- About
- Mission Statement
Education. Evidence. Regrowth.
- Education.
Prioritize knowledge. Make better choices.
- Evidence.
Sort good studies from the bad.
- Regrowth.
Get bigger hair gains.
Team MembersPhD's, resarchers, & consumer advocates.
- Rob English
Founder, researcher, & consumer advocate
- Research Team
Our team of PhD’s, researchers, & more
Editorial PolicyDiscover how we conduct our research.
ContactHave questions? Contact us.
Before-Afters- Transformation Photos
Our library of before-after photos.
- — Jenna, 31, U.S.A.
I have attached my before and afters of my progress since joining this group...
- — Tom, 30, U.K.
I’m convinced I’ve recovered to probably the hairline I had 3 years ago. Super stoked…
- — Rabih, 30’s, U.S.A.
My friends actually told me, “Your hairline improved. Your hair looks thicker...
- — RDB, 35, New York, U.S.A.
I also feel my hair has a different texture to it now…
- — Aayush, 20’s, Boston, MA
Firstly thank you for your work in this field. I am immensely grateful that...
- — Ben M., U.S.A
I just wanted to thank you for all your research, for introducing me to this method...
- — Raul, 50, Spain
To be honest I am having fun with all this and I still don’t know how much...
- — Lisa, 52, U.S.
I see a massive amount of regrowth that is all less than about 8 cm long...
Client Testimonials150+ member experiences.
 Scroll DownPopular Treatments
Scroll DownPopular Treatments- Treatments
Popular treatments. But do they work?
- Finasteride
- Oral
- Topical
- Dutasteride
- Oral
- Topical
- Mesotherapy
- Minoxidil
- Oral
- Topical
- Ketoconazole
- Shampoo
- Topical
- Low-Level Laser Therapy
- Therapy
- Microneedling
- Therapy
- Platelet-Rich Plasma Therapy (PRP)
- Therapy
- Scalp Massages
- Therapy
 More
More
IngredientsTop-selling ingredients, quantified.
- Saw Palmetto
- Redensyl
- Melatonin
- Caffeine
- Biotin
- Rosemary Oil
- Lilac Stem Cells
- Hydrolyzed Wheat Protein
- Sodium Lauryl Sulfate
 More
More
ProductsThe truth about hair loss "best sellers".
- Minoxidil Tablets
Xyon Health
- Finasteride
Strut Health
- Hair Growth Supplements
Happy Head
- REVITA Tablets for Hair Growth Support
DS Laboratories
- FoliGROWTH Ultimate Hair Neutraceutical
Advanced Trichology
- Enhance Hair Density Serum
Fully Vital
- Topical Finasteride and Minoxidil
Xyon Health
- HairOmega Foaming Hair Growth Serum
DrFormulas
- Bio-Cleansing Shampoo
Revivogen MD
- more
Key MetricsStandardized rubrics to evaluate all treatments.
- Evidence Quality
Is this treatment well studied?
- Regrowth Potential
How much regrowth can you expect?
- Long-Term Viability
Is this treatment safe & sustainable?
Free Research- Free Resources
Apps, tools, guides, freebies, & more.
- Free CalculatorTopical Finasteride Calculator
- Free Interactive GuideInteractive Guide: What Causes Hair Loss?
- Free ResourceFree Guide: Standardized Scalp Massages
- Free Course7-Day Hair Loss Email Course
- Free DatabaseIngredients Database
- Free Interactive GuideInteractive Guide: Hair Loss Disorders
- Free DatabaseTreatment Guides
- Free Lab TestsProduct Lab Tests: Purity & Potency
- Free Video & Write-upEvidence Quality Masterclass
- Free Interactive GuideDermatology Appointment Guide
- More
Articles100+ free articles.
-
Which Hormones Cause Hair Loss in Females?
-
Does Zepbound Cause Hair Loss?
-
Does Wegovy Cause Hair Loss?
-
Strut Health Review: 5 Things to Consider Before Purchasing
-
Does Tirzepatide Cause Hair Loss?
-
Musely Reviews for Hair Loss: Are They Trustworthy?
