- About
- Mission Statement
Education. Evidence. Regrowth.
- Education.
Prioritize knowledge. Make better choices.
- Evidence.
Sort good studies from the bad.
- Regrowth.
Get bigger hair gains.
Team MembersPhD's, resarchers, & consumer advocates.
- Rob English
Founder, researcher, & consumer advocate
- Research Team
Our team of PhD’s, researchers, & more
Editorial PolicyDiscover how we conduct our research.
ContactHave questions? Contact us.
Before-Afters- Transformation Photos
Our library of before-after photos.
- — Jenna, 31, U.S.A.
I have attached my before and afters of my progress since joining this group...
- — Tom, 30, U.K.
I’m convinced I’ve recovered to probably the hairline I had 3 years ago. Super stoked…
- — Rabih, 30’s, U.S.A.
My friends actually told me, “Your hairline improved. Your hair looks thicker...
- — RDB, 35, New York, U.S.A.
I also feel my hair has a different texture to it now…
- — Aayush, 20’s, Boston, MA
Firstly thank you for your work in this field. I am immensely grateful that...
- — Ben M., U.S.A
I just wanted to thank you for all your research, for introducing me to this method...
- — Raul, 50, Spain
To be honest I am having fun with all this and I still don’t know how much...
- — Lisa, 52, U.S.
I see a massive amount of regrowth that is all less than about 8 cm long...
Client Testimonials150+ member experiences.
 Scroll DownPopular Treatments
Scroll DownPopular Treatments- Treatments
Popular treatments. But do they work?
- Finasteride
- Oral
- Topical
- Dutasteride
- Oral
- Topical
- Mesotherapy
- Minoxidil
- Oral
- Topical
- Ketoconazole
- Shampoo
- Topical
- Low-Level Laser Therapy
- Therapy
- Microneedling
- Therapy
- Platelet-Rich Plasma Therapy (PRP)
- Therapy
- Scalp Massages
- Therapy
- More
IngredientsTop-selling ingredients, quantified.
- Saw Palmetto
- Redensyl
- Melatonin
- Caffeine
- Biotin
- Rosemary Oil
- Lilac Stem Cells
- Hydrolyzed Wheat Protein
- Sodium Lauryl Sulfate
- More
ProductsThe truth about hair loss "best sellers".
- Minoxidil Tablets
Xyon Health
- Finasteride
Strut Health
- Hair Growth Supplements
Happy Head
- REVITA Tablets for Hair Growth Support
DS Laboratories
- FoliGROWTH Ultimate Hair Neutraceutical
Advanced Trichology
- Enhance Hair Density Serum
Fully Vital
- Topical Finasteride and Minoxidil
Xyon Health
- HairOmega Foaming Hair Growth Serum
DrFormulas
- Bio-Cleansing Shampoo
Revivogen MD
- more
Key MetricsStandardized rubrics to evaluate all treatments.
- Evidence Quality
Is this treatment well studied?
- Regrowth Potential
How much regrowth can you expect?
- Long-Term Viability
Is this treatment safe & sustainable?
Free Research- Free Resources
Apps, tools, guides, freebies, & more.
- Free CalculatorTopical Finasteride Calculator
- Free Interactive GuideInteractive Guide: What Causes Hair Loss?
- Free ResourceFree Guide: Standardized Scalp Massages
- Free Course7-Day Hair Loss Email Course
- Free DatabaseIngredients Database
- Free Interactive GuideInteractive Guide: Hair Loss Disorders
- Free DatabaseTreatment Guides
- Free Lab TestsProduct Lab Tests: Purity & Potency
- Free Video & Write-upEvidence Quality Masterclass
- Free Interactive GuideDermatology Appointment Guide
- More
Articles100+ free articles.
-
10 Best Shampoos for Hair Loss in 2026
-
XYON Review: Do Their Products Actually Regrow Hair?
-
Minoxidil Before and After Photos [2026] | Does It Work?
-
How to Get Finasteride: Is It Over the Counter?
-
Keeps Review: The Truth About Their Hair Loss Treatments?
-
7 Best Oils for Hair Growth
-
Hims Hair Growth Reviews: The Pros, Cons, and Real Results
-
Topical Finasteride Before and After: Real Case Studies
PublicationsOur team’s peer-reviewed studies.
- Microneedling and Its Use in Hair Loss Disorders: A Systematic Review
- Use of Botulinum Toxin for Androgenic Alopecia: A Systematic Review
- Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia
- Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results
- A Hypothetical Pathogenesis Model For Androgenic Alopecia:Clarifying The Dihydrotestosterone Paradox And Rate-Limiting Recovery Factors
Menu- AboutAbout
- Mission Statement
Education. Evidence. Regrowth.
