a bit more complicated than that.
Systemic absorption isn’t just about dilution percentages. Topical finasteride’s systemic absorption actually depends on (at least) for variables:
- The drug’s formulation. Common carrier agents include alcohol and propylene glycol.
- The amount applied per use. The amount of topical finasteride applied to the scalp greatly varies.
- The application frequency. Applying the drug twice per day can more than double its effects on serum DHT.
- The days of application. Topical finasteride can take many days to “leak” into the blood before its final effects on serum DHT are realized.
For an example, see this figure from a 2014 study measuring how one versus two applications of 1 mL of 0.25% topical finasteride affected serum DHT levels.{{https://www.ncbi.nlm.nih.gov/pubmed/25074865}}
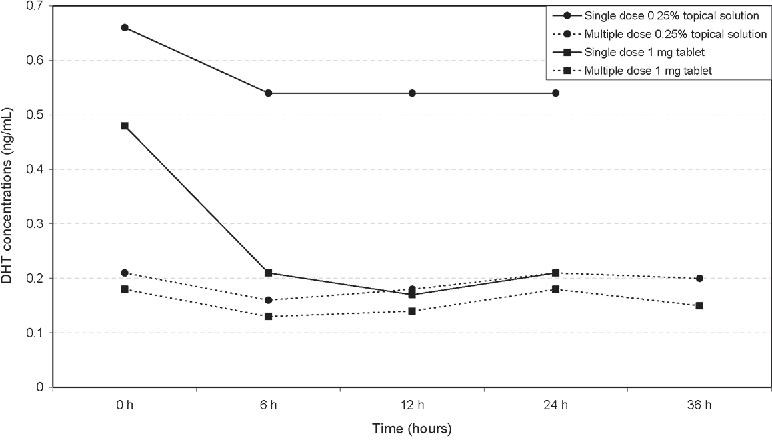
Caserini, M., Radicioni, M., Leuratti, C., Annoni, O., & Palmieri, R. (2014). A novel finasteride 0.25% topical solution for androgenetic alopecia: pharmacokinetics and effects on plasma androgen levels in healthy male volunteers. International journal of clinical pharmacology and therapeutics, 52(10), 842–849.
Over a 24-hour period, what were the findings?
- One application (i.e., 1 mL of 0.25% topical finasteride) lowered blood DHT levels by ~20%
- Two applications (i.e., 2 mL total) lowered blood DHT levels by ~70%
As such, we need to factor in these variables if we plan on sticking with topical finasteride for the long-term. Otherwise, we risk lowering our DHT levels to the same degree as 1 mg of oral finasteride, which would defeat the purpose of using the topical in the first place.
Topical Finasteride and Serum DHT: What Do The Clinical Studies Say?
Let’s take a closer look at some of the studies mentioned above. In addition to the percentage of active drug in the formula, there are a few more variables to understand. How much of the topical was applied, and which carrier agents were used?
The table below shows how even a .25% formula, for example, can reduce DHT in the serum by 24-70%
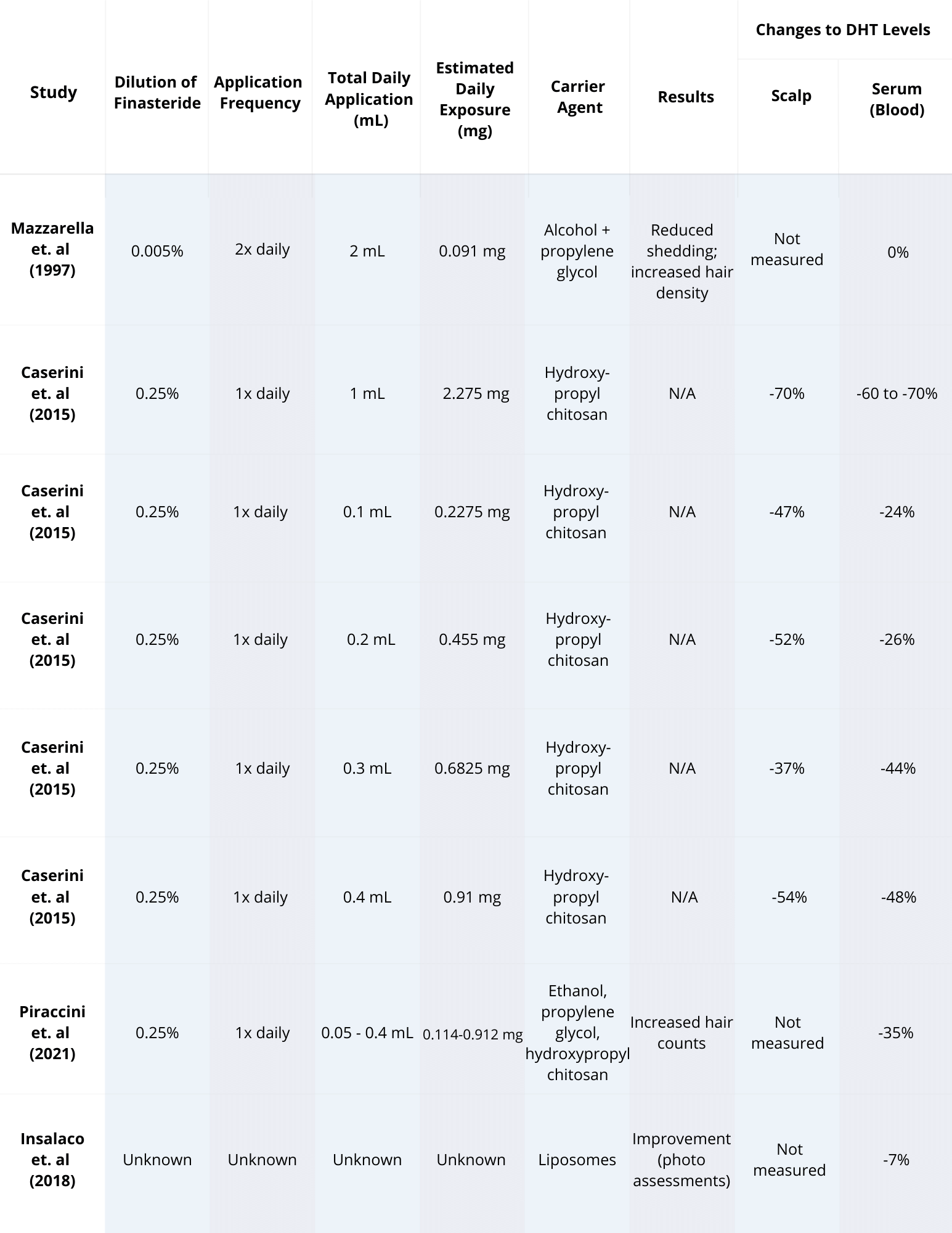
Based on this table, our total mg of daily finasteride exposure is probably the biggest factor in determining systemic leakage. And our total daily exposure (in mg) is a function of topical finasteride dilution (%) and the amount (mL) applied daily.
Knowing this, we can turn this table into a chart and sort it by mg of daily exposure. In doing so, we see a clear trend:
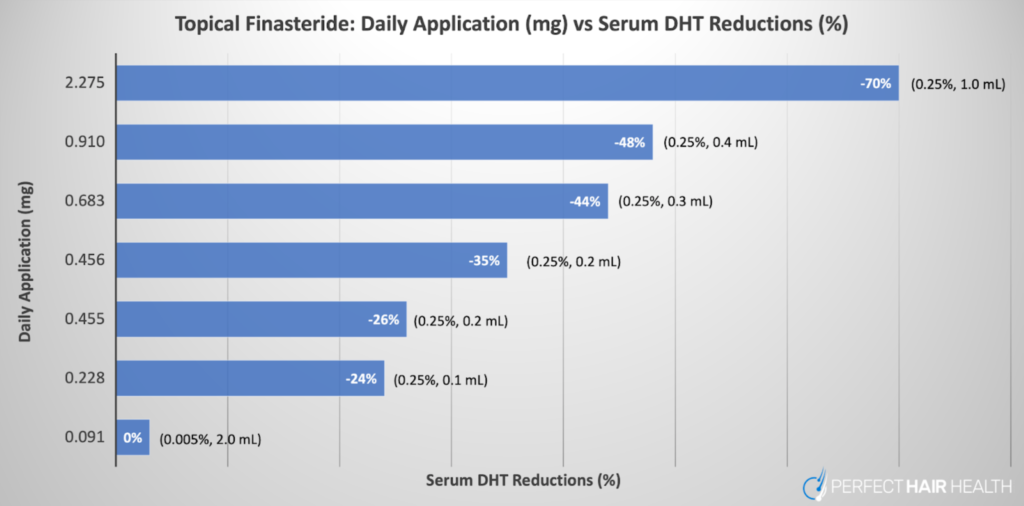
The good news? At both extremes of this chart – 0.091 mg and 2.275 mg daily – topical finasteride was shown to produce clinical results in improving hair parameters. Based on this, if we’re going for topical finasteride, we probably want to be prescribed topical finasteride solutions that net us daily exposure volumes of 0.228 mg and lower. After all, at 0.091 mg of topical finasteride daily, no systemic effects on DHT were observed.{{https://www.tandfonline.com/doi/abs/10.3109/09546639709160517}}
In other words, low dilutions (i.e., 1-2 mL of 0.005% to 0.02% of topical finasteride) confer significant benefits but at reduced risks of side effects due to lower systemic absorption – provided that guidelines for daily amounts (in mL) are also followed.
So What’s the Perfect Amount and Formula?
Our analyses from member-submitted lab tests and the clinical data suggest that 10-15% of topical finasteride will enter the bloodstream, at least when it’s formulated with alcohol and/or propylene glycol as carrier ingredients (as most compounding pharmacies do). So, if we apply 1-2 mL of 0.005% to 0.02% topical finasteride, this might equate to just 0.01-0.03 mg of systemic drug exposure.
For the overwhelming majority of people, that’s not enough systemic leakage to significantly lower DHT levels in the body. But it is enough to produce great hair loss outcomes.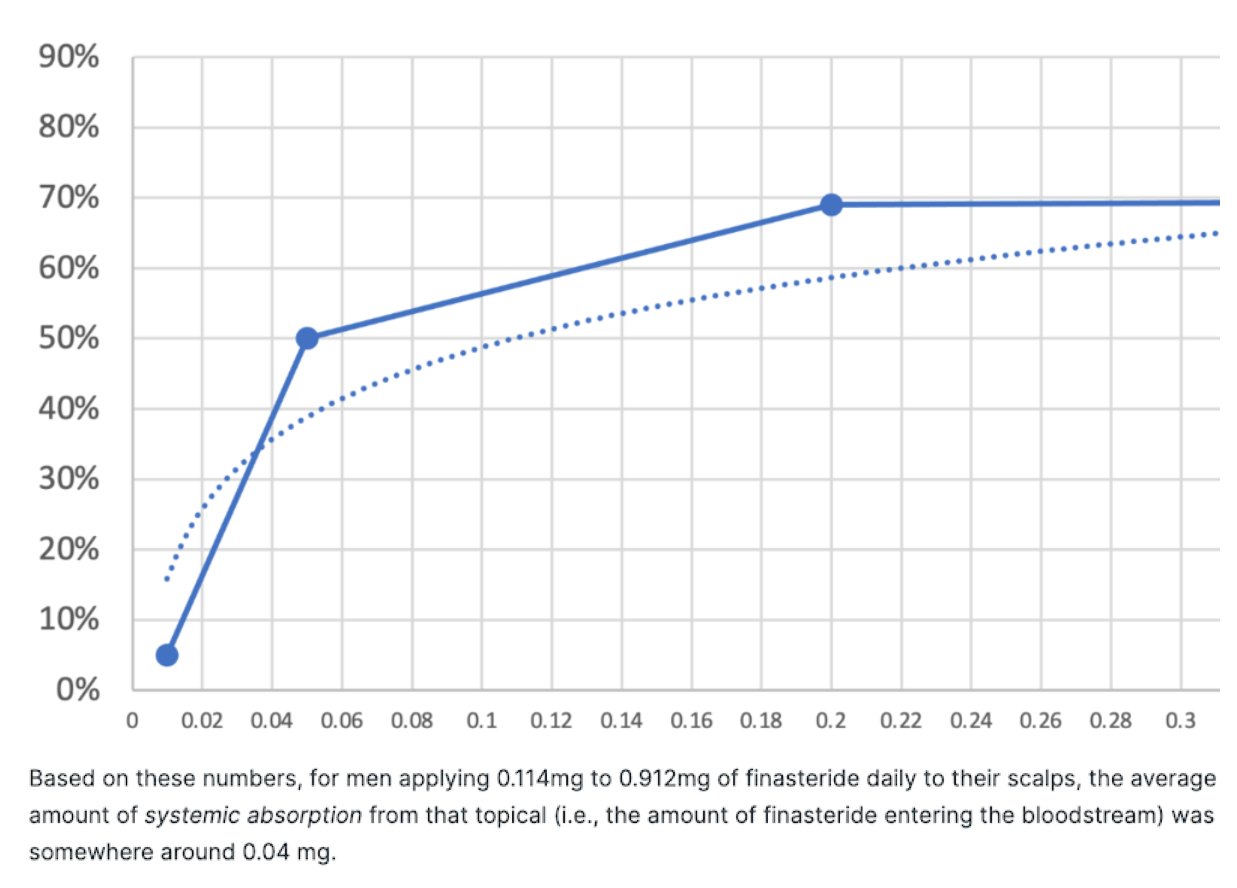
Our partial analysis estimating systemic leakage of topical finasteride from the study: Efficacy and safety of topical finasteride spray solution for male androgenetic alopecia: a phase III, randomized, controlled clinical trial (2021)
Join our Membership Program to get the full analysis.
Long-story short: stick to 1-2 mL of 0.005% to 0.02% topical finasteride solutions. This equates to roughly 0.1-0.2mg of daily finasteride exposure to the scalp. Any more than that, and there’s risk of significant systemic leakage, which defeats the purpose of using topical finasteride altogether.
How to Maximize Gains and Minimize Side Effects
Maximizing gains while minimizing the side effects of finasteride can be done, but it’s not a perfect science. We’ve outlined several tips below that we think might help. Due to individual variance, the most important step is to always start with testing.
1. Get Lab Tests for DHT
The goal with topical finasteride is to reduce the risk of side effects. To do this, we must minimize the amount of finasteride that leaks into the bloodstream. The best way to do this isn’t to rely on estimated metrics from clinical studies, but to collect personal data.
Get a serum DHT test before using the topical to establish a baseline. Then, DHT levels should be retested at one month to gauge just how much is going systemic. Testing is easier than most expect, and in our experience, the expenses are worth the peace of mind.
If future lab tests deviate from baseline, it’s an indication of just how much topical finasteride is going systemic. According to the clinical data, 30 days of application is more than enough time for finasteride to saturate at its maximum levels in the scalp and serum.
As such, measuring DHT levels after one month of finasteride use offers a great reference point to see if topical finasteride is impacting serum DHT levels. If needed, changes can be made to the application or use frequency depending on any changes to your blood levels of DHT.
2. Understand That DHT Levels Fluctuate Diurnally
Keep in mind, some fluctuation in DHT levels is normal. DHT levels fluctuate throughout the day and across seasons. As such, 15-20% differences across tests are normal and expected. Anything beyond 20% suggests that topical finasteride might be having slight systemic effects.
Because of this fluctuation, however, it’s important to get blood draws done at the same time of day – preferably in the morning and while in a fasted state. Also, try not to make drastic changes to diet, lifestyle, or environment prior to testing. Heavy drinking, deviations from a typical daily diet, the introduction of creatine powders, and/or sleep deprivation can all influence DHT levels and muddy test results. In the 3-5 days prior to the second test, try to keep things as they were when you first went in for testing.
3. Avoid supplementing with Quercetin and/or Creatine
Maintaining systemic DHT levels, while maximizing the effects of finasteride, isn’t just about the drug. There are other activities that could potentially affect DHT levels. Supplementing with quercetin and/or creatine is one common mistake that could impact results.
Studies on mice suggest that quercetin can inhibit the DHT-reducing effects of finasteride.{{https://joe.bioscientifica.com/view/journals/joe/181/3/493.xml}}While the translatability to humans has not yet been studied, the dosages used in these mouse models were comparable to what humans typically consume from quercetin supplements. As such, it may be best for those using finasteride to avoid this supplement.
When it comes to creatine, one study found that in training athletes, creatine supplementation increased serum DHT levels by over 70%.{{https://pubmed.ncbi.nlm.nih.gov/19741313/}} While the study was small, we have to reconcile these findings with the reality that for the overwhelming majority of training athletes, creatine is unnecessary. Bodybuilders can still look great without using it, and so can the every-day gym goer. Competitive bodybuilders are, however, a different story.
4. Set Realistic Expectations and Track Progress
Finasteride is the best-studied intervention for androgenic alopecia. In order to appreciate its full effects, consider the following:
- Know the timeline for results. Clinical studies show that finasteride improves pattern hair loss outcomes in 80-90% of men. Having said that, cosmetic degrees of hair regrowth don’t often occur until after 10-12 months of treatment. Moreover, the drug’s full effects typically take two years to manifest, with the biggest degrees of cosmetic regrowth occurring between year one and year two. As such, don’t expect any miracles in the first six months, it may take the full two years to see an effect.
- Track progress. It’s hard to know if something is improving without objective measurements. While not all of us have access to trichoscopic hair-counting equipment, most of us do have a smartphone, which can easily be used to take photos to track progress (particularly when the photosets are standardized). This can be done relatively effortlessly.