-
Best Minoxidil for Women: Top 6 Brands of 2026
-
Best Topical Finasteride: 5 Top Products of 2026
PublicationsOur team’s peer-reviewed studies.
- Microneedling and Its Use in Hair Loss Disorders: A Systematic Review
- Use of Botulinum Toxin for Androgenic Alopecia: A Systematic Review
- Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia
- Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results
- A Hypothetical Pathogenesis Model For Androgenic Alopecia:Clarifying The Dihydrotestosterone Paradox And Rate-Limiting Recovery Factors
Menu- AboutAbout
- Mission Statement
Education. Evidence. Regrowth.
- Team Members
PhD's, resarchers, & consumer advocates.
- Editorial Policy
Discover how we conduct our research.
- Contact
Have questions? Contact us.
- Before-Afters
Before-Afters- Transformation Photos
Our library of before-after photos.
- Client Testimonials
Read the experiences of members
Before-Afters/ Client Testimonials- Popular Treatments
-
ArticlesThe Scalp Tension Theory Of Hair Loss: A Scientific Breakdown
First Published Jan 9 2019Last Updated Sep 19 2025MiscellaneousNatural RemediesPharmaceutical Researched & Written By:Perfect Hair Health Team
Researched & Written By:Perfect Hair Health Team Reviewed By:Rob English, Medical Editor
Reviewed By:Rob English, Medical Editor
Want help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Learn MoreArticle Summary
Does a tight scalp cause hair loss? Sixty years ago, researchers abandoned this theory. Now, studies on Botox and hair regrowth are making scientists revisit the scalp tension theory of hair loss. Here’s everything you need to know.
Full Article
Can Scalp Tension Cause Hair Loss? It’s Possible.
Is there a connection between scalp tension and pattern hair loss (androgenic alopecia)? Sixty years ago, researchers thought no. Today, many are changing their tune.
The scalp tightness theory recently regained popularity in hair loss forums, but it isn’t new. Over 100 years ago, Bernarr Macfadden noted an association between scalp tightness and androgenic alopecia (AGA) in his book Hair Culture. And in 1950, the scalp tension theory of hair loss even advanced into the academia. For the next decade, androgenic alopecia researchers supported its plausibility.
Then in 1959, everything changed. Most of the scalp tightness theory’s advocates turned from supportive to dismissive… and almost overnight.
What happened? Why did researchers change their minds?
Well, a series of hair transplantation studies were published that contradicted the scalp tightness theory of androgenic alopecia. This led researchers to assess the evidence, reevaluate their opinions, and abandon the scalp tightness theory altogether. For the next forty years, the idea that scalp tension could cause hair loss remained “unrealistic.”
That is, until recently.
In the last five years, new studies have emerged that are forcing researchers to reevaluate the scalp tension-androgenic alopecia hypothesis yet again. These studies not only help build a biological rationale for the scalp tightness hypothesis, but they also present evidence opposing the counterarguments of theory.
So what are these studies? And what’s making researchers waver yet again? This article series explains it all.
This is a three-part series on the scalp tightness theory of hair loss. In this article, we’ll uncover the science behind scalp tension and its potential relationship to pattern hair loss.
In the next article, we’ll dive into the debate over this theory. After all, a few studies from the 50’s and 70’s seemingly contradicted the theory entirely. But now – over forty years later, new evidence is challenging these counterarguments… and bringing the debate back to life again.
In the last article, we’ll try to settle this debate and uncover where scalp tension might come from. Does scalp tightness cause androgenic alopecia? Is scalp tension merely associative with hair loss? And if does cause pattern hair loss… what can we do about it? As always, when it comes to hair loss research, the answers aren’t so cut-and-dry.
Interested in Topical Finasteride?
Low-dose & full-strength finasteride available, if prescribed*
Take the next step in your hair regrowth journey. Get started today with a provider who can prescribe a topical solution tailored for you.
*Only available in the U.S. Prescriptions not guaranteed. Restrictions apply. Off-label products are not endorsed by the FDA.

Scalp Tension Theory: The Basics
We’ll soon get into the details of the scalp tension-androgenic alopecia hypothesis. For now, here are the basic principles.