- Team Members
PhD's, resarchers, & consumer advocates.
- Editorial Policy
Discover how we conduct our research.
- Contact
Have questions? Contact us.
- Before-Afters
Before-Afters- Transformation Photos
Our library of before-after photos.
- Client Testimonials
Read the experiences of members
Before-Afters/ Client Testimonials- Popular Treatments
-
ArticlesSwitching From Topical Minoxidil To Oral Minoxidil
First Published Jan 12 2026Last Updated Jan 12 2026Pharmaceutical Researched & Written By:Michael Williams, PhD
Researched & Written By:Michael Williams, PhD Reviewed By:Rob English, Medical Editor
Reviewed By:Rob English, Medical Editor
Want help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Learn MoreArticle Summary
Thinking about switching from topical to oral minoxidil, or back again? Changing your approach to hair loss can significantly improve your results, but changing treatment can also be a gamble that sets back progress. We break down what the evidence actually shows, when you might want to consider switching, and highlight potential pitfalls.
Full Article
Minoxidil has been a cornerstone of hair-loss treatment for decades, and the options have expanded well beyond over-the-counter 2% and 5% topicals. Low-dose oral minoxidil has become increasingly common off-label, especially for people who struggle with topical routines or don’t respond well to them.
As a result, many people find themselves re-evaluating their approach and thinking about switching to oral minoxidil. We’ll break down how the oral and topical formulations compare and outline when a switch is likely to help.
Interested in Oral Minoxidil?
Low-dose oral minoxidil available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.

How Does Minoxidil Work?
Topical and oral minoxidil both work through the same basic mechanisms. At a biological level, minoxidil alters the hair cycle by shortening the resting (telogen) phase and promoting earlier entry into the growth (anagen) phase. This increases the proportion of follicles actively producing hair at any given time. Minoxidil also enlarges miniaturized hair follicles, resulting in thicker, longer hair shafts.[1]Messenger, A. G., & Rundegren, J. (2004). Minoxidil: mechanisms of action on hair growth. British Journal of Dermatology. 150(2). 186–194. Available at: … Continue reading
Beyond hair-cycle effects, minoxidil influences several signaling and support pathways within the follicle. It increases local blood flow, activates the Wnt/β-catenin signaling pathway involved in follicular cell proliferation and differentiation, and appears to have cytoprotective and anti-inflammatory effects, in part by increasing prostaglandin E2 production.
What is the Difference Between Topical and Oral Minoxidil?
Where topical and oral minoxidil meaningfully diverge is not in what the drug does once active, but in how it becomes active and reaches the follicle.
Topical minoxidil must first penetrate the scalp barrier and then be converted into its active form within the hair follicle itself. This conversion depends on local sulfotransferase enzyme activity, which varies between individuals and even between scalp regions. As a result, exposure to active minoxidil can be highly variable, even when application is consistent.
Oral minoxidil, by contrast, is absorbed through the gastrointestinal tract and converted to its active form primarily in the liver, where sulfotransferase activity is abundant and consistent. The active drug is then delivered to hair follicles via the bloodstream, largely bypassing both the scalp barrier and variability in local enzymatic activation.
These differences in activation and delivery are what make switching between topical and oral formulations clinically meaningful.
Why Do People Switch Between Minoxidil Forms?
Switching is rarely about chasing a small theoretical advantage. Most switches happen for one of three reasons:
1. Convenience and Adherence
Topical minoxidil can work well in trials, but adherence is hard in real life. Many people struggle with twice-daily application for months, and discontinuation rates in real-world settings are high, with the most commonly cited reason being a lack of compliance (i.e., people couldn’t maintain their treatment regimen).[2]Shadi, Z. (2023). Compliance to topical minoxidil and reasons for discontinuation among patients with androgenetic alopecia. Dermatology and Therapy. 13(5). 1157–1169. Available at: … Continue reading
Topical minoxidil can also present cosmetic challenges that influence long-term adherence. Liquid solutions may leave the hair feeling greasy or stiff, create visible residue or flaking that can resemble dandruff, and interfere with hairstyling, particularly in people with longer hair or finer textures.
Oral minoxidil is simpler, usually a once-daily pill, and for many people, that alone changes outcomes.