Following the tips above allows for the best possible shot at measurable hair growth results, while minimizing the potential effects of systemic DHT reduction.
Summary
Oral finasteride works great for male pattern hair loss, but by significantly reducing serum DHT, it can cause unwanted side effects.
Topical finasteride was developed as a solution, with a goal to reduce DHT in the scalp only. But when applied in high percentages or large amounts, it too, can go systemic and reduce serum DHT levels.
To minimize the side effects of finasteride without missing out on the benefits, stick to 1-2 mL of 0.005% to 0.02% topical finasteride solutions. This equates to roughly 0.1-0.2mg of daily finasteride exposure to the scalp.
The best way to ensure a reduced risk for side effects is to track serum DHT levels. Establish a baseline by taking one test before using finasteride, then test again one month later.
The range of treatments available for hair loss can seem bewildering. Over-the-counter options range from clinically proven pharmaceuticals to ineffective fads and overpriced shampoos. Prescription options can provide robust results for many, but come with a long list of potential side effects, drawbacks, and tradeoffs.
We started Perfect Hair Health to provide clarity and evidence-based information in a space that is too often characterized by exaggerated claims and misinformation. Unfortunately, the more we learned about the hair loss industry, the more stark the reality of the problems became. While telehealth companies have made effective treatments more accessible than ever, too often brands rely on poorly formulated pharmaceuticals that present unnecessary risks to users and ignore clinical data.
We co-founded Ulo in response to these issues to provide evidence-backed hair loss treatments that can be truly customized to work for you. In this Ulo review, we’ll take a deeper look at the issues in the industry and how Ulo does things differently. We’ll review the clinical evidence supporting Ulo’s choice of pharmaceuticals and ingredients, and see how its approach translates into real-world outcomes for safety, tolerability, and hair regrowth.
[ulo_promo title=”Interested in Topical Finasteride?” subtitle=”Low-dose & full-strength finasteride available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-finasteride?variant=42249746186319″ prescription=”true”]
What is Ulo?
After many years of consumer advocacy and watching hair loss brands provide suboptimal service and promote ineffective treatments, we co-founded Ulo.
Ulo is a telehealth provider focused on hair loss treatments. It’s committed to evidence-based treatments, real personalization, and customer safety. At its core, Ulo is built around three principles: evidence, personalization, and consumer safety. These principles are applied to ingredient selection, dosing strategies, and formulation design.

Figure 1. The Ulo range of products.
Problems in the Hair Loss Industry
There is a range of options available for hair loss that can produce real results. Best-selling pharmaceuticals like minoxidil and finasteride are backed by many years of clinical research, as well as the personal experiences of millions of users. So do you just need to pick the treatment that offers the most powerful regrowth?
Unfortunately, it’s not so simple. Finding the best treatment for you depends on finding the right dose and the most appropriate delivery method, as well as understanding potential side effects and whether combinations of treatments might optimize your results. That’s why customization is so essential for producing the best results.
However, instead of providing clear routes to effective treatments, telehealth companies sometimes compound these issues by introducing a whole new set of problems.
Problem #1: Unproven Treatments and Ingredients
The hair loss telehealth industry is a crowded one, and it’s sometimes hard to stand out. Because of this, many brands turn to unique ingredients and trends to attract new customers. Unfortunately, many of these treatments are not backed up by robust evidence.
It’s important to differentiate between strong evidence, which typically comes from multiple clinical trials conducted in humans, and weaker, limited evidence. Many drugs, compounds, and natural ingredients show some promise in petri dishes in the lab. Many even appear to regrow hair in animal models, typically mice. But this rarely translates directly into measurable outcomes in real people.
Unfortunately, some brands use this limited evidence as a basis to include these ingredients in treatments, even using them as unique selling points. If you’ve been watching progress in the hair loss industry for as long as we have, you’ll have seen these trends come and go.
Today, it’s peptides. Peptides have exploded in popularity and are touted as the solution to a wide range of health issues. You’re most likely to come across copper peptides in lists of ingredients for over-the-counter hair loss products, as well as prescription formulations.
One copper peptide, called AHK-Cu, has been shown to enhance the growth of human hair follicle cells in the lab, while another, GHK-Cu, has been shown to have anti-inflammatory properties.{{Gruchlik, A., Jurzak, M., Chodurek, E. W. A., & Dzierzewicz, Z. (2012). Effect of Gly-Gly-His, Gly-His-Lys and their copper complexes on TNF-alpha-dependent IL-6 secretion in normal human dermal fibroblasts. *Acta Poloniae Pharmaceutica.* 69(6). 1303–1306. Available at: https://pubmed.ncbi.nlm.nih.gov/23285694/}} These experiments on cells in a petri dish are an important step in finding new drugs and understanding the molecular mechanisms behind hair loss. Unfortunately, they don’t tell us much about what will happen in actual humans.
For that, we need clinical data, preferably from placebo-controlled clinical trials. The only clinical trial we’re aware of that tested copper peptides in humans found no statistical difference in hair length or thickness after 6 months of treatment with GHK-Cu.{{Lee, W. J., Sim, H. B., Jang, Y. H., Lee, S. J., Kim, D. W., & Yim, S. H. (2016). Efficacy of a complex of 5-aminolevulinic acid and glycyl-histidyl-lysine peptide on hair growth. *Annals of Dermatology.* 28(4). 438–443. Available at: https://doi.org/10.5021/ad.2016.28.4.438}}
That is not to say that copper peptides might not be effective at the right dose for the right person. But without clinical evidence, there’s no reason for you to expect improved outcomes, or for telehealth and hair loss brands to market them for hair loss. Copper peptides are only one example of a vast range of unproven ingredients that are regularly used in expensive hair loss treatments.
You can read more about understanding evidence in the hair loss industry in our article.
Problem #2: Irritants and Potentially Dangerous Ingredients
Ineffective ingredients can be an expensive, but ultimately harmless, addition to formulations. But what if ingredients went beyond useless, and were actually actively harmful? Unfortunately, that is potentially the case in some treatments currently on the market.
Propylene Glycol
On the low end of the scale are irritants, like propylene glycol. Propylene glycol is used in hair loss treatments as a carrier, meaning it’s a vehicle and helper for the active ingredients. Propylene glycol helps moisturize the skin and has been shown to improve the penetration of drugs into the skin in some models.{{Carrer, V., Alonso, C., Pont, M., Zanuy, M., Córdoba, M., Espinosa, S., Barba, C., Oliver, M. A., Martí, M., & Coderch, L. (2020). Effect of propylene glycol on the skin penetration of drugs. *Archives of Dermatological Research.* 312(5). 337–352. Available at: https://doi.org/10.1007/s00403-019-02017-5}},{{Lessmann, H., Schnuch, A., Geier, J., Uter, W. (2005). Skin-sensitizing and irritant properties of propylene glycol. Contact Dermatitis. 53(5). 247-259. Available at: https://doi.org/10.1111/j.0105-1873.2005.00693.x.}}
Unfortunately, it’s also a known irritant and can cause contact dermatitis in a small proportion of people.{{Shadi, Z. (2023). Compliance to Topical Minoxidil and Reasons for Discontinuation among Patients with Androgenetic Alopecia. Dermatology and Therapy (Heidelb). 13(5). 1157-1169. Available at: https://doi.org/10.1007/s13555-023-00919-x}}. This might be a fair trade-off if it were an essential ingredient. However, it’s perfectly possible to produce effective topicals for hair loss without propylene glycol.
Ingredients like propylene glycol can cause inflammation and irritation, which can make hair loss worse and stop treatments from working. Some brands use additional ingredients to dampen this inflammation, rather than stopping it at the source by removing potentially inflammatory, inessential components.
Corticosteroids
Corticosteroids, for example, help lower scalp inflammation and may provide additional benefits for people with alopecia areata or scarring alopecia.{{Alsantali, A. (2011). Alopecia areata: a new treatment plan. *Clinical, Cosmetic and Investigational Dermatology.* 4. 107–115. Available at: https://doi.org/10.2147/CCID.S22767}} However, they are not designed for long-term use, and applying steroids like fluocinolone to your skin every day for a year can cause conditions like skin thinning and spider veins.{{Torok, H. M., Jones, T., Rich, P., Smith, S., & Tschen, E. (2005). Hydroquinone 4%, tretinoin 0.05%, fluocinolone acetonide 0.01%: a safe and efficacious 12-month treatment for melasma. *Cutis.* 75(1). 57–62. Available at: https://pubmed.ncbi.nlm.nih.gov/15732437/}} What’s more, hair loss treatments are typically taken daily for many years, even decades, further increasing the likelihood of complications.
You can read more about the safety concerns behind corticosteroids in our full-length article.
Latanoprost
You might also spot hair loss formulations that include a drug called latanoprost. After initial promise in studies, latanoprost has had very mixed results from a number of clinical trials. Regardless, it was branded as new and exciting, becoming a popular treatment option.{{Blume-Peytavi, U., Lönnfors, S., Hillmann, K., & Garcia Bartels, N. (2012). A randomized double-blind placebo-controlled pilot study to assess the efficacy of a 24-week topical treatment by latanoprost 0.1% on hair growth and pigmentation in healthy volunteers with androgenetic alopecia. *Journal of the American Academy of Dermatology.* 66(5). 794–800. Available at: https://doi.org/10.1016/j.jaad.2011.05.026}},{{Bloch, L. D., Escudeiro, C. C., Sarruf, F. D., & Sakai Valente, N. Y. (2018). Latanoprost and minoxidil: comparative double-blind, placebo-controlled study for the treatment of hair loss. *Surgical & Cosmetic Dermatology.* 10(1). 39–43. Available at: https://doi.org/10.5935/scd1984-8773.20181011015}}
However, latanoprost was initially developed as a glaucoma treatment, and studies have shown that it can potentially change iris color in anywhere between 10% and 70% of patients.{{Teus, M. A., Arranz-Marquez, E., & Lucea-Suescun, P. (2002). Incidence of iris colour change in latanoprost treated eyes. *British Journal of Ophthalmology.* 86(10). 1085–1088. Available at: https://doi.org/10.1136/bjo.86.10.1085}} This risk of permanent side effects might be reasonable for glaucoma patients, but it’s difficult to justify for those with hair loss who might not see any benefits at all.
Problem #3: Mega-Dosed Topicals
Finasteride is an effective treatment for hair loss that works by lowering the level of dihydrotestosterone (DHT) in the scalp. DHT drives changes in the follicles that lead to androgenic alopecia (AGA). However, finasteride can also lower DHT in other parts of the body, leading to side effects.{{Zito, P. M., Bistas, K. G., Patel, P., & Syed, K. (2024). Finasteride. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Available at: https://www.ncbi.nlm.nih.gov/books/NBK513329/ (Accessed: October 2025)}}
Topical treatments are often presented as a way to localize drug activity to the scalp while minimizing systemic exposure. However, the extent to which drugs stay localized is heavily dependent on dosing.
Importantly, the relationship between the dose of finasteride and DHT reduction is not linear. When taken orally, even small amounts of the drug can significantly suppress serum DHT levels, reflecting systemic absorption of the drug into the blood. This means that for topical formulations applied to the scalp, even small amounts of absorption into the bloodstream can have an effect.
Data we’ve compiled from multiple clinical trials shows that only at doses of 0.005% is there no significant decrease in serum DHT. Despite this, many telehealth brands now offer high-strength topical finasteride formulations, often in the range of 0.25% to 0.3%, up to 60 times higher. These concentrations significantly increase the chances of side effects caused by systemic DHT reduction, while offering diminishing returns in terms of regrowth potential.
Figure 2. Data collected from multiple studies shows only application of very low (0.005%) concentrations of finasteride does not lower serum DHT levels.
If the aim of topical formulations is to reduce systemic absorption of DHT and minimize side effects, then mega-dose topicals run counter to this basic premise.
You can read more about finasteride dosing in our in-depth article.
Problem #4: No Customization
Hair loss is not a one-size-fits-all condition. The rate of hair loss, response to treatment, and incidence of side effects can vary significantly from person to person. Despite this, many telehealth platforms rely on highly standardized formulations.
This is a major issue when users experience side effects. The absence of options to decrease doses or look for alternatives can lead people to struggle through their treatment, or to abandon it entirely.
Conversely, if you find that your hair growth has plateaued or hair loss is increasing, there is no route to increase dosing or add additional treatments to your plan.
Problem #5 Improper Dutasteride Compounding
Dutasteride is a highly effective drug for reducing DHT, but its effectiveness depends heavily on its formulation. Unlike finasteride or minoxidil, dutasteride is poorly soluble in water and requires a lipid-based delivery system to be properly absorbed. That’s why it’s typically formulated as a soft-gel capsule
However, some providers are now compounding dutasteride into powder form in order to combine it with other ingredients, such as minoxidil or vitamins, in a single capsule. This can then be marketed as a more convenient, all-in-one solution.
Unfortunately, this may significantly reduce the drug’s bioavailability. To test this, we performed a small test. One participant took 3 pills of 0.5 mg powdered dutasteride (i.e., 1.5 mg total) and then checked changes in their blood DHT levels 12 hours later. Based on pharmacological data, we’d expect to see around an 80-90% reduction in DHT. However, we saw a reduction of only 13.6%.
Compounding of dutasteride without proper emulsifiers may be leading to lower DHT reduction, and therefore worse outcomes for hair regrowth.
[ulo_promo title=”Interested in Oral Dutasteride?” subtitle=”Oral Dutasteride Hair gains bigger than finasteride? Dutasteride makes this possible, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/oral-dutasteride?variant=42292746551375” prescription=”true” type=”oral” ]
How Does Ulo Solve These Problems?
Rather than searching for the newest trends and gimmicks, Ulo only uses pharmaceuticals and treatments backed by robust clinical evidence. This means clinical trials performed in humans, not only preliminary data from cell-based models or animal studies.
When it comes to incorporating these clinically validated ingredients into effective treatments, Ulo prioritizes customizability rather than relying on high-strength, one-size-fits-all topical formulations. Ulo offers both low-dose and full-strength versions of topical finasteride and dutasteride, with optional additions such as higher-strength minoxidil, tretinoin, caffeine, melatonin, or cetirizine, depending on individual needs and tolerability.
What Does Ulo Offer?
Ulo offers a range of proven hair loss treatments at a range of concentrations. Here, we’ll explore the catalog in detail and look at some of the evidence supporting it.
Finasteride
As we’ve noted above, finasteride is backed by many years of clinical evidence and the experience of hundreds of thousands of users across the globe. {{Kaufman, K.D., Olsen, E.A., Whiting, D., Savin, R., DeVillez, R., Bergfeld, W., Price, V.H., Van Neste, D., Roberts, J.L., Hordinsky, M., Shapiro, J., Binkowitz, B., Gormley, G.J. (1998). Finasteride In The Treatment Of Men With Androgenetic Alopecia. Journal Of The American Academy Of Dermatology. 39(4 Pt 1). 578-589. Available at: https://doi.org/10.1016/s0190-9622(98)70007-6}} Oral finasteride, typically taken as a 1 mg tablet daily, is one of only two FDA-approved treatments for hair loss. Ulo offers oral finasteride at the FDA-approved concentration of 1mg.

Figure 3. Ulo oral hair loss treatments.
As we’ve already discussed, androgenic alopecia (AGA) can be driven by increases in DHT. Finasteride works by blocking an enzyme called 5ɑ-reductase (5AR), which converts testosterone into DHT. Therefore, by blocking this conversion, the drug can decrease DHT in the scalp, and therefore inhibit its effects on hair.{{Ho, C.H., Sood, T., Zito, P.M. (2024). Androgenetic Alopecia. StatPearls. Available at: https://www.ncbi.nlm.nih.gov/books/NBK430924/}}
However, there are some downsides to oral finasteride. Because taking oral finasteride decreases DHT throughout the body, it can cause secondary side effects. This inlcludes decreased libido, erectile dysfunction, and ejaculation disorders, which affect a small proportion of users. {{Hirshburg, J. M., Kelsey, P. A., Therrien, C. A., Gavino, A. C., & Reichenberg, J. S. (2016). Adverse effects and safety of 5-alpha reductase inhibitors (finasteride, dutasteride): a systematic review. *The Journal of Clinical and Aesthetic Dermatology.* 9(7). 56–62. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC5023004/}}, {{Kaplan, S. A., Chung, D. E., Lee, R. K., Scofield, S., & Te, A. E. (2012). A 5-year retrospective analysis of 5α-reductase inhibitors in men with benign prostatic hyperplasia: finasteride has comparable urinary symptom efficacy and prostate volume reduction, but less sexual side effects and breast complications than dutasteride. *International Journal of Clinical Practice.* 66(11). 1052–1055. Available at: https://doi.org/10.1111/j.1742-1241.2012.03010.x}}
Due to these side effects, topical formulations of finasteride have been developed to localize the drug to the scalp. As we’ve already seen, how localized the drug stays depends on the dose and volume of finasteride applied. Ulo offers finasteride at a very low dose of 0.005% and at 0.2%.