Skin tension tends to restrict blood flow to tissues – much like a bent finger tightens our knuckle and turns it white. Interestingly, research suggests that balding men and women tend to have chronically tighter scalps than those without hair loss.
Across the body, excessive tissue tension can evoke an inflammatory response which, if left unresolved, leads to scar tissue formation. We’ve seen this in stressed periodontal ligaments, the eyelids of patients with Graves’ disease, enlarged prostates, and in the hand tissues of people with Dupuytren’s contracture. The bottom line: more tissue tension, more inflammation, more scar tissue.
As scar tissue settles in, it simultaneously restricts blood, oxygen, and nutrients to tissues. Fascinatingly, the same phenomena and observations – tissue tension, inflammation, reduced blood flow, lower oxygen, and increased scar tissue – are also seen in balding scalps. In fact, we see the onset of these observations in the same pattern and progression as hair loss.
Interestingly, studies on scarring-related diseases – like scleroderma – reveal that once enough scarring settles, hair cannot grow. Putting it all together, this suggests that scalp tension might be involved in the inflammatory cascade which leads to pattern hair loss.
Tension evokes inflammation, inflammation evokes scar tissue, scar tissue restricts oxygen and nutrients to the hair follicles, and this slowly miniaturizes the hair follicles until eventually… we’re left with pattern baldness. Thus, in its most basic form, the scalp tightness-androgenic alopecia theory looks something like this:
Scalp tissue tension >> inflammation >> scar tissue >> pattern hair loss
Does the scalp tension theory differ from our current understanding of androgenic alopecia?
Yes and no. The scalp tightness-hair loss theory fits well in the literature, and of what we already know about androgenic alopecia (or AGA). In fact, it might even enhance our understanding of AGA.
To get a full picture of why, we need to understand…
- The current model of AGA pathology (what researchers currently believe is the cause of AGA).
- Questions this AGA model cannot answer
- How the scalp tension theory answers these questions while still making sense of previous findings in AGA research.
Let’s take these one-by-one.
What Causes AGA? Our Current Understandings
AGA is the world’s most common hair loss disorder – affecting 50% of women and 80% of men throughout a lifetime. And it’s unique because it only affects a certain region: the top part of our scalps.
In men, the hair loss often begins at the temples and vertex. In women, it begins as more globalized (diffuse) thinning. In both genders, the condition is chronic and progressive – meaning that with time and without treatment, it will continue to worsen.
If you’ve ever looked into the causes of AGA, you’ve probably come across the term dihydrotestosterone, or DHT. DHT is a hormone that’s made from testosterone. In fact, most dermatologists will tell you that an interaction of our genetics and DHT is what causes pattern hair loss. Hence the medical name, androgenic alopecia. Andro = androgens; genic = genes; alopecia = hair loss.
So is there any truth to this claim? Yes. There’s an overwhelming amount of evidence that DHT is causally linked to pattern hair loss.
Firstly, studies show that DHT is higher in the scalps of men with thinning hair. Secondly, if a man is castrated, his testosterone (and DHT) levels plummet permanently. Men castrated before puberty (i.e., before their DHT levels spike) don’t go bald later in life. And thirdly, men with a genetic deficiency in an enzyme that converts testosterone into DHT in scalp tissues never develop pattern hair loss.

These are pretty indicting findings. Just look at the endpoints: men who never produce DHT never develop pattern hair loss. Men with higher amounts of DHT in their scalps have AGA. Based on these findings, DHT must play some causal role in AGA.
But beyond that, things start to get complicated…
DHT is causally linked to AGA. But eliminating DHT doesn’t lead to a complete hair recovery
Finasteride is an FDA-approved drug that men use to help fight AGA. It works by reducing DHT levels. In fact, when taken as prescribed, finasteride can reduce scalp DHT levels by over 60%.
But just how effective is it at treating AGA?
Well, clinical studies suggest finasteride improves hair loss outcomes for 80-90% of users. That means it helps slow, stop, or partially reverse hair loss for 80-90% of the people taking it. But just how much hair can we expect to recover?
Over a two-year period, those same studies suggest that finasteride, on average, leads to just a 10% increase in hair count – with hair count plateauing thereafter.