2. Inconsistent Response to Topical Therapy
Some people use topical minoxidil correctly for long enough and still see little benefit. This can happen even when everything “looks right” on paper. The second most cited reason for discontinuing topical minoxidil was unsatisfactory results, and clinical data have shown that response rates are high in the first 3-6 months, but drop after a year or longer of use.[3]Olsen, E. A., Weiner, M. S., Amara, I. A., & DeLong, E. R. (1990). Five-year follow-up of men with androgenetic alopecia treated with topical minoxidil. *Journal of the American Academy of … Continue reading
3. Side Effects
The side effects most commonly associated with topical minoxidil are local rather than systemic, reflecting the fact that only a small fraction of the applied drug enters the bloodstream. The most frequently reported issues include scalp irritation, dryness, flaking, itching, and contact dermatitis. In many cases, these reactions are driven less by minoxidil itself and more by the vehicle used to deliver it, particularly formulations containing propylene glycol.[4]Olsen, E. A., DeLong, E. R., & Weiner, M. S. (1987). Long-term follow-up of men with male pattern baldness treated with topical minoxidil. Journal of the American Academy of Dermatology. 16(3). … Continue reading
Minoxidil is also toxic to pets, and even small exposures to topical or oral products can cause severe, sometimes fatal cardiovascular events. Because topical formulations can be harder to control, and need to be handled with care, some users may switch to oral formulations to decrease the risk of accidental exposure.[5]Tater, K. C., Gwaltney-Brant, S., & Wismer, T. (2021). Topical minoxidil exposures and toxicoses in dogs and cats: 211 cases (2001–2019). *Journal of the American Animal Hospital Association.* … Continue reading
Propylene glycol is included in many liquid formulations to enhance solubility and penetration, but it is a well-known irritant and contact sensitizer. In susceptible individuals, this can lead to erythema, scaling, burning, or eczematous dermatitis, particularly with twice-daily use.
Oral minoxidil produces a different side-effect profile because it is systemically absorbed and pharmacologically active throughout the body. At the low doses used for hair loss, it is generally well tolerated, but adverse effects occur more frequently than with topical formulations and tend to be dose-dependent.
The most common side effect is hypertrichosis, or unwanted hair growth outside the scalp, including on the face. This was reported in 15% of 1404 users in a follow-up study.[6]Vañó-Galván, S., Pirmez, R., Hermosa-Gelbard, A., Moreno-Arrones, Ó. M., Saceda-Corralo, D., Rodrigues-Barata, R., Jimenez-Cauhe, J., et al. (2021). Safety of low-dose oral minoxidil for hair … Continue reading
Hypertrichosis is typically more of an issue for women taking minoxidil, for whom hair on the face and body may be off-putting.
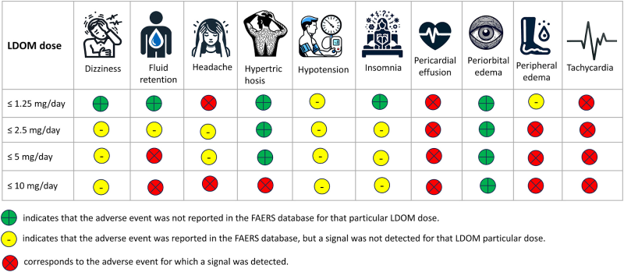
Other common side effects reported in the follow-up study included lightheadedness (1.7%), fluid retention (1.3%), tachycardia (elevated heart rate, 0.9%), and headache (0.4%). Serious cardiovascular complications are rare at the low doses used for hair loss and have been reported primarily in higher-dose antihypertensive use or in individuals with pre-existing cardiovascular disease.

Figure 1. Occurrence of adverse events in individuals taking low-dose oral minoxidil (LDOM), as reported in the FDA Adverse Event Reporting System. Adapted from Figure 1.[7]Gupta, A. K., Bamimore, M. A., Abdel-Qadir, H., Williams, G., Tosti, A., Piguet, V., & Talukder, M. (2025). Low-dose oral minoxidil and associated adverse events: analyses of the FDA Adverse … Continue reading Image used under Creative Commons License.
If you’re concerned about minoxidil side effects, check out our article on 10 ways to reduce them.
Why Oral Minoxidil Might Work Better for Some
Topical minoxidil relies heavily on follicular sulfotransferase activity (notably SULT1A1). Lower activity is associated with weaker response.[8]Pietrauszka, K., & Bergler-Czop, B. (2022). Sulfotransferase SULT1A1 activity in hair follicle, a prognostic marker of response to the minoxidil treatment in patients with androgenetic alopecia: … Continue reading
As such, minoxidil’s “ceiling” isn’t the same for everyone: people with lower SULT1A1 activity will generally not respond as well.