Very low concentrations are designed to minimize systemic exposure as much as possible. One small clinical study showed that 0.005% topical finasteride found no significant changes in serum DHT levels, suggesting minimal systemic absorption. Despite this, participants still experienced meaningful hair growth.{{Mazzarella, G. F., Loconsole, G. F., Cammisa, G. A., Mastrolonardo, G. M., & Vena, G. A. (1997). Topical finasteride in the treatment of androgenic alopecia: preliminary evaluations after a 16-month therapy course. *Journal of Dermatological Treatment.* 8(3). 189–192. Available at: https://doi.org/10.3109/09546639709160517}}
In line with Ulo’s commitment to customization, a higher dose is available for those looking for a more powerful solution for growth. Finding the right balance of strength vs side effects is tricky. One study showed that 0.1% topical finasteride showed comparable efficacy to 1 mg oral finasteride, while a more recent trial found that 0.25% topical significantly improved target area hair count compared to placebo.{{Hajheydari, Z., Akbari, J., Saeedi, M., & Shokoohi, L. (2009). Comparing the therapeutic effects of finasteride gel and tablet in treatment of the androgenetic alopecia. *Indian Journal of Dermatology, Venereology and Leprology.* 75. 47. Available at: https://doi.org/10.4103/0378-6323.45220}}
Figure 4. Customizable topicals formulations from Ulo.
Increasing topical concentrations above 0.2% appears to provide diminishing returns for hair growth while increasing the risk of side effects. As such, this is the highest concentration available from Ulo.
Importantly, Ulo’s topical formulations are fully customizable, including the addition of growth stimulants and other add-ons to help you better find the right combination for you.
Minoxidil
Minoxidil is one such growth stimulant, which can work alone or in combination with treatments. Topical minoxidil is an FDA-approved treatment for hair loss at 5% concentrations, and it works through different mechanisms to finasteride. It alters the hair cycle, promoting entry of hair follicles into the growth phase, while shortening the resting phase. It can also increase blood flow around follicles and activate pro-growth molecular signaling pathways.{{Messenger, A. G., & Rundegren, J. (2004). Minoxidil: mechanisms of action on hair growth. British Journal of Dermatology. 150(2). 186–194. Available at: https://doi.org/10.1111/j.1365-2133.2004.05785.x}}
Multiple clinical trials have demonstrated the efficacy of minoxidil for increasing hair growth. {{Gupta, A.K., Charrette, A. (2015). Topical Minoxidil: Systematic Review And Meta-Analysis Of Its Efficacy In Androgenetic Alopecia. Skinmed. 13(3). 185-189}} Because minoxidil works via different mechanisms, using the drug in combination with DHT-blockers like finasteride can promote growth by multiple routes.
Ulo offers minoxidil at 7%, higher than the over-the-counter concentration of 5%. Topical minoxidil is typically safe, with the most common side effects including scalp irritation and itching. Many incidences of itching and irritation are likely due to the inclusion of propylene glycol, which is entirely absent from all of Ulo’s formulations.
Because the risk of adverse effects is relatively low, this higher concentration can improve results without incurring significant risk. Perfect hair health members have consistently reported strong results using 7% minoxidil, particularly when combined with enhancers like tretinoin that can help the drug to penetrate into the skin.
DHT-blockers like finasteride are not typically recommended for women who may become pregnant, due to significant danger during pregnancy. As such, minoxidil may be a better solution for pre-menopausal women, or anyone concerned about side effects.
Ulo also offers oral minoxidil in a 2.5mg tablet. This may be a good solution for users who struggle with the appearance of their hair after using topical formulations, or who find it hard to maintain consistent, daily application. Treating hair loss is a long game, and often the best solution is one that you can apply consistently every day over many years.
Oral minoxidil does come with some increased risk of side effects that users should be aware of. These include hypertrichosis (excessive hair growth outside of the scalp), mild fluid retention or ankle swelling, and lightheadedness. Cardiac issues are a more serious, but less commonly reported, issue.{{Vañó-Galván, S., Pirmez, R., Hermosa-Gelbard, A., Moreno-Arrones, Ó. M., Saceda-Corralo, D., Rodrigues-Barata, R., Jimenez-Cauhe, J., et al. (2021). Safety of low-dose oral minoxidil for hair loss: a multicenter study of 1404 patients. Journal of the American Academy of Dermatology. 84(6). 1644–1651. Available at: https://doi.org/10.1016/j.jaad.2021.02.054}}
Again, customization is key. Minoxidil can be effective on its own, or in combination with other therapies. Ulo offers a range of options to suit your needs and priorities.
Dutasteride
Like finasteride, dutasteride lowers levels of DHT by blocking 5AR. However, dutasteride blocks two forms of the enzyme, while finasteride only blocks one, which can lead to even greater DHT reduction. Clinical evidence consistently supports this, and across multiple studies, 0.5 mg oral dutasteride has been shown to outperform 1 mg finasteride in increasing total hair count, improving hair thickness, and reversing follicle miniaturization.{{Shanshanwal, S. J., & Dhurat, R. S. (2017). Superiority of dutasteride over finasteride in hair regrowth and reversal of miniaturization in men with androgenetic alopecia: a randomized controlled open-label, evaluator-blinded study. *Indian Journal of Dermatology, Venereology and Leprology.* 83. 47. Available at: https://doi.org/10.4103/0378-6323.188652}}
However, this mechanism of action can also result in side effects, as we saw with finasteride. For this reason, topical formulations were developed. A 2025 randomized controlled trial comparing topical dutasteride (0.01-0.05%) to oral finasteride reported greater improvements in hair density and global photographic assessments in the topical dutasteride group.{{Panuganti, V.K., Kumar Madala, P., Ramalingayya Grandhi, V., Varma Alluri, C., Mohammad, J., Rao, K.S.S.V.V., Reddy Dundigalla, M., (2025). A Randomized, Double-Blind, Placebo and Active Controlled Phase II Study to Evaluate the Safety and Efficacy of Novel Dutasteride Topical Solution (0.01%, 0.02%, and 0.05% w/v) in Male Subjects With Androgenetic Alopecia. Cureus. 17(8). e89309. Available at: https://doi.org/10.7759/cureus.89309}}
Ulo offers dutasteride at concentrations of 0.02% to 0.2%, again allowing users to balance tolerability with the strength of treatment.
[ulo_promo title=”Interested in Topical Dutasteride?” subtitle=”Hair gains bigger than finasteride? Dutasteride makes this possible, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-dutasteride?variant=42249748349007” prescription=”true” type=”topical” ]
Tretinoin (Retinoic Acid)
Perfect Hair Health’s many years of consumer advocacy and the insights from our community have highlighted the importance of add-ons to well-established pharmaceutical options.
Tretonoin is a derivative of retinoic acid and has been shown to have a modest impact on hair growth when used alone.{{Bazzano, G. S., Terezakis, N., & Galen, W. (1986). Topical tretinoin for hair growth promotion. *Journal of the American Academy of Dermatology.* 15(4). 880–893. Available at: https://doi.org/10.1016/S0190-9622(86)80024-X}} However, it’s most effective when used alongside minoxidil.
For minoxidil to work, it first has to be activated in the scalp by an enzyme called SULT1A1. As a result, the efficacy of minoxidil is highly dependent on levels of SULT1A1. Tretinoin has been shown to increase SULT1A1 in the outer root sheath, enhancing the local activation of minoxidil. {{Sharma, A., Goren, A., Dhurat, R., Agrawal, S., Sinclair, R., Trueb, R.M., Vano-Galvin, S., Chen, G., Tan, Y., Kovacevic, M., Situm, M., McCoy, J. (2019). Tretinoin enhances minoxidil response in androgenetic alopecia patients by upregulating follicular sulfotransferase enzymes. Dermatologic Therapy. 32(3). 12915. Available at: https://doi.org/10.1111/dth.12915}}
Ulo allows you to add tretinoin to your formulations to optimize their efficacy and drive better results, and may be particularly beneficial for patients who have responded poorly to minoxidil or have low levels of SULT1A1.
Melatonin
Another available add-on is melatonin. While it doesn’t provide the same kind of results as pharmaceutical options, topical melatonin has been shown to reduce rates of active hair shedding and, in some cases, improve hair density and counts, particularly in individuals with early-stage AGA.{{Fischer, T. W., Trüeb, R. M., Hänggi, G., Innocenti, M., & Elsner, P. (2012). Topical melatonin for treatment of androgenetic alopecia. *International Journal of Trichology.* 4(4). 236–245. Available at: https://doi.org/10.4103/0974-7753.111199}}
Ulo offers 0.01% melatonin to add to topical hair loss formulations. Melatonin alone is unlikely to drive significant results, but as an adjunct to drugs like finasteride and minoxidil, it can help reduce shedding and is recommended for those with early signs of AGA.
Caffeine
Caffeine is commonly found in shampoos and conditioners, though it’s unlikely to have any significant impact on hair growth in these wash-off treatments. There is some evidence to suggest that topical solutions of 0.2% can help boost growth, though caffeine hasn’t been as thoroughly investigated as the other ingredients we see here.{{Dhurat, R., Chitallia, J., May, T. W., Jayaraaman, A. M., Madhukara, J., Anandan, S., Vaidya, P., & Klenk, A. (2018). An open-label randomized multicenter study assessing the noninferiority of a caffeine-based topical liquid 0.2% versus minoxidil 5% solution in male androgenetic alopecia. *Skin Pharmacology and Physiology.* 30(6). 298–305. Available at: https://doi.org/10.1159/000481141}}
Instead of acting as the primary active ingredient, caffeine is also best used as an add-on. Clinical evidence suggests that 5% minoxidil with 1% caffeine and 1.5% azelaic acid can be more effective than minoxidil alone.{{Pazoki-Toroudi, H., Moghadam, R. M., Ajami, M., Nassiri-Kashani, M., Ehsani, A., Tabatabaie, H., Khani, S., Abbasi, Z., Shizarpour, M., Firooz, A., & Dowlati, Y. (2013). The efficacy and safety of minoxidil 5% combination with azelaic acid 1/5% and caffeine 1% solution on male pattern hair loss. *Journal of Investigative Dermatology.* 133. S84–S84. Available at: https://doi.org/10.1038/jid.2013.97}}
Caffeine, therefore, is probably best understood as a relatively low-risk addition that may provide modest benefits when used alongside better-supported therapies. For this reason, Ulo offers 0.2% caffeine as an add-on to prescription therapies.
Cetirizine
Cetirizine is an antihistamine best known as a treatment for allergies. There is, however, encouraging clinical evidence suggesting it can help treat hair loss. In one placebo-controlled trial, 43.3% of participants using topical cetirizine showed hair regrowth, compared to none in the placebo group. In another trial, cetirizine improved hair density, although minoxidil performed better overall.[[Zaky, M. S., Abo Khodeir, H., Ahmed, H. A., & Elsaie, M. L. (2021). Therapeutic implications of topical cetirizine 1% in treatment of male androgenetic alopecia: a case‐controlled study. Journal of Cosmetic Dermatology. 20(4). 1154-1159. Available at: https://doi.org/10.1111/jocd.13940}}
It’s unclear whether cetirizine will be effective as a stand-alone treatment. Following this evidence, Ulo offers it as an add-on to better evidenced treatments to take advantage of its hair growth potential. What’s more, because it’s so widely used in allergy medications, the safety profile of cetirizine is very well understood.
Is Ulo the #1 Customized Hair Loss Treatment in 2026?
There is a range of telehealth brands that offer great solutions for many people. Some companies have made amazing progress in improving access to hair loss treatments, offering combinations of oral and topical therapies, simplified prescription processes, and greater flexibility in delivery.
However, these solutions are often still built around standardized formulations and rigid ingredient lists. For many people, these platforms can still deliver solid results, particularly for those who respond well to first-line therapies and don’t require fine-tuning.
Ulo builds on the strengths of these platforms, including accessibility, convenience, and clinically validated treatments, but expands them by offering genuine flexibility in treatment design. Users can choose between oral and topical treatments, low-dose and full-strength formulations, and can add evidence-supported adjuncts like tretinoin, melatonin, caffeine, or cetirizine depending on their goals, tolerability, and stage of hair loss.
Available Ulo before and afters and reviews suggest this approach is providing meaningful results for customers, with treatment on their terms. Some users need to start cautiously to minimize side effects, while others need stronger interventions or add-ons to push beyond a plateau. Ulo’s range of oral and topical finasteride and dutasteride, higher-strength minoxidil, and customizable adjuncts allows treatment to be adjusted around the individual.
Ulo distinguishes itself by combining a foundation of evidence-based therapies with customization, formulation control, and evidence-based decision-making that are still largely absent elsewhere.
Looking to the Future of Ulo
Ulo’s approach is not limited to its current product line. A core part of its long-term strategy is continued investment in research and development, with the goal of improving both the effectiveness and safety of hair loss treatments over time. This includes work on new proprietary base formulations designed to enhance localization, helping active ingredients remain targeted to the scalp while minimizing systemic exposure.
Future treatments also aim to provide more options for individuals with sensitivities, as well as a broader range of concentrations, formulations, and ingredient combinations tailored to different stages of hair loss and treatment goals.
Final Thoughts
At Perfect Hair Health, our goal has never been to criticize the industry without cause. However, we continue to highlight issues because, as they persist, they continue to provide a less effective, less safe treatment space for consumers.
Ultimately, we would prefer a world where these issues no longer exist, where treatments are consistently evidence-based, properly formulated, and tailored to the individual. That would be better for consumers, and it would mean there’s less need to constantly question the quality of what’s being offered.
Ulo is our attempt to move in that direction. It reflects the standards we’ve been advocating for over the past decade: better formulations, better dosing strategies, and a more thoughtful approach to customization.
When starting a hair growth journey, it’s easy to feel overwhelmed. A quick search online brings up hundreds of treatments. From prescription medications and over-the-counter solutions to devices, supplements, and medical procedures, all of which claim to regrow hair. With so many options, it’s hard to know which treatments are actually backed by scientific evidence and are worth spending your time and money on.
In reality, there is no single best hair loss treatment that works for everyone. That’s because male pattern hair loss does not look the same for everyone. It can vary widely in pattern, progression, and the underlying biology. Meaning some treatments tend to work better in certain situations than in others. Some are more effective for diffuse thinning, while others are better for localized recession. Some treatments are better for convenience, while others need consistency and long-term application to see results.
In this article, we break down 10 of the best hair loss treatments for men. We have not ranked them from best to worst because each works best in specific circumstances. We look into how each treatment works, the clinical evidence backing it, safety considerations, and who it’s most likely to work best for.
Oral Finasteride
Ideal For:
- Men looking for an FDA-approved treatment
- Men who prefer the convenience of taking one pill per day versus a topical application regimen.
- Men with diffuse thinning rather than localized thinning. With diffuse thinning, applying topical treatments evenly every day can be time-consuming and difficult compared to targeting a small area.
Finasteride is a prescription medication that treats androgenic alopecia (AGA) by inhibiting the enzyme 5ɑ-reductase (5AR), which converts testosterone into dihydrotestosterone (DHT). In people with AGA, DHT is elevated and binds to androgen receptors, which act as landing pads for DHT to have its effect. The binding of DHT to androgen receptors in the scalp leads to follicular miniaturization and leads to hair loss.{{Ho, C.H., Sood, T., Zito, P.M. (2024). Androgenetic Alopecia. StatPearls. Available at: https://www.ncbi.nlm.nih.gov/books/NBK430924/}}
Finasteride works by selectively inhibiting type II 5AR. By blocking this enzyme, finasteride reduces the conversion of testosterone to DHT. DHT levels drop, and the hormonal process that causes pattern hair loss is disrupted, helping to maintain existing hair and induce hair regrowth.
Figure 1. Structure of finasteride.{{Wikipedia, (2009), Finasteride. Available at: https://en.wikipedia.org/wiki/Finasteride#/media/File:Finasteride.svg (Accessed: 24 February 2026)}} Image in the public domain.
Clinical Evidence for Oral Finasteride
Oral finasteride is one of the most well-studied hair loss treatments and is one of two FDA-approved treatments for AGA. Over the years, there have been many clinical studies that demonstrate oral finasteride is able to slow hair loss and promote new hair growth in many patients. Large randomized placebo-controlled trials consistently show that daily oral finasteride leads to improvements in hair count, hair density, and participant satisfaction.
A notable trial involved 1,500 men with AGA. Of those treated with oral finasteride (1 mg), 48% were rated as improved based on standardized photographs after 12 months, compared to 7% in the placebo-treated group.{{Kaufman, K.D., Olsen, E.A., Whiting, D., Savin, R., DeVillez, R., Bergfeld, W., Price, V.H., Van Neste, D., Roberts, J.L., Hordinsky, M., Shapiro, J., Binkowitz, B., Gormley, G.J. (1998). Finasteride In The Treatment Of Men With Androgenetic Alopecia. Journal Of The American Academy Of Dermatology. 39(4 Pt 1). 578-589. Available at: https://doi.org/10.1016/s0190-9622(98)70007-6}} Also, hair counts in the oral finasteride group increased or stabilized, whereas those in the placebo group experienced progressive hair loss.
The typical dose of oral finasteride for AGA is 1 mg. Increasing the dose to 5 mg does not tend to improve hair regrowth or further suppress scalp DHT in a meaningful way. For example, studies found scalp DHT reductions of 64% with 1 mg and 69% with 5 mg, which is a negligible difference.{{Drake, L., Hordinsky, M., Fiedler, V., Swinehart, J., Unger, W.P., Cotterill, P.C., Thiboutot, D.M., Lowe, N., Jacobson, C., Whiting, D., Stieglitz, S., Kraus, S.J., Griffin, E.I., Weiss, D., Carrington, P., Gencheff, C., Cole, G.W., Pariser, D.M., Epstein, E.S., Tanaka, W., Dallob, A., Vandormael, K., Geissler, L., Waldstreicher, J. (1999). The Effects Of Finasteride On Scalp Skin And Serum Androgen Levels In Men With Androgenetic Alopecia. Journal Of The American Academy Of Dermatology. 41(4). 550-554}}
Lowering the dose to 0.2 mg daily shows promising results. In one 48-week trial, 54% of men who took 0.2 mg oral finasteride showed improvement, compared to 58% on 1 mg, suggesting only a marginal difference. That said, the relative percentage change in terminal hair counts was higher in the 1 mg versus 0.2 mg group.{{Fertig, R.M., Caresse, G.A., Darwin, E., Gaudi, S. (2017). Sexual Side Effects Of 5-ɑ-Reductase Inhibitors Finasteride And Dutasteride: A Comprehensive Review. Dermatology Online Journal. 23(11). 1-19. Available at: https://doi.org/10.5070/D32311037240}}
If you’re looking for more information on how to take oral finasteride, read our article here.