This suggests that finasteride is mostly limited to stopping hair loss progression, rather than reversing the condition entirely. Similar observations were made in castrates. Castration (and thereby near-full DHT reduction) only seems to stop pattern baldness. It doesn’t fully reverse it.
And therein lies the first big “question” of the DHT-hair loss hypothesis.
Question: If DHT causes pattern hair loss, how come eliminating DHT only stops AGA? How come it doesn’t lead to a full hair recovery?
This actually isn’t impossible to answer.
Many researchers have hypothesized that this may be due to DHT’s relationship with scar tissue. In scalp tissues, the arrival of DHT seems to also remodel our scalps – causing increased disorganized collagen crosshatchings. In other words, scalp DHT causes fibrosis (or scarring).
In fact, balding scalp regions have four times the amount of excess collagen deposition (scar tissue) than non-balding regions. And as we’ve learned in scleroderma studies, where there’s scar tissue, hair cannot grow.
DHT >> scar tissue >> hair loss
So maybe the reason why eliminating DHT doesn’t fully reverse hair loss… is simply because stopping DHT only stops the progression of scar tissue. It doesn’t necessarily reverse the scar tissue already present.
This makes sense. In fact, this is the explanation many AGA researchers use to describe why our recovery from AGA is “limited”. But interestingly, this explanation brings up another question that the DHT-hair loss theory has a much harder time answering.
Question: If DHT causes scarring and hair loss in the scalp… why does DHT encourage hair growth in other parts of the body?
Why does DHT encourage hair loss in the scalp… but hair growth in the chest and face?
You may have noticed that a lot of bald men also have incredibly hairy bodies. Well, this is because DHT can have two totally opposite effects on hair. It all depends on its location in the body.
For instance, studies show that while DHT in our scalps appears to encourage hair loss, DHT in body tissues (i.e., facial and chest skin) appears to encourage hair growth.
How can that be? How can DHT encourage hair growth in secondary body and facial hair… while simultaneously encouraging hair loss in our scalps?
Unfortunately, this is something the current DHT-androgenic alopecia pathology model cannot explain. So its supporters chalk it up to genetics – explaining it must be due to gene variants that are associated with more androgen receptors and their co-activators.
There’s some truth to this, but the reality is that nearly every single cell in our body carries the exact same genes. What differentiates a cornea cell from a skin cell is the combined influence of gene programming + a cell’s environment.
This means that “genetics” is sort of a blanket explanation for things we don’t understand. Not only is it the go-to answer for questions that exceed our knowledge base… it also completely undermines the influence of environment – which is often half (or more) of the equation.
In fact, there are several more questions that the DHT-AGA pathology model answers with the idea of “genetics” – but in reality, isn’t as supported by the literature as most tend to believe. Here they are:
Question #1: what causes DHT to increase in balding scalp tissues in the first place?
Question #2: why does DHT encourage hair loss in the scalp… but secondary hair growth in the body and face?
Question #3: why is there a pattern to AGA? Why does it begin at the temples and vertex for most men and generalized thinning for most women?
Question #4: why does AGA only affect the top part of our scalps – in areas that overlie the dense fibrous membrane known as the galea aponeurotica?
So, is it possible to answer these unanswered questions of AGA pathology, and in doing so, create a better model to explain the causes of pattern hair loss… all while not undermining any research demonstrating that DHT is causally linked to AGA?
Potentially. This is where the scalp tension theory of hair loss comes into play.
Scalp Tightness-Pattern Hair Loss Theory: A Deep-Dive
In 2017, I reintroduced the scalp tightness theory in a scholarly paper – particularly in light of new studies that reinforce its role in AGA. The rest of this article will explain the basics of that paper.
The best place to start is to attempt to provide answer those unanswered questions – and beyond “genetics”. Our first question: why does DHT increase in balding scalps?
Question #1: Why does DHT increase in balding scalps?
To get an idea of what might cause DHT to increase in balding scalp tissues, we need to have a bigger picture of what’s going on balding scalp tissues. That means it’s worth cataloguing most of the observations researchers have seen in balding scalps.