Similarly, the penetration of topical minoxidil through the scalp is essential for it to function. This can depend on a range of factors, including the type of formulation, scalp health, contact time, and application technique.
Oral minoxidil bypasses these barriers to absorption. It is absorbed through the gastrointestinal tract and converted into its active form primarily in the liver, where sulfotransferase activity is abundant. Systemic activation makes exposure more uniform across the scalp and less dependent on follicular enzyme variability.
Oral Minoxidil vs Topical Minoxidil
So what does the clinical evidence tell us about the efficacy of the two approaches?
Both topical and oral minoxidil are supported by robust clinical evidence demonstrating their effectiveness in treating hair loss, including androgenic alopecia (AGA).[9]Jaén, P., & Arias-Santiago, S. (n.d.). Efficacy and safety of oral minoxidil 5 mg daily during 24-week treatment in male androgenetic alopecia. Available at: … Continue reading,[10]Panchaprateep, R., & Lueangarun, S. (2020). Efficacy and safety of oral minoxidil 5 mg once daily in the treatment of male patients with androgenetic alopecia: an open-label and global … Continue reading,[11]Silva, M. N. E., Ramos, P. M., Silva, M. R., Silva, R. N. E., & Raposo, N. R. B. (2022). Randomized clinical trial of low-dose oral minoxidil for the treatment of female pattern hair loss: 0.25 … Continue reading,[12]Sinclair, R. D. (2018). Female pattern hair loss: a pilot study investigating combination therapy with low-dose oral minoxidil and spironolactone. *International Journal of Dermatology.* 57(1). … Continue reading,[13]Olsen, E. A., Dunlap, F. E., Funicella, T., Koperski, J. A., Swinehart, J. M., Tschen, E. H., & Trancik, R. J. (2002). A randomized clinical trial of 5% topical minoxidil versus 2% topical … Continue reading,[14]Adil, A., & Godwin, M. (2017). The effectiveness of treatments for androgenetic alopecia: a systematic review and meta-analysis. *Journal of the American Academy of Dermatology.* 77(1). … Continue reading
Direct head-to-head comparisons, however, are less common.
Direct Comparisons in Men
A 2024 randomized clinical trial compared 5 mg oral minoxidil once daily vs 5% topical minoxidil twice daily for 24 weeks in men with AGA. They found no significant difference in hair outcomes overall, but oral trended higher for density and showed significantly greater improvement in photographic assessment at the crown.[15]Penha, M. A., Miot, H. A., Kasprzak, M., & Ramos, P. M. (2024). Oral minoxidil vs topical minoxidil for male androgenetic alopecia: a randomized clinical trial. JAMA Dermatology. 160(6). … Continue reading
This matches the broader trend seen across male oral minoxidil studies at 2.5-5 mg daily: more consistent, dose-dependent results with cosmetic relevance.[16]Panchaprateep, R., & Lueangarun, S. (2020). Efficacy and safety of oral minoxidil 5 mg once daily in the treatment of male patients with androgenetic alopecia: an open-label and global … Continue reading
Direct Comparisons in Women
As we’ve already noted, doses for women tend to be lower than for men, typically 1 mg daily versus 5 mg daily, so as to avoid hypertrichosis.
The first direct comparison in women comes from a 24-week randomized, open comparative study conducted in Brazil, which evaluated oral minoxidil 1 mg once daily versus topical minoxidil 5% solution applied once daily in women aged 18–65 with pattern hair loss.[17]Ramos, P. M., Melo, D. F., Radwanski, H., Cortez de Almeida, R. F., & Miot, H. A. (2023). Female-pattern hair loss: therapeutic update. Anais Brasileiros de Dermatologia. 98. 506–519. Available … Continue reading
After 24 weeks, terminal hair density increased by 12% in the oral minoxidil group and 7.2% in the topical group. While this improvement favored oral therapy, the difference was not statistically significant.
Side-effect patterns differed in expected ways. Hypertrichosis was reported in 27% of women taking oral minoxidil, compared with 4% in the topical group.
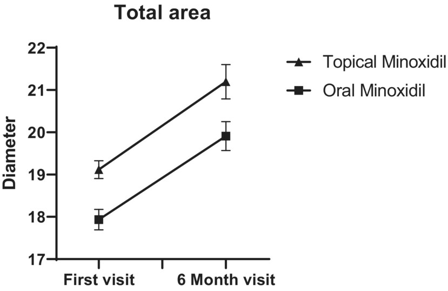
A similar trial comparing 1mg oral minoxidil to 5% topical minoxidil also found no statistically significant differences between the two groups in hair diameter. They did, however, report improvement in photographic assessment in the topical group.[18]Asilian, A., Farmani, A., & Saber, M. (2024). Clinical efficacy and safety of low-dose oral minoxidil versus topical solution in the improvement of androgenetic alopecia: a randomized controlled … Continue reading
Lower doses of oral minoxidil for women may reduce its efficacy compared to topical treatments, which are typically applied at similar concentrations to men (5%).