[ulo_promo title=”Interested in Oral Finasteride?” subtitle=”Oral finasteride & minoxidil available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/oral-finasteride?variant=42292837711951” prescription=”true” type=”oral” ]
How Safe is Oral Finasteride?
Oral finasteride is generally well tolerated. However, as oral finasteride is ingested and reaches the systemic circulation, some people may experience sexual side effects, including reduced libido and erectile difficulties. Clinical trials suggest the risk is around 15% of users; however, these effects usually resolve after stopping medication.{{Estill, M.C., Ford, A., Omeira, R., Rodman, M. (2023). Finasteride And Dutasteride For The Treatment Of Male Androgenetic Alopecia: A Review Of Efficacy And Reproductive Adverse Effects. Georgetown Medical Review. 7(1). Available at: https://doi.org/10.52504/001c.88531}} Oral finasteride may temporarily reduce sperm count or semen volume, but this is typically reversible.{{Amory, J.K., Wang, C., Swerdloff, R.S., Anawalt, B.D., Matsumoto, A.M., Bremner, W.J., Walker, S.E., Haberer, L.J., Clark, R.V. (2007). The Effect Of 5ɑ-Reductase Inhibition With Dutasteride And Finasteride On Semen Parameters And Serum Hormones In Healthy Men. The Journal Of Clinical Endocrinology & Metabolism. 92(5). 1659-1665. Available at: https://doi.org/10.1210/jc.2006-2203}} Other potential side effects include breast tenderness and mood changes.
As with any medication, if you are considering finasteride, you should discuss potential risk factors and fertility plans with a clinician before beginning treatment and ensure you consult with a clinician if you experience any side effects.
If you’re a member and would like to find out more about oral finasteride, read our ultimate guide here.
Topical Minoxidil
Ideal For:
- Men who are looking for an over-the-counter, FDA-approved treatment for localized thinning.
- Men who are looking for a standard 5% minoxidil formulation or higher-strength, compounded formulations (e.g., 7%) if they have not responded to standard formulations.
- Men who are willing to consider combination therapies with tretinoin or microneedling.
Topical minoxidil at standard 2% and 5% concentrations is an over-the-counter, FDA-approved liquid or foam treatment. It can also be custom-compounded at higher concentrations from 7-15%, but this is not FDA-approved.
Topical minoxidil is a prodrug and is converted to its active form (minoxidil sulfate) by scalp enzymes called sulfotransferases, primarily the SULT1A1 enzyme. The activity of this enzyme can differ between people and in different regions of the scalp.
Minoxidil works by altering the hair cycle by shortening the resting (telogen) phase and promoting earlier entry into the growth (anagen) phase. This increases the proportion of follicles that actively produce hair. Minoxidil can also increase the size of miniaturized hair follicles, resulting in thicker and longer hair shafts.{{Messenger, A. G., & Rundegren, J. (2004). Minoxidil: mechanisms of action on hair growth. British Journal of Dermatology. 150(2). 186–194. Available at: https://doi.org/10.1111/j.1365-2133.2004.05785.x}}
Minoxidil can also increase local blood flow, activate the Wnt/β-catenin signaling pathway involved in follicular cell proliferation and differentiation, and has some cytoprotective and anti-inflammatory effects, which may increase prostaglandin E2 production.
Figure 2. Structure of minoxidil.{{Wikipedia, (2015), Minoxidil Structure Svg. Available at: https://en.wikipedia.org/wiki/Minoxidil#/media/File:Minoxidil_structure.svg (Accessed: 20 February 2026)}} Image in the public domain.
Clinical Evidence for Topical Minoxidil
Topical minoxidil has consistently been shown in many randomized controlled trials to increase hair count, prolong the anagen phase, and improve short-term patient satisfaction, especially at a 5% concentration.{{Gupta, A.K., Charrette, A. (2015). Topical Minoxidil: Systematic Review And Meta-Analysis Of Its Efficacy In Androgenetic Alopecia. Skinmed. 13(3). 185-189}}
That said, despite strong early efficacy, after one year or longer, response rates tend to drop or plateau, particularly when used without adjunctive therapies like microneedling or anti-androgens.
Multiple studies report rates below 30%, and even lower in five-year follow-up populations, with only about 20-30% of users satisfied with their results.{{Olsen, E.A., Weiner, M.S., Amara, I.A., DeLong, E.R. (1990). Five-Year Follow-Up Of Men With Androgenetic Alopecia Treated With Topical Minoxidil. Journal Of The American Academy Of Dermatology. 22(4). 643-646. Available at: https://doi.org/10.1016/0190-9622(90)70089-z}} In one trial, men using 5% minoxidil twice daily saw a nearly 60% increase in hair “weight” (total mass of regrown/thickened hair) at 6 months. By 96 weeks, gains had diminished to just 25% above the baseline, a significant drop from the initial response.{{Price, V.H., Menefee, E., Strauss, P.C. (1999). Changes In Hair Weight And Hair Count In Men With Androgenetic Alopecia, After Application Of 5% And 2% Topical Minoxidil, Placebo, Or No Treatment. Journal Of The American Academy Of Dermatology. 41(5 Pt 1). 717-721. Available at: https://doi.org/10.1016/s0190-9622(99)70006-x}}
In men with AGA, once-daily application of 5% topical minoxidil achieves hair count improvements comparable to twice-daily use of a 2% solution.{{Olsen, E.A., Dunlap, F.E., Funicella, T., Koperski, J.A., Swinehart, J.M., Tschen, E.H., Trancik, R.J. (2002). A Randomized Clinical Trial Of 5% Topical Minoxidil Versus 2% Topical Minoxidil And Placebo In The Treatment Of Androgenetic Alopecia In Men. Journal Of The American Academy Of Dermatology. 47(3). 377-385. Available at: https://doi.org/10.1067/mjd.2002.124088}} Higher concentrations (7%) may offer incremental benefit in some non-responders. With 7% formulations showing modest additional improvement in some studies, but results are mixed, and overall evidence remains limited.{{Singh, S., Patil, A., Kianfar, N., Waskiel-Burnat, A., Rudnicka, L., Sinclair, R., Goldust, M. (2022). Does Topical Minoxidil At Concentrations Higher Than 5% Provide Additional Clinical Benefit? Clinical And Experimental Dermatology. 47(11). 1951-1955. Available at: https://doi.org/10.1111/ced.15338}}
Data on 10-15% topical minoxidil are conflicting. Some studies report no meaningful advantage over 5%, while others report small gains in specific subgroups. However, adverse effects tend to increase at these higher concentrations.{{Vasantha, K.L. (2025). Efficiency And Safety Of 10% Minoxidil In The Treatment Of Alopecia Areata: A Randomised Controlled Trial. Journal Of Population Therapeutics And Clinical Pharmacology. 32(4). 724-730. Available at: https://doi.org/10.53555/56ggpq88}},{{Ghonemy, S., Alarawi, A., Bessar, H. (2021). Efficacy And Safety Of A New 10% Topical Minoxidil Versus 5% Topical Minoxidil And Placebo In The Treatment Of Male Androgenetic Alopecia: A Trichoscopic Evaluation. Journal Of Dermatological Treatment. 32(2). 236-241. Available at: https://doi.org/10.1080/09546634.2019.1654070}}
Adjunctive strategies aimed at enhancing minoxidil activation and penetration have shown promising results. Anecdotal evidence from our PHH members suggests that prescription concentration of topical minoxidil (7%) in combination with enhancers like tretinoin often improves outcomes.
One landmark study reported a nearly fourfold greater increase in hair count (approximately a 40% gain) compared to minoxidil alone at 12 weeks, with participants experiencing actual visible improvements in density.{{Ahmed, K.M.A., Kozaa, Y.A., Abuawwad, M.T., Al-Najdawi, A.I.A., Mahmoud, Y.W., Ahmed, A.M., Taha, M.J.J., Fadhli, T., Giannopoulou, A. (2025). Evaluating The Efficacy And Safety Of Combined Microneedling Therapy Versus Topical Minoxidil In Androgenetic Alopecia: A Systematic Review And Meta-Analysis. Archives Of Dermatological Research. 317(1). 528. Available at: https://doi.org/10.1007/s00403-025-04032-1}}
Topical retinoic acid (such as tretinoin) can also be combined with minoxidil to upregulate SULT1A1 activity. Thereby enhancing the local activation of minoxidil in the hair follicle. Peer-reviewed research indicates that applying topical tretinoin upregulates follicle sulfotransferase enzymes, thereby enhancing the response to minoxidil.{{Sharma, A., Goren, A., Dhurat, R., Agrawal, S., Sinclair, R., Trueb, R.M., Vano-Galvan, S., Chen, G., Tan, Y., Kovacevic, M., Situm, M., McCoy, J. (2019). Tretinoin Enhances Minoxidil Response In Androgenetic Alopecia Patients By Upregulating Follicular Sulfotransferase Enzymes. Dermatologic Therapy. 32(3). E12915. Available at: https://doi.org/10.1111/dth.12915}}
[ulo_promo title=”Interested in Topical Minoxidil?” subtitle=”High-strength topical minoxidil available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-minoxidil?variant=42247221313615” prescription=”true” type=”topical” ]
How Safe is Topical Minoxidil?
Topical minoxidil is generally safe. As it is applied directly to the scalp, it has a low risk of systemic side effects because it is minimally absorbed into the bloodstream. The most common adverse reactions are local, such as scalp irritation, itching, and flaking. These effects are usually due to the presence of propylene glycol in liquid formulations, which is known to cause scalp irritation.{{Patel, K., Palmer, A., Nixon, R. (2023). Allergic Contact Dermatitis From Propylene Glycol: A Case Series From Australia. Contact Dermatitis. 89(2). 79-84. Available at: https://doi.org/10.1111/cod.14325}} Foam formulations tend to be propylene glycol-free and fast-drying.
More severe side effects, like hypertrichosis (unwanted hair growth outside the scalp) or cardiovascular symptoms, are rare and tend to be linked to misuse or highly sensitive individuals. Topical minoxidil is highly toxic to cats, so it should be handled with care by pet owners.
Learn more about topical minoxidil in our article here.
Topical Finasteride
Ideal For:
- Men with localized AGA who want the DHT-lowering benefits of finasteride but prefer a topical, scalp-focused approach.
- Men who have concerns about systemic side effects with oral finasteride or have previously experienced unwanted effects on oral therapy.
- Men seeking a more potent topical option than minoxidil alone, particularly in DHT-driven thinning at the frontal scalp or crown.
Topical finasteride has emerged as a potential alternative to oral finasteride for AGA. It works by the same mechanism as oral finasteride, blocking type II 5AR to prevent the conversion of testosterone to DHT. But the difference is that topical finasteride is applied directly to the scalp rather than ingested.
By delivering finasteride directly locally to the hair follicles, the aim is to reduce scalp DHT whilst limiting systemic absorption. The goal of this approach is to maintain the benefits for hair regrowth while lowering the risk of whole-body side effects.
You can find more information on how topical finasteride works in our article here.
[ulo_promo title=”Interested in Topical Finasteride?” subtitle=”Low-dose & full-strength finasteride available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-finasteride?variant=42249746186319” prescription=”true”]
Clinical Evidence for Topical Finasteride
Clinical studies suggest that topical finasteride can improve hair parameters in men with AGA. One study reported that 1% topical finasteride showed comparable efficacy to 1 mg oral finasteride in terms of hair thickness, hair counts, and the size of the bald area.{{Hajheydari, Z., Akbari, J., Saeedi, M., & Shokoohi, L. (2009). Comparing the therapeutic effects of finasteride gel and tablet in treatment of the androgenetic alopecia. *Indian Journal of Dermatology, Venereology and Leprology.* 75. 47. Available at: https://doi.org/10.4103/0378-6323.45220}}
In a randomized controlled trial carried out in men with AGA over 24 weeks, they found that topical finasteride (0.25%) significantly improved target area hair count compared to placebo.{{Piraccini, B.M., Blume-Peytavi, U., Scarci, F., Jansat, J.M., Falqués, M., Otero, R., Tamarit, M.L., Galván, J., Tebbs, V., Massana, E. (2021). Efficacy And Safety Of Topical Finasteride Spray Solution For Male Androgenetic Alopecia: A Phase III, Randomized, Controlled Clinical Trial. Journal Of The European Academy Of Dermatology And Venereology. 36(2). 286–294. Available at: https://doi.org/10.1111/jdv.17738}}
How Safe is Topical Finasteride?
Topical finasteride has a different safety profile than oral finasteride. Studies show that while some systemic absorption still occurs, circulating finasteride and DHT changes are substantially smaller than with oral finasteride.{{Piraccini, B.M., Blume-Peytavi, U., Scarci, F., Jansat, J.M., Falqués, M., Otero, R., Tamarit, M.L., Galván, J., Tebbs, V., Massana, E. (2022). Efficacy And Safety Of Topical Finasteride Spray Solution For Male Androgenetic Alopecia: A Phase III, Randomized, Controlled Clinical Trial. Journal Of The European Academy Of Dermatology And Venereology. 36(2). 286–294. Available at: https://doi.org/10.1111/jdv.17738}}
But systemic effects are still possible. A 2025 FDA pharmacovigilance review of adverse event reports submitted between 2019 and 2024 identified 32 cases involving topical finasteride formulations. Most of these cases involved the use of compounded products. Reported symptoms included erectile dysfunction, anxiety, brain fog, depression, fatigue, insomnia, decreased libido, and testicular pain.{{US Food and Drug Administration. (2025). FDA alerts health care providers, compounders and consumers of potential risks associated with compounded topical finasteride products. FDA. Available at: https://www.fda.gov/drugs/human-drug-compounding/fda-alerts-health-care-providers-compounders-and-consumers-potential-risks-associated-compounded (Accessed: December 2025)}}
That said, the most common side effects associated with topical finasteride are local skin reactions. A 2018 systematic review noted reports of erythema, contact dermatitis, and scalp irritation in several studies; but serious cutaneous adverse events were absent.{{Lee, S.W., Juhasz, M., Mobasher, P., Ekelem, C., Mesinkovska, N.A. (2018). A Systematic Review of Topical Finasteride in the Treatment of Androgenetic Alopecia in Men and Women. Journal of Drugs in Dermatology. 17(4). 457-463. Available at: PMID: 29601622}} In many cases, scalp irritation is thought to be related to the formulation itself, particularly ingredients like propylene glycol.
If you’re a member, you can find out more about topical finasteride in our ultimate guide here.
Oral Dutasteride
Ideal For:
- Men who are willing to consider a stronger systemic therapy with more extensive or diffuse AGA.
- Men with progressive thinning across the scalp rather than isolated areas.
- Men who are looking for the next step if they have not achieved their desired results, or whose results have plateaued with finasteride.
So we know that DHT drives follicle miniaturization, and testosterone is converted to DHT by 5AR. But there are two types of 5AR: type I and type II.
This is where dutasteride and finasteride differ. Finasteride only blocks type II 5AR, whereas dutasteride can block both type I and type II 5AR. Because dutasteride blocks both types of 5AR, it suppresses DHT more strongly than finasteride. Oral dutasteride is FDA-approved for benign prostatic hyperplasia, but is commonly prescribed off-label for hair loss.
Figure 3. Structure of dutasteride.{{Wikipedia, (2009), Dutasteride. Available at: https://en.wikipedia.org/wiki/Dutasteride#/media/File:Dutasteride.svg (Accessed: 24 February 2026)}} Image in the public domain.
Clinical Evidence for Oral Dutasteride
Across multiple studies, dutasteride has been shown to consistently outperform finasteride on hair parameters. In one notable study carried out in men with AGA over 24 weeks, 0.5 mg dutasteride significantly increased total hair count and decreased thin hair count per cm2 compared to 1 mg finasteride.{{Shanshanwal, S. J., & Dhurat, R. S. (2017). Superiority of dutasteride over finasteride in hair regrowth and reversal of miniaturization in men with androgenetic alopecia: a randomized controlled open-label, evaluator-blinded study. *Indian Journal of Dermatology, Venereology and Leprology.* 83. 47. Available at: https://doi.org/10.4103/0378-6323.188652}}
Notably, another study carried out in men with AGA over 24 weeks, showed that 0.5 mg dutasteride significantly increased terminal hair count and hair width compared to 1 mg finasteride.{{Harcha, W. G., Barboza Martínez, J., Tsai, T.-F., Katsuoka, K., Kawashima, M., Tsuboi, R., Barnes, A., Ferron-Brady, G., & Chetty, D. (2014). A randomized, active- and placebo-controlled study of the efficacy and safety of different doses of dutasteride versus placebo and finasteride in the treatment of male subjects with androgenetic alopecia. *Journal of the American Academy of Dermatology.* 70(3). 489–498. Available at: https://doi.org/10.1016/j.jaad.2013.10.049}}
Additionally, across studies, investigators were more likely to rate dutasteride users as “improved” or “markedly improved” compared to those receiving finasteride.{{Choi, G.-S., Sim, W.-Y., Kang, H., Huh, C. H., Lee, Y. W., Shantakumar, S., Ho, Y.-F., et al. (2022). Long-term effectiveness and safety of dutasteride versus finasteride in patients with male androgenic alopecia in South Korea: a multicentre chart review study. *Annals of Dermatology.* 34(5). 349. Available at: https://doi.org/10.5021/ad.22.027}}
[ulo_promo title=”Interested in Oral Dutasteride?” subtitle=”Oral Dutasteride Hair gains bigger than finasteride? Dutasteride makes this possible, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/oral-dutasteride?variant=42292746551375” prescription=”true” type=”oral” ]
How Safe is Oral Dutasteride?