We’ve already discussed a few of these – like DHT and scar tissue. But there are many other things happening, too. And if we know what they are, maybe we can begin to parcel out a cause-and-effect relationship between balding scalps and increased DHT.
Here are the big ones from the paper.
Biological. Balding scalps have higher levels of androgen activity – specifically, DHT. And interestingly, balding scalps also express higher amounts of inflammation. We see this in the form of specific signaling proteins and reactive oxygen species (more on this later). These are things that commonly arrive in sites of “stress” – i.e., where the body senses an injury or an infection.
Physiological. Balding scalps have four-fold more disorganized collagen fibers (i.e., scar tissue) than non-balding scalps. And interestingly, the patterning and progression of this scar tissue appears to match the patterning and progression of AGA. In other words, where we see an increase in disorganized collagen cross-hatchings, we also see hair loss. Moreover, we also see that balding scalps have lower blood flow and lower oxygen levels than non-balding tissues – and that in all likelihood, the reduced blood flow occurs outside of our natural hair cycling.
Structural. Several dermatologists and AGA researchers have noted, anecdotally, that balding scalps appear to just “feel” tighter than non-balding scalps. This was also discussed by Dr. Brian Freund – a former university lecturer and hair loss researcher. He mentioned that his male and female patients with AGA almost always had incredibly tight scalps. There’s some evidence that this tension may come from involuntary contractions from our scalp’s perimeter muscles – which would pull the top of the scalp tightly – much like bending a finger pulls the knuckles tight.
Now that we have a better understanding of what’s going on in a balding scalp, we can revisit that initial question:
What causes DHT to increase in balding scalp tissues?
After all, maybe the answer is in one of these observations…
Clue #1: DHT is anti-inflammatory
Beyond its role in sexual maturation, studies also show that DHT can over-express in tissues as a response to inflammation – and that specifically, DHT is anti-inflammatory.
This is incredibly telling, especially in regard to androgenic alopecia research. After all, balding scalps show both increased inflammation and increased DHT. Maybe the inflammation observed in balding scalp tissues is what causes DHT to increase.
However, this opens a new question. If inflammation is what causes DHT to increase in balding scalps… what causes inflammation in the first place?
Reflecting back on our catalogue, there’s at least one possible culprit: chronic tissue tension.
Clue #2: tissue tension can “activate” inflammation and DHT
The relationship between tension, inflammation, and androgen activity isn’t very shocking. In fact, it’s been observed in several other regions. For instance…
- Inflamed periodontal tissues can signal to increase androgen activity.
- Men with a tendon-contracting condition known as Dupuytren’s contracture also express more inflammation and male hormones in the affected tissues.
- Graves’ disease sufferers often have chronic eyelid retraction due to the involuntary contraction of the Mueller muscle). In biopsies, this muscle shows higher markers of inflammation and often androgen activity.
- Prostate tissues, when exposed to cyclical stretching, induce inflammation and DHT-induced transforming growth factor beta-1 (more on that later).
All of this suggests that in balding scalps, chronic tension may induce the arrival of inflammation and DHT. To put it simply:
Chronic tension >> inflammation >> DHT
Now that we’ve have a potential reason for the “arrival” of DHT, we can ask a harder question:
Why is DHT linked to hair loss in the scalp… but hair growth in other body regions?
Fascinatingly, tension might also help explain this DHT paradox. Here’s how.
Chronic tension and androgens can induce scar tissue
Research shows that DHT behaves differently depending on its location. Specifically, DHT can increase hair loss in the scalp but also increase hair growth in the best and face. This suggests, at a minimum, that a tissue’s location has some sort of influence on the effects of DHT.
So, can tissue tension help us answer this DHT paradox?
Yes.
When DHT in chest and facial tissues, it induces more hair growth. But when DHT is expressed in the scalp – i.e., in tissues under chronic tension – DHT induces the arrival of a signaling protein called transforming growth factor beta 1 (or TGFβ-1).
This is interesting, because DHT doesn’t always appear to induce this signaling protein in tissues that aren’t under added contraction.
However, we do see DHT-induced TGFβ-1 in periodontal tissues, Dupreyene’s contracture, and in benign prostate hyperplasia. And fascinatingly, we also see DHT induce TGFB-1 in balding scalp dermal papilla cells (i.e., the cell clusters that influence the size of our hair follicle).