Figure 2. Improvements in average hair diameter were comparable between 5% topical solution or 1 mg/day oral minoxidil over a six-month study period. Adapted from Figure 2.[19]Asilian, A., Farmani, A., & Saber, M. (2024). Clinical efficacy and safety of low-dose oral minoxidil versus topical solution in the improvement of androgenetic alopecia: a randomized controlled … Continue reading Image used under Creative Commons License.
What About Higher Concentrations of Topical Minoxidil?
As we’ve seen, most clinical research focuses on 5% topical minoxidil. However, in practice, many people use higher concentrations of minoxidil, with 7-8% being common, and sometimes concentrations as high as 10-15% are employed as a more aggressive treatment.
What’s more, minoxidil is often paired with tretinoin/retinoic acid, which enhances activation and penetration of the drug. While there is limited clinical data on such pairings, anecdotal evidence from our members suggests that this combination could help to optimize topical minoxidil’s efficacy.
We see that 7-8% minoxidil paired with 0.005-0.02% retinoic acid appears to outperform 5 mg oral minoxidil, even in cases of diffuse thinning.
For comprehensive information about using retinoic acid for hair loss, check out our ultimate guide.
Anecdotal evidence from our members also suggests that higher concentrations of topical minoxidil (10-15%) can generate similar results to 5 mg oral minoxidil.
Is there a clear winner?
In short, no. A 2025 meta-analysis comparing topical and oral minoxidil found no significant difference between approaches overall, which reflects how much outcomes depend on dose, population, and study design.[20]Fazal, F., Malik, B. H., Malik, H. M., Sabir, B., Mustafa, H., Ahmed, M., Abid, A., Adil, M. L., Shafi, U., & Saad, M. (2025). Can oral minoxidil be the game changer in androgenetic alopecia? A … Continue reading
It is important to note that adherence to a strict routine in trials is typically well enforced, and topical treatments are applied with consistent volumes at consistent times. This doesn’t necessarily reflect how people use topical minoxidil in the real world.
On the other hand, many users find that they can optimize a topical approach by increasing the strength or frequency of application, or by adding enhancer ingredients like tretinoin/retinoic acid. If you’re using such a combination therapy, you might, in fact, see worse results when switching to oral.
When Switching From Topical to Oral Makes the Most Sense
Switching to oral minoxidil is most rational when the limiting factor is activation or adherence, or when topical treatment isn’t delivering the results you expect.
Good Candidates for Switching to Oral Minoxidil
If systemic exposure is acceptable from a safety and tolerability standpoint, there are circumstances in which switching from an oral to a topical formulation makes sense.
Poor topical responders – If you’ve used topical minoxidil consistently for 6-12 months and can reasonably say adherence wasn’t the problem, oral is a logical next step because it bypasses follicular enzyme variability.[21]Pietrauszka, K., & Bergler-Czop, B. (2022). Sulfotransferase SULT1A1 activity in hair follicle, a prognostic marker of response to the minoxidil treatment in patients with androgenetic alopecia: … Continue reading
Diffuse or Advanced Thinning – As larger areas of the scalp are affected, ensuring even coverage requires more time, higher product volumes, and careful technique, which many people struggle to sustain long term. Missed areas and uneven delivery are common and can limit results even when follicles remain responsive.
Oral minoxidil avoids these practical constraints by delivering the drug systemically, allowing uniform exposure across the entire scalp and making treatment easier to scale as hair loss progresses.
Convenience-driven adherence problems – When adherence is the primary issue, oral minoxidil often has a practical advantage. Topical therapy requires regular scalp application, drying time, and styling time, all of which can erode consistency over months or years of use. Missed applications are common and can reduce effectiveness. Oral minoxidil makes consistent long-term use more achievable for many people.
Scalp Inflammation – Inflammation of the scalp occurs in a high proportion of individuals with AGA, with seborrheic dermatitis being common. If you’re pairing minoxidil with inflammatory treatments like retinoic acid, this can exacerbate underlying chronic inflammation and prevent regrowth.