Oral dutasteride is generally well-tolerated by many users. But some people may experience the following side effects:
- Sexual side effects: Reduced libido, erectile dysfunction, or ejaculatory disorders (reduced volume or delayed ejaculation) may occur. These effects are often dependent on the dose and usually improve after stopping treatment.{{Choi, G.S., Sim, W.Y., Kang, H., Huh, C.H., Lee, Y.W., Shantakumar, S., Ho, Y.F., Oh, E.J., Duh, M.S., Cheng, W.Y., Bobbili, P., Thompson-Leduc, P., Ong, G. (2022). Long-Term Effectiveness And Safety Of Dutasteride Versus Finasteride In Patients With Male Androgenic Alopecia In South Korea: A Multicentre Chart Review Study. Annals Of Dermatology. 34(5). 349-359. Available at: https://doi.org/10.5021/ad.22.027}}
- Mood changes: Low mood or depressive symptoms, increased anxiety, or lack of motivation. These are uncommon, but any mood changes should be taken seriously if they do occur.{{Hirshburg, J.M., Kelsey, P.A., Therrien, C.A., Gavino, A.C., Reichenberg, J.S. (2016). Adverse Effects And Safety Of 5-Alpha Reductase Inhibitors (Finasteride, Dutasteride): A Systematic Review. Journal Of Clinical And Aesthetic Dermatology. 9(7). 56-62}}
- Breast changes: Hormonal shifts may lead to breast tenderness or enlargement (gynecomastia), which warrants medical review.{{Marihart, S., Harik, M., Djavan, B. (2005). Dutasteride: A Review Of Current Data On A Novel Dual Inhibitor Of 5alpha Reductase. Reviews In Urology. 7(4). 203-210}}
- Prostate-specific antigen (PSA): Dutasteride may lower PSA, which could mask early signs of prostate cancer.{{Marihart, S., Harik, M., Djavan, B. (2005). Dutasteride: A Review Of Current Data On A Novel Dual Inhibitor Of 5alpha Reductase. Reviews In Urology. 7(4). 203-210}}
Check out our article here on oral dutasteride to find out more about side effects, dosing, and how it compares to finasteride.
Topical Dutasteride
Ideal For:
- Men with AGA and localized thinning (e.g., the crown or frontal scalp).
- Men who have experienced side effects with oral dutasteride or are concerned about systemic effects.
- Men who are looking for a potentially stronger topical DHT-targeting option than finasteride.
- Men who are comfortable using a newer treatment that has relatively limited clinical evidence.
Topical dutasteride is another emerging therapy that works by the same mechanism as oral dutasteride, inhibiting both type I and type II 5AR to prevent the conversion of testosterone to DHT.
The difference is that topical dutasteride is applied directly to the scalp, with the goal of limiting systemic side effects. Topical dutasteride is not FDA-approved and is usually obtained through compounding pharmacies.
[ulo_promo title=”Interested in Topical Dutasteride?” subtitle=”Hair gains bigger than finasteride? Dutasteride makes this possible, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/topical-dutasteride?variant=42249748349007” prescription=”true” type=”topical” ]
Clinical Evidence for Topical Dutasteride
Clinical evidence for topical dutasteride is still limited compared with oral therapies. But, at the end of 2025, the first RCT involving 135 men with AGA comparing 1 mg oral finasteride to (0.01-0.05%) topical dutasteride over 24 weeks was published.{{Panuganti, V.K., Kumar Madala, P., Ramalingayya Grandhi, V., Varma Alluri, C., Mohammad, J., Rao, K.S.S.V.V., Reddy Dundigalla, M., (2025). A Randomized, Double-Blind, Placebo and Active Controlled Phase II Study to Evaluate the Safety and Efficacy of Novel Dutasteride Topical Solution (0.01%, 0.02%, and 0.05% w/v) in Male Subjects With Androgenetic Alopecia. Cureus. 17(8). e89309. Available at: https://doi.org/10.7759/cureus.89309}}
In the study, several hair parameters appeared to improve more in the topical dutasteride (0.05%) group than in those receiving oral finasteride (1 mg). The authors reported an average increase of 75 hairs per cm² with topical dutasteride compared to 41 hairs per cm² with oral finasteride.
Additionally, 69% of participants using topical dutasteride were rated as “improved” on global photographic assessment, compared with 21% in the oral finasteride group.
But it’s important to note that we are a little skeptical of the results from this study. This is because the baseline hair counts are suspicious, and the measurement circle clearly moves in location, size, and shape.
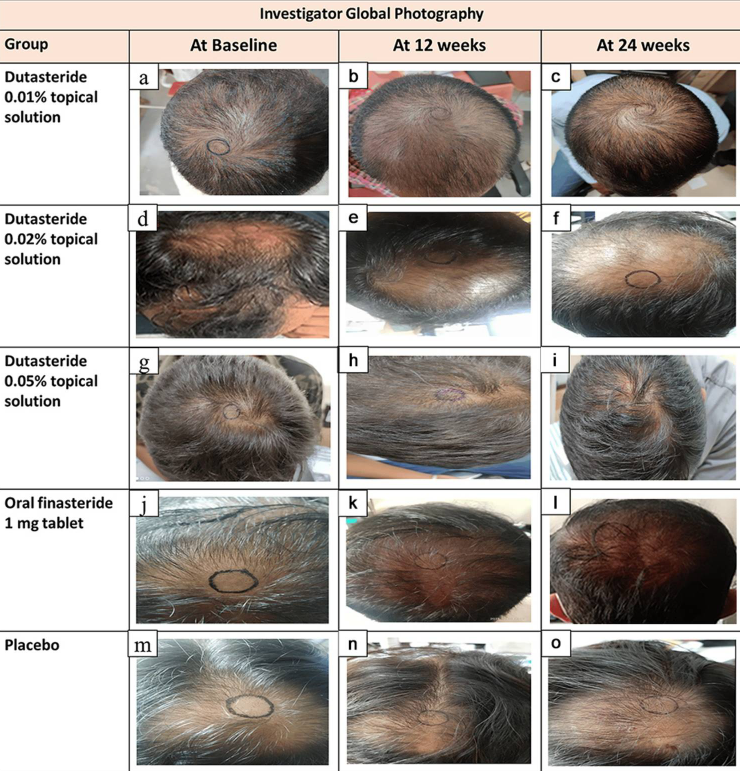
Figure 4. Representative hair growth images. Adapted from Figure 2.{{Panuganti, V.K., Kumar Madala, P., Ramalingayya Grandhi, V., Varma Alluri, C., Mohammad, J., Rao, K.S.S.V.V., Reddy Dundigalla, M., (2025). A Randomized, Double-Blind, Placebo and Active Controlled Phase II Study to Evaluate the Safety and Efficacy of Novel Dutasteride Topical Solution (0.01%, 0.02%, and 0.05% w/v) in Male Subjects With Androgenetic Alopecia. Cureus. 17(8). e89309. Available at: https://doi.org/10.7759/cureus.89309}} Image used under Creative Commons License
If you’d like to learn more about our take on this study, read our article here.
How Safe is Topical Dutasteride?
In this same study, systemic hormone changes with topical dutasteride were minimal. Plasma dutasteride levels were mostly near the quantification limit, but some samples spiked to 2,555 pg/mL, and dutasteride remained detectable at day 168 while participants were still receiving treatment. This suggests that average exposure was low, but absorption may be unpredictable in some people.
Because topical dutasteride is applied directly to the scalp, it may have fewer side effects than oral dutasteride. The most common side effects are local scalp reactions, including redness, itching, flaking, or contact dermatitis.
This is usually related to the carrier solution rather than the dutasteride itself. Switching carriers or adjusting how often it is applied often helps these symptoms.{{Panuganti, V.K., Kumar Madala, P., Ramalingayya Grandhi, V., Varma Alluri, C., Mohammad, J., Rao, K.S.S.V.V., Reddy Dundigalla, M., (2025). A Randomized, Double-Blind, Placebo and Active Controlled Phase II Study to Evaluate the Safety and Efficacy of Novel Dutasteride Topical Solution (0.01%, 0.02%, and 0.05% w/v) in Male Subjects With Androgenetic Alopecia. Cureus. 17(8). e89309. Available at: https://doi.org/10.7759/cureus.89309}}
If you’re interested in finding out more about how topical dutasteride works, have a read of our article here.
Oral Minoxidil
Ideal For:
- Men who have experienced side effects from finasteride or dutasteride.
- Men who prefer the convenience of a once-daily pill over topical application.
- Men who have struggled with adherence to topical treatments due to cosmetic residue, scalp irritation, or lifestyle factors.
- Men who have not responded well to topical minoxidil, including those with poor scalp absorption or SULT1A1 activity.
Oral minoxidil is a prescription medication that was originally used to treat high blood pressure. At lower doses (0.25-5 mg daily), it’s prescribed off-label to treat hair loss, especially in people who don’t respond well to topical minoxidil or struggle with applying topical treatments consistently.
Oral minoxidil supports regrowth by improving blood flow around follicles, shifting more hairs into the growth (anagen) phase, and activating follicular growth pathways.
Some people prefer oral minoxidil over topical due to the key differences in how each one is activated and delivered to the hair follicles. Topical minoxidil is a pro-drug that needs conversion to its active form by SULT1A1 enzymes located in scalp hair follicles.{{Pietrauszka, K., Bergler-Czop, B. (2020). Sulfotransferase SULT1A1 Activity In Hair Follicle, A Prognostic Marker Of Response To The Minoxidil Treatment In Patients With Androgenetic Alopecia: A Review. Advances In Dermatology And Allergology. 39(3). 472-478. Available at: https://doi.org/10.5114/ada.2020.99947}}
The activity of this enzyme varies significantly between people. Also, topical minoxidil faces a penetration problem where only about 1.4% of the drug applied is actually absorbed into the scalp skin under normal conditions.{{Suchonwanit, P., Thammarucha, S., Leerunyakul, K. (2019). Minoxidil And Its Use In Hair Disorders: A Review. Drug Design, Development And Therapy. 13. 2777-2786. Available at: https://doi.org/10.2147/DDDT.S214907}}
Oral minoxidil helps to bypass these limitations. Oral minoxidil is absorbed through the gastrointestinal tract and converted to its active form in the liver, where sulfotransferase activity is abundant.
This ensures that nearly all minoxidil that is ingested is activated and delivered systemically to the hair follicles throughout the scalp and body, regardless of individual differences in scalp enzyme activity. As a result, oral minoxidil can be effective even for people who have not responded to topical minoxidil due to low scalp sulfotransferase activity or poor drug penetration.{{Beach, R.A. (2018). Case Series Of Oral Minoxidil For Androgenetic And Traction Alopecia: Tolerability & The Five C’s Of Oral Therapy. Dermatologic Therapy. 31(6). E12707. Available at: https://doi.org/10.1111/dth.12707}}
[ulo_promo title=”Interested in Oral Minoxidil?” subtitle=”Low-dose oral minoxidil available, if prescribed*” description=”Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.” button_text=”Click Here For 15% Off” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/oral-minoxidil?variant=40943885484111” prescription=”true” type=”oral” ]
Clinical Evidence for Oral Minoxidil
One study in men with AGA reported a 100% response rate with 5 mg daily oral minoxidil, alongside an average 19% increase in hair count at 24 weeks.{{Lueangarun, S., Panchaprateep, R., Tempark, T., Noppakun, N. (2015). Efficacy And Safety Of Oral Minoxidil 5 Mg Daily During 24-Week Treatment In Male Androgenetic Alopecia. Journal Of The American Academy Of Dermatology. 72(5). AB113. Available at: https://doi.org/10.1016/j.jaad.2015.02.466}} Additionally, a retrospective study showed a 90% response rate at 6-12 months for men taking 2.5-5 mg of oral minoxidil daily. Notably, around 60% of these men had tried other treatments for AGA, but had previously quit due to side effects or lack of efficacy.{{Jimenez-Cauhe, J., Saceda-Corralo, D., Rodrigues-Barata, R., Hermosa-Gelbard, A., Moreno-Arrones, O.M., Fernandez-Nieto, D., Vano-Galvan, S. (2019). Effectiveness And Safety Of Low-Dose Oral Minoxidil In Male Androgenetic Alopecia. Journal Of The American Academy Of Dermatology. 81(2). 648-649. Available at: https://doi.org/10.1016/j.jaad.2019.04.054}}
Lower doses of oral minoxidil may still be effective in stabilizing progression. In one study, 0.25 mg minoxidil achieved a response rate of 60% in men with AGA. That’s lower than what is typically seen at 2.5-5 mg concentrations, but it is favourable nevertheless.{{Pirmez, R., Salas-Callo, C.I. (2020). Very-Low-Dose Oral Minoxidil In Male Androgenetic Alopecia: A Study With Quantitative Trichoscopic Documentation. Journal Of The American Academy Of Dermatology. 82(1). E21-E22. Available at: https://doi.org/10.1016/j.jaad.2019.08.084}}
How Safe is Oral Minoxidil?
At low doses, oral minoxidil is generally well tolerated, but side effects are more common than with topical minoxidil because the drug circulates systemically.{{Vañó-Galván, S., Pirmez, R., Hermosa-Gelbard, A., Moreno-Arrones, Ó. M., Saceda-Corralo, D., Rodrigues-Barata, R., Jimenez-Cauhe, J., et al. (2021). Safety of low-dose oral minoxidil for hair loss: a multicenter study of 1404 patients. Journal of the American Academy of Dermatology. 84(6). 1644–1651. Available at: https://doi.org/10.1016/j.jaad.2021.02.054}}
The most common side effects include hypertrichosis, mild fluid retention or ankle swelling, and lightheadedness, particularly when starting or increasing the dose.
Less commonly, oral minoxidil can affect heart rate or cardiac function. Rare but serious events (e.g., pericardial effusion) have been reported, particularly in people with underlying cardiovascular or renal issues. Most side effects are dependent on the dose and often improve with dose reduction or discontinuation.
If you’re considering starting oral minoxidil treatment, start with a lower dose and only increase gradually if it is needed. Splitting the dose between morning and evening can improve tolerability for some. If results plateau, oral minoxidil is often combined with other therapies such as microneedling or topical agents rather than increasing the dose alone.
Oral minoxidil should be used under medical supervision, especially in anyone with cardiovascular, renal, or hepatic concerns.
If you are a member and would like to learn more about oral minoxidil, read our ultimate guide here.
Low-Level Laser Therapy (LLLT)
Ideal For:
- Men with early AGA who are looking to avoid pharmaceutical treatments.
- Men who are willing to be consistent with long-term device use.
- Men willing to pay the costs for device use, either at home or through visits to a clinic.
- Men who are willing to try more experimental methods.
- Men who are willing to try combination treatments, as LLLT will most likely have minimal effects as a standalone solution.
LLLT is therapeutic exposure to red or near-infrared radiation. For hair loss, this involves placing the scalp under infrared-emitting laser diodes. A typical laser therapy session lasts from 20 to 60 minutes, and you can complete them at a doctor’s office, with a take-home laser helmet, or even with a laser brush.
Laser diodes for hair loss emit red light at wavelengths of 630-670 nanometers. The sun emits wavelengths from 250 to 2,500 nanometers. LLLT is essentially exposure to one part of the sun’s spectrum for a controlled period of time. It turns out that some wavelengths show benefits to human physiology, from wound healing to inflammation resolution and even hair recovery.
Currently, there is still speculation about how LLLT actually works for hair regrowth. Potential explanations include:
- The laser’s heat activates heat shock proteins.{{Wikramanayake, T.C., Rodriguez, R., Choudhary, S., Mauro, L.M., Nouri, K., Schachner, L.A., Jimenez, J.J. (2012). Effects of the Lexington LaserComb on Hair Regrowth in the C3H/HeJ Mouse Model of Alopecia Areata. Lasers in Medical Science. 27(2). 431-436. Available at: https://doi.org/10.1007/s10103-011-0953-7}}
- The laser’s light increases tissue oxygenation.{{Chung, H., Dai, T., Sharma, S.K., Huang, Y.Y., Carroll, J.D., Hamblin, M.R. (2012). The Nuts and Bolts of Low-Level Laser (Light) Therapy. Annals of Biomedical Engineering. 40(2). 516-533. Available at: https://doi.org/10.1007/s10439-011-0454-7}}
- The laser’s light increases blood flow.{{Makihara, E., Masumi, S. (2008). Blood Flow Changes of a Superficial Temporal Artery Before and After Low-Level Laser Irradiation Applied to the Temporomandibular Joint Area. Nihon Hotetsu Shika Gakkai Zasshi. 52(2). 167-170. Available at: https://doi.org/10.2186/jjps.52.167}}
- The laser’s light generates acute tissue inflammation.{{Bouzari, N., Firooz, A.R. (2006). Lasers May Induce Terminal Hair Growth. Dermatologic Surgery. 32(3). 460. Available at: https://doi.org/10.1111/j.1524-4725.2006.32092.x}}
- The laser’s light can inhibit 5AR.