This signaling protein – TGFβ-1 – is universally condemned across biology as a biomarker for aging, and more specifically, as a prerequisite for the onset of fibrosis (scar tissue).
Studies have shown that wherever TGFβ-1 over-expresses, fibrosis soon follows. And as a reminder, balding scalps have four-fold more disorganized collagen crosshatchings (i.e., fibrosis) than non-balding scalps.
In fact, this scar tissue seems to develop alongside the pattern and progression of AGA. For men, it begins at the temples and vertex… and spreads to the rest of the scalp in accordance with hair follicle miniaturization.
The DHT-hair loss hypothesis suggests that fibrosis might be what limits our ability to regrow hair. But if fibrosis actually causes hair follicle miniaturization, then this would explain why DHT grows hair in the chest and face… but leads to hair loss in the scalp.
So, is there evidence that fibrosis or excess collagen deposition leads to baldness?
Yes.
Excess collagen (or scar tissue) can prevent hair growth
In the medical literature, one defining characteristic of scar tissue (i.e., fibrosis) is the absence of hair. In fibrosis-related disorders (like scleroderma), researchers have consistently observed that as fibrosis sets in, hair loss soon follows – even in the scalp.
And in this article, I lay out a few step-processes behind how fibrosis might contribute to hair follicle miniaturization. The gist is that excess collagen appears to onset outside of normal hair cycling and it seems to progress throughout hair follicle miniaturization – implying that its presence may possibly explain the production of smaller hairs in AGA.
This suggests that in AGA, fibrosis may cause hair loss, and through a few mechanisms: firstly, through the constriction of space for a hair follicle to grow. And secondly, through tissue degradation. Specifically, the restriction of blood, oxygen, and nutrients to the hair follicles.
DHT >> TGFβ-1 >> fibrosis >> reduced blood and oxygen >> hair loss
Taking a step back, DHT’s opposing “behavior” in the scalp versus the body might be explainable through the evidence that…
- In the presence of chronic tension, DHT induces signaling proteins which lead to scar tissue (and thereby hair follicle miniaturization)
- In the absence of chronic tension, DHT doesn’t induce these signaling proteins… so it simply encourages hair growth.
This is a subtle difference, but with potentially huge implications in the world of AGA. And we can now add these findings to our revised AGA model.
Chronic tension >> inflammatory response >> DHT >> TGFβ-1 >> fibrosis >> restricted blood flow >> hair follicle miniaturization >> pattern hair loss
However, there’s still one outstanding question… can tension also explain the pattern and progression of AGA? And if so, can it explain the differences in thinning patterns for both men and women?
The evidence points to yes.
Scalp tension may also explain the pattern and progression of AGA
In men with AGA, hair loss often starts at the temples and vertex. And fascinatingly, we also see this same patterning with scalp tension.
There are certain modeling softwares that allow us to estimate the tensile force of any surface – so long as we know the surface area and the direction and magnitude of forces applied to that surface.
In 2015, researchers decided to use a modeling software to map the tensile projections of the tops of male scalps. The forces applied to that surface? The contractions of the scalp perimeter muscles – the same chronic contractions noted by Dr. Brian Freund and other AGA researchers.
The findings? A near-perfect correlation between scalp tension peaks, the patterning of AGA, and the progression of male pattern hair loss. For a graphic reference…
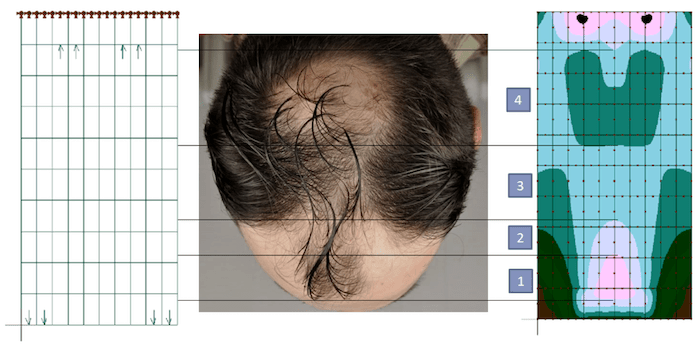
(source)
Since scar tissue also onsets in the pattern and progression of male AGA – this perfectly aligns with the idea that scalp tension might be the beginning of the hair loss cascade.