Scalp inflammation decreases the efficacy of topical minoxidil.[22]Whiting, D. A. (1993). Diagnostic and predictive value of horizontal sections of scalp biopsy specimens in male pattern androgenetic alopecia. *Journal of the American Academy of Dermatology.* 28(5). … Continue reading Switching to oral minoxidil, or even removing the inflammatory component from your treatment, can help improve underlying inflammation.
People Who Should Be Cautious Switching
Anyone with cardiovascular disease, kidney issues, fluid retention tendencies, low blood pressure, or unexplained palpitations should be conservative and involve a clinician before starting or escalating oral minoxidil.[23]Gupta, A. K., Bamimore, M. A., Abdel-Qadir, H., Williams, G., Tosti, A., Piguet, V., & Talukder, M. (2025). Low-dose oral minoxidil and associated adverse events: analyses of the FDA Adverse … Continue reading
When Switching From Oral to Topical Makes the Most Sense
There are also times when switching from topical oral minoxidil might be a sensible decision. These will most commonly occur when side effects have made use difficult or intolerable.
You might also consider an optimized topical approach, incorporating enhancers such as tretinoin/retinoic acid or increasing topical dosage. Anecdotal experiences of our members suggest these topical combinations can outperform low-dose oral minoxidil.
If you’’re interested in topical minoxidil for, check out our articles for men and women on the best products currently available.
Hair Shedding: Should You Be Concerned?
When people start a new hair loss treatment, shedding events are common. This includes treatments that are working! ‘Treatment-induced telogen effluvium shedding’ is the term used to describe this phenomenon, and can actually be a good predictor of whether minoxidil treatment will work down the line.[24]Bi, L., Kan, H., Wang, J., Ding, Y., Huang, Y., Wang, C., & Fan, W. (2025). Whether the transient hair shedding phase exist after minoxidil treatment and does it predict treatment efficacy? A … Continue reading
However, it’s hard to tell if shedding when you switch treatments is a positive sign, or if it’s a indicator of decreased efficacy. These cases are referred to as a ‘treatment withdrawal telogen effluvium shed’, and won’t lead to improvement in the future.
Information from our members indicates that shedding after switching from topical to oral minoxodil tends to fall into the latter camp: shedding is a result of the treatment working less well.
Be aware of shedding after switching treatments, as it could be an indicator that your new treatment isn’t working as well.
You can read more about minoxidil shedding in our comprehensive article.
How to Switch
There’s no universally validated switching protocol supported by large controlled trials. But there are sensible principles that reduce avoidable problems.
-
Avoid Abrupt Stop and Start Changes
Minoxidil works by keeping follicles in a growth-supportive environment. Abrupt discontinuation can allow hairs that were being prolonged in anagen to shed as cycles normalize.
-
Expect a Transition Period
Whether switching to oral or topical, you’re changing local concentrations and the consistency of follicular exposure. That can mean a temporary shed or plateau before stabilization, so don’t judge too early.
-
Be Patient and Track Longterm Changes
As with all hair loss treatments, consistency is key. Because minoxidil primarily influences hair-cycle timing rather than creating new follicles, benefits accrue gradually and are best assessed over 6–12 months of consistent use. Tracking progress with standardized photographs, consistent lighting, and fixed time intervals can help distinguish true treatment effects from normal cycle-related variation.
If you experience severe adverse effects, you should discontinue treatment and speak to a clinician.
Final Thoughts
Switching between topical and oral minoxidil should be a deliberate and strategic decision guided by potential reasons your current approach isn’t working. The evidence consistently shows that both topical and oral minoxidil can be effective, but their real-world performance is shaped by adherence, activation, dose, side effects, and how well the treatment fits into your life.
For people with limited topical response, inconsistent application, or large areas of thinning, oral minoxidil can provide more uniform exposure and better long-term consistency. However, real-world experience and member data suggest that higher-strength topical formulations (7–8%), especially when paired with penetration or activation enhancers like retinoic acid, often produce stronger results.
In some cases, these optimized topical approaches appear to match or even outperform low-dose oral minoxidil. For people who tolerate topical therapy well and can maintain consistency, increasing topical strength may be a more effective next step than switching to oral treatment.
Ultimately, switching treatments always carries trade-offs and some risk. The safest path forward is deliberate, not reactive: avoid abrupt changes, allow sufficient time to assess outcomes, and monitor both hair and systemic responses carefully.