Clinical Evidence for Low-Level Laser Therapy
Clinical trials of LLLT devices for AGA generally report modest improvements in hair density versus placebo (sham) devices. A systematic review and meta-analysis of seven randomized controlled trials using FDA-approved home-use LLLT devices found significantly greater increases in hair density in treated participants compared with sham controls in both men and women, particularly with helmet and comb-type devices.{{Lueangarun, S., Visutjindaporn, P., Parcharoen, Y., Jamparuang, P., Tempark, T. (2021). A Systematic Review and Meta-Analysis of Randomized Controlled Trials of United States Food and Drug Administration-Approved, Home-Use, Low-Level Light/Laser Therapy Devices for Pattern Hair Loss: Device Design and Technology. Journal of Clinical and Aesthetic Dermatology. 14(11). E64-E75}}
In a recently published study, they investigated the effects of using a helmet-type LLLT device (646-675 nm) for 20 mins, 3 times per week, on AGA in both men and women (51 men, 17 women) over 48 weeks.
They found that hair density significantly increased from baseline from 99.2 to 124.2 hairs/cm2, and mean hair shaft thickness increased from 65.1 to 74.9 μm. Also, 59% of participants were rated as improved based on global photographs, and over 85% expressed satisfaction with treatment.{{Shin, J.W., Paik, K., Na, J.I., Lew, B.L., Huh, C.H. (2026). Long-Term Efficacy and Safety of Low-Level Laser Therapy for Androgenetic Alopecia: A 12-Month Prospective Trial. Dermatologic Therapy. Available at: https://doi.org/10.1155/dth/6621458}}
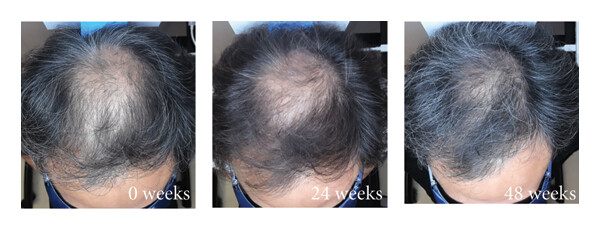
Figure 5. Investigator-assessed clinical improvement over time after use of an LLLT device. Adapted from Figure 3a.{{Shin, J.W., Paik, K., Na, J.I., Lew, B.L., Huh, C.H. (2026). Long-Term Efficacy and Safety of Low-Level Laser Therapy for Androgenetic Alopecia: A 12-Month Prospective Trial. Dermatologic Therapy. Available at: https://doi.org/10.1155/dth/6621458}} Used under Creative Commons license.
However, based on anecdotal evidence from our members, we have not seen a single case where LLLT has worked, so take this information with a pinch of salt.
There is also a broader methodological issue with LLLT device trials that is worth noting. Human hair growth shows seasonal variation, with increased telogen shedding often happening in late summer and early autumn in the Northern Hemisphere.
Because many LLLT devices emit wavelengths that overlap with natural sunlight exposure, trial timing across this seasonal window could theoretically amplify any differences seen between LLLT devices and sham devices if light exposure modifies the dynamics of seasonal shedding.
This does not invalidate the clinical evidence, but it highlights how environmental biology can also interact with LLLT trials in ways that may exaggerate benefits.
If you’re a member and would like more info on this topic, watch our video here.
How Safe is LLLT?
LLLT is generally safe and well-tolerated for most people. Most effects are mild and localized to the scalp, including scalp warmth, redness, or itching during or after use.
Find out more about LLLT in our article here.
Microneedling
Ideal For:
- Men who are willing to be consistent with use.
- Men who are looking to boost the impact of topical treatment like minoxidil, especially if they’ve seen plateauing results or suspect poor topical response.
Microneedling, also known as percutaneous wound induction, is the act of deliberately wounding skin tissues for therapeutic benefit. This is generally done with hundreds of tiny, medical-grade needles ranging in length from 0.1 to 5.0mm.
There are a variety of microneedling devices, from hand-held rollers to automated pens to stamps. But the ones people are most familiar with (in the hair loss world) are dermarollers. When rolled against the skin, they puncture its top layers to evoke acute inflammation. And yes, being rolled with essentially a tiny lint roller covered in spikes does hurt.
There are multiple possible explanations as to how microneedling may improve AGA:
- Micro-wounding may increase proteins and growth factors linked to hair growth.
- Micro-wounding might downregulate proteins linked to scarring.
- Micro-wounding might promote angiogenesis (new blood vessel formation).
- Microneedling may improve the absorption/efficacy of other hair loss treatments.

Figure 6. Image of a dermaroller
Clinical Evidence for Microneedling
There are many before-and-after photos online from microneedling regimens. If you’d like to see these photos, a user at HairLossTalk has done a great job accumulating them, which you can view here.{{HairLossTalk, (2019), Microneedling Photo Results Summary. Available at: https://www.hairlosstalk.com/interact/threads/microneedling-photo-results-summary.121072/ (Accessed: 24 February 2026)}}
But the more useful question is what the clinical literature shows. Overall, microneedling appears to improve outcomes when combined with other therapies, such as topical minoxidil, finasteride, or platelet-rich plasma (PRP).
A systematic review and meta-analysis of 13 randomized controlled trials showed that microneedling in combination with other treatments resulted in greater improvements in hair density and diameter compared to treatments used alone.{{Pei, D., Zeng, L., Huang, X., Wang, B., Liu, L., Zhang, G. (2024). Efficacy and Safety of Combined Microneedling Therapy for Androgenic Alopecia: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Journal of Cosmetic Dermatology. Available at: https://doi.org/10.1111/jocd.16186}}
Notably, over 12 weeks, once-weekly microneedling plus twice-daily minoxidil increased hair counts by 4X compared with minoxidil alone.{{Dhurat, R., Sukesh, M., Avhad, G., Dandale, A., Pal, A., Pund, P. (2013). A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study. International Journal of Trichology. 5(1). 6-11. Available at: https://doi.org/10.4103/0974-7753.114700}} Also over 6 months, once-weekly microneedling alongside daily finasteride and 5% minoxidil resulted in a +2 or +3 improvement in hair loss gradient for non-responders to both finasteride and minoxidil.{{Dhurat, R., Mathapati, S. (2015). Response to Microneedling Treatment in Men with Androgenetic Alopecia Who Failed to Respond to Conventional Therapy. Indian Journal of Dermatology. 60(3). 260-263. Available at: https://doi.org/10.4103/0019-5154.156361}}
There is also evidence that microneedling may have a standalone benefit. In one 24-week study, microneedling carried out every 14 days produced greater increases in hair density than topical minoxidil alone (23.4 vs 18.8 hairs/cm² from baseline).{{Bao, L., Gong, L., Guo, M., Liu, T., Shi, A., Zong, H. (2020). Randomized Trial of Electrodynamic Microneedle Combined with 5% Minoxidil Topical Solution for the Treatment of Chinese Male Androgenetic Alopecia. Journal of Dermatological Treatment. Available at: https://doi.org/10.1080/14764172.2017.1376094}}
Ultimately, microneedling tends to work best as an adjunct (especially with minoxidil), but it may still offer meaningful benefit as a standalone option for some people.
The choice of needle length also matters. In general, we currently recommend sticking with 0.6-0.8mm needle lengths for automated pens, and 1.0-1.5mm needle lengths for rollers, needling once weekly, or once every two weeks.
To find out more about the best microneedling length, read our article here.
How Safe is Microneedling?
In short-term studies, microneedling is generally safe. The most common side effects are mild and localized, including redness, swelling, itching, pinpoint bleeding, and discomfort during treatment.
Some people also notice temporary flaking in the days after treatment. Scarring is rare when users use a sensible needle depth and avoid overdoing it. But anyone prone to keloid scarring should be cautious.
You can find more information on microneedling and scarring in our article here.
The risk of infection is low with basic hygiene (e.g., clean scalp, clean hands, and proper device sterilization). As a general safety rule, sticking to needle lengths of 2.0 mm or less and avoiding excessive session frequency reduces risk.
If you’re a member, you can learn more about microneedling in our ultimate guide here.
Ketoconazole
Ideal For:
- Men with AGA who also have dandruff, seborrheic dermatitis, oily scalp, or scalp inflammation, as these factors can worsen follicle miniaturization.
- Men with AGA alone, or AGA plus seborrheic dermatitis or telogen effluvium.
- Men with hair shedding disorders where microbial overgrowth or scalp inflammation contributes to shedding may particularly benefit from ketoconazole due to its antifungal and anti-inflammatory effects.
You might have heard about ketoconazole under the brand name Nizoral®, and you might know about it as a shampoo. Ketoconazole is an antifungal medication used to help improve fungal-related conditions such as dandruff, fungal infections, certain hormone-linked diseases, and even hair loss from fungal and non-fungal causes.
Figure 7. Structure of ketoconazole. Adapted from Wikimedia.{{Wikimedia Commons, (2025), Ketoconazole Chemical Structure (SVG). Available at: https://commons.wikimedia.org/wiki/Category:Ketoconazole#/media/File:(2S,4R)-Ketoconazol.svg (Accessed: 24 February 2026)}} Image in the public domain.
Ketoconazole may improve telogen effluvium by killing scalp pathogens, thereby normalizing excessive hair shedding triggered by microorganism-mediated inflammation. It may also prolong the anagen phase of the hair cycle.
Ketoconazole may improve AGA via three key mechanisms:
- Killing pathogens in the scalp, therefore normalizing excessive hair shedding triggered by microorganism-mediated inflammation.
- Reducing scalp DHT levels by inhibiting 5-alpha reductase (a key enzyme that converts testosterone to DHT) and blocking androgen receptors (“landing pads” for DHT to exert its effects).
- Prolonging the anagen phase of the hair cycle.
You can buy 1% ketoconazole shampoo over the counter, typically at around $16 for 200 mL. Whereas, 2% ketoconazole shampoo usually requires a prescription.

Figure 8. Image of Nizoral shampoo, containing 1% ketoconazole. Available at Walmart.
Clinical Evidence for Ketoconazole
Clinical studies on ketoconazole shampoo, especially 2% strength, provide evidence that ketoconazole can improve hair parameters in men with AGA, including hair density, shaft diameter, and the proportion of hairs in the anagen phase.
In one study involving men with AGA comparing 2% ketoconazole shampoo with a non-medicated shampoo over 21 months, ketoconazole showed progressive increases in a composite hair growth index (anagen percentage × shaft diameter). Those using standard shampoo experienced a gradual decline.{{Piérard-Franchimont, C., De Doncker, P., Cauwenbergh, G., Piérard, G.E. (1998). Ketoconazole Shampoo: Effect of Long-Term Use in Androgenic Alopecia. Dermatology. 196(4). 474-7. Available at: https://doi.org/10.1159/000017954}}
Also, a pilot study showed that 2% ketoconazole may produce hair shaft diameter improvements similar to 2% minoxidil, with reductions in sebaceous gland size, which was not seen in the minoxidil-only group.{{Piérard-Franchimont, C., De Doncker, P., Cauwenbergh, G., Piérard, G.E. (1998). Ketoconazole Shampoo: Effect of Long-Term Use in Androgenic Alopecia. Dermatology. 196(4). 474-7. Available at: https://doi.org/10.1159/000017954}}
Evidence for 1% ketoconazole is weaker but still supportive. In men with AGA associated with dandruff or telogen effluvium, 1% ketoconazole used 2 to 3 times per week reduced hair shedding and increased anagen hair proportion and shaft diameter over 6 months.{{Piérard-Franchimont, C., Goffin, V., Henry, F., Uhoda, I., Braham, C., Piérard, G.E. (2002). Nudging Hair Shedding By Antidandruff Shampoos: A Comparison Of 1% Ketoconazole, 1% Piroctone Olamine And 1% Zinc Pyrithione Formulations. International Journal Of Cosmetic Science. 24(5). 249-256. Available at: https://doi.org/10.1046/j.1467-2494.2002.00145.x}}
Ketoconazole also tends to work well when used in combination with other treatments. In one study, finasteride plus ketoconazole demonstrated improvements in self- and physician-assessments.{{Khandpur, S., Suman, M., Reddy, B.S. (2002). Comparative Efficacy Of Various Treatment Regimens For Androgenetic Alopecia In Men. J Dermatol. 29(8). 489-98. Available at: https://doi.org/10.1111/j.1346-8138.2002.tb00314.x}}
Based on the available clinical evidence, there is stronger support for the use of 2% ketoconazole shampoo for hair growth than for 1%. But, as there are currently no direct head-to-head studies comparing the effectiveness of 1% ketoconazole shampoo versus 2% for hair regrowth, this is purely speculative.
How Safe is Ketoconazole?
Ketoconazole shampoo is generally safe and well-tolerated when used as directed. Because it is applied briefly to the scalp and then rinsed off, systemic absorption is minimal, and side effects are usually limited to mild, local scalp irritation or dryness.
Leave-on topical ketoconazole is available in some countries, but this increases the risk of systemic exposure. These non-shampoo formulations have not been studied for hair loss in humans. So even though in theory topical ketoconazole may seem more effective, it’s sensible to stick with ketoconazole shampoo, which has science-backed evidence.
Oral ketoconazole has significant systemic risks, but these concerns do not apply to shampoo use due to the much lower exposure. Overall, 2% ketoconazole shampoo has a favourable safety profile when used a few times per week.
If you’re a member, you can find out more information on ketoconazole in our ultimate guide here.
Saw Palmetto
Ideal For:
- Men with early to mid-stage AGA.
- Men who want to avoid pharmaceutical options.
- Men who are willing to try combinational treatments.
Saw palmetto (Serenoa repens) is a palm plant native to the Southeastern United States. It grows up to 10 feet tall and can live over 700 years. It’s a botanical extract used for hair loss because it can reduce 5AR activity and may lower DHT signalling.
Saw palmetto is different from finasteride and dutasteride as it is not a standardized pharmaceutical. So its strength can vary across products depending on how it is harvested and extracted.
Saw palmetto is available in both oral and topical formulations (serums/lotions/shampoos).
[ulo_promo title=”All-Natural Hair Topical” subtitle=”The top natural ingredients for hair growth, all in one serum.” description=”Take the next step in your hair growth journey with a world-class natural serum. Ingredients, doses, & concentrations built by science. ” button_text=”Shop Serums” button_url=”https://ulo.co/discount/perfecthairhealth15?redirect=/products/hair-growth-serum?variant=41588624392271” prescription=”true” type=”otc-serum” ]
Clinical Evidence for Saw Palmetto
Overall, the clinical evidence for saw palmetto is mixed and tends to be of lower quality than the evidence that is available for pharmaceutical treatments like finasteride, minoxidil, or dutasteride.
Nevertheless, there is some clinical evidence to back this treatment. In one 16-week randomized controlled trial involving adults with AGA, both oral and topical standardized saw palmetto oil (named VISPO™) significantly reduced hair shedding compared to placebo and produced small increases in hair density (around 5-7%). Oral saw palmetto also reduced serum DHT, whereas topical did not.{{Sudeep, H.V., Rashmi, S., Jestin, T.V., Richards, A., Gouthamchandra, K., Shyamprasad, K. (2023). Oral And Topical Administration Of A Standardized Saw Palmetto Oil Reduces Hair Fall And Improves The Hair Growth In Androgenetic Alopecia Subjects – A 16-Week Randomized, Placebo-Controlled Study. Clinical, Cosmetic And Investigational Dermatology. 16. 3251–3266. Available at: https://doi.org/10.2147/CCID.S435795}}
Also, in one study, oral saw palmetto (320 mg/day) was compared to finasteride (1 mg/day) in 100 men with mild to moderate AGA over 24 months. Hair regrowth assessed by global photographic assessment was reported 38% of the saw palmetto group compared to 68% in the finasteride group.{{Rossi, A., Mari, E., Scarno, M., Garelli, V., Maxia, C., Scali, E., Iorio, A., Carlesimo, M. (2012). Comparitive Effectiveness of Finasteride vs Serenoa Repens in Male Androgenetic Alopecia: A Two-Year Study. International Journal of Immunopathology and Pharmacology. 25(4). 1167-1173. Available at: https://doi.org/10.1177/039463201202500435}}
What people often miss from this study is that of those saw palmetto users, 45/50 men saw a stop in hair loss. In fact, that number was the same in the finasteride group (45/50). In other words, saw palmetto stopped the progression of hair loss in 90% of men. And even better, the saw palmetto group also reported zero side effects.{{Rossi, A., Mari, E., Scarno, M., Garelli, V., Maxia, C., Scali, E., Iorio, A., Carlesimo, M. (2012). Comparitive Effectiveness of Finasteride vs Serenoa Repens in Male Androgenetic Alopecia: A Two-Year Study. International Journal of Immunopathology and Pharmacology. 25(4). 1167-1173. Available at: https://doi.org/10.1177/039463201202500435}}
In terms of topical saw palmetto, this formulation tends to look more effective for hair regrowth when combined with other hair growth-supporting ingredients.{{Wessagowit, V., Tangjaturonrusamee, C., Kootiratrakarn, T., Bunnag, T., Pimonrat, T., Muangdang, N., Pichai, P. (2016). Treatment of Male Androgenetic Alopecia with Topical Products Containing Serenoa Repens Extract. Australasian Journal of Dermatology. 57(3). e76-e82. Available at: https://doi.org/10.1111/ajd.12352}} But it’s difficult to see how much contribution saw palmetto made because it has been studied in multi-ingredient blends.