But what about women?
Unlike most men, most women don’t start thinning at the temples or vertex. Rather, they tend to lose hair in a diffuse pattern.
And what about hair loss that occurs in advanced stages of AGA – like hair loss we see at the nape of the neck, or behind the ears? Could tension also explain this?
Preliminary research points to yes.
In fact, other investigators have used the same modeling software to “play” with these tension projections. What they’ve found is that by making small tweaks head shape, size, and contraction force, it’s possible to create tensile patterns that match the pattern of hair loss we see in women.
In fact, it’s also possible to do the same for more advanced stages of AGA – like hair loss above the ears and at the nape of the neck. One researcher even shared his findings for free – which you can access here.
Where might this scalp tension come from?
This is going to be saved for another article. The short answer is that there are likely three major sources of scalp tension, and each creates a feedback loop with the others:
- The chronic involuntary contraction of muscles surrounding the perimeter of our scalps. Specifically, the muscles connected to the galea aponeurotica.
- Skull bone growth and skull suture settlement during and after puberty.
- Fascia remodeling surrounding the galea and its connected tissue networks.
Tying it all together – genetics, scalp tension, and AGA
This is a lot of information, and as such, it might help to see a visualization of everything above. As such, here’s the flowchart that I presented in my paper:

I know we didn’t cover every aspect on this flowchart. Doing so would’ve made this post twice as long. But I hope you can see the logic progression, and how everything ties together:
Scalp tension >> inflammation >> DHT >> TGFβ-1 >> fibrosis >> restricted blood flow >> hair follicle miniaturization >> pattern hair loss
So if scalp tension is a contributor to AGA… does relieving scalp tension improve AGA outcomes?
Yes.
Dr. Brian Freund demonstrated that in AGA sufferers, botox injections to relieve tension in chronically contracted scalp muscles increased hair counts by 18%. And this year, a new study confirmed Dr. Freund’s original findings. Finally, tension offloading devices also appear to improve hair growth in AGA subjects over 3-12 months periods. So at a minimum, it seems like targeting scalp tension improves hair growth in men and women with AGA.
Does the scalp tightness-hair loss hypothesis fit into all of the literature on AGA?
At face-value, the AGA theory of scalp tension satisfies the questions left unanswered in the current DHT-hair loss pathology model.
- Why does DHT increase in balding scalp tissues? It increased as part of an inflammatory response, and this inflammation is mediated by skin tension.
- Why is DHT associated with scalp hair loss and body hair growth? If expressed while under tension, DHT induces the expression of transforming growth factor beta 1, which leads to scarring and thereby hair loss. This tension is present in the scalp, but not in body tissues.
- Why is there a specific pattern and progression to AGA? This patterning matches the tensile patterning and progression of scalp tissues – with the highest tension points as the first to suffer from hair loss.
But does the scalp tightness-AGA theory make sense of all aspects of AGA research?
Not necessarily.
The reality is that I just presented the entire scalp tension argument to you in a bubble. I didn’t yet introduce a layer of complexity that, at first glance, could dismantle the theory entirely.
There is a complication to the scalp tightness hypothesis: a compelling counterargument. And it’s a big one. It’s the early findings from hair transplantation studies.
The scalp tension counterargument: hair transplantations
Remember in 1950 – when the scalp tension hypothesis made its way into academia? And in 1959 – how the scalp tightness theory was swiftly abandoned?
This is because that year (and the years following), researchers published several studies on hair transplants which completely changed the trajectory of hair loss research.
These studies sought to confirm if going bald had anything to do with the environment of our scalp tissues. Specifically, things like scalp tension.
To test this question, researchers decided to transplant skin grafts containing healthy hair into balding regions… and take skin grafts containing balding hair and transplant them into other parts of the body.
The findings? If we transplant hair follicles to or from a balding region…
- Non-thinning hairs moved to balding scalps keep growing normally.
- Thinning hairs moved to non-thinning regions keep thinning… at the same rate as thinning scalp hairs.
What did this suggest? That our scalp environment has nothing to do with balding.
Otherwise, why would thinning hairs transplanted out of a tense scalp environment keep thinning – even when placed in non-thinning regions? And why would healthy hairs transplanted into a tense environment keep growing – even as the hairs around them continue to thin?
This led researchers to abandon the scalp tension hypothesis, and instead conclude that baldness must be due to genetic programming within the hair follicle itself.
This idea of genetic determinism has been the prevailing theory for the last sixty years… until recently. Now new studies are making us question whether we drew the right conclusions about hair follicle miniaturization all those years ago.
And what are those studies? That’s for the next article.
Scalp Tension Summary
Research shows that balding men and women tend to have tighter scalp tissues than their non-balding counterparts. And interestingly, this scalp tension tends to align with the pattern and progression of AGA.
In men, tension is the highest where hair loss first begins (i.e., the vertex and temples), with skin tension dissipating alongside the “spread” of pattern hair loss. In women, equal tension can be modeled throughout the scalp skin – similar to a diffuse thinning pattern.
When our bodies sense a stressor (i.e., a cut, an impact, or an infection), they evoke an inflammatory response. Interestingly, this is also true for tissues under chronic tension. DHT has been shown to be anti-inflammatory, and when a tissue is under chronic tension, DHT tends to over-express. We’ve seen this in several disease states related to involuntary contractions. Resultantly, chronic scalp tension might not only explain the inflammatory biomarkers we see in balding scalps, but also the arrival of DHT (something the DHT-gene theory of AGA does not satisfactorily answer).
In cases where DHT is activated through tension, we also see DHT induce a signaling protein that causes scarring; specifically, TGFβ-1. This creates excess collagen deposition and scarring (or fibrosis), which then restricts blood, nutrient, and oxygen supplies to the affected tissues.
Interestingly, we see all of the above in balding tissues: increased DHT, increased TGFβ-1, increased fibrosis, lower blood flow, and lower oxygen levels… and in the exact same patterning as AGA.
Studies on scarring-related diseases demonstrate that where scar tissue accumulates, hair does not grow. And evidence suggests that fibrosis in our scalps may precede hair thinning. As fibrosis accumulates, this would cause hair follicle miniaturization through space restrictions alongside tissue degradation (i.e., reduced blood supply). The end-result: hair thinning in the pattern of AGA.
The scalp tension-AGA hypothesis, in my opinion, is the only hypothesis that satisfactorily makes sense of these unanswered questions in AGA research: 1) why does DHT increase in balding scalps, 2) why does DHT encourage hair loss and hair growth depending on its tissue location, and 3) why is there a “pattern” to pattern hair loss?
Unfortunately, hair transplantation studies from fifty years ago led researchers to conclude that our scalp environment – and specifically, scalp tension – have nothing to do with the onset of pattern hair loss. This led to the abandonment of the theory…
Until recently. In the next article, we’ll uncover why.
Note: Regardless of the evidence for or against scalp tension, there are potentially dozens of other factors kickstarting the inflammatory cascade that leads to hair loss. Therefore, scalp tension – if it truly does cause hair thinning – is just a contributor (and not a root cause). Future articles will explain why.
Want help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Learn More
Perfect Hair Health Team
"... Can’t thank @Rob (PHH) and @sanderson17 enough for allowing me to understand a bit what was going on with me and why all these [things were] happening ... "

 — RDB, 35, New York, U.S.A.
— RDB, 35, New York, U.S.A."... There is a lot improvement that I am seeing and my scalp feel alive nowadays... Thanks everyone. "

 — Aayush, 20’s, Boston, MA
— Aayush, 20’s, Boston, MA"... I can say that my hair volume/thickness is about 30% more than it was when I first started."

 — Douglas, 50’s, Montréal, Canada
— Douglas, 50’s, Montréal, CanadaWant help with your hair regrowth journey?
Get personalized support, product recommendations, video calls, and more from our researchers, trichologists, and PhD's dedicated to getting you the best possible outcomes.
Join Now - Mission Statement