References[+]
References ↑1 Messenger, A. G., & Rundegren, J. (2004). Minoxidil: mechanisms of action on hair growth. British Journal of Dermatology. 150(2). 186–194. Available at: https://doi.org/10.1111/j.1365-2133.2004.05785.x ↑2 Shadi, Z. (2023). Compliance to topical minoxidil and reasons for discontinuation among patients with androgenetic alopecia. Dermatology and Therapy. 13(5). 1157–1169. Available at: https://doi.org/10.1007/s13555-023-00919-x ↑3 Olsen, E. A., Weiner, M. S., Amara, I. A., & DeLong, E. R. (1990). Five-year follow-up of men with androgenetic alopecia treated with topical minoxidil. *Journal of the American Academy of Dermatology.* 22(4). 643–646. Available at: https://doi.org/10.1016/0190-9622(90)70089-Z ↑4 Olsen, E. A., DeLong, E. R., & Weiner, M. S. (1987). Long-term follow-up of men with male pattern baldness treated with topical minoxidil. Journal of the American Academy of Dermatology. 16(3). 688–695. Available at: https://doi.org/10.1016/S0190-9622(87)70089-9 ↑5 Tater, K. C., Gwaltney-Brant, S., & Wismer, T. (2021). Topical minoxidil exposures and toxicoses in dogs and cats: 211 cases (2001–2019). *Journal of the American Animal Hospital Association.* 57(5). 225–231. Available at: https://doi.org/10.5326/jaaha-ms-7154 ↑6 Vañó-Galván, S., Pirmez, R., Hermosa-Gelbard, A., Moreno-Arrones, Ó. M., Saceda-Corralo, D., Rodrigues-Barata, R., Jimenez-Cauhe, J., et al. (2021). Safety of low-dose oral minoxidil for hair loss: a multicenter study of 1404 patients. Journal of the American Academy of Dermatology. 84(6). 1644–1651. Available at: https://doi.org/10.1016/j.jaad.2021.02.054 ↑7 Gupta, A. K., Bamimore, M. A., Abdel-Qadir, H., Williams, G., Tosti, A., Piguet, V., & Talukder, M. (2025). Low-dose oral minoxidil and associated adverse events: analyses of the FDA Adverse Event Reporting System (FAERS) with a focus on pericardial effusions. *Journal of Cosmetic Dermatology.* 24(1). e16574. Available at: https://doi.org/10.1111/jocd.16574 ↑8, ↑21 Pietrauszka, K., & Bergler-Czop, B. (2022). Sulfotransferase SULT1A1 activity in hair follicle, a prognostic marker of response to the minoxidil treatment in patients with androgenetic alopecia: a review. Advances in Dermatology and Allergology / Postępy Dermatologii i Alergologii. 39(3). 472–478. Available at: https://doi.org/10.5114/ada.2020.99947 ↑9 Jaén, P., & Arias-Santiago, S. (n.d.). Efficacy and safety of oral minoxidil 5 mg daily during 24-week treatment in male androgenetic alopecia. Available at: https://www.researchgate.net/profile/Suparuj-Lueangarun/publication/319006716_Efficacy_and_safety_of_oral_minoxidil_5_mg_daily_during_24-week_treatment_in_male_androgenetic_alopecia/links/5b46f1690f7e9b4637cde38b/Efficacy-and-safety-of-oral-minoxidil-5-mg-daily-during-24-week-treatment-in-male-androgenetic-alopecia.pdf ↑10 Panchaprateep, R., & Lueangarun, S. (2020). Efficacy and safety of oral minoxidil 5 mg once daily in the treatment of male patients with androgenetic alopecia: an open-label and global photographic assessment. *Dermatology and Therapy.* 10(6). 1345–1357. Available at: https://doi.org/10.1007/s13555-020-00448-x ↑11 Silva, M. N. E., Ramos, P. M., Silva, M. R., Silva, R. N. E., & Raposo, N. R. B. (2022). Randomized clinical trial of low-dose oral minoxidil for the treatment of female pattern hair loss: 0.25 mg versus 1 mg. 396–399. Available at: https://doi.org/10.1016/j.jaad.2022.01.017 ↑12 Sinclair, R. D. (2018). Female pattern hair loss: a pilot study investigating combination therapy with low-dose oral minoxidil and spironolactone. *International Journal of Dermatology.* 57(1). 104–109. Available at: https://doi.org/10.1111/ijd.13838 ↑13 Olsen, E. A., Dunlap, F. E., Funicella, T., Koperski, J. A., Swinehart, J. M., Tschen, E. H., & Trancik, R. J. (2002). A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men. *Journal of the American Academy of Dermatology.* 47(3). 377–385. Available at: https://doi.org/10.1067/mjd.2002.124088 ↑14 Adil, A., & Godwin, M. (2017). The effectiveness of treatments for androgenetic alopecia: a systematic review and meta-analysis. *Journal of the American Academy of Dermatology.