There is one 24-week pilot study published on topical saw palmetto, but they reported a very large increase in terminal-hair count of 74.1%, and the study lacked a placebo control, so we recommend taking these results with a pinch of salt.{{Wessagowit, V., Tangjaturonrusamee, C., Kootiratrakarn, T., et al. (2016). Treatment of male androgenetic alopecia with topical products containing Serenoa repens extract. Australas J Dermatol. 57(3), e76-e82. Available at: https://doi.org/10.1111/ajd.12352}}
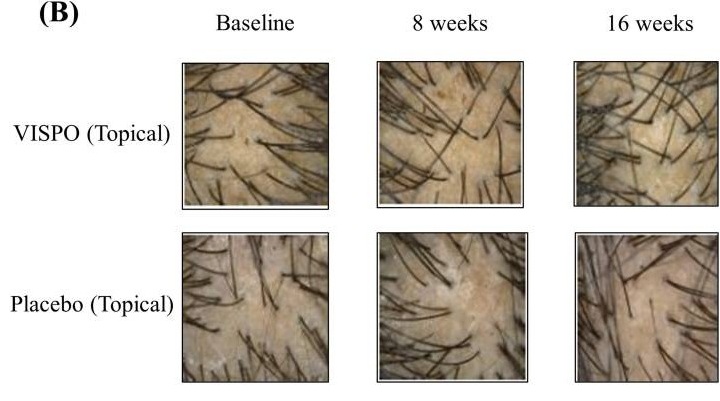
Figure 9: Images showing changes in scalp hair following 16-week treatment of VISPO™ oil or a placebo oil. Adapted from Figure 4.{{Sudeep, H.V., Rashmi, S., Jestin, T.V., Richards, A., Gouthamchandra, K., Shyamprasad, K. (2023). Oral and Topical Administration of a Standardized Saw Palmetto Oil Reduces Hair Fall and Improves the Hair Growth in Androgenetic Alopecia Subjects – A 16-Week Randomized, Placebo-Controlled Study. Clin Cosmet Investig Dermatol. 16, 3251-3266. Available at: https://doi.org/10.2147/CCID.S435795}} Image obtained in line with the Creative Commons License.
How Safe is Saw Palmetto?
Saw palmetto is generally safe and well-tolerated. The most common adverse effects of oral saw palmetto include stomach upset, headache, or fatigue. Sexual side effects are uncommon compared to pharmaceutical 5AR inhibitors (e.g., finasteride and dutasteride).
For topical saw palmetto, most of the effects are localized to the scalp, including inflammation, itching, dryness, and flaking.
Because saw palmetto supplements are not tightly regulated, the quality and strength of the product can vary across brands, which can affect the safety and tolerability.
Find out more about saw palmetto in our article here.
General Guidelines for Use
When starting hair loss treatment, it can feel daunting and difficult to know where to begin. While each treatment has its own considerations around dosing, frequency, and application, some general tips and recommendations could help when starting any new hair loss treatment:
- Speak to a clinician first: This is especially important for any prescription treatments or if you have any underlying health concerns, risk factors, or fertility plans.
- Give treatments enough time: Most evidence-based hair loss treatments take at least 3 to 6 months before meaningful changes are visible.
- Track your progress: Take consistent photographs in the same lighting and at the same angle. This makes it much easier to assess whether something is working or isn’t.
- Monitor any side effects: If you do notice any unwanted effects, it’s important to discuss any adjustments or alternatives with a licensed clinician rather than pushing through discomfort.
- Prioritize consistency: The best treatment is one you can use consistently over time. If you’re not able to stick with it, even a strong medication won’t work as well as it should.
- Adjust when needed: Hair loss changes over time, and treatment plans must be able to evolve with it.
Final Thoughts
Ultimately, there is no single best hair loss treatment for men. The right choice depends on your specific pattern of hair loss, your goals, and your preferences. Whether that’s a prescription medication, an over-the-counter option, a natural approach like saw palmetto, or a technique like microneedling.
What matters is choosing a hair loss treatment you can tolerate and stick with consistently over time. Hair loss treatment is rarely about finding the strongest option. It’s more about finding one that you can realistically fit into your routine and that you are comfortable maintaining.
With the right expectations and a tailored plan, many men are able to stabilize their hair loss and maintain hair growth improvements over time.
Men’s hair loss is a booming multi-billion-dollar industry, yet the vast majority of over-the-counter products fall short when measured against rigorous clinical evidence. This landscape is cluttered with quick-fix promises, leaving consumers sifting through marketing claims with little scientific support. Among all topical hair regrowth options, minoxidil is one of the most extensively studied. It is also one of two FDA-approved treatments for male pattern hair loss (in its topical form).
In this comprehensive guide, we rank our top minoxidil picks of 2026 across Best Overall, Best Value, and other categories to help you navigate the crowded hair loss market with more clarity and confidence.
Quick Look: Best Minoxidil for Men in 2026
Product Strength Format Customization Price Best: Ulo 7% Solution High $41.65 Overall Kirkland Minoxidil 5% Solution None $17.99 Value Rogaine 5% Solution/Foam None $49.97 Sensitive Scalp Keeps 5% Solution/Foam/Spray Low $16.67 Subscription Convenience Happy Head 5-8% Solution/Gel High $59 Strength What is Minoxidil and How Does it Work?
Minoxidil was originally developed to treat high blood pressure and is now widely used in both topical and oral forms as a first-line therapy for androgenic alopecia (AGA).
What is Minoxidil?
Minoxidil was first introduced in the 1970s as a powerful oral vasodilator for resistant hypertension. Clinicians soon noticed a frequent side effect, generalized increased hair growth (hypertrichosis).{{Gupta, A.K., Talukder, M., Venkataraman, M., Bamimore, M.A. (2021). Minoxidil: a comprehensive review. Journal of Dermatological Treatment. 33(4). 1896-1906. Available at: https://doi.org/10.1080/09546634.2021.1945527}} This led to the development of topical formulations specifically for AGA. Today, 2-5% topical minoxidil is FDA-approved for both male and female pattern hair loss and is used off-label for other alopecias.
How Does Minoxidil Work?
Minoxidil is a potassium-channel opener that causes vasodilation and improves microcirculation around hair follicles.{{Hussein, R.S., Dayel, S.B., Abahussein, O., El-Sherbiny, A.A. (2024). Applications and efficacy of minoxidil in dermatology. Skin Health and Disease. 4(6). E472. Available at: https://doi.org/10.1002/ski2.472}} It also acts as a prodrug; sulfotransferase converts it to minoxidil sulfate, which prolongs the anagen (growth) phase and shortens the telogen (resting) phase, shifting more hair follicles into active growth.{{Pietrauszka, K., Bergler-Czop, B. (2020). Sulfotransferase SULT1A1 activity in hair follicle, a prognostic marker of response to the minoxidil treatment in patients with androgenetic alopecia: a review. Advances in Dermatology and Allergology. 39(3). 472-478. Available at: https://doi.org/10.5114/ada.2020.99947}} Additional data suggests that induction of key growth factors like vascular endothelial growth factor (VEGF) and activation of Wnt/ꞵ-catenin signaling further support hair regrowth.{{Gupta, A.K., Talukder, M., Shemer, A., Piraccini, B.M., Tosti, A. (2023). Low-Dose Oral Minoxidil for Alopecia: A Comprehensive Review. Skin Appendage Disorders. 9(6). 423-437. Available at: https://doi.org/10.1159/0000531890}}
Although minoxidil doesn’t target dihydrotestosterone, it can improve the effectiveness of other treatments by targeting multiple other targets. When combined with anti-DHT drugs like finasteride, which reduce the hormonal trigger of AGA, minoxidil provides a complementary, non-hormonal pathway. The two treatments have been shown to provide synergistic improvement in hair density in men.{{Asad, N., Naseer, M., Ghafoor, R. (2024). Efficacy of Topical Finasteride 0.25% with Minoxidil 5% versus Topical Minoxidil 5% Alone in Treatment of Male Pattern Androgenic Alopecia. Journal of Drugs in Dermatology. 23(11). 1003-1008. Available at: https://doi.org/10.36849/JDD.7826}}
OTC vs Prescription-Strength
Over-the-counter (OTC) minoxidil solutions (2% and 5%) can be effective for many men, but absorption and vehicle limits mean “stronger” drug percentages above 5% often add irritation rather than results unless the entire formulation is engineered and supervised medically.
Early minoxidil development work showed a clear dose-response between low strengths (1-2%) and mid-strength (5%) solutions, with 5% yielding larger gains in hair counts and shaft diameter in AGA.{{Olsen, E.A., Dunlap, F.E., Funicella, T., Koperski, J.A., Swinehart, J.M., Tschen, E.H., Trancik, R.J. (2002). A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men. Journal of the American Academy of Dermatology. 47(3). 377-385. Available at: https://doi.org/10.1067/mjd.2002.124088}}
Other companies offer concentrations of 10% or over; however, recent head-to-head studies have shown that 5% topical minoxidil is moderately superior to the higher concentration.{{Ghonemy, S., Alarawi, A., Bessar, H. (2021). Efficacy and safety of a new 10% topical minoxidil versus 5% topical minoxidil and placebo in the treatment of male androgenetic alopecia: a trichoscopic evaluation. Journal of Dermatological Treatment. 32(2). 236-241. Available at: https://doi.org/10.1080/09546634.2019.1654070}} Additionally, the 10% minoxidil was associated with more marked irritation.
So, with that in mind, let’s take a look at some of our top minoxidil picks of 2026.
Best Minoxidil Picks for Men
#1 Best Overall: Ulo Minoxidil Rx
Pros: Cons: ✓ Clinically-backed combinations ✗Prescription products are only available in the USA ✓ Ongoing medical monitoring and a user-friendly platform ✓ Quality-tested ingredients free of irritants Ulo’s Minoxidil Rx takes the top spot for men who want a data-driven, medically supervised approach rather than a one-size-fits-all bottle. Custom strengths and evidence-based optional add-ons allow precise targeting for hair regrowth.
Their high-strength concentration can be combined with tretinoin 0.01% to enhance absorption and efficacy, as well as cetirizine 1%, melatonin 0.01% for antioxidant protection, and caffeine 0.2% to boost circulation, which further improves the product’s effectiveness.
This treatment begins at $49 per month, increasing to $54 if you choose to have all of the add-ons.
Bottom Line: Ulo’s customizable, science-driven minoxidil prescription offers one of the most advanced, value-conscious options for men who are serious about long-term hair regrowth.
#2 Best Value – Kirkland Signature Minoxidil 5%

Pros: Cons: ✓ Lowest cost we could find for 6 months’ worth. ✗Contains propylene glycol, which can cause irritation or dryness in some users. ✓ Same core 5% minoxidil strength. ✗ No customization possible for strength or add-on ingredients. ✓ Widely available at multiple stores, including Amazon, Costco, etc. ✗ No medical consultation or tailoring of treatment included. ✓ Simple formula. Kirkland Signature Minoxidil 5% is the classic value choice for me who want an over-the-counter treatment without paying for branding or bundled medical services. You get a standard 5% solution similar in strength to more expensive competitors, making it ideal for cost-conscious users who are happy to follow a simple twice-daily routine and do not need personalized compounding.
Bottom line: If you want the most affordable entry point into 5% minoxidil, Kirkland’s no-frills formula is hard to beat for sheer value per effective dose.
#3 Best for Sensitive Scalps: Rogaine 5% Foam

Pros: Cons: ✓ Clinically proven 5% minoxidil strength ✗On the higher end in terms of price. ✓ Foam vehicle is propylene glycol-free, so it is usually better tolerated on sensitive or irritated scalps. ✗ Fixed strength for men with no customization or add-on actives. ✓ Quick drying, less greasy texture ✗ No medical consultation or tailoring of treatment included. ✓ Widely available OTC Rogaine 5% is a strong pick for men who need minoxidil but find traditional liquid formulas too irritating or cosmetically heavy. The foam format avoids common irritants found in many solutions and tends to be more comfortable for daily use, which can improve adherence and long-term outcomes.
Bottom Line: For sensitive scalps that still need full-strength 5% minoxidil, Rogaine Foam provides a gentler, easy-to-use option that balances proven efficacy with better tolerability.
#4 Best Subscription Convenience: Keeps Minoxidil

Pros: Cons: ✓ Automatic subscription refills so you rarely run out or miss doses. ✗More expensive than buying generic minoxidil in bulk. ✓ Offers both 5% foam and 5% solution to suit different scalp and styling preferences. ✗ Limited to preset strengths and formulas with no true custom compounding. ✓ Option to bundle with finasteride and other treatments for a complete regimen. ✓ Online prescribing and follow-up. Keeps Minoxidil is designed for men who value a set-and-forget routine, trading a price increase ($16.67 for 3 months compared to Kirkland’s $17.99 for 6 months) for automatic deliveries and integrated telehealth support. The ability to pair minoxidil with finasteride and keep everything managed through a single platform could make adherence simpler for busy users.
Bottom Line: If you want 5% minoxidil with minimal hassle, Keeps’ subscription model is a strong fit for convenience-focused men who prefer not to manage refills and prescriptions on their own.
#5 Best High-Strength Formula: Happy Head

Pros: Cons: ✓ Offers high-strength minoxidil concentrations beyond standard 5%. ✗Higher strengths may carry a greater risk of irritation or systemic absorption. ✓ Can be combined with topical finasteride and other actives in a single solution. ✗ More expensive than generic 5% minoxidil and some standard telehealth offerings. ✓ Telehealth model with online consultation and prescription management. ✗Corticosteroids used to offset irritation from propylene glycol. ✓ Multiple formula options aimed at men who have plateaued on basic OTC products. Happy Head is built for men who want to move past entry-level minoxidil and explore higher-strength, prescription-only blends under medical oversight. By pairing elevated minoxidil concentrations (8%) with agents like tretinoin and topical finasteride, Happy Head targets users seeking a more comprehensive protocol. With that said, some ingredients included, like the carrier agent propylene glycol, which is used in their base formula, can cause irritation. To offset this, Happy Head uses corticosteroids; however, this may cause skin thinning long-term.
You can read more about corticosteroid usage in hair loss treatments here.
Bottom Line: Happy Head delivers a good jump in strength for minoxidil users who need to increase efficacy.
Timeline: What Results to Expect from Minoxidil
It’s important that realistic expectations are set for regrowth when starting out on your minoxidil usage journey.
Timeframe What to Expect Clinical Evidence Months 0-3 This is the initial shedding phase, which usually resolves in the first 4-8 weeks. {{Nohria, A., Desai, D., Sikora, M., Mandal, S., Shapiro, J., Lo Sicco, K. (2024). Combating “dread shed”: The impact of overlapping topical and oral minoxidil on temporary hair shedding during oral minoxidil initiation. JAAD International. 15. 220-224. Available at: https://doi.org/10.1016/j.jdin.2024.03.005}} Months 3-6 Early visible improvements, like the appearance of new hairs, can be expected. {{Amit, K., Mansukh, G., Satyaprakash, M., Dhiraj, D., Hanmant, B. (2023). Real-World Effectiveness, Safety, and Tolerability of Cetosomal Minoxidil 5% Alone and a Fixed Drug Combination of Cetosomal Minoxidil 5% With Finasteride 0.1% in the Management of Androgenetic Alopecia (Inbilt Study). Cureus. 15(7). E41681. Available at: https://doi.org/10.7759/cureus.41681}} Months 6-12 Cosmetic changes peak, with stronger hair, increased density, and most coverage is seen. {{Katz, H.I., Hien, N.T., Prawer, S.E., Goldman, S.J. (1987). Long-term efficacy of topical minoxidil in male pattern baldness. Journal of the American Academy of Dermatology. 16(3). 711-718. Available at: https://doi.org/10.1016/s0190-9622(87)70092-9}} Months 12+ Further gains plateau, continued use needed to maintain improvements. {{Katz, H.I., Hien, N.T., Prawer, S.E., Goldman, S.J. (1987). Long-term efficacy of topical minoxidil in male pattern baldness. Journal of the American Academy of Dermatology. 16(3). 711-718. Available at: https://doi.org/10.1016/s0190-9622(87)70092-9}} Consistency is Everything
Minoxidil works by prolonging the anagen phase and shortening the telogen phase. Regular dosing maintains these effects at the follicle level; repeatedly missing applications reduces the cumulative time that hair follicles spend in a pro-growth, anagen-biased state.{{Messenger, A.G., Rundegren, J. (2004). Minoxidil: mechanisms of action on hair growth. British Journal of Dermatology. 2(1). 186-194. Available at: https://doi.org/https://doi.org/10.1111/j.1365-2133.2004.05785.x}}
Because human scalp follicles cycle slowly (anagen can last years), many follicles need months of uninterrupted exposure before visible density gains can be seen.{{Hoover E, Alhajj M, Flores JL. Physiology, Hair. [Updated 2023 Jul 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499948/ (Accessed: November 2025)}} This is why most guidance recommends at least 6 months of continuous use before judging the response.
Why Stopping Reverses Progress
Minoxidil is not disease-modifying for AGA, meaning that it does not correct androgen-driven miniaturization but counteracts it while present by improving hair cycle dynamics and follicle size. When treatment is stopped, these pharmacologic effects wane, and follicles gradually revert toward their genetically determined, androgen-sensitive pattern.
Clinical and patient information sources consistently note that any gain from minoxidil is maintained only while therapy continues. After discontinuation, increased shedding and loss of density over months are typical, ultimately leading to a reversal of gains to the original starting point.
What Minoxidil Formulations are Available?
You can buy minoxidil in several different vehicles that differ mainly in tolerability, practicality, and how well they fit a given scalp and routine. Choosing the “best” format is less about raw efficacy and more about matching the base to skin sensitivity and your preference of application.
- Foam – Best for Sensitive Skin: Propylene glycol-free foams were developed to reduce contact dermatitis and dryness seen with classic liquid solutions. Reviews note lower rates of irritation and quicker drying, which makes them better for patients with reactive or dry scalps.{{Purnak, T., Senel, E., Sahin, C. (2011). Liquid formulation of minoxidil versus its foam formulation. Indian Journal of Dermatology. 56(4). 462. Available at: https://doi.org/10.4103/0019-5154.84714}}
- Liquid – Best for Cost-Effectiveness: Traditional solutions with alcohol and propylene glycol are widely available, inexpensive, and easy to use, but they may cause increased itching, flaking, and stinging. This formulation may suit users with non-sensitive skin who are price-conscious.
- Spray – Easiest for Coverage: Spray tops or aerosolized formats can make it faster to hit broad thinning areas, especially in longer hair. However, the product may end up more on the hair shafts or adjacent skin.
- Gel – Targeted and Controlled: Gel or cream-gel vehicles (often from compounders) sit where you place them, minimize dripping, and are useful for localized areas such as temples or post-transplant zones.
- Liposomal Delivery: Newer liposomal or phospholipid bases aim to enhance follicular penetration while limiting systemic absorption and irritation. This is usually marketed as an “advanced delivery” method.
Side Effects and Safety
Minoxidil is generally well tolerated, but like any active drug, it can cause local irritation, a transient shedding phase, and very rare systemic effects, especially in people with underlying skin or cardiovascular issues.
Common local side effects include:
- Itching
- Flaking
- Redness
- Burning
- Temporary shedding
Systemic and heart-related side effects are very rare with correctly used topical minoxidil, but case reports and product information advise seeking medical help if symptoms like chest pain, palpitations, dizziness, or unexplained swelling occur, as these could reflect systemic absorption or accidental ingestion. Risk is higher with oral minoxidil or overdose, where hypotension, tachycardia, and even heart failure have been documented.{{Tripathee, S., Benyovszky, A., Devbhandari, R., Quiza, K., Boris, J. (2024). A Very Bad Hair Day: Minoxidil Ingestion Causing Shock and Heart Failure. Cureus. 16(8). E66039. Available at: https://doi.org/10.7759/cureus.66039}}
To minimize problems, many clinicians suggest starting once daily and titrating up, choosing foam or gentler vehicles to reduce dermatitis, and using custom compounded formulas (for example, lower alcohol, lower strength, or liposomal bases) in those with sensitive or disease-prone scalps.
People with chronic inflammatory scalp conditions such as active psoriasis, eczema, or severe seborrheic dermatitis are typically advised to get the primary condition under control before adding topical minoxidil or other actives, as applying them to an inflamed barrier increases irritation, may worsen the disease, and can unpredictably alter absorption.{{Junge, A., Jic-Hoesli, S.R., Bossart, S., Simon, D., de Viragh, P., Hunger, R.E., Heidemeye, K., Seyed Jafari, S.M. (2025). Contact Dermatitis Caused by Topical Minoxidil: Allergy or Just Irritation. Acta Dermato-Venereologica. 105. 42401. Available at: https://doi.org/10.2340/actadv.v105.42401}}
Final Verdict – Best Minoxidil for Men in 2026
In 2026, several minoxidil-based options stand out for different priorities, from cost to customization. All of them rely on the same core ingredient, but vehicle, strength, and add-ons make a real-world difference in adherence and results.
Whichever route you choose, there is strong evidence that consistent minoxidil use can stabilize loss and improve density for many men, and modern platforms make it easier than ever to find a formulation that fits your scalp, schedule, and risk tolerance.
IngredientsPharmaceuticalsNatural RemediesCompany Reviews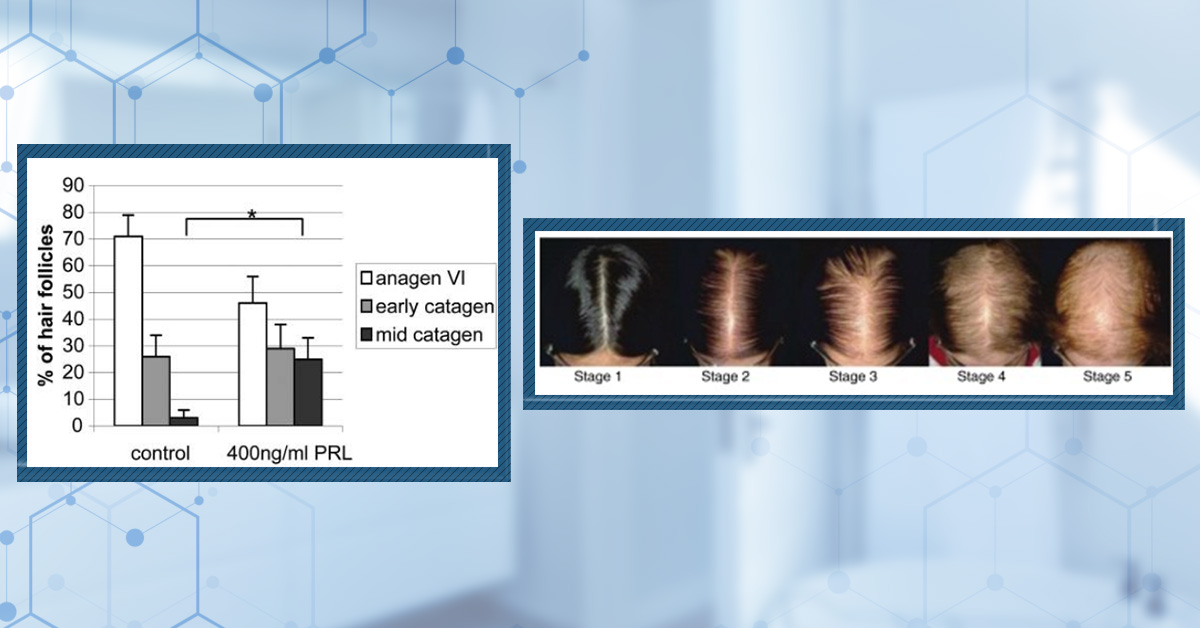 By Sarah King, PhDJun 30, 2026
By Sarah King, PhDJun 30, 2026Which Hormones Cause Hair Loss in Females?
Hair loss in women isn’t driven by a single hormone or pathway. While androgens like DHT play a role in some cases, factors such as estrogen decline, adrenal hormones, prolactin, and chronic stress can all disrupt normal hair cycling. This article explores the evidence behind each hormone and explai...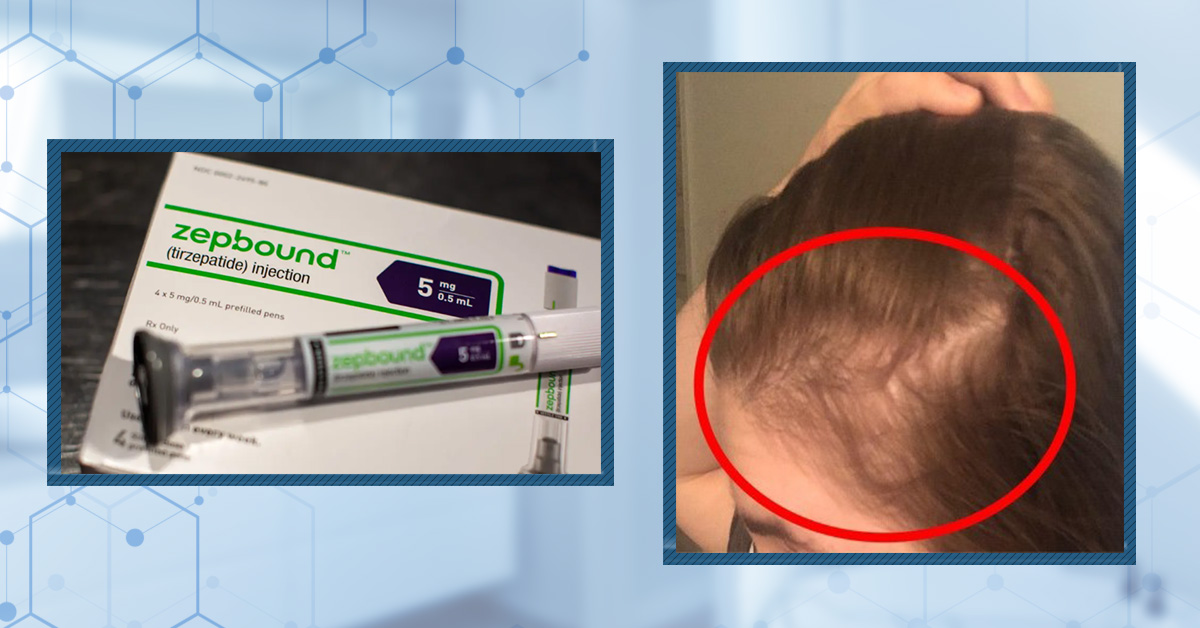 By Cassie Hopton, PhDJun 26, 2026
By Cassie Hopton, PhDJun 26, 2026Does Zepbound Cause Hair Loss?
Zepbound is a GLP-1 medication FDA-approved as a treatment for chronic weight management. But could it also cause hair loss? Reports from users provide anecdotal evidence that this drug may contribute to hair thinning. In this article, we break down the science behind these reports: what Zepbound is...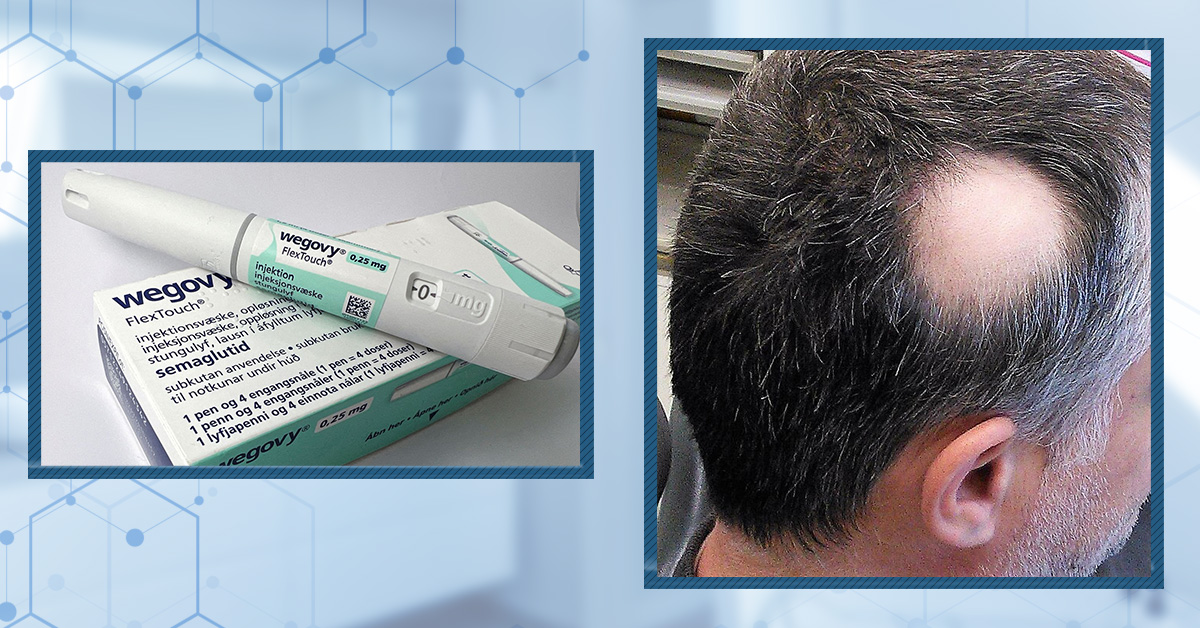 By Cassie Hopton, PhDJun 19, 2026
By Cassie Hopton, PhDJun 19, 2026Does Wegovy Cause Hair Loss?
GLP-1 medications like Ozempic and Wegovy are transforming weight loss and diabetes care, but increasing reports of hair loss have raised concerns. Are these treatments really causing shedding, or is something else at play? In this article, we examine the current evidence, explore the possible mecha... By Cassie Hopton, PhDJun 12, 2026
By Cassie Hopton, PhDJun 12, 2026Strut Health Review: 5 Things to Consider Before Purchasing
Is Strut Health right for your hair regrowth journey? We examine ingredient safety, dosing strategies, formulation methods, and customization options to help you make an informed decision. Before purchasing, understand the clinical evidence, potential risks, and limitations behind this popular teleh... By Catherine Kennedy, PhDJun 5, 2026
By Catherine Kennedy, PhDJun 5, 2026Does Tirzepatide Cause Hair Loss?
GLP-1 drugs like tirzepatide are taking over weight loss and diabetes care – but rising reports of hair loss are causing concern. Is this a real side effect or online hype? This article dives into the latest evidence, unpacking what science actually says and why the answer may be more complex than i...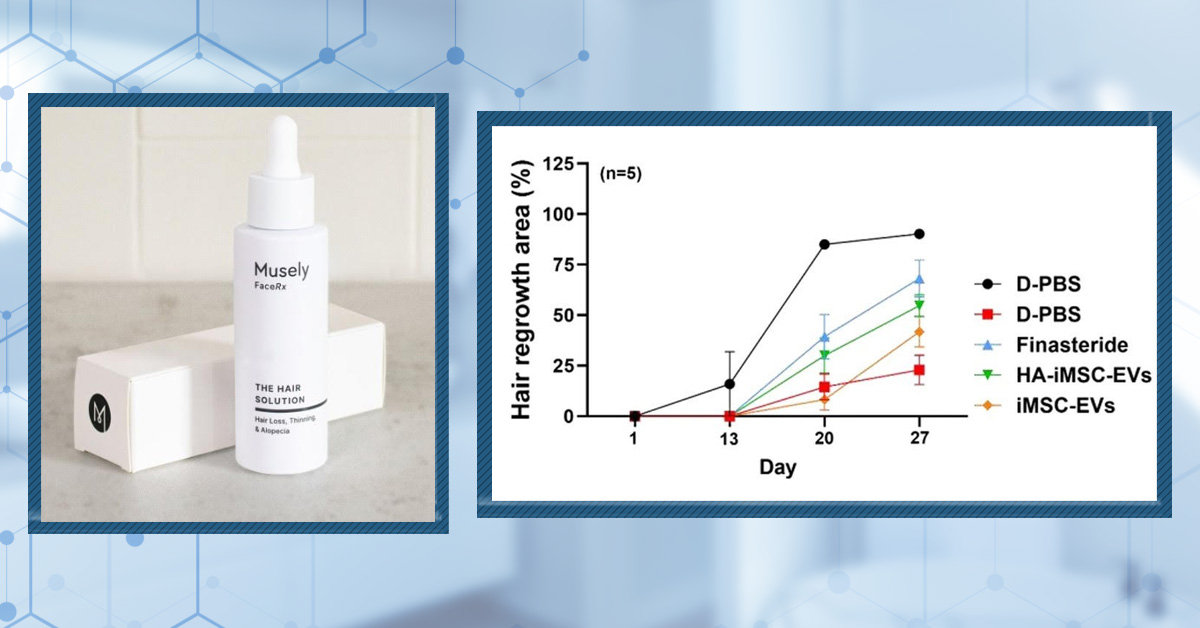 By Cassie Hopton, PhDMay 29, 2026
By Cassie Hopton, PhDMay 29, 2026Musely Reviews for Hair Loss: Are They Trustworthy?
Musely promises affordable, convenient prescription hair loss treatments, but how well do those claims hold up under scientific scrutiny? This in-depth review breaks down Musely’s topical and oral formulas, examines the evidence behind each ingredient. If you’re considering Musely for hair loss, thi... By Perfect Hair Health TeamMay 28, 2026
By Perfect Hair Health TeamMay 28, 2026Best Minoxidil for Women: Top 6 Brands of 2026
With so many hair-thinning treatments marketed to women, it can be difficult to separate what truly works from what’s just hype. This evidence-based guide ranks the best minoxidil options for women in 2026, including prescription and over-the-counter formulas, based on effectiveness, tolerability, c... By Perfect Hair Health TeamMay 28, 2026
By Perfect Hair Health TeamMay 28, 2026Best Topical Finasteride: 5 Top Products of 2026
Topical finasteride is exploding in popularity, but not all formulas are created equal. This guide breaks down the 5 best topical finasteride treatments on the market, comparing strength, safety, customization, and real-world value. From ultra-tailored prescriptions like Ulo to big telehealth brands... By Perfect Hair Health TeamMay 27, 2026
By Perfect Hair Health TeamMay 27, 2026Best Topical Dutasteride: 8 Choices for 2026
Topical dutasteride is emerging as a powerful next-generation option for treating hair loss. This expert-reviewed guide ranks the 8 best topical dutasteride treatments, comparing strength, safety, and customization, to help you find the most effective DHT-blocking solution for your needs. From Ulo’s... By Sophie Grice, PhDMay 23, 2026
By Sophie Grice, PhDMay 23, 202610 Best Shampoos for Thinning Hair Men
If you’re looking into products for thinning hair, shampoos are often one of the first options to consider. They’re quick, convenient, and easy to add into a routine. But a lot of these products rely on heavy marketing, and only a handful of ingredients actually have clinical evidence behind them in... - Mission Statement