* 77(1). 136–141. Available at: https://doi.org/10.1016/j.jaad.2017.02.054 ↑15 Penha, M. A., Miot, H. A., Kasprzak, M., & Ramos, P. M. (2024). Oral minoxidil vs topical minoxidil for male androgenetic alopecia: a randomized clinical trial. JAMA Dermatology. 160(6). 600–605. Available at: https://doi:10.1001/jamadermatol.2024.0284 ↑16 Panchaprateep, R., & Lueangarun, S. (2020). Efficacy and safety of oral minoxidil 5 mg once daily in the treatment of male patients with androgenetic alopecia: an open-label and global photographic assessment. Dermatology and Therapy. 10(6). 1345–1357. Available at: https://doi.org/10.1007/s13555-020-00448-x ↑17 Ramos, P. M., Melo, D. F., Radwanski, H., Cortez de Almeida, R. F., & Miot, H. A. (2023). Female-pattern hair loss: therapeutic update. Anais Brasileiros de Dermatologia. 98. 506–519. Available at: https://doi.org/10.1016/j.abd.2022.09.006 ↑18 Asilian, A., Farmani, A., & Saber, M. (2024). Clinical efficacy and safety of low-dose oral minoxidil versus topical solution in the improvement of androgenetic alopecia: a randomized controlled trial. Journal of Cosmetic Dermatology. 23(3). 949–957. Available at: https://doi.org/10.1111/jocd.16086 ↑19 Asilian, A., Farmani, A., & Saber, M. (2024). Clinical efficacy and safety of low-dose oral minoxidil versus topical solution in the improvement of androgenetic alopecia: a randomized controlled trial. *Journal of Cosmetic Dermatology.* 23(3). 949–957. Available at: https://doi.org/10.1111/jocd.16086 ↑20 Fazal, F., Malik, B. H., Malik, H. M., Sabir, B., Mustafa, H., Ahmed, M., Abid, A., Adil, M. L., Shafi, U., & Saad, M. (2025). Can oral minoxidil be the game changer in androgenetic alopecia? A comprehensive review and meta-analysis comparing topical and oral minoxidil for treating androgenetic alopecia. Skin Health and Disease. vzaf009. Available at: https://doi.org/10.1093/skinhd/vzaf009 ↑22 Whiting, D. A. (1993). Diagnostic and predictive value of horizontal sections of scalp biopsy specimens in male pattern androgenetic alopecia. *Journal of the American Academy of Dermatology.* 28(5). 755–763. Available at: https://doi.org/10.1016/0190-9622(93)70106-4 ↑23 Gupta, A. K., Bamimore, M. A., Abdel-Qadir, H., Williams, G., Tosti, A., Piguet, V., & Talukder, M. (2025). Low-dose oral minoxidil and associated adverse events: analyses of the FDA Adverse Event Reporting System (FAERS) with a focus on pericardial effusions. Journal of Cosmetic Dermatology. 24(1). e16574. Available at: https://doi.org/10.1111/jocd.16574 ↑24 Bi, L., Kan, H., Wang, J., Ding, Y., Huang, Y., Wang, C., & Fan, W. (2025). Whether the transient hair shedding phase exist after minoxidil treatment and does it predict treatment efficacy? A retrospective study in androgenetic alopecia patients. *Journal of Dermatological Treatment.* 36(1). 2480739. Available at: https://doi.org/10.1080/09546634.2025.2480739 Want help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Learn More
Michael Williams, PhD
Michael is a researcher and writer who holds a BSc in Bioscience, an MSc in Regenerative Medicine, and a PhD in Translational Biomedicine. He undertook his PhD research at Houston Methodist Research Institute, Texas, focusing on cell signaling in the ovarian cancer tumor microenvironment. He conducted postdoctoral research at Barts Cancer Institute in London, exploring cellular metabolism in acute myeloid leukemia. He has published work in a range of fields, including oncology, nanomedicine, and cell-based therapeutics.
"... Can’t thank @Rob (PHH) and @sanderson17 enough for allowing me to understand a bit what was going on with me and why all these [things were] happening ... "
— RDB, 35, New York, U.S.A."... There is a lot improvement that I am seeing and my scalp feel alive nowadays... Thanks everyone. "
— Aayush, 20’s, Boston, MA"... I can say that my hair volume/thickness is about 30% more than it was when I first started."
— Douglas, 50’s, Montréal, CanadaWant help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Join Now - Mission Statement
 Scroll Down
Scroll Down More
More More